On-Treatment Changes in FIB-4 and 1-Year FIB-4 Values Help Identify Patients with Chronic Hepatitis B Receiving Entecavir Therapy Who Have the Lowest Risk of Hepatocellular Carcinoma

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Baseline and On-Treatment Characteristics
2.2. APRI, FIB-4, and On-Treatment Changes
2.3. Baseline and On-Treatment Factors Associated with HCC Occurrence
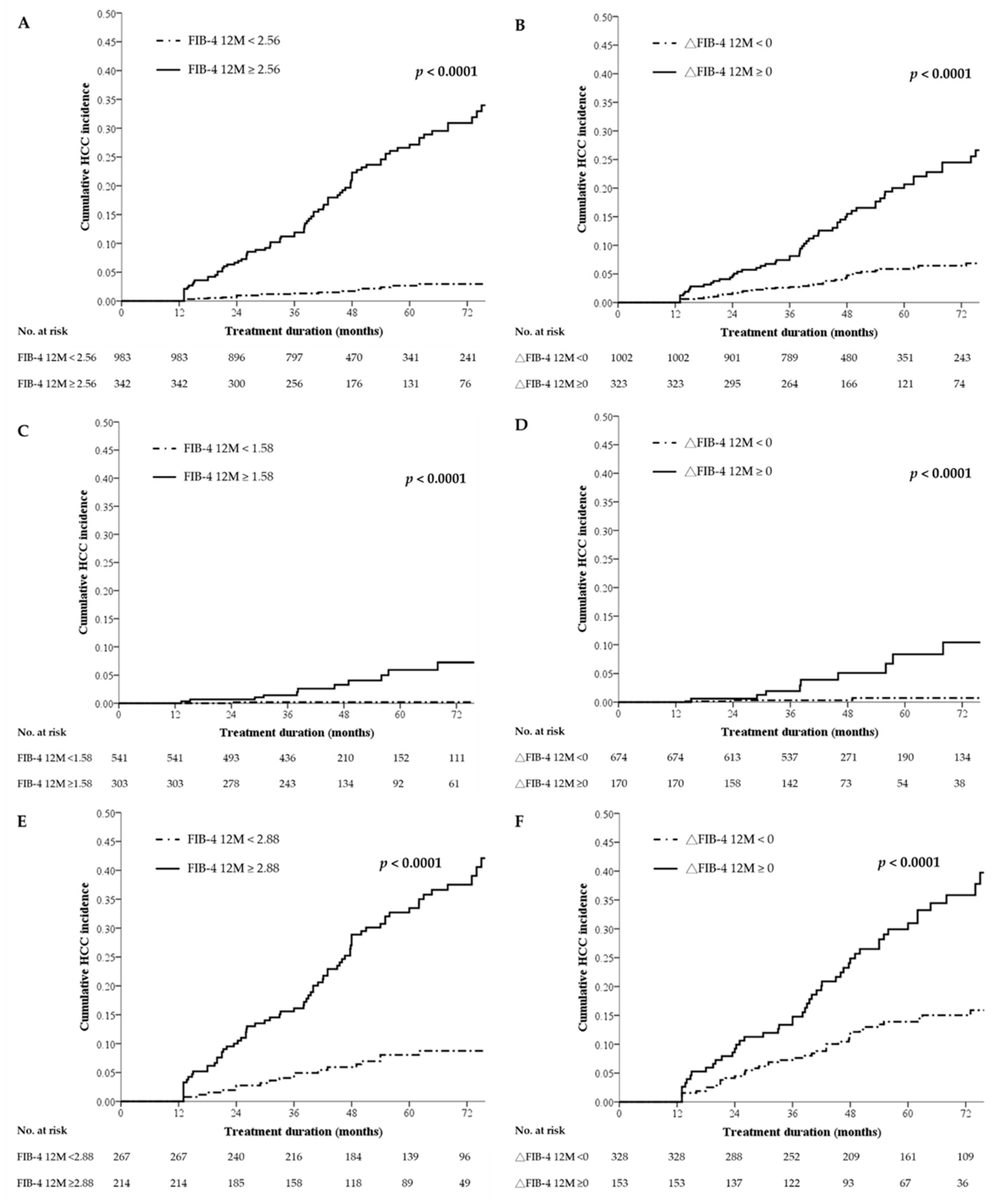
2.4. Cumulative Incidence of HCC Stratified by 1-Year FIB-4 Values or On-Treatment Changes in FIB-4
2.5. Comparison of Baseline Characteristics among the Subgroups Stratified by On-Treatment Changes in FIB-4
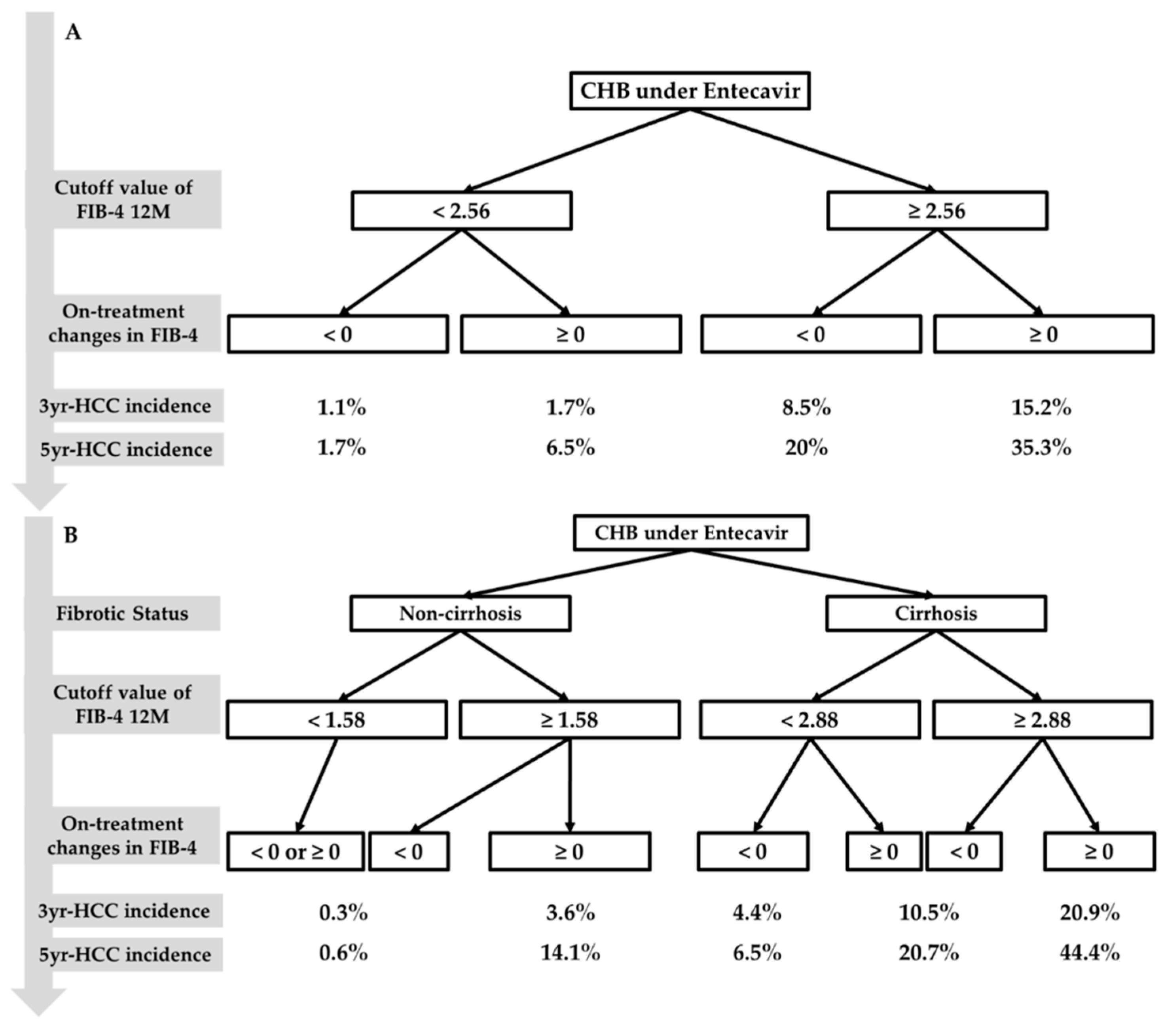
2.6. Cumulative Incidence of HCC Stratified by the Combination of On-Treatment Changes in FIB-4 and 1-Year FIB-4 Values
2.7. Performance of the Predictive Algorithm for HCC in the Cirrhotic Subgroup with Liver Biopsies
2.8. Performance of the Predictive Algorithm in Cohorts Who Received 3 or 5 Years of Continuous Entecavir Therapy
2.9. Comparison of AUROCs among Different HCC Prediction Models
3. Discussion
4. Materials and Methods
4.1. Patient Recruitment and Definitions
4.2. Statistical Analysis
5. Conclusions
Supplementary Materials
 Group 1, FIB-4 12M < 2.88 and △FIB-4 < 0;
