
Relationship between Peak Inspiratory Flow and Patient and Disease Characteristics in Individuals with COPD—A Systematic Scoping Review

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population of Interest
2.2. Information Source
2.3. Eligibility Criteria
2.4. Data Charting and Quality Assessment
2.5. Statistical Analysis
3. Results
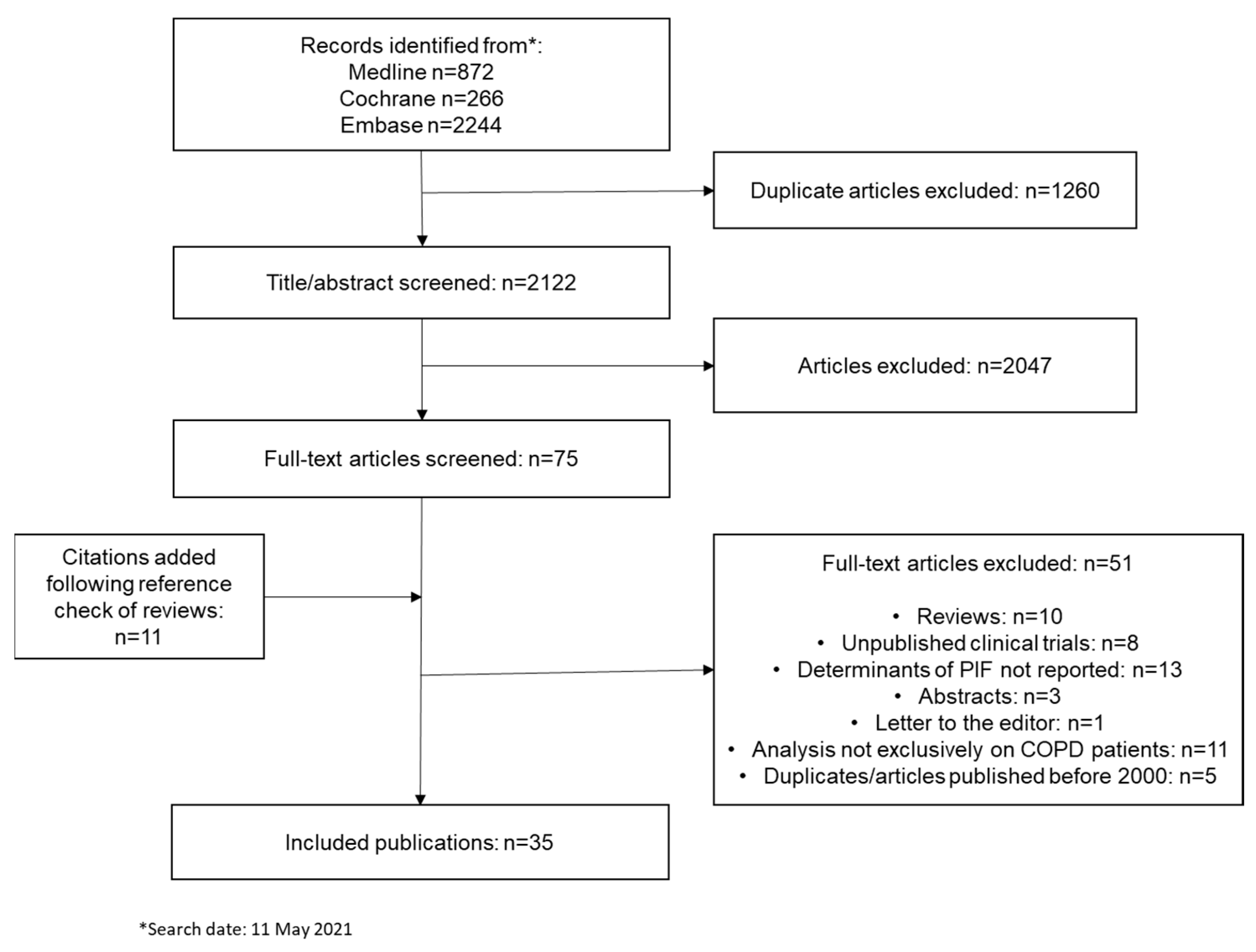
3.1. Selection of Papers
3.2. Quality Assessment of Papers
