
Development and Validation of Prognostic Models for Oral Squamous Cell Carcinoma: A Systematic Review and Appraisal of the Literature

 , , , ,
, , , ,  ,
,  , and
, and
Abstract
:Simple Summary
Abstract
1. Background
2. Materials and Methods
2.1. Protocol
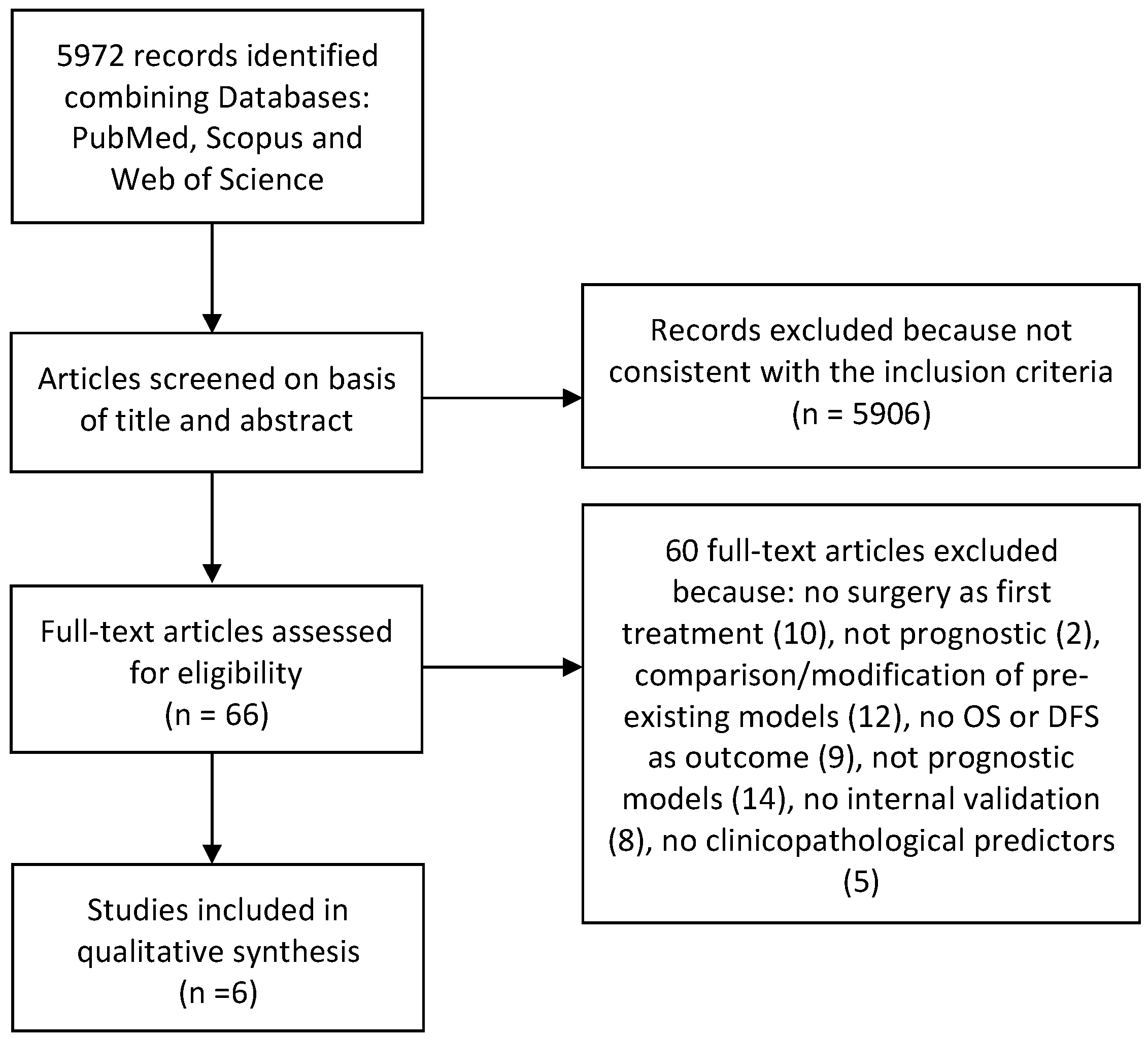
2.2. Search Strategy
2.3. Eligibility Criteria
2.4. Article Selection, Data Collection Process, and Data Items
2.5. Risk of Bias Assessment
3. Results
3.1. Study Characteristics and Model Development
3.2. Validation of the Models
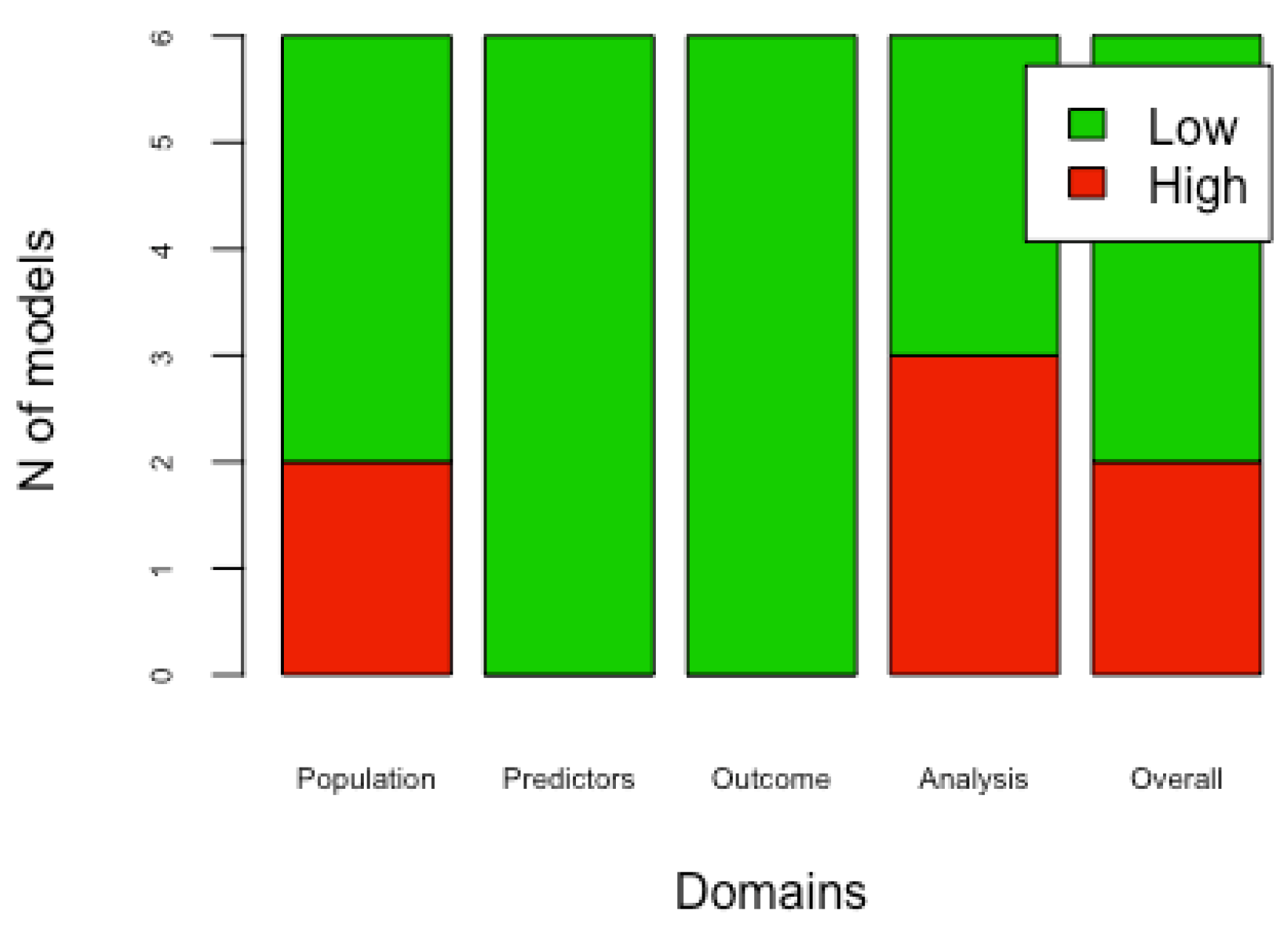
3.3. Risk of Bias
4. Discussions
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jiang, X.; Wu, J.; Wang, J.; Huang, R. Tobacco and oral squamous cell carcinoma: A review of carcinogenic pathways. Tob. Induc. Dis. 2019, 17, 1–9. [Google Scholar] [CrossRef]
- Fitzmaurice, C.; Abate, D.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdel-Rahman, O.; Abdelalim, A.; Abdoli, A.; Abdollahpour, I.; Abdulle, A.S.M.; et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2017. JAMA Oncol. 2019, 5, 1749. [Google Scholar] [CrossRef] [Green Version]
- Vassiliou, L.V.; Acero, J.; Gulati, A.; Hölzle, F.; Hutchison, I.L.; Prabhu, S.; Testelin, S.; Wolff, K.D.; Kalavrezos, N. Management of the clinically N0 neck in early-stage oral squamous cell carcinoma (OSCC). An EACMFS position paper. J. Cranio-Maxillofac. Surg. 2020, 48, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Almangush, A.; Mäkitie, A.A.; Triantafyllou, A.; de Bree, R.; Strojan, P.; Rinaldo, A.; Hernandez-Prera, J.C.; Suárez, C.; Kowalski, L.P.; Ferlito, A.; et al. Staging and grading of oral squamous cell carcinoma: An update. Oral Oncol. 2020, 107, 104799. [Google Scholar] [CrossRef]
- Rahman, N.; MacNeill, M.; Wallace, W.; Conn, B. Reframing Histological Risk Assessment of Oral Squamous Cell Carcinoma in the Era of UICC 8th Edition TNM Staging. Head Neck Pathol. 2021, 15, 202–211. [Google Scholar] [CrossRef]
- Moeckelmann, N.; Ebrahimi, A.; Tou, Y.K.; Gupta, R.; Low, T.H.; Ashford, B.; Ch’ng, S.; Palme, C.E.; Clark, J.R. Prognostic implications of the 8th edition American Joint Committee on Cancer (AJCC) staging system in oral cavity squamous cell carcinoma. Oral Oncol. 2018, 85, 82–86. [Google Scholar] [CrossRef]
- Steyerberg, E.W.; Moons, K.G.M.; van der Windt, D.A.; Hayden, J.A.; Perel, P.; Schroter, S.; Riley, R.D.; Hemingway, H.; Altman, D.G. Prognosis Research Strategy (PROGRESS) 3: Prognostic Model Research. PLoS Med. 2013, 10, e1001381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riley, R.D.; Moons, K.G.M.; Snell, K.I.E.; Ensor, J.; Hooft, L.; Altman, D.G.; Hayden, J.; Collins, G.S.; Debray, T.P.A. A guide to systematic review and meta-analysis of prognostic factor studies. BMJ 2019, 364, k4597. [Google Scholar] [CrossRef] [Green Version]