Group 1, FIB-4 12M < 2.88 and △FIB-4 < 0;  Group 2 FIB-4 12M ≥ 2.88 and △FIB-4 < 0 or FIB-4 12M < 2.88 and △FIB-4 ≥ 0;
Group 2 FIB-4 12M ≥ 2.88 and △FIB-4 < 0 or FIB-4 12M < 2.88 and △FIB-4 ≥ 0;  Group 3 FIB-4 12M ≥ 2.88 and △FIB-4 ≥ 0, Figure S2: HCC risk stratification by a combination of FIB-4 12M and △FIB-4 in (A) all patients treated with entecavir ≥ 3 years:
Group 3 FIB-4 12M ≥ 2.88 and △FIB-4 ≥ 0, Figure S2: HCC risk stratification by a combination of FIB-4 12M and △FIB-4 in (A) all patients treated with entecavir ≥ 3 years:  Group 1, FIB-4 12M < 2.56 and △FIB-4 < 0; Group 2, FIB-4 12M < 2.56 and △FIB-4 ≥ 0;
Group 1, FIB-4 12M < 2.56 and △FIB-4 < 0; Group 2, FIB-4 12M < 2.56 and △FIB-4 ≥ 0;  Group 3, FIB-4 12M ≥ 2.56 and △FIB-4 < 0; Group 4, FIB-4 12M ≥ 2.56 and △FIB-4 ≥ 0; (B) noncirrhotic patients treated with entecavir ≥ 3 years: Group 1, FIB-4 12M < 1.58 and △FIB-4 < 0; Group 2, FIB-4 12M ≥ 1.58 and △FIB-4 < 0 or FIB-4 12M < 1.58 and △FIB-4 ≥ 0; Group 3, FIB-4 12M ≥ 1.58 and △FIB-4 ≥ 0 and (C) cirrhotic patients treated with entecavir ≥ 3 years: Group 1, FIB-4 12M < 2.88 and △FIB-4 < 0; Group 2 FIB-4 12M ≥ 2.88 and △FIB-4 < 0 or FIB-4 12M < 2.88 and △FIB-4 ≥ 0; Group 3 FIB-4 12M ≥ 2.88 and △FIB-4 ≥ 0, Supplementary Methods: Details on multiple imputation.