3.3. Definition and Measurement of PIF
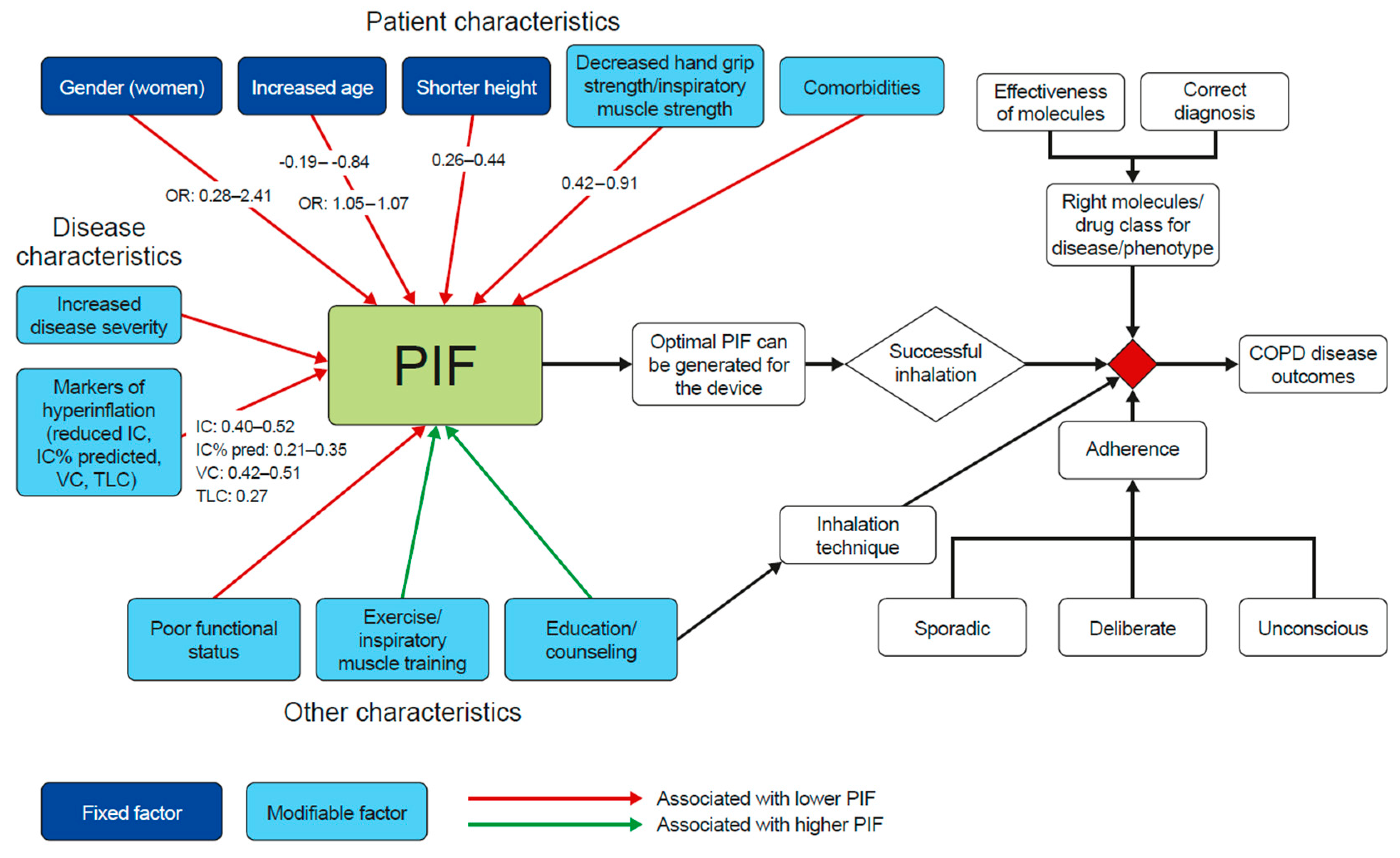
3.4. Association of PIF with Patient or Disease Characteristics

3.4.1. Patient Characteristics
3.4.2. Disease Characteristics
3.4.3. Other Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease 2021 Report; Global Initiative for Chronic Obstructive Lung Disease, 2021; Available online: https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20_WMV.pdf (accessed on 14 April 2021).
