
Radiomics-Based Prediction of Future Portal Vein Tumor Infiltration in Patients with HCC—A Proof-of-Concept Study

 , , , , , ,
, , , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Recruitment
2.2. CT Examinations and Imaging Analysis
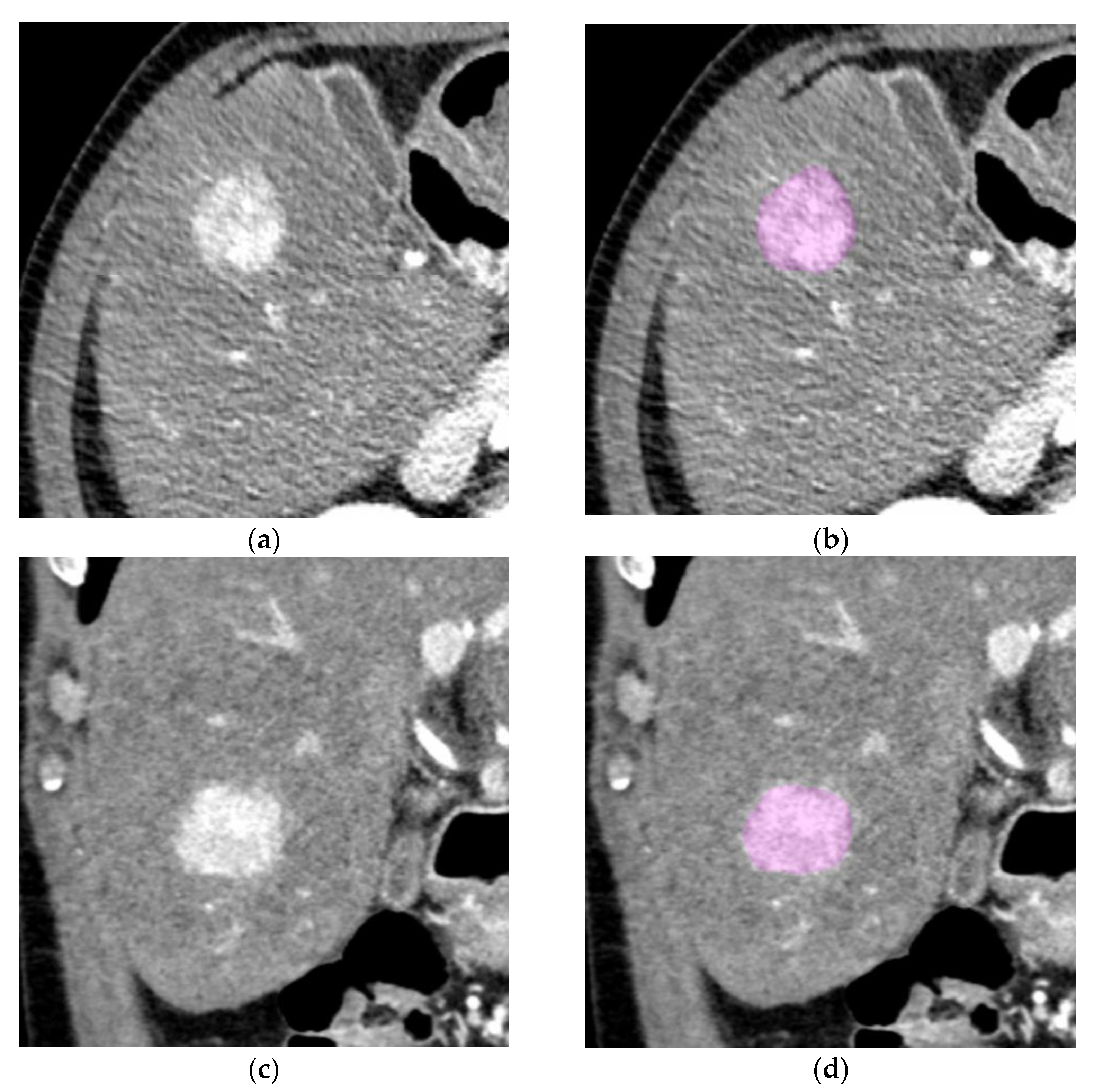
2.3. Segmentation and Texture Analysis
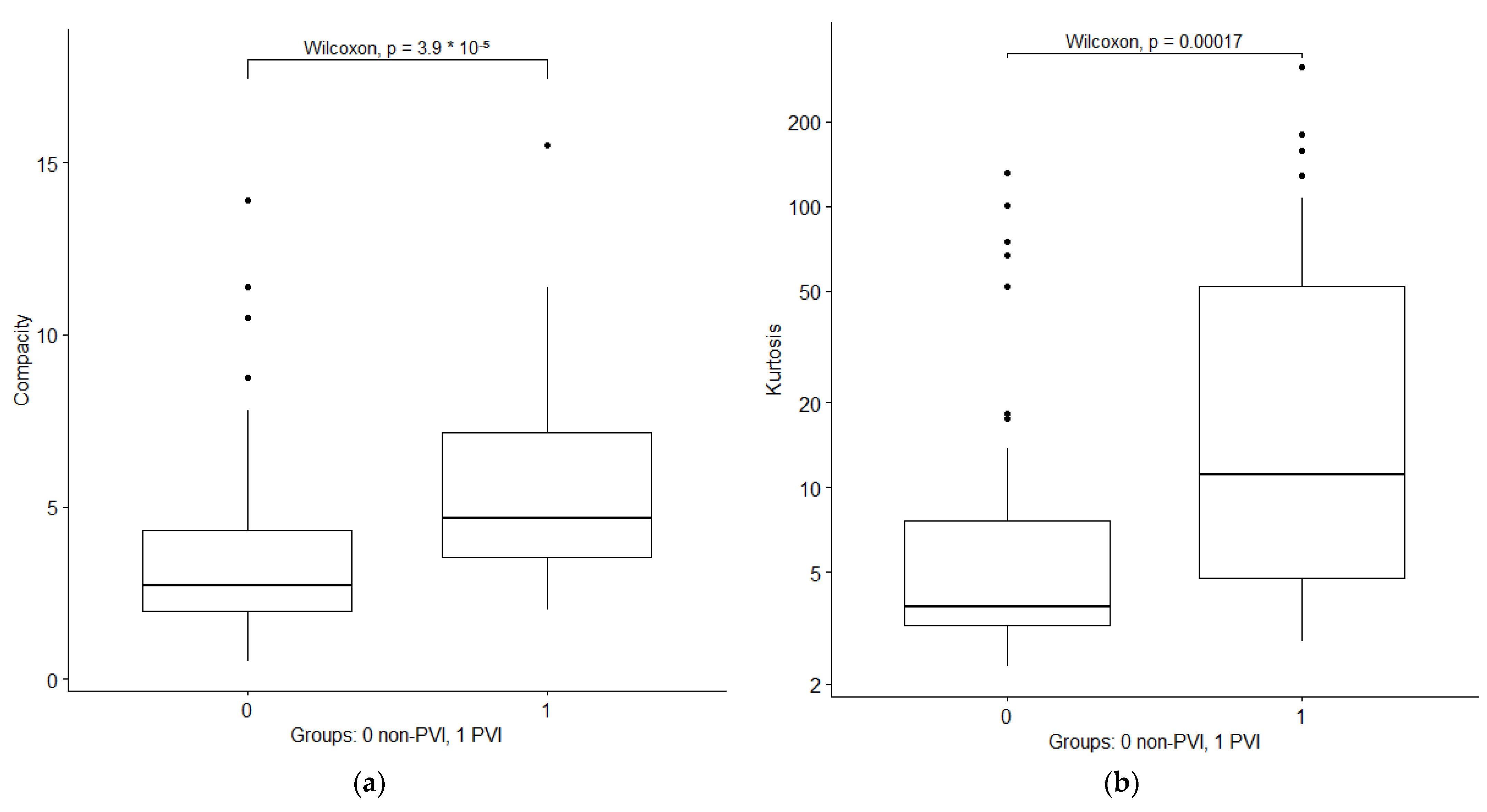
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
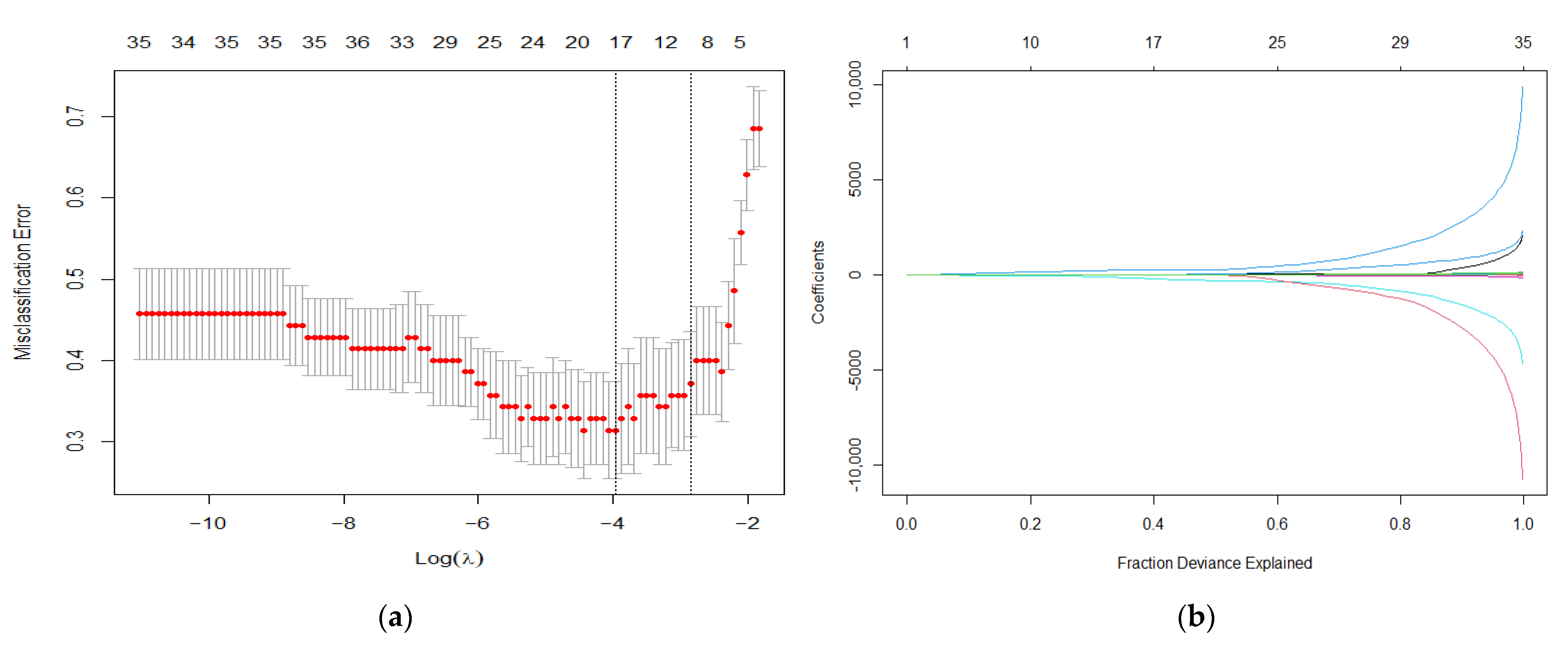
3.2. Feature Selection and Prediction Model Using LASSO Regression
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Llovet, J.M.; Zucman-Rossi, J.; Pikarsky, E.; Sangro, B.; Schwartz, M.; Sherman, M.; Gores, G. Hepatocellular carcinoma. Nat. Rev. Dis. Prim. 2016, 2, 16018. [Google Scholar] [CrossRef] [Green Version]
- Petrick, J.L.; Braunlin, M.; Laversanne, M.; Valery, P.C.; Bray, F.; McGlynn, K.A. International trends in liver cancer incidence, overall and by histologic subtype, 1978–2007. Int. J. Cancer 2016, 139, 1534–1545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [CrossRef] [PubMed] [Green Version]
- Cabibbo, G.; Enea, M.; Attanasio, M.; Bruix, J.; Craxì, A.; Cammà, C. A meta-analysis of survival rates of untreated patients in randomized clinical trials of hepatocellular carcinoma. Hepatology 2010, 51, 1274–1283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, T.-K.; Lai, C.-L.; Wong, B.C.-Y.; Fung, J.; Yuen, M.-F. Clinical features, biochemical parameters, and virological profiles of patients with hepatocellular carcinoma in Hong Kong. Aliment. Pharmacol. Ther. 2006, 24, 573–583. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.-F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.-L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mähringer-Kunz, A.; Steinle, V.; Düber, C.; Weinmann, A.; Koch, S.; Schmidtmann, I.; Schotten, S.; Hinrichs, J.B.; Graafen, D.; Pinto dos Santos, D.; et al. Extent of portal vein tumour thrombosis in patients with hepatocellular carcinoma: The more, the worse? Liver Int. 2019, 39, 324–331. [Google Scholar] [CrossRef]