Group 3, FIB-4 12M ≥ 2.56 and △FIB-4 < 0; Group 4, FIB-4 12M ≥ 2.56 and △FIB-4 ≥ 0; (B) noncirrhotic patients treated with entecavir ≥ 3 years: Group 1, FIB-4 12M < 1.58 and △FIB-4 < 0; Group 2, FIB-4 12M ≥ 1.58 and △FIB-4 < 0 or FIB-4 12M < 1.58 and △FIB-4 ≥ 0; Group 3, FIB-4 12M ≥ 1.58 and △FIB-4 ≥ 0 and (C) cirrhotic patients treated with entecavir ≥ 3 years: Group 1, FIB-4 12M < 2.88 and △FIB-4 < 0; Group 2 FIB-4 12M ≥ 2.88 and △FIB-4 < 0 or FIB-4 12M < 2.88 and △FIB-4 ≥ 0; Group 3 FIB-4 12M ≥ 2.88 and △FIB-4 ≥ 0, Supplementary Methods: Details on multiple imputation.Author Contributions
Funding
Conflicts of Interest
References
- Perz, J.F.; Armstrong, G.L.; Farrington, L.A.; Hutin, Y.J.; Bell, B.P. The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. J. Hepatol. 2006, 45, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Chang, T.-T.; Liaw, Y.-F.; Wu, S.-S.; Schiff, E.; Han, K.-H.; Lai, C.; Safadi, R.; Lee, S.S.; Halota, W.; Goodman, Z.; et al. Long-term entecavir therapy results in the reversal of fibrosis/cirrhosis and continued histological improvement in patients with chronic hepatitis B. Hepatology 2010, 52, 886–893. [Google Scholar] [CrossRef] [PubMed]
- Hosaka, T.; Suzuki, F.; Kobayashi, M.; Seko, Y.; Kawamura, Y.; Sezaki, H.; Akuta, N.; Suzuki, Y.; Saitoh, S.; Arase, Y.; et al. Long-term entecavir treatment reduces hepatocellular carcinoma incidence in patients with hepatitis B virus infection. Hepatology 2013, 58, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Hou, J.; Zhao, W.; Lee, C.; Hann, H.-W.; Peng, C.-Y.; Tanwandee, T.; Morozov, V.; Klinker, H.; Sollano, J.D.; Streinu-Cercel, A.; et al. Outcomes of Long-term Treatment of Chronic HBV Infection with Entecavir or Other Agents From a Randomized Trial in 24 Countries. Clin. Gastroenterol. Hepatol. 2020, 18, 457–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiramatsu, N.; Yamada, R.; Takehara, T. The suppressive effect of nucleos(t)ide analogue treatment on the incidence of hepatocellular carcinoma in chronic hepatitis B patients. J. Gastroenterol. Hepatol. 2016, 31, 546–552. [Google Scholar] [CrossRef]
- Papatheodoridis, G.V.; Sypsa, V.; Dalekos, G.; Yurdaydin, C.; Van Boemmel, F.; Buti, M.; Goulis, J.; Calleja-Panero, J.L.; Chi, H.; Manolakopoulos, S.; et al. Eight-year survival in chronic hepatitis B patients under long-term entecavir or tenofovir therapy is similar to the general population. J. Hepatol. 2018, 68, 1129–1136. [Google Scholar] [CrossRef]
- Papatheodoridis, G.V.; Manolakopoulos, S.; Touloumi, G.; Vourli, G.; Raptopoulou-Gigi, M.; Vafiadis-Zoumbouli, I.; Vasileiadis, T.; Mimidis, K.; Gogos, C.; Ketikoglou, I.; et al. Virological suppression does not prevent the development of hepatocellular carcinoma in HBeAg-negative chronic hepatitis B patients with cirrhosis receiving oral antiviral(s) starting with lamivudine monotherapy: Results of the nationwide HEPNET. Greece cohort study. Gut 2011, 60, 1109–1116. [Google Scholar] [CrossRef]
- Arends, P.; Sonneveld, M.J.; Zoutendijk, R.; Carey, I.; Brown, A.; Fasano, M.; Mutimer, D.; Deterding, K.; Reijnders, J.G.P.; Oo, Y.H.; et al. Entecavir treatment does not eliminate the risk of hepatocellular carcinoma in chronic hepatitis B: Limited role for risk scores in Caucasians. Gut 2015, 64, 1289–1295. [Google Scholar] [CrossRef]
- Wang, H.-W.; Peng, C.-Y.; Lai, H.-C.; Su, W.-P.; Lin, C.-H.; Chuang, P.-H.; Chen, S.-H.; Chen, C.-H.; Hsu, W.-F.; Huang, G.-T. New noninvasive index for predicting liver fibrosis in Asian patients with chronic viral hepatitis. Sci. Rep. 2017, 7, 3259. [Google Scholar] [CrossRef] [Green Version]
- Martínez, S.M.; Crespo, G.; Navasa, M.; Forns, X. Noninvasive assessment of liver fibrosis. Hepatology 2011, 53, 325–335. [Google Scholar] [CrossRef]
- European Association for Study of the Liver, Asociacion Latinoamericana para el Estudio del H. EASL-ALEH Clinical Practice Guidelines: Non-invasive tests for evaluation of liver disease severity and prognosis. J. Hepatol. 2015, 63, 237–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, G.; Yang, J.; Yan, L. Comparison of diagnostic accuracy of aspartate aminotransferase to platelet ratio index and fibrosis-4 index for detecting liver fibrosis in adult patients with chronic hepatitis B virus infection: A systemic review and meta-analysis. Hepatology 2015, 61, 292–302. [Google Scholar] [CrossRef] [PubMed]