- Tham, T.; Machado, R.; Herman, S.W.; Kraus, D.; Costantino, P.; Roche, A. Personalized prognostication in head and neck cancer: A systematic review of nomograms according to the AJCC precision medicine core (PMC) criteria. Head Neck 2019, 41, 2811–2822. [Google Scholar] [CrossRef] [PubMed]
- Mattavelli, D.; Lombardi, D.; Missale, F.; Calza, S.; Battocchio, S.; Paderno, A.; Bozzola, A.; Bossi, P.; Vermi, W.; Piazza, C.; et al. Prognostic nomograms in oral squamous cell carcinoma: The negative impact of low neutrophil to lymphocyte ratio. Front. Oncol. 2019, 9, 339. [Google Scholar] [CrossRef] [Green Version]
- Troiano, G.; Caponio, V.C.A.; Botti, G.; Aquino, G.; Losito, N.S.; Pedicillo, M.C.; Zhurakivska, K.; Arena, C.; Ciavarella, D.; Mastrangelo, F.; et al. Immunohistochemical Analysis Revealed a Correlation between Musashi-2 and Cyclin-D1 Expression in Patients with Oral Squamous Cells Carcinoma. Int. J. Mol. Sci. 2019, 21, 121. [Google Scholar] [CrossRef] [Green Version]
- Heus, P.; Damen, J.A.A.G.; Pajouheshnia, R.; Scholten, R.J.P.M.; Reitsma, J.B.; Collins, G.S.; Altman, D.G.; Moons, K.G.M.; Hooft, L. Uniformity in measuring adherence to reporting guidelines: The example of TRIPOD for assessing completeness of reporting of prediction model studies. BMJ Open 2019, 9, e025611. [Google Scholar] [CrossRef] [PubMed]
- Moons, K.G.M.; Altman, D.G.; Reitsma, J.B.; Ioannidis, J.P.A.; Macaskill, P.; Steyerberg, E.W.; Vickers, A.J.; Ransohoff, D.F.; Collins, G.S. Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD): Explanation and Elaboration. Ann. Intern. Med. 2015, 162, W1–W73. [Google Scholar] [CrossRef] [Green Version]
- Kattan, M.W.; Hess, K.R.; Amin, M.B.; Lu, Y.; Moons, K.G.; Gershenwald, J.E.; Gimotty, P.A.; Guinney, J.H.; Halabi, S.; Lazar, A.J.; et al. American Joint Committee on Cancer acceptance criteria for inclusion of risk models for individualized prognosis in the practice of precision medicine. CA Cancer J. Clin. 2016, 66, 370–374. [Google Scholar] [CrossRef] [Green Version]
- Debray, T.P.A.; Damen, J.A.A.G.; Snell, K.I.E.; Ensor, J.; Hooft, L.; Reitsma, J.B.; Riley, R.D.; Moons, K.G.M. A guide to systematic review and meta-analysis of prediction model performance. BMJ 2017, 356, i6460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolff, R.F.; Moons, K.G.M.; Riley, R.D.; Whiting, P.F.; Westwood, M.; Collins, G.S.; Reitsma, J.B.; Kleijnen, J.; Mallett, S. PROBAST: A tool to assess the risk of bias and applicability of prediction model studies. Ann. Intern. Med. 2019, 170, 51–58. [Google Scholar] [CrossRef] [Green Version]
