
Intraoperative Digital Analysis of Ablation Margins (DAAM) by Fluorescent Confocal Microscopy to Improve Partial Prostate Gland Cryoablation Outcomes

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Multiparametric Magnetic Resonance Imaging and Prostate Biopsy Technique
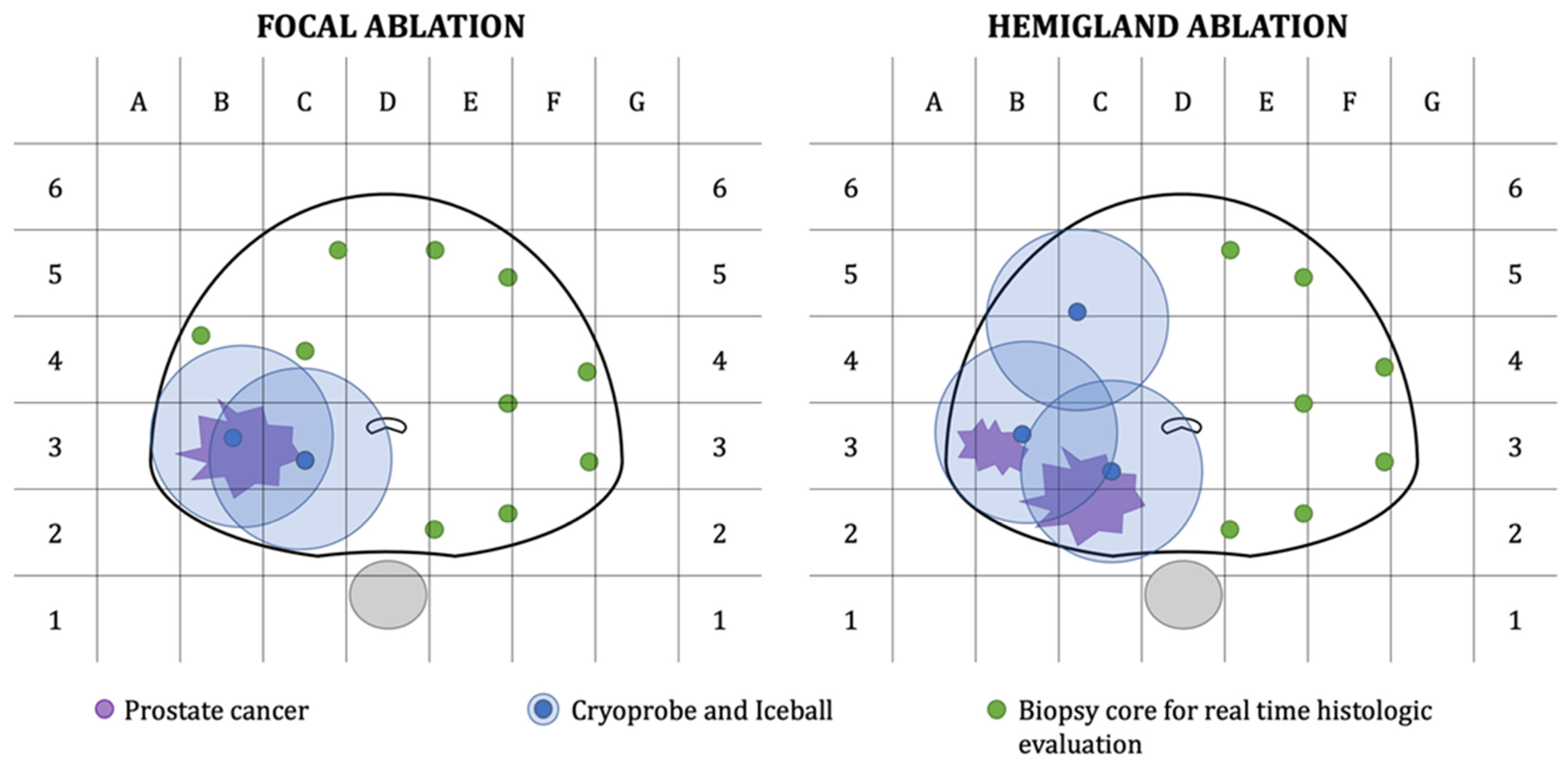
2.3. Prostate Gland Cryoablation with Intraoperative Digital Analysis of Ablation Margins (DAAM)
2.4. Final Pathology Examination
2.5. Study Endpoints and Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Cornford, P.; De Santis, M.; Fanti, S.; Gillessen, S.; Grummet, J.; Henry, A.M.; Lam, T.B.; et al. EAU-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer 2020. In European Association of Urology Guidelines; European Association of Urology Guidelines Office: Arnhem, The Netherlands, 2020. [Google Scholar]
- Oishi, M.; Gill, I.S.; Tafuri, A.; Shakir, A.; Cacciamani, G.E.; Iwata, T.; Iwata, A.; Ashrafi, A.; Park, D.; Cai, J.; et al. Hemigland Cryoablation of Localized Low, Intermediate and High Risk Prostate Cancer: Oncologic and Functional Outcomes at 5 Years. J. Urol. 2019, 202, 1188–1198. [Google Scholar] [CrossRef] [PubMed]
- Tran, M.; Thompson, J.; Bohm, M.; Pulbrook, M.; Moses, D.; Shnier, R.; Brenner, P.; Delprado, W.; Haynes, A.M.; Savdie, R.; et al. Combination of multiparametric MRI and transperineal template-guided mapping biopsy of the prostate to identify candidates for hemi-ablative focal therapy. BJU Int. 2016, 117, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Shah, T.T.; Peters, M.; Eldred-Evans, D.; Miah, S.; Yap, T.; Faure-Walker, N.A.; Hosking-Jervis, F.; Thomas, B.; Dudderidge, T.; Hindley, R.G.; et al. Early-Medium-Term Outcomes of Primary Focal Cryotherapy to Treat Nonmetastatic Clinically Significant Prostate Cancer from a Prospective Multicentre Registry. Eur. Urol. 2019, 76, 98–105. [Google Scholar] [CrossRef]
- Chuang, R.; Kinnaird, A.; Kwan, L.; Sisk, A.; Barsa, D.; Felker, E.; Delfin, M.; Marks, L. Hemigland Cryoablation of Clinically Significant Prostate Cancer: Intermediate-Term Followup via Magnetic Resonance Imaging Guided Biopsy. J. Urol. 2020, 204, 941–949. [Google Scholar] [CrossRef]
- Wajswol, E.; Winoker, J.S.; Anastos, H.; Falagario, U.; Okhawere, K.; Martini, A.; Treacy, P.J.; Voutsinas, N.; Knauer, C.J.; Sfakianos, J.P.; et al. A cohort of transperineal electromagnetically tracked magnetic resonance imaging/ultrasonography fusion-guided biopsy: Assessing the impact of inter-reader variability on cancer detection. BJU Int. 2019, 125, 531–540. [Google Scholar] [CrossRef]
- Moreira, P.; Tuncali, K.; Tempany, C.M.; Tokuda, J. The Impact of Placement Errors on the Tumor Coverage in MRI-Guided Focal Cryoablation of Prostate Cancer. Acad. Radiol. 2020, 28, 841–848. [Google Scholar] [CrossRef]