- Wai, C.T.; Greenson, J.K.; Fontana, R.J.; Kalbfleisch, J.D.; Marrero, J.A.; Conjeevaram, H.S.; Lok, A.S. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology 2003, 38, 518–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, M.S.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef]
- Nishikawa, H.; Nishijima, N.; Enomoto, H.; Sakamoto, A.; Nasu, A.; Komekado, H.; Nishimura, T.; Kita, R.; Kimura, T.; Iijima, H.; et al. Comparison of FIB-4 index and aspartate aminotransferase to platelet ratio index on carcinogenesis in chronic hepatitis B treated with entecavir. J. Cancer 2017, 8, 152–161. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.H.; Kim, J.W.; Seo, J.W.; Choe, W.H.; Kwon, S.Y. Noninvasive tests for fibrosis predict 5-year mortality and hepatocellular carcinoma in patients with chronic hepatitis B. J. Clin. Gastroenterol. 2016, 50, 882–888. [Google Scholar] [CrossRef]
- Kim, M.N.; Lee, J.H.; Chon, Y.E.; Ha, Y.; Hwang, S.G. Fibrosis-4, aspartate transaminase-to-platelet ratio index, and gamma-glutamyl transpeptidase-to-platelet ratio for risk assessment of hepatocellular carcinoma in chronic hepatitis B patients: Comparison with liver biopsy. Eur. J. Gastroenterol. Hepatol. 2020, 32, 433–439. [Google Scholar] [CrossRef]
- Tseng, T.C.; Liu, C.J.; Su, T.H.; Yang, W.T.; Chen, C.L.; Yang, H.C.; Wang, C.C.; Kuo, S.F.; Liu, C.H.; Chen, P.J.; et al. Fibrosis-4 index helps identify HBV carriers with the lowest risk of hepatocellular carcinoma. Am. J. Gastroenterol. 2017, 112, 1564–1574. [Google Scholar] [CrossRef]
- Papatheodoridis, G.; Dalekos, G.; Sypsa, V.; Yurdaydin, C.; Buti, M.; Goulis, J.; Calleja, J.L.; Chi, H.; Manolakopoulos, S.; Mangia, G.; et al. PAGE-B predicts the risk of developing hepatocellular carcinoma in Caucasians with chronic hepatitis B on 5-year antiviral therapy. J. Hepatol. 2016, 64, 800–806. [Google Scholar] [CrossRef]
- Papatheodoridis, G.V.; Idilman, R.; Dalekos, G.N.; Buti, M.; Chi, H.; van Boemmel, F.; Calleja, J.L.; Sypsa, V.; Goulis, J.; Manolakopoulos, S.; et al. The risk of hepatocellular carcinoma decreases after the first 5 years of entecavir or tenofovir in Caucasians with chronic hepatitis B. Hepatology. 2017, 66, 1444–1453. [Google Scholar] [CrossRef]
- Papatheodoridis, G.V.; Sypsa, V.; Dalekos, G.N.; Yurdaydin, C.; Van Boemmel, F.; Buti, M.; Calleja, J.L.; Chi, H.; Goulis, J.; Manolakopoulos, S.; et al. Hepatocellular carcinoma prediction beyond year 5 of oral therapy in a large cohort of Caucasian patients with chronic hepatitis B. J. Hepatol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.W.; Chan, S.L.; Mo, F.; Chan, T.C.; Loong, H.H.; Wong, G.L.; Lui, Y.Y.; Chan, A.T.; Sung, J.J.; Yeo, W.; et al. Clinical scoring system to predict hepatocellular carcinoma in chronic hepatitis B carriers. J. Clin. Oncol. 2010, 28, 1660–1665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, H.I.; Yuen, M.F.; Chan, H.L.; Han, K.H.; Chen, P.J.; Kim, D.Y.; Ahn, S.H.; Chen, C.J.; Wong, V.W.; Seto, W.K.; et al. Risk estimation for hepatocellular carcinoma in chronic hepatitis B (REACH-B): Development and validation of a predictive score. Lancet Oncol. 2011, 12, 568–574. [Google Scholar] [CrossRef]
- Chen, C.H.; Lee, C.M.; Lai, H.C.; Hu, T.H.; Su, W.P.; Lu, S.N.; Lin, C.H.; Hung, C.H.; Wang, J.H.; Lee, M.H.; et al. Prediction model of hepatocellular carcinoma risk in Asian patients with chronic hepatitis B treated with entecavir. Oncotarget 2017, 8, 92431–92441. [Google Scholar] [CrossRef] [Green Version]
- Hsu, Y.C.; Yip, T.C.; Ho, H.J.; Wong, V.W.; Huang, Y.T.; El-Serag, H.B.; Lee, T.Y.; Wu, M.S.; Lin, J.T.; Wong, G.L.; et al. Development of a scoring system to predict hepatocellular carcinoma in Asians on antivirals for chronic hepatitis B. J. Hepatol. 2018, 69, 278–285. [Google Scholar] [CrossRef]
- Yang, H.I.; Yeh, M.L.; Wong, G.L.; Peng, C.Y.; Chen, C.H.; Trinh, H.N.; Cheung, K.S.; Xie, Q.; Su, T.H.; Kozuka, R.; et al. REAL-B (Real-world Effectiveness from the Asia Pacific Rim Liver Consortium for HBV) risk score for the prediction of hepatocellular carcinoma in chronic hepatitis B patients treated with oral antiviral therapy. J. Infect. Dis. 2020, 221, 389–399. [Google Scholar] [CrossRef]