- Tsiligianni, I.; Kocks, J.W.H. Daytime symptoms of chronic obstructive pulmonary disease: A systematic review. NPJ Prim. Care Respir. Med. 2020, 30, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahler, D.A. Peak Inspiratory Flow Rate as a Criterion for Dry Powder Inhaler Use in Chronic Obstructive Pulmonary Disease. Ann. Am. Thorac. Soc. 2017, 14, 1103–1107. [Google Scholar] [CrossRef] [PubMed]
- Lavorini, F.; Corrigan, C.; Barnes, P.; Dekhuijzen, P.; Levy, M.; Pedersen, S.; Roche, N.; Vincken, W.; Crompton, G. Retail sales of inhalation devices in European countries: So much for a global policy. Respir. Med. 2011, 105, 1099–1103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panigone, S.; Sandri, F.; Ferri, R.; Volpato, A.; Nudo, E.; Nicolini, G. Environmental impact of inhalers for respiratory diseases: Decreasing the carbon footprint while preserving patient-tailored treatment. BMJ Open Respir. Res. 2020, 7, e000571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- British Thoracic Society. Position Statement: Environment and Lung Health 2020; British Thoracic Society: London, UK, 2020; Available online: https://www.brit-thoracic.org.uk/document-library/governance-and-policy-documents/position-statements/environment-and-lung-health-position-statement-2020/ (accessed on 30 November 2021).
- Mahler, D.A. The role of inspiratory flow in selection and use of inhaled therapy for patients with chronic obstructive pulmonary disease. Respir. Med. 2020, 161, 105857. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.; Ohar, J.A.; Drummond, M.B. Peak Inspiratory Flow Rate in Chronic Obstructive Pulmonary Disease: Implications for Dry Powder Inhalers. J. Aerosol Med. Pulm. Drug Deliv. 2017, 30, 381–387. [Google Scholar] [CrossRef]
- Lavorini, F.; Pistolesi, M.; Usmani, O.S. Recent advances in capsule-based dry powder inhaler technology. Multidiscip. Respir. Med. 2017, 12, 11. [Google Scholar] [CrossRef]
- Price, D.B.; Roman-Rodriguez, M.; McQueen, R.B.; Bosnic-Anticevich, S.; Carter, V.; Gruffydd-Jones, K.; Haughney, J.; Henrichsen, S.; Hutton, C.; Infantino, A.; et al. Inhaler Errors in the CRITIKAL Study: Type, Frequency, and Association with Asthma Outcomes. J. Allergy Clin. Immunol. Pract. 2017, 5, 1071–1081.e1079. [Google Scholar] [CrossRef]
- Loh, C.H.; Peters, S.P.; Lovings, T.M.; Ohar, J.A. Suboptimal Inspiratory Flow Rates Are Associated with Chronic Obstructive Pulmonary Disease and All-Cause Readmissions. Ann. Am. Thorac. Soc. 2017, 14, 1305–1311. [Google Scholar] [CrossRef]
- Loh, C.H.; Ohar, J.A. Personalization of Device Therapy—Prime Time for Peak Inspiratory Flow Rate. Chronic Obstr. Pulm. Dis. J. COPD Found. 2017, 4, 172–176. [Google Scholar] [CrossRef] [Green Version]
- Price, D.B.; Yang, S.; Ming, S.W.Y.; Hardjojo, A.; Cabrera, C.; Papaioannou, A.I.; Loukides, S.; Kritikos, V.; Bosnic-Anticevich, S.Z.; Carter, V.; et al. Physiological predictors Of peak inspiRatory flow using Observed lung function resultS (POROS): Evaluation at discharge among patients hospitalized for a COPD exacerbation. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 3937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnes, C.N.; Mahler, D.A.; Ohar, J.A.; Lombardi, D.A.; Crater, G.D. Peak Inspiratory Flows: Defining Repeatability Limits and a Predictive Equation for Different Inhalers. Chest 2020, 158, 1413–1419. [Google Scholar] [CrossRef] [PubMed]
- Ohar, J.A.; Ferguson, G.T.; Mahler, D.A.; Drummond, M.B.; Dhand, R.; Pleasants, R.A.; Anzueto, A.; Halpin, D.M.; Price, D.B.; Drescher, G.S.; et al. Measuring peak inspiratory flow in patients with chronic obstructive pulmonary disease. Int. J. Chronic Obstr. Pulm. Dis. 2022, 17, 79–92. [Google Scholar] [CrossRef] [PubMed]