- Bossuyt, P.; Davenport, C.; Deeks, J.; Hyde, C.; Leeflang, M.; Scholten, R. Cochrane Handbook for Systematic Reviews of Diagnostic Test Accuracy Chapter 11 Interpreting Results and Drawing Conclusions. 2013, pp. 1–31. Available online: http://srdta.cochrane.org/ (accessed on 5 September 2021).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Moons, K.G.M.; de Groot, J.A.H.; Bouwmeester, W.; Vergouwe, Y.; Mallett, S.; Altman, D.G.; Reitsma, J.B.; Collins, G.S. Critical Appraisal and Data Extraction for Systematic Reviews of Prediction Modelling Studies: The CHARMS Checklist. PLoS Med. 2014, 11, e1001744. [Google Scholar] [CrossRef] [PubMed]
- Bobdey, S.; Balasubramaniam, G.; Mishra, P. Nomogram prediction for survival of patients with oral cavity squamous cell carcinoma. Head Neck 2016, 38, 1826–1831. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhao, Z.; Liu, X.; Ju, J.; Chai, J.; Ni, Q.; Ma, C.; Gao, T.; Sun, M. Nomograms to estimate long-term overall survival and tongue cancer-specific survival of patients with tongue squamous cell carcinoma. Cancer Med. 2017, 6, 1002–1013. [Google Scholar] [CrossRef]
- Montero, P.H.; Yu, C.; Palmer, F.L.; Patel, P.D.; Ganly, I.; Shah, J.P.; Shaha, A.R.; Boyle, J.O.; Kraus, D.H.; Singh, B.; et al. Nomograms for preoperative prediction of prognosis in patients with oral cavity squamous cell carcinoma. Cancer 2014, 120, 214–221. [Google Scholar] [CrossRef]
- Sun, W.; Cheng, M.; Zhuang, S.; Chen, H.; Yang, S.; Qiu, Z. Nomograms to predict survival of stage IV tongue squamous cell carcinoma after surgery. Medicine 2019, 98, e16206. [Google Scholar] [CrossRef]
- Bobdey, S.; Mair, M.; Nair, S.; Nair, D.; Balasubramaniam, G.; Chaturvedi, P. A Nomogram based prognostic score that is superior to conventional TNM staging in predicting outcome of surgically treated T4 buccal mucosa cancer: Time to think beyond TNM. Oral Oncol. 2018, 81, 10–15. [Google Scholar] [CrossRef]
- Chang, B.; He, W.; Ouyang, H.; Peng, J.; Shen, L.; Wang, A.; Wu, P. A prognostic nomogram incorporating depth of tumor invasion to predict long-term overall survival for tongue squamous cell carcinoma with R0 resection. J. Cancer 2018, 9, 2107–2115. [Google Scholar] [CrossRef] [Green Version]