- Su, T.H.; Hu, T.H.; Chen, C.Y.; Huang, Y.H.; Chuang, W.L.; Lin, C.C.; Wang, C.C.; Su, W.W.; Chen, M.Y.; Peng, C.Y.; et al. Four-year entecavir therapy reduces hepatocellular carcinoma, cirrhotic events and mortality in chronic hepatitis B patients. Liver Int. 2016, 36, 1755–1764. [Google Scholar] [CrossRef]
- Papatheodoridis, G.V.; Dalekos, G.N.; Yurdaydin, C.; Buti, M.; Goulis, J.; Arends, P.; Sypsa, V.; Manolakopoulos, S.; Mangia, G.; Gatselis, N.; et al. Incidence and predictors of hepatocellular carcinoma in Caucasian chronic hepatitis B patients receiving entecavir or tenofovir. J. Hepatol. 2015, 62, 363–370. [Google Scholar] [CrossRef]
- Raffetti, E.; Fattovich, G.; Donato, F. Incidence of hepatocellular carcinoma in untreated subjects with chronic hepatitis B: A systematic review and meta-analysis. Liver Int. 2016, 36, 1239–1251. [Google Scholar] [CrossRef]
- Papatheodoridis, G.V.; Manolakopoulos, S.; Touloumi, G.; Nikolopoulou, G.; Raptopoulou-Gigi, M.; Gogos, C.; Vafiadis-Zouboulis, I.; Karamanolis, D.; Chouta, A.; Ilias, A.; et al. Hepatocellular carcinoma risk in HBeAg-negative chronic hepatitis B patients with or without cirrhosis treated with entecavir: HepNet.Greece cohort. J. Viral. Hepat. 2015, 22, 120–127. [Google Scholar] [CrossRef]
- Singh, S.; Muir, A.J.; Dieterich, D.T.; Falck-Ytter, Y.T. American Gastroenterological Association Institute technical review on the role of elastography in chronic liver diseases. Gastroenterology 2017, 152, 1544–1577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tada, T.; Kumada, T.; Toyoda, H.; Tsuji, K.; Hiraoka, A.; Tanaka, J. Impact of FIB-4 index on hepatocellular carcinoma incidence during nucleos(t)ide analogue therapy in patients with chronic hepatitis B: An analysis using time-dependent receiver operating characteristic. J. Gastroenterol. Hepatol. 2017, 32, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Chiang, H.H.; Lee, C.M.; Hu, T.H.; Hung, C.H.; Wang, J.H.; Lu, S.N.; Lai, H.C.; Su, W.P.; Lin, C.H.; Peng, C.Y.; et al. A combination of the on-treatment FIB-4 and alpha-foetoprotein predicts clinical outcomes in cirrhotic patients receiving entecavir. Liver Int. 2018, 38, 1997–2005. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, D.Y.; Sheen, I.S.; Chiu, C.T.; Lin, S.M.; Kuo, Y.C.; Liaw, Y.F. Ultrasonographic changes of early liver cirrhosis in chronic hepatitis B: A longitudinal study. J. Clin. Ultrasound 1993, 21, 303–308. [Google Scholar] [CrossRef]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2010, 33, S62–S69. [Google Scholar] [CrossRef] [Green Version]
- Rubin, D.B.; Schenker, N. Multiple imputation in health-care databases: An overview and some applications. Stat. Med. 1991, 10, 585–598. [Google Scholar] [CrossRef]
- Little, R.J.A.; Rubin, D.B. Statistical Analysis with Missing Data; Wiley: Hoboken, NJ, USA, 2002. [Google Scholar]
 Group 1, FIB-4 12M < 2.56 and △FIB-4 < 0; Group 2, FIB-4 12M < 2.56 and △FIB-4 ≥ 0; Group 3, FIB-4 12M ≥ 2.56 and △FIB-4 < 0; Group 4, FIB-4 12M ≥ 2.56 and △FIB-4 ≥ 0. (B) Noncirrhotic patients: Group 1, FIB-4 12M < 1.58 and △FIB-4 < 0; Group 2, FIB-4 12M ≥ 1.58 and △FIB-4 < 0 or FIB-4 12M < 1.58 and △FIB-4 ≥ 0; Group 3, FIB-4 12M ≥ 1.58 and △FIB-4 ≥ 0. (C) Cirrhotic patients: Group 1, FIB-4 12M < 2.88 and △FIB-4 < 0; Group 2 FIB-4 12M ≥ 2.88 and △FIB-4 < 0 or FIB-4 12M < 2.88 and △FIB-4 ≥ 0; Group 3 FIB-4 12M ≥ 2.88 and △FIB-4 ≥ 0. FIB-4—fibrosis index based on four factors; HCC—hepatocellular carcinoma; M—months.
Group 1, FIB-4 12M < 2.56 and △FIB-4 < 0; Group 2, FIB-4 12M < 2.56 and △FIB-4 ≥ 0; Group 3, FIB-4 12M ≥ 2.56 and △FIB-4 < 0; Group 4, FIB-4 12M ≥ 2.56 and △FIB-4 ≥ 0. (B) Noncirrhotic patients: Group 1, FIB-4 12M < 1.58 and △FIB-4 < 0; Group 2, FIB-4 12M ≥ 1.58 and △FIB-4 < 0 or FIB-4 12M < 1.58 and △FIB-4 ≥ 0; Group 3, FIB-4 12M ≥ 1.58 and △FIB-4 ≥ 0. (C) Cirrhotic patients: Group 1, FIB-4 12M < 2.88 and △FIB-4 < 0; Group 2 FIB-4 12M ≥ 2.88 and △FIB-4 < 0 or FIB-4 12M < 2.88 and △FIB-4 ≥ 0; Group 3 FIB-4 12M ≥ 2.88 and △FIB-4 ≥ 0. FIB-4—fibrosis index based on four factors; HCC—hepatocellular carcinoma; M—months.