- Minagawa, M.; Makuuchi, M. Treatment of hepatocellular carcinoma accompanied by portal vein tumor thrombus. World J. Gastroenterol. 2006, 12, 7561–7567. [Google Scholar] [CrossRef]
- Mähringer-Kunz, A.; Meyer, F.I.; Hahn, F.; Müller, L.; Düber, C.; Pinto dos Santos, D.; Galle, P.R.; Weinmann, A.; Kloeckner, R.; Schotten, S. Hepatic vein tumor thrombosis in patients with hepatocellular carcinoma: Prevalence and clinical significance. United Eur. Gastroenterol. J. 2021, 9, 590–597. [Google Scholar] [CrossRef]
- Kaufmann, S.; Schulze, M.; Spira, D.; Horger, M. Modern multimodality diagnosis of portal vein infiltration in hepatocellular carcinoma and expected changes during current therapies. Acta Radiol. 2015, 56, 1283–1292. [Google Scholar] [CrossRef]
- Thompson, S.M.; Wells, M.L.; Andrews, J.C.; Ehman, E.C.; Menias, C.O.; Hallemeier, C.L.; Roberts, L.R.; Venkatesh, S.K. Venous invasion by hepatic tumors: Imaging appearance and implications for management. Abdom. Radiol. 2018, 43, 1947–1967. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.L.; Chong, C.C.N.; Chan, A.W.H.; Poon, D.M.C.; Chok, K.S.H. Management of hepatocellular carcinoma with portal vein tumor thrombosis: Review and update at 2016. World J. Gastroenterol. 2016, 22, 7289–7300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connolly, G.C.; Chen, R.; Hyrien, O.; Mantry, P.; Bozorgzadeh, A.; Abt, P.; Khorana, A.A. Incidence, risk factors and consequences of portal vein and systemic thromboses in hepatocellular carcinoma. Thromb. Res. 2008, 122, 299–306. [Google Scholar] [CrossRef] [Green Version]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Kloeckner, R.; Galle, P.R.; Bruix, J. Local and Regional Therapies for Hepatocellular Carcinoma. Hepatology 2020, 73, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miranda Magalhaes Santos, J.M.; Clemente Oliveira, B.; Araujo-Filho, J.d.A.B.; Assuncao, A.N., Jr.; de M Machado, F.A.; Carlos Tavares Rocha, C.; Horvat, J.V.; Menezes, M.R.; Horvat, N. State-of-the-art in radiomics of hepatocellular carcinoma: A review of basic principles, applications, and limitations. Abdom. Radiol. 2020, 45, 342–353. [Google Scholar] [CrossRef]
- Davnall, F.; Yip, C.S.P.; Ljungqvist, G.; Selmi, M.; Ng, F.; Sanghera, B.; Ganeshan, B.; Miles, K.A.; Cook, G.J.; Goh, V. Assessment of tumor heterogeneity: An emerging imaging tool for clinical practice? Insights Imaging 2012, 3, 573–589. [Google Scholar] [CrossRef] [Green Version]
- Ganeshan, B.; Panayiotou, E.; Burnand, K.; Dizdarevic, S.; Miles, K. Tumour heterogeneity in non-small cell lung carcinoma assessed by CT texture analysis: A potential marker of survival. Eur. Radiol. 2012, 22, 796–802. [Google Scholar] [CrossRef]
- Weinmann, A.; Koch, S.; Niederle, I.M.; Schulze-Bergkamen, H.; König, J.; Hoppe-Lotichius, M.; Hansen, T.; Pitton, M.B.; Düber, C.; Otto, G.; et al. Trends in epidemiology, treatment, and survival of hepatocellular carcinoma patients between 1998 and 2009: An analysis of 1066 cases of a German HCC Registry. J. Clin. Gastroenterol. 2014, 48, 279–289. [Google Scholar] [CrossRef]
- Nioche, C.; Orlhac, F.; Boughdad, S.; Reuzé, S.; Goya-Outi, J.; Robert, C.; Pellot-Barakat, C.; Soussan, M.; Frouin, F.; Buvat, I. LIFEx: A Freeware for Radiomic Feature Calculation in Multimodality Imaging to Accelerate Advances in the Characterization of Tumor Heterogeneity. Cancer Res. 2018, 78, 4786–4789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherman, M. The Radiological Diagnosis of Hepatocellular Carcinoma. Am. J. Gastroenterol. 2010, 105, 610–612. [Google Scholar] [CrossRef] [PubMed]