- Chang, W.C.; Chang, C.F.; Li, Y.H.; Yang, C.Y.; Su, R.Y.; Lin, C.K.; Chen, Y.W. A histopathological evaluation and potential prognostic implications of oral squamous cell carcinoma with adverse features. Oral Oncol. 2019, 95, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Feng, Q.; May, M.T.; Ingle, S.; Lu, M.; Yang, Z.; Tang, J. Prognostic Models for Predicting Overall Survival in Patients with Primary Gastric Cancer: A Systematic Review. Biomed Res. Int. 2019, 2019, 5634598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wesdorp, N.J.; van Goor, V.J.; Kemna, R.; Jansma, E.P.; van Waesberghe, J.H.T.M.; Swijnenburg, R.J.; Punt, C.J.A.; Huiskens, J.; Kazemier, G. Advanced image analytics predicting clinical outcomes in patients with colorectal liver metastases: A systematic review of the literature. Surg. Oncol. 2021, 38, 101578. [Google Scholar] [CrossRef]
- Bradley, A.; Van Der Meer, R.; McKay, C.J. A systematic review of methodological quality of model development studies predicting prognostic outcome for resectable pancreatic cancer. BMJ Open 2019, 9, e027192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kreuzberger, N.; Damen, J.A.; Trivella, M.; Estcourt, L.J.; Aldin, A.; Umlauff, L.; Vazquez-Montes, M.D.; Wolff, R.; Moons, K.G.; Monsef, I.; et al. Prognostic models for newly-diagnosed chronic lymphocytic leukaemia in adults: A systematic review and meta-analysis. Cochrane Database Syst. Rev. 2020. [Google Scholar] [CrossRef]
- Wang, S.; Guan, X.; Ma, M.; Zhuang, M.; Ma, T.; Liu, Z.; Chen, H.; Jiang, Z.; Chen, Y.; Wang, G.; et al. Reconsidering the prognostic significance of tumour deposit count in the TNM staging system for colorectal cancer. Sci. Rep. 2020, 10, 89. [Google Scholar] [CrossRef]
- Brierley, J.; O’Sullivan, B.; Asamura, H.; Byrd, D.; Huang, S.H.; Lee, A.; Piñeros, M.; Mason, M.; Moraes, F.Y.; Rösler, W.; et al. Global Consultation on Cancer Staging: Promoting consistent understanding and use. Nat. Rev. Clin. Oncol. 2019, 16, 763–771. [Google Scholar] [CrossRef] [Green Version]
- Dijkland, S.A.; Retel Helmrich, I.R.A.; Steyerberg, E.W. Validation of prognostic models: Challenges and opportunities. J. Emerg. Crit. Care Med. 2018, 2, 91. [Google Scholar] [CrossRef] [Green Version]
- Bellou, V.; Belbasis, L.; Konstantinidis, A.K.; Tzoulaki, I.; Evangelou, E. Prognostic models for outcome prediction in patients with chronic obstructive pulmonary disease: Systematic review and critical appraisal. BMJ 2019, 367, l5358. [Google Scholar] [CrossRef] [Green Version]
- Iba, K.; Shinozaki, T.; Maruo, K.; Noma, H. Re-evaluation of the comparative effectiveness of bootstrap-based optimism correction methods in the development of multivariable clinical prediction models. BMC Med. Res. Methodol. 2021, 21, 9. [Google Scholar] [CrossRef]
- Zhang, Z.; Cortese, G.; Combescure, C.; Marshall, R.; Lee, M.; Lim, H.; Haller, B. Overview of model validation for survival regression model with competing risks using melanoma study data. Ann. Transl. Med. 2018, 6, 325. [Google Scholar] [CrossRef]