Group 1, FIB-4 12M < 2.56 and △FIB-4 < 0; Group 2, FIB-4 12M < 2.56 and △FIB-4 ≥ 0; Group 3, FIB-4 12M ≥ 2.56 and △FIB-4 < 0; Group 4, FIB-4 12M ≥ 2.56 and △FIB-4 ≥ 0. (B) Noncirrhotic patients: Group 1, FIB-4 12M < 1.58 and △FIB-4 < 0; Group 2, FIB-4 12M ≥ 1.58 and △FIB-4 < 0 or FIB-4 12M < 1.58 and △FIB-4 ≥ 0; Group 3, FIB-4 12M ≥ 1.58 and △FIB-4 ≥ 0. (C) Cirrhotic patients: Group 1, FIB-4 12M < 2.88 and △FIB-4 < 0; Group 2 FIB-4 12M ≥ 2.88 and △FIB-4 < 0 or FIB-4 12M < 2.88 and △FIB-4 ≥ 0; Group 3 FIB-4 12M ≥ 2.88 and △FIB-4 ≥ 0. FIB-4—fibrosis index based on four factors; HCC—hepatocellular carcinoma; M—months.
Group 1, FIB-4 12M < 2.56 and △FIB-4 < 0; Group 2, FIB-4 12M < 2.56 and △FIB-4 ≥ 0; Group 3, FIB-4 12M ≥ 2.56 and △FIB-4 < 0; Group 4, FIB-4 12M ≥ 2.56 and △FIB-4 ≥ 0. (B) Noncirrhotic patients: Group 1, FIB-4 12M < 1.58 and △FIB-4 < 0; Group 2, FIB-4 12M ≥ 1.58 and △FIB-4 < 0 or FIB-4 12M < 1.58 and △FIB-4 ≥ 0; Group 3, FIB-4 12M ≥ 1.58 and △FIB-4 ≥ 0. (C) Cirrhotic patients: Group 1, FIB-4 12M < 2.88 and △FIB-4 < 0; Group 2 FIB-4 12M ≥ 2.88 and △FIB-4 < 0 or FIB-4 12M < 2.88 and △FIB-4 ≥ 0; Group 3 FIB-4 12M ≥ 2.88 and △FIB-4 ≥ 0. FIB-4—fibrosis index based on four factors; HCC—hepatocellular carcinoma; M—months.


{kind=link}
{kind=link}
{kind=link}
| Variables Median ± IQR or n (%) | Total n = 1325 | HCC Occurrence | p Value | |
|---|---|---|---|---|
| Yes (n =105) | No (n = 1220) | |||
| Age (years) | 50 ± 17 | 58 ± 14 | 49 ± 17 | <0.0001 |
| Sex (male) | 963 (72.7) | 79 (75.2) | 884 (72.5) | 0.5397 |
| HBeAg-positive status | 475 (35.8) | 29 (27.6) | 446 (36.6) | 0.0669 |
| Cirrhosis status | 481 (36.3) | 93 (88.6) | 388 (31.8) | <0.0001 |
| Diabetes mellitus (yes) | 158 (11.9) | 22 (21.0) | 136 (11.1) | 0.0029 |
| Albumin, g/dL | 4.11 ± 0.6 | 3.9 ± 0.7 | 4.2 ± 0.6 | <0.0001 |
| AST, U/L | 72 ± 115 | 60 ± 46 | 73 ± 123 | 0.0028 |
| ALT, U/L | 106 ± 207 | 64 ± 59 | 113 ± 220 | <0.0001 |
| Total bilirubin, mg/dL | 1 ± 0.78 | 1.1 ± 0.7 | 1 ± 0.8 | 0.5459 |
| INR | 1.08 ± 0.15 | 1.11 ± 0.17 | 1.07 ± 0.14 | 0.0090 |
| Platelets, ×103/μL | 163 ± 76 | 120 ± 70 | 167 ± 73.5 | <0.0001 |
| Histology grading | ||||
| F 1/2/3/4/NA | 57/84/30/122/1032 | 0/2/1/17/85 | 57/82/29/105/947 | |
| A 0/1/2/3/NA | 40/138/64/51/1032 | 3/11/2/4/85 | 37/127/62/47/947 | |
| AFP, ng/mL | 6.01 ± 10.31 | 8.25 ± 11.94 | 5.82 ± 10.18 | 0.0002 |
| AFP 12M, ng/mL | 3.41 ± 2.35 | 5.63 ± 4.63 | 3.28 ± 2.09 | <0.0001 |
| HBV DNA, log IU/mL | 5.96 ± 7.28 | 5.49 ± 6.46 | 6.04 ± 7.34 | <0.0001 |
| Time to VR (M) | 6.0 (6.3) | 6.0 (0) | 6.0 (6.4) | 0.9267 |
| VR 12M (yes) | 1160 (87.5) | 98 (93.3) | 1062 (87) | 0.0613 |
| APRI | 1.22 ± 2.1 | 1.43 ± 1.73 | 1.19 ± 2.13 | 0.1881 |
| APRI (≥0.90) | 855 (64.5) | 80 (76.2) | 775 (63.5) | 0.0092 |
| APRI 12M | 0.42 ± 0.37 | 1.04 ± 0.67 | 0.41 ± 0.31 | <0.0001 |
| APRI 12M (≥0.53) | 473 (35.7) | 92 (87.6) | 381 (31.2) | <0.0001 |
| △APRI (12M-0M) (≥0) | 136 (10.3) | 33 (31.4) | 103 (8.4) | <0.0001 |
| FIB-4 | 2.45 ± 2.69 | 4.09 ± 4.03 | 2.37 ± 2.51 | <0.0001 |
| FIB-4 (≥2.53) | 637 (48.1) | 82 (78.1) | 555 (45.5) | <0.0001 |
| FIB-4 12M | 1.64 ± 1.56 | 4.09 ± 3.22 | 1.55 ± 1.38 | <0.0001 |
| FIB-4 12M (≥2.56) | 342 (25.8) | 84 (80.0) | 258 (21.1) | <0.0001 |
| △FIB-4 (12M–0M) (≥0) | 323 (24.4) | 60 (57.1) | 263 (21.6) | <0.0001 |