- Demirjian, A.; Peng, P.; Geschwind, J.-F.H.; Cosgrove, D.; Schutz, J.; Kamel, I.R.; Pawlik, T.M. Infiltrating Hepatocellular Carcinoma: Seeing the Tree through the Forest. J. Gastrointest. Surg. 2011, 15, 2089–2097. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.K.; Han, Y.M.; Kim, C.S. Comparison of diffuse hepatocellular carcinoma and intrahepatic cholangiocarcinoma using sequentially acquired gadolinium-enhanced and Resovist-enhanced MRI. Eur. J. Radiol. 2009, 70, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Ganeshan, B.; Miles, K.A. Quantifying tumour heterogeneity with CT. Cancer Imaging 2013, 13, 140–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeong, W.K.; Jamshidi, N.; Felker, E.R.; Raman, S.S.; Lu, D.S. Radiomics and radiogenomics of primary liver cancers. Clin. Mol. Hepatol. 2018, 25, 21–29. [Google Scholar] [CrossRef]
- Yang, L.; Dong, D.; Fang, M.; Zhu, Y.; Zang, Y.; Liu, Z.; Zhang, H.; Ying, J.; Zhao, X.; Tian, J. Can CT-based radiomics signature predict KRAS/NRAS/BRAF mutations in colorectal cancer? Eur. Radiol. 2018, 28, 2058–2067. [Google Scholar] [CrossRef]
- Xu, X.; Zhang, H.-L.; Liu, Q.-P.; Sun, S.-W.; Zhang, J.; Zhu, F.-P.; Yang, G.; Yan, X.; Zhang, Y.-D.; Liu, X.-S. Radiomic analysis of contrast-enhanced CT predicts microvascular invasion and outcome in hepatocellular carcinoma. J. Hepatol. 2019, 70, 1133–1144. [Google Scholar] [CrossRef]
- Shan, Q.-Y.; Hu, H.-T.; Feng, S.-T.; Peng, Z.-P.; Chen, S.-L.; Zhou, Q.; Li, X.; Xie, X.-Y.; Lu, M.; Wang, W.; et al. CT-based peritumoral radiomics signatures to predict early recurrence in hepatocellular carcinoma after curative tumor resection or ablation. Cancer Imaging 2019, 19, 11. [Google Scholar] [CrossRef]
- Shah, S.A.; Tan, J.C.C.; McGilvray, I.D.; Cattral, M.S.; Levy, G.A.; Greig, P.D.; Grant, D.R. Does microvascular invasion affect outcomes after liver transplantation for HCC? A histopathological analysis of 155 consecutive explants. J. Gastrointest. Surg. 2007, 11, 464–471. [Google Scholar] [CrossRef]