- Steyerberg, E.W.; Vickers, A.J.; Cook, N.R.; Gerds, T.; Gonen, M.; Obuchowski, N.; Pencina, M.J.; Kattan, M.W. Assessing the performance of prediction models: A framework for traditional and novel measures. Epidemiology 2010, 21, 128–138. [Google Scholar] [CrossRef] [Green Version]
- Austin, P.C.; Harrell, F.E.; van Klaveren, D. Graphical calibration curves and the integrated calibration index (ICI) for survival models. Stat. Med. 2020, 39, 2714–2742. [Google Scholar] [CrossRef]
- Pencina, M.J.; D’Agostino, R.B. Evaluating discrimination of risk prediction models: The C statistic. J. Am. Med. Assoc. 2015, 314, 1063–1064. [Google Scholar] [CrossRef]
- Harrell, F.E.; Lee, K.L.; Mark, D.B. Prognostic/Clinical Prediction Models: Multivariable Prognostic Models: Issues in Developing Models, Evaluating Assumptions and Adequacy, and Measuring and Reducing Errors. In Tutorials in Biostatistics; John Wiley & Sons, Ltd.: Chichester, UK, 2005; Volume 1, pp. 223–249. [Google Scholar] [CrossRef]
- Brentnall, A.R.; Cuzick, J. Use of the concordance index for predictors of censored survival data. Stat. Methods Med. Res. 2018, 27, 2359–2373. [Google Scholar] [CrossRef] [Green Version]
- Riley, R.D.; Hayden, J.A.; Steyerberg, E.W.; Moons, K.G.M.; Abrams, K.; Kyzas, P.A.; Malats, N.; Briggs, A.; Schroter, S.; Altman, D.G.; et al. Prognosis Research Strategy (PROGRESS) 2: Prognostic Factor Research. PLoS Med. 2013, 10, e1001380. [Google Scholar] [CrossRef] [Green Version]
- van Buuren, S.; Groothuis-Oudshoorn, K. mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef] [Green Version]
- Ramspek, C.L.; Jager, K.J.; Dekker, F.W.; Zoccali, C.; van Diepen, M. External validation of prognostic models: What, why, how, when and where? Clin. Kidney J. 2021, 14, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Kundu, S.; Mazumdar, M.; Ferket, B. Impact of correlation of predictors on discrimination of risk models in development and external populations. BMC Med. Res. Methodol. 2017, 17, 63. [Google Scholar] [CrossRef] [Green Version]
- Hingorani, A.D.; Van Der Windt, D.A.; Riley, R.D.; Abrams, K.; Moons, K.G.M.; Steyerberg, E.W.; Schroter, S.; Sauerbrei, W.; Altman, D.G.; Hemingway, H.; et al. Prognosis research strategy (PROGRESS) 4: Stratified medicine research. BMJ 2013, 346, e5793. [Google Scholar] [CrossRef] [Green Version]
- Bradburn, M.J.; Clark, T.G.; Love, S.B.; Altman, D.G. Survival Analysis Part II: Multivariate data analysis—An introduction to concepts and methods. Br. J. Cancer 2003, 89, 431–436. [Google Scholar] [CrossRef]
- Steyerberg, E.W.; Vergouwe, Y. Towards better clinical prediction models: Seven steps for development and an ABCD for validation. Eur. Heart J. 2014, 35, 1925–1931. [Google Scholar] [CrossRef] [Green Version]