- Bertoni, L.; Puliatti, S.; Reggiani Bonetti, L.; Maiorana, A.; Eissa, A.; Azzoni, P.; Bevilacqua, L.; Spandri, V.; Kaleci, S.; Zoeir, A.; et al. Ex vivo fluorescence confocal microscopy: Prostatic and periprostatic tissues atlas and evaluation of the learning curve. Virchows Arch. 2020, 476, 511–520. [Google Scholar] [CrossRef] [Green Version]
- Rocco, B.; Sighinolfi, M.C.; Sandri, M.; Spandri, V.; Cimadamore, A.; Volavsek, M.; Mazzucchelli, R.; Lopez-Beltran, A.; Eissa, A.; Bertoni, L.; et al. Digital Biopsy with Fluorescence Confocal Microscope for Effective Real-time Diagnosis of Prostate Cancer: A Prospective, Comparative Study. Eur. Urol. Oncol. 2020, S2588–S9311. [Google Scholar] [CrossRef]
- Rocco, B.; Sighinolfi, M.C.; Cimadamore, A.; Reggiani Bonetti, L.; Bertoni, L.; Puliatti, S.; Eissa, A.; Spandri, V.; Azzoni, P.; Dinneen, E.; et al. Digital frozen section of the prostate surface during radical prostatectomy: A novel approach to evaluate surgical margins. BJU Int. 2020, 126, 336–338. [Google Scholar] [CrossRef]
- Turkbey, B.; Rosenkrantz, A.B.; Haider, M.A.; Padhani, A.R.; Villeirs, G.; Macura, K.J.; Tempany, C.M.; Choyke, P.L.; Cornud, F.; Margolis, D.J.; et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur. Urol 2019, 76, 340–351. [Google Scholar] [CrossRef] [PubMed]
- Cormio, L.; Lucarelli, G.; Selvaggio, O.; Di Fino, G.; Mancini, V.; Massenio, P.; Troiano, F.; Sanguedolce, F.; Bufo, P.; Carrieri, G. Absence of Bladder Outlet Obstruction Is an Independent Risk Factor for Prostate Cancer in Men Undergoing Prostate Biopsy. Medicine 2016, 95, e2551. [Google Scholar] [CrossRef] [PubMed]
- van Leenders, G.; van der Kwast, T.H.; Grignon, D.J.; Evans, A.J.; Kristiansen, G.; Kweldam, C.F.; Litjens, G.; McKenney, J.K.; Melamed, J.; Mottet, N.; et al. The 2019 International Society of Urological Pathology (ISUP) Consensus Conference on Grading of Prostatic Carcinoma. Am. J. Surg. Pathol. 2020, 44, e87–e99. [Google Scholar] [CrossRef]
- Sanguedolce, F.; Cormio, A.; Musci, G.; Troiano, F.; Carrieri, G.; Bufo, P.; Cormio, L. Typing the atypical: Diagnostic issues and predictive markers in suspicious prostate lesions. Crit. Rev. Clin. Lab. Sci. 2017, 54, 309–325. [Google Scholar] [CrossRef]
- Mitropoulos, D.; Artibani, W.; Biyani, C.S.; Bjerggaard Jensen, J.; Roupret, M.; Truss, M. Validation of the Clavien-Dindo Grading System in Urology by the European Association of Urology Guidelines Ad Hoc Panel. Eur. Urol. Focus 2018, 4, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Stabile, A.; Orczyk, C.; Giganti, F.; Moschini, M.; Allen, C.; Punwani, S.; Cathala, N.; Ahmed, H.U.; Cathelineau, X.; Montorsi, F.; et al. The Role of Percentage of Prostate-specific Antigen Reduction