- Chen, W.; Zhang, T.; Xu, L.; Zhao, L.; Liu, H.; Gu, L.R.; Wang, D.Z.; Zhang, M. Radiomics Analysis of Contrast-Enhanced CT for Hepatocellular Carcinoma Grading. Front. Oncol. 2021, 11, 660509. [Google Scholar] [CrossRef] [PubMed]
- Forner, A.; Reig, M.; Bruix, J. Hepatocellular carcinoma. Lancet 2018, 391, 1301–1314. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Brú, C.; Bruix, J. Prognosis of hepatocellular carcinoma: The BCLC staging classification. Semin. Liver Dis. 1999, 19, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef] [PubMed]
- Bolondi, L.; Burroughs, A.; Dufour, J.-F.; Galle, P.R.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.L.; Sangro, B. Heterogeneity of patients with intermediate (BCLC B) Hepatocellular Carcinoma: Proposal for a subclassification to facilitate treatment decisions. Semin. Liver Dis. 2012, 32, 348–359. [Google Scholar] [CrossRef]
- Hoshida, Y.; Villanueva, A.; Kobayashi, M.; Peix, J.; Chiang, D.Y.; Camargo, A.; Gupta, S.; Moore, J.; Wrobel, M.J.; Lerner, J.; et al. Gene expression in fixed tissues and outcome in hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 1995–2004. [Google Scholar] [CrossRef] [Green Version]
- Wakabayashi, T.; Ouhmich, F.; Gonzalez-Cabrera, C.; Felli, E.; Saviano, A.; Agnus, V.; Savadjiev, P.; Baumert, T.F.; Pessaux, P.; Marescaux, J.; et al. Radiomics in hepatocellular carcinoma: A quantitative review. Hepatol. Int. 2019, 13, 546–559. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Park, C.M.; Lee, M.; Park, S.J.; Song, Y.S.; Lee, J.H.; Hwang, E.J.; Goo, J.M. Impact of Reconstruction Algorithms on CT Radiomic Features of Pulmonary Tumors: Analysis of Intra- and Inter-Reader Variability and Inter-Reconstruction Algorithm Variability. PLoS ONE 2016, 11, e0164924. [Google Scholar] [CrossRef] [Green Version]