- Duggan, M.A.; Anderson, W.F.; Altekruse, S.; Penberthy, L.; Sherman, M.E. The Surveillance, Epidemiology, and End Results (SEER) Program and Pathology. Am. J. Surg. Pathol. 2016, 40, e94–e102. [Google Scholar] [CrossRef]
- Zamanipoor Najafabadi, A.H.; Ramspek, C.L.; Dekker, F.W.; Heus, P.; Hooft, L.; Moons, K.G.M.; Peul, W.C.; Collins, G.S.; Steyerberg, E.W.; van Diepen, M. TRIPOD statement: A preliminary pre-post analysis of reporting and methods of prediction models. BMJ Open 2020, 10, e041537. [Google Scholar] [CrossRef]
- Zhao, R.; Jia, T.; Qiao, B.; Liang, J.; Qu, S.; Zhu, L.; Feng, H.; Xing, L.; Ren, Y.; Wang, F.; et al. Nomogram predicting long-term overall survival and cancer-specific survival of lip carcinoma patients based on the SEER database: A retrospective case-control study. Medicine 2019, 98, e16727. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Authors | Year | Country | Title | Source of Data | Sample Size | Validation Saple Size | Tumor Site | Outcome | Study |
|---|---|---|---|---|---|---|---|---|---|
| Bobdey [20] | 2016 | India | Nomogram prediction for survival of patients with oral cavity squamous cell carcinoma | Hospital-based | 609 | None | Lip, tongue, gum; floor of the mouth; hard palate; cheek mucosa; vestibule of mouth; retromolar trigone | 5 years Overall Survival | Retrospective study |
| Li [21] | 2017 | China | Nomograms to estimate long-term overall survival and tongue cancer-specific survival of patients with tongue squamous cell carcinoma | Population-based | 7587 | 191 | Tongue | 5 and 8 years Overall Survival | Retrospective study |
| Montero [22] | 2014 | USA | Nomograms for preoperative prediction of prognosis in patients with oral cavity squamous cell carcinoma | Hospital-based | 1617 | None | Buccal mucosa; tongue; floor of mouth; hard palate; upper gum; lower gum; retromolar trigone | 5 years Overall Survival | Retrospective study |
| Sun [23] | 2019 | China | Nomograms to predict survival of stage IV tongue squamous cell carcinoma after surgery | Population-based | 1085 | 465 | Tongue | 3 and 5 years Overall Survival | Retrospective study |
| Bobdey [24] | 2018 | India | A Nomogram based prognostic score that is superior to conventional TNM staging in predicting outcome of surgically treated T4 buccal mucosa cancer: Time to think beyond TNM | Hospital-based | 205 | 198 | Buccal mucosa | 3 years Overall Survival | Retrospective study |
| Chang [25] | 2018 | China | “A Prognostic Nomogram Incorporating Depth of Tumor Invasion to Predict Long-term Overall Survival for Tongue Squamous Cell Carcinoma with R0 Resection” | Hospital-based | 235 | 223 | Tongue | 5 years Overall Survival | Retrospective study |