After Focal Therapy Using High-intensity Focused Ultrasound for Primary Localised Prostate Cancer. Results from a Large Multi-institutional Series. Eur. Urol. 2020, 78, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Gross, M.D.; Sedrakyan, A.; Bianco, F.J.; Carroll, P.R.; Daskivich, T.J.; Eggener, S.E.; Ehdaie, B.; Fisher, B.; Gorin, M.A.; Hunt, B.; et al. SPARED Collaboration: Patient Selection for Partial Gland Ablation in Men with Localized Prostate Cancer. J. Urol. 2019, 202, 952–958. [Google Scholar] [CrossRef]
- Fereidouni, F.; Harmany, Z.T.; Tian, M.; Todd, A.; Kintner, J.A.; McPherson, J.D.; Borowsky, A.D.; Bishop, J.; Lechpammer, M.; Demos, S.G.; et al. Microscopy with ultraviolet surface excitation for rapid slide-free histology. Nat. Biomed. Eng. 2017, 1, 957–966. [Google Scholar] [CrossRef]
- Glaser, A.K.; Reder, N.P.; Chen, Y.; McCarty, E.F.; Yin, C.; Wei, L.; Wang, Y.; True, L.D.; Liu, J.T.C. Light-sheet microscopy for slide-free non-destructive pathology of large clinical specimens. Nat. Biomed. Eng. 2017, 1, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.T.W.; Zhang, R.; Hai, P.; Zhang, C.; Pleitez, M.A.; Aft, R.L.; Novack, D.V.; Wang, L.V. Fast label-free multilayered histology-like imaging of human breast cancer by photoacoustic microscopy. Sci. Adv. 2017, 3, e1602168. [Google Scholar] [CrossRef] [Green Version]
- Assayag, O.; Antoine, M.; Sigal-Zafrani, B.; Riben, M.; Harms, F.; Burcheri, A.; Grieve, K.; Dalimier, E.; Le Conte de Poly, B.; Boccara, C. Large field, high resolution full-field optical coherence tomography: A pre-clinical study of human breast tissue and cancer assessment. Technol. Cancer Res. Treat. 2014, 13, 455–468. [Google Scholar] [CrossRef] [Green Version]
- Tao, Y.K.; Shen, D.; Sheikine, Y.; Ahsen, O.O.; Wang, H.H.; Schmolze, D.B.; Johnson, N.B.; Brooker, J.S.; Cable, A.E.; Connolly, J.L.; et al. Assessment of breast pathologies using nonlinear microscopy. Proc. Natl. Acad. Sci. USA 2014, 111, 15304–15309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- You, S.; Sun, Y.; Chaney, E.J.; Zhao, Y.; Chen, J.; Boppart, S.A.; Tu, H. Slide-free virtual histochemistry (Part II): Detection of field cancerization. Biomed. Opt. Express 2018, 9, 5253–5268. [Google Scholar] [CrossRef] [PubMed]
- Schlomm, T.; Tennstedt, P.; Huxhold, C.; Steuber, T.; Salomon, G.; Michl, U.; Heinzer, H.; Hansen, J.; Budaus, L.; Steurer, S.; et al. Neurovascular structure-adjacent frozen-section examination (NeuroSAFE) increases nerve-sparing frequency and reduces positive surgical margins in open and robot-assisted laparoscopic radical prostatectomy: Experience after 11,069 consecutive patients. Eur. Urol. 2012, 62, 333–340. [Google Scholar] [CrossRef]