| Treatment duration (year) | 4.09 (2.94) | 3.29 (2.32) | 4.11 (3.00) | <0.0001 |
| Follow-up period (year) | 4.09 (2.94) | 3.29 (2.32) | 4.11 (3.00) | <0.0001 |
| Variables Median ± IQR or n (%) | Univariate | |
|---|---|---|
| Hazard Ratio (95% CI) | p Value | |
| Age (year) | 1.056 (1.039–1.074) | <0.0001 |
| Sex, male vs. female | 1.103 (0.708–1.718) | 0.6653 |
| HBeAg, positive vs. negative | 0.717 (0.467–1.100) | 0.1272 |
| Cirrhosis status, yes vs. no | 11.29 (6.180–20.63) | <0.0001 |
| Diabetes mellitus, yes vs. no | 2.280 (1.424–3.650) | 0.0006 |
| Albumin, g/dL | 0.406 (0.294–0.559) | <0.0001 |
| AST, U/L | 0.998 (0.997–1.000) | 0.0117 |
| ALT, U/L | 0.998 (0.996–0.999) | 0.0006 |
| Total bilirubin, mg/dL | 0.929 (0.829–1.042) | 0.2087 |
| INR | 1.618 (0.866–3.021) | 0.1311 |
| Platelets, ×103/μL | 0.985 (0.982–0.989) | <0.0001 |
| AFP, ng/mL | 0.999 (0.996–1.001) | 0.3951 |
| AFP 12M, ng/mL | 1.005 (1.002–1.007) | <0.0001 |
| HBV DNA, log IU/mL | 1.000 (1.000–1.000) | 0.1854 |
| VR 12M, yes vs. no | 1.931 (0.897–4.159) | 0.0925 |
| APRI, ≥0.90 vs. <0.90 | 1.991 (1.270–3.121) | 0.0027 |
| APRI 12M, ≥0.53 vs. <0.53 | 11.79 (6.596–21.09) | <0.0001 |
| △APRI (12M-0M), ≥0 vs. <0 | 3.845 (2.546–5.807) | <0.0001 |
| FIB-4, ≥2.53 vs. <2.53 | 3.919 (2.467–6.223) | <0.0001 |
| FIB-4 12M, ≥2.56 vs. <2.56 | 11.31 (7.009–18.25) | <0.0001 |
| △FIB-4 (12M–0M), ≥0 vs. <0 | 3.953 (2.685–5.819) | <0.0001 |
| Risk Factors | Multivariate | |
|---|---|---|
| Hazard Ratio (95% CI) | p Value | |
| All patients (n = 1325) | ||
| Diabetes mellitus, yes vs. no | 1.726 (1.076–2.770) | 0.0235 |
| AFP 12M, ng/mL | 1.005 (1.003–1.008) | <0.0001 |
| FIB-4 12M, ≥2.56 vs. <2.56 | 9.198 (5.610–15.08) | <0.0001 |
| △FIB-4 (12M-0M), ≥0 vs. <0 | 2.353 (1.585–3.495) | <0.0001 |
| Noncirrhotic patients (n = 844) | ||
| FIB-4 12M, ≥1.58 vs. <1.58 | 12.10 (1.531–95.60) | 0.0181 |
| △FIB-4 (12M-0M), ≥0 vs. <0 | 7.013 (1.874–26.24) | 0.0038 |
| Cirrhotic patients (n = 481) | ||
| Sex, male vs. female | 1.758 (1.082–2.856) | 0.0226 |
| Diabetes mellitus, yes | 1.665 (1.006–2.756) | 0.0472 |
| AFP 12M, ng/mL | 1.008 (1.005–1.012) | <0.0001 |
| FIB-4 12M, ≥2.88 vs. <2.88 | 4.821 (2.908–7.992) | <0.0001 |
| △FIB-4 (12M-0M), ≥0 vs. <0 | 1.981 (1.301–3.016) | 0.0014 |
| Variables Median ± IQR or n (%) | △FIB-4 < 0 n = 1002 | △FIB-4 ≥ 0 n = 323 | p Value |
|---|---|---|---|
| Baseline | |||
| Age (years) | 49 ± 17 | 51 ± 16 | 0.002 |
| Sex (male) | 727 (72.6) | 236 (73.1) | 0.719 |
| HBeAg-positive status (yes) | 367 (36.6) | 108 (33.4) | 0.298 |
| Diabetes mellitus (yes) | 120 (11.9) | 38 (11.8) | 0.919 |
| Cirrhosis (yes) | 328 (32.7) | 153 (47.4) | <0.001 |
| HCC | 45 (4.5) | 60 (18.6) | <0.001 |
| Albumin, g/dL | 4.1 ± 0.6 | 4.2 ± 0.5 | 0.163 |
| AST, U/L | 92 ± 187 | 46 ± 26 | <0.001 |
| ALT, U/L | 137 ± 316 | 60 ± 50 | <0.001 |
| Total bilirubin, mg/dL | 1.1 ± 1.0 | 0.9 ± 0.6 | <0.001 |
| INR | 1.09 ± 0.16 | 1.06 ± 0.13 | <0.001 |
| Platelets, ×103/μL | 162 ± 75 | 166 ± 83 | 0.297 |
| AFP, ng/mL | 6.53 ± 13.3 | 4.87 ± 5.25 | <0.001 |
| HBV DNA, log IU/mL | 6.19 ± 7.43 | 5.36 ± 6.54 | <0.001 |
| FIB-4 | 2.69 ± 3.00 | 1.73 ± 1.72 | <0.001 |
| One-year treatment | |||
| AST 12M, U/L | 26 ± 11 | 31 ± 16 | <0.001 |