- Drechsler, K.; Strosche, M.; Oyarzun Laura, C. Automatic ROI identification for fast liver tumor segmentation using graph-cuts. In Proceedings of the Medical Imaging 2011: Image Processing, SPIE Medical Imaging, Lake Buena Vista, FL, USA, 12–17 February 2011. [Google Scholar]
- Hänsch, A.; Chlebus, G.; Meine, H.; Thielke, F.; Kock, F.; Paulus, T.; Abolmaali, N.; Schenk, A. Improving automatic liver tumor segmentation in late-phase MRI using multi-model training and 3D convolutional neural networks. Sci. Rep. 2022, 12, 12262. [Google Scholar] [CrossRef]
- Rahman, H.; Bukht, T.F.N.; Imran, A.; Tariq, J.; Tu, S.; Alzahrani, A. A Deep Learning Approach for Liver and Tumor Segmentation in CT Images Using ResUNet. Bioengineering 2022, 9, 368. [Google Scholar] [CrossRef]
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular carcinoma. Nat. Rev. Dis. Prim. 2021, 7, 6. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Wang, L.; Chai, Z.-T.; Zhu, Z.-M.; Zhu, X.-D.; Ma, D.-N.; Zhang, Q.-B.; Zhao, Y.-M.; Wang, M.; Ao, J.-Y.; et al. Incomplete radiofrequency ablation enhances invasiveness and metastasis of residual cancer of hepatocellular carcinoma cell HCCLM3 via activating β-catenin signaling. PLoS ONE 2014, 9, e115949. [Google Scholar] [CrossRef] [PubMed]
- Song, K.D.; Lee, M.W.; Rhim, H.; Kim, Y.-S.; Kang, T.W.; Shin, S.W.; Cho, S.K. Aggressive Intrasegmental Recurrence of Hepatocellular Carcinoma After Combined Transarterial Chemoembolization and Radiofrequency Ablation. AJR Am. J. Roentgenol. 2016, 207, 1122–1127. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Non-PVI Group (n = 44) | PVI Group (n = 44) | p-Value |
|---|---|---|---|
| Age, years [IQR] | 65 [59–72] | 71 [63–74] | 0.05 |
| Number of lesions, n [IQR] | 3 [1–6] | 4 [2–9] | 0.59 |
| Size of lesions, mm, median [IQR] | 39 [28–56] | 44 [32–68] | 0.62 |
| Growth type | |||
| nodular, n | 36 | 34 | |
| diffuse, n | 8 | 10 | 0.71 |
| Non-rim arterial enhancement pattern | |||
| hypervascular, n | 23 | 25 | |