- Mirmilstein, G.; Rai, B.P.; Gbolahan, O.; Srirangam, V.; Narula, A.; Agarwal, S.; Lane, T.M.; Vasdev, N.; Adshead, J. The neurovascular structure-adjacent frozen-section examination (NeuroSAFE) approach to nerve sparing in robot-assisted laparoscopic radical prostatectomy in a British setting—A prospective observational comparative study. BJU Int. 2018, 121, 854–862. [Google Scholar] [CrossRef] [PubMed]
- Marenco, J.; Calatrava, A.; Casanova, J.; Claps, F.; Mascaros, J.; Wong, A.; Barrios, M.; Martin, I.; Rubio, J. Evaluation of Fluorescent Confocal Microscopy for Intraoperative Analysis of Prostate Biopsy Cores. Eur. Urol. Focus 2020. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study Population (N = 10) | |
|---|---|
| Age, years | 70 (68, 73) |
| PSA, ng/mL | 6.9 (6.2, 8.9) |
| DRE, n (%) | |
| Negative | 4 (40.0%) |
| Positive | 6 (60.0%) |
| PIRADS, n (%) | |
| 2 | 2 (20.0%) |
| 3 | 2 (20.0%) |
| 4 | 4 (40.0%) |
| 5 | 2 (20.0%) |
| Prostate Volume, cc | 41.5 (40.0, 50.0) |
| Positive cores | 3.5 (3.0, 5.0) |
| Bx GG, n (%) | |
| 1 | 4 (40.0%) |
| 2 | 4 (40.0%) |
| 3 | 2 (20.0%) |
| EAU risk, n (%) | |
| Low risk | 3 (30.0%) |
| Intermediate Risk | 7 (70.0%) |
| Treatment, n (%) | |
| Focal ablation | 4 (40.0%) |
| Hemigland Ablation | 6 (60.0%) |
| N of Probes | 3.5 (2.0, 4.0) |
| Intraoperative cores, n (%) | |
| 7 | 8 (80.0%) |
| 10 | 2 (20.0%) |
| Time to FCM diagnosis | 25 (25, 27) |
| 3-month PSA, ng/mL | 1.4 (1.0, 1.6) |
| PSA drop, ng/mL | 5.7 (4.7, 6.6) |
| Percentage of PSA reduction | 79.0 (78.0, 85.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Selvaggio, O.; Falagario, U.G.; Bruno, S.M.; Recchia, M.; Sighinolfi, M.C.; Sanguedolce, F.; Milillo, P.; Macarini, L.; Rastinehad, A.R.; Sanchez-Salas, R.; et al. Intraoperative Digital Analysis of Ablation Margins (DAAM) by Fluorescent Confocal Microscopy to Improve Partial Prostate Gland Cryoablation Outcomes. Cancers 2021, 13, 4382. https://doi.org/10.3390/cancers13174382
Selvaggio O, Falagario UG, Bruno SM, Recchia M, Sighinolfi MC, Sanguedolce F, Milillo P, Macarini L, Rastinehad AR, Sanchez-Salas R, et al. Intraoperative Digital Analysis of Ablation Margins (DAAM) by Fluorescent Confocal Microscopy to Improve Partial Prostate Gland Cryoablation Outcomes. Cancers. 2021; 13(17):4382. https://doi.org/10.3390/cancers13174382
Chicago/Turabian StyleSelvaggio, Oscar, Ugo Giovanni Falagario, Salvatore Mariano Bruno, Marco Recchia, Maria Chiara Sighinolfi, Francesca Sanguedolce, Paola Milillo, Luca Macarini, Ardeshir R. Rastinehad, Rafael Sanchez-Salas, and et al. 2021. "Intraoperative Digital Analysis of Ablation Margins (DAAM) by Fluorescent Confocal Microscopy to Improve Partial Prostate Gland Cryoablation Outcomes" Cancers 13, no. 17: 4382. https://doi.org/10.3390/cancers13174382