| Author Year | Candidate Predictors | Final Predictors |
|---|---|---|
| Bobdey 2016 [20] | Age | Age |
| Bone infiltration | Clinical lymph node status | |
| Clinical lymph node status | Comorbidities | |
| Comorbidities | Differentiation | |
| Differentiation | Perineural invasion | |
| Perineural invasion | Stage | |
| Sex | Tumor thicknesss | |
| Stage | ||
| Tumor thicknesss | ||
| Li 2017 [21] | Age | Age |
| Grade | Grade | |
| M stage | M stage | |
| Martial status | Martial status | |
| N stage | N stage | |
| Race | Race | |
| Radiotherapy | T stage | |
| Sex | ||
| T stage | ||
| Montero 2014 [22] | Age | Age |
| Alcohol use | Clinical lymph node status | |
| Clinical lymph node status | Comorbidities | |
| Comorbidities | Race | |
| Invasion of other structures | Tobacco use | |
| Race | Tumor size | |
| Sex | ||
| Tobacco use | ||
| Tumor site | ||
| Tumor size | ||
| Sun 2019 [23] | Age | Age |
| Chemotherapy | M stage | |
| Grade | Martial status | |
| M stage | N stage | |
| Martial status | Race | |
| N stage | Radiotherapy | |
| Race | T stage | |
| Radiotherapy | Tumor site | |
| T stage | ||
| Tumor site | ||
| Bobdey 2017 [24] | Age | Bone infiltration |
| Bone infiltration | N stage | |
| Differentiation | Perineural invasion | |
| Extracapsular spread | ||
| N stage | ||
| Perineural invasion | ||
| Status of surgical margin | ||
| T stage | ||
| Chang 2018 [25] | Age | Age |
| Alcohol use | Depth of invasion | |
| Body mass index | N stage | |
| Clinical tumor stage | Neck dissection | |
| Crossing the midline of the tongue | ||
| Diabetes | ||
| Depth of invasion | ||
| Grade | ||
| Hypertension | ||
| M stage | ||
| Metabolic syndrome | ||
| N stage | ||
| Neck dissection | ||
| Race | ||
| Sex | ||
| T stage | ||
| Tobacco use | ||
| Treatment | ||
| Tumor site |
| Authors and Year | Internal Validation | Modelling Method | Handling of Missing Data | Model Discrimination | Model Calibration | Model Presentation | Handling of Continuous Predictors | Non-Linearity | Internal Validation C-Index | External Validation C-Index |
|---|---|---|---|---|---|---|---|---|---|---|
| Bobdey 2016 [20] | 1000-time bootstrapping | Multivariable Cox proportional hazards regression models and stepdown reduction method | n/a | C-statistic | n/a | Nomogram | Mixed: Continuous; Categorical/dichotomous | none | 0.7263 | none |
| Li 2017 [21] | 1000-time bootstrapping | Multivariable Cox proportional hazards regression models | n/a | C-statistic | Calibration plot | Nomogram | Categorical/dichotomous | n/a | 0.709 | 0.691 |