| hypovascular, n | 4 | 4 | |
| mixed, n | 27 | 15 | 0.90 |
| Child–Pugh stage | |||
| A, n | 22 | 26 | |
| B, n | 22 | 17 | |
| C, n | 0 | 1 | 0.37 |
| AFP levels, ng/mL, mean [IQR] | 11,946 [16–22,316] | 15,193 [38–43,866] | 0.45 |
| Etiology | |||
| C2, n | 18 | 21 | |
| chronic hepatitis B, n | 8 | 6 | |
| chronic hepatitis C, n | 12 | 10 | |
| NASH, n | 4 | 3 | |
| unknown, n | 2 | 4 | 0.83 |
| Initial treatment * | |||
| curative, n | 10 | 8 | |
| intra-arterial, n | 33 | 35 | |
| systemic, n | 1 | 1 | 0.87 |
| Training Set | No PVI Occurred | PVI Occurred |
|---|---|---|
| No PVI predicted | 25 (71%) | 6 (17%) |
| PVI predicted | 10 (29%) | 29 (83%) |
| Holdout validation set | No PVI occurred | PVI occurred |
| No PVI predicted | 7 (78%) | 2 (22%) |
| PVI predicted | 2 (22%) | 7 (78%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stoehr, F.; Kloeckner, R.; Pinto dos Santos, D.; Schnier, M.; Müller, L.; Mähringer-Kunz, A.; Dratsch, T.; Schotten, S.; Weinmann, A.; Galle, P.R.; et al. Radiomics-Based Prediction of Future Portal Vein Tumor Infiltration in Patients with HCC—A Proof-of-Concept Study. Cancers 2022, 14, 6036. https://doi.org/10.3390/cancers14246036
Stoehr F, Kloeckner R, Pinto dos Santos D, Schnier M, Müller L, Mähringer-Kunz A, Dratsch T, Schotten S, Weinmann A, Galle PR, et al. Radiomics-Based Prediction of Future Portal Vein Tumor Infiltration in Patients with HCC—A Proof-of-Concept Study. Cancers. 2022; 14(24):6036. https://doi.org/10.3390/cancers14246036
Chicago/Turabian StyleStoehr, Fabian, Roman Kloeckner, Daniel Pinto dos Santos, Mira Schnier, Lukas Müller, Aline Mähringer-Kunz, Thomas Dratsch, Sebastian Schotten, Arndt Weinmann, Peter Robert Galle, and et al. 2022. "Radiomics-Based Prediction of Future Portal Vein Tumor Infiltration in Patients with HCC—A Proof-of-Concept Study" Cancers 14, no. 24: 6036. https://doi.org/10.3390/cancers14246036