| ALT 12M, U/L | 26 ± 16 | 29 ± 18 | <0.001 |
| Platelets 12M, ×103/μL | 171 ± 77 | 141 ± 81 | <0.001 |
| AFP 12M, ng/mL | 3.33 ± 2.25 | 3.69 ± 2.97 | 0.009 |
| VR 12M (yes) | 871 (86.9) | 289 (89.5) | 0.228 |
| FIB-4 12M | 1.53 ± 1.36 | 2.11 ± 2.34 | <0.001 |
| Combined risk factors | Crude HR | 95% CI | p Value |
|---|---|---|---|
| All patients (n = 1325) | |||
| FIB-4 12M < 2.56 and △FIB-4 < 0 (n = 795) | 1 | ||
| FIB-4 12M < 2.56 and △FIB-4 ≥ 0 (n = 188) | 3.673 | 1.560–8.649 | 0.0029 |
| FIB-4 12M ≥ 2.56 and △FIB-4 < 0 (n = 207) | 11.74 | 5.948–23.18 | <0.0001 |
| FIB-4 12M ≥ 2.56 and △FIB-4 ≥ 0 (n = 135) | 25.58 | 13.31–49.15 | <0.0001 |
| Noncirrhotic patients (n = 844) | |||
| FIB-4 12M < 1.58 and △FIB-4 < 0 (n = 459) | 1 | ||
| FIB-4 12M ≥ 1.58 and △FIB-4 < 0 or FIB-4 12M < 1.58 and △FIB-4 ≥ 0 (n = 297) | 3.076 | 0.279–33.93 | 0.3589 |
| FIB-4 12M ≥ 1.58 and △FIB-4 ≥ 0 (n = 88) | 40.35 | 5.107–318.7 | <0.0001 |
| Cirrhotic patients (n = 481) | |||
| FIB-4 12M < 2.88 and △FIB-4 < 0 (n = 203) | 1 | ||
| FIB-4 12M ≥ 2.88 and △FIB-4 < 0 or FIB-4 12M < 2.88 and △FIB-4 ≥ 0 (n = 189) | 3.625 | 1.897–6.927 | <0.0001 |
| FIB-4 12M ≥ 2.88 and △FIB-4 ≥ 0 (n = 89) | 9.576 | 5.033–18.22 | <0.0001 |
| Risk Scores | PAGE-B | REACH-B | CU-HCC | APA-B | FIB-4-Based Model |
|---|---|---|---|---|---|
| AUROC (95% CI) | AUROC (95% CI) | AUROC (95% CI) | AUROC (95% CI) | AUROC (95% CI) | |
| 2 years | 0.7379 (0.6526–0.8233) | 0.6673 (0.5801–0.7545) | 0.7666 (0.7033–0.8298) | 0.8815 (0.8236–0.9395) | 0.8192 (0.7482–0.8902) |
| 3 years | 0.7415 (0.6741–0.8089) | 0.6640 (0.5950–0.7329) | 0.7771 (0.7210–0.8333) | 0.8820 (0.8393–0.9247) | 0.8359 (0.7858–0.8860) |
| 4 years | 0.7665 (0.7163–0.8167) | 0.6679 (0.6112–0.7246) | 0.7857 (0.7433–0.8280) | 0.8910 (0.8591–0.9229) | 0.8701 (0.8341–0.9060) |
| 5 years | 0.7471 (0.6980–0.7962) | 0.6535 (0.5992–0.7078) | 0.7809 (0.7394–0.8225) | 0.8775 (0.8450–0.9100) | 0.8659 (0.8321–0.8997) |
| C-statistic | 0.7394 (0.6920–0.7868) | 0.6551 (0.6033–0.7069) | 0.7755 (0.7366–0.8145) | 0.8825 (0.8532–0.9118) | 0.8736 (0.8434–0.9038) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, H.-W.; Lai, H.-C.; Hu, T.-H.; Su, W.-P.; Lu, S.-N.; Lin, C.-H.; Hung, C.-H.; Chuang, P.-H.; Wang, J.-H.; Lee, M.-H.; et al. On-Treatment Changes in FIB-4 and 1-Year FIB-4 Values Help Identify Patients with Chronic Hepatitis B Receiving Entecavir Therapy Who Have the Lowest Risk of Hepatocellular Carcinoma. Cancers 2020, 12, 1177. https://doi.org/10.3390/cancers12051177
Wang H-W, Lai H-C, Hu T-H, Su W-P, Lu S-N, Lin C-H, Hung C-H, Chuang P-H, Wang J-H, Lee M-H, et al. On-Treatment Changes in FIB-4 and 1-Year FIB-4 Values Help Identify Patients with Chronic Hepatitis B Receiving Entecavir Therapy Who Have the Lowest Risk of Hepatocellular Carcinoma. Cancers. 2020; 12(5):1177. https://doi.org/10.3390/cancers12051177
Chicago/Turabian StyleWang, Hung-Wei, Hsueh-Chou Lai, Tsung-Hui Hu, Wen-Pang Su, Sheng-Nan Lu, Chia-Hsin Lin, Chao-Hung Hung, Po-Heng Chuang, Jing-Houng Wang, Mei-Hsuan Lee, and et al. 2020. "On-Treatment Changes in FIB-4 and 1-Year FIB-4 Values Help Identify Patients with Chronic Hepatitis B Receiving Entecavir Therapy Who Have the Lowest Risk of Hepatocellular Carcinoma" Cancers 12, no. 5: 1177. https://doi.org/10.3390/cancers12051177