| Montero 2014 [22] | 1000-time bootstrapping | Multivariable Cox proportional hazards regression models and stepdown reduction method | Imputation | C-statistic | Calibration plot | Nomogram | Categorical/dichotomous | Cubic splines | 0.67 | none |
| Sun 2019 [23] | Combination of methods: 500-time bootstrapping; 5-fold cross-validation | Multivariable Cox proportional hazards regression models | n/a | C-statistic | Calibration plot | Nomogram | Mixed: Continuous; Categorical/dichotomous | none | 0.705 | 0.664 |
| Bobdey 2017 [24] | 1000-time bootstrapping | Multivariable Cox proportional hazards regression models and stepdown reduction method | n/a | C-statistic | n/a | Nomogram | Categorical/dichotomous | n/a | 0.7266 | 0.740 |
| Chang 2018 [25] | 1000-time bootstrapping | Multivariable Cox proportional hazards regression models | n/a | AUC | Calibration plot | Nomogram | Categorical/dichotomous | Cubic splines | 0.78 | 0.71 |
| Author Year | Domain 1 | Domain 2 | Domain 3 | Overall |
|---|---|---|---|---|
| Bodbey 2016 [20] | Low | Low | Low | Low |
| Li 2017 [21] | Low | Low | Low | Low |
| Montero 2014 [22] | Low | Low | Low | Low |
| Sun 2019 [23] | Low | Low | Low | Low |
| Bobdey 2017 [24] | Low | Low | High | High |
| Chang 2018 [25] | Low | Low | Low | Low |
| PROBAST_External Validation_Applicability | ||||
|---|---|---|---|---|
| Author Year | Domain 1 | Domain 2 | Domain 3 | Overall |
| Li 2017 [21] | Low | Low | Low | Low |
| Sun 2019 [23] | Low | Low | Low | Low |
| Bobday 2017 [24] | Low | Low | High | Low |
| Chang 2018 [25] | Low | Low | Low | Low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Russo, D.; Mariani, P.; Caponio, V.C.A.; Lo Russo, L.; Fiorillo, L.; Zhurakivska, K.; Lo Muzio, L.; Laino, L.; Troiano, G. Development and Validation of Prognostic Models for Oral Squamous Cell Carcinoma: A Systematic Review and Appraisal of the Literature. Cancers 2021, 13, 5755. https://doi.org/10.3390/cancers13225755
Russo D, Mariani P, Caponio VCA, Lo Russo L, Fiorillo L, Zhurakivska K, Lo Muzio L, Laino L, Troiano G. Development and Validation of Prognostic Models for Oral Squamous Cell Carcinoma: A Systematic Review and Appraisal of the Literature. Cancers. 2021; 13(22):5755. https://doi.org/10.3390/cancers13225755
Chicago/Turabian StyleRusso, Diana, Pierluigi Mariani, Vito Carlo Alberto Caponio, Lucio Lo Russo, Luca Fiorillo, Khrystyna Zhurakivska, Lorenzo Lo Muzio, Luigi Laino, and Giuseppe Troiano. 2021. "Development and Validation of Prognostic Models for Oral Squamous Cell Carcinoma: A Systematic Review and Appraisal of the Literature" Cancers 13, no. 22: 5755. https://doi.org/10.3390/cancers13225755