- Duarte, A.G.; Tung, L.; Zhang, W.; Hsu, E.S.; Kuo, Y.F.; Sharma, G. Spirometry Measurement of Peak Inspiratory Flow Identifies Suboptimal Use of Dry Powder Inhalers in Ambulatory Patients with COPD. Chronic Obstr. Pulm. Dis. J. COPD Found. 2019, 6, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Malmberg, L.P.; Rytila, P.; Happonen, P.; Haahtela, T. Inspiratory flows through dry powder inhaler in chronic obstructive pulmonary disease: Age and gender rather than severity matters. Int. J. Chronic Obstr. Pulm. Dis. 2010, 5, 257–262. [Google Scholar] [CrossRef] [Green Version]
- Ghosh, S.; Pleasants, R.A.; Ohar, J.A.; Donohue, J.F.; Drummond, M.B. Prevalence and factors associated with suboptimal peak inspiratory flow rates in COPD. Int. J. Chronic Obstr. Pulm. Dis. 2019, 14, 585–595. [Google Scholar] [CrossRef] [Green Version]
- Harb, H.S.; Laz, N.I.; Rabea, H.; Abdelrahim, M.E.A. Prevalence and predictors of suboptimal peak inspiratory flow rate in COPD patients. Eur. J. Pharm. Sci. 2020, 147, 105298. [Google Scholar] [CrossRef]
- Price, D.; Keininger, D.L.; Viswanad, B.; Gasser, M.; Walda, S.; Gutzwiller, F.S. Factors associated with appropriate inhaler use in patients with COPD—Lessons from the REAL survey. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 695–702. [Google Scholar] [CrossRef]
- Samarghandi, A.; Ioachimescu, O.C.; Qayyum, R. Association between peak inspiratory flow rate and hand grip muscle strength in hospitalized patients with acute exacerbation of chronic obstructive pulmonary disease. PLoS ONE 2020, 15, e0227737. [Google Scholar] [CrossRef]
- Mahler, D.A.; Waterman, L.A.; Gifford, A.H. Prevalence and COPD phenotype for a suboptimal peak inspiratory flow rate against the simulated resistance of the Diskus® dry powder inhaler. J. Aerosol Med. Pulm. Drug Deliv. 2013, 26, 174–179. [Google Scholar] [CrossRef]
- Agarwal, D.; Hanafi, N.S.; Chippagiri, S.; Brakema, E.A.; Pinnock, H.; Khoo, E.M.; Sheikh, A.; Liew, S.M.; Ng, C.W.; Isaac, R.; et al. Systematic scoping review protocol of methodologies of chronic respiratory disease surveys in low/middle-income countries. NPJ Prim. Care Respir. Med. 2019, 29, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.Y.; Huang, C.K.; Peng, H.C.; Yu, C.J.; Chien, J.Y. Inappropriate Peak Inspiratory Flow Rate with Dry Powder Inhaler in Chronic Obstructive Pulmonary Disease. Sci. Rep. 2020, 10, 7271. [Google Scholar] [CrossRef] [PubMed]
- Weiner, P.; Weiner, M. Inspiratory muscle training may increase peak inspiratory flow in chronic obstructive pulmonary disease. Respiration 2006, 73, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Terzano, C.; Oriolo, F. Lung characteristics in elderly males and females patients with COPD: Differences and optimal use of dry powder inhalers (DPIs). Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 2708–2716. [Google Scholar]
- Janssens, W.; VandenBrande, P.; Hardeman, E.; De Langhe, E.; Philps, T.; Troosters, T.; Decramer, M. Inspiratory flow rates at different levels of resistance in elderly COPD patients. Eur. Respir. J. 2008, 31, 78–83. [Google Scholar] [CrossRef]
- Papaioannou, A.I.; Herodotou, Y.; Tomos, I.; Apollonatou, V.; Verykokou, G.; Papathanasiou, E.; Manali, E.D.; Loukides, S.; Papiris, S.A. Ability of using different dry powder inhalers during COPD exacerbations. Pulm. Pharmacol. Ther. 2018, 48, 211–216. [Google Scholar] [CrossRef]
- Jarvis, S.; Ind, P.W.; Shiner, R.J. Inhaled therapy in elderly COPD patients; time for re-evaluation? Age Ageing 2007, 36, 213–218. [Google Scholar] [CrossRef] [Green Version]
- Azouz, W.; Chetcuti, P.; Hosker, H.; Saralaya, D.; Chrystyn, H. Inhalation characteristics of asthma patients, COPD patients and healthy volunteers with the Spiromax® and Turbuhaler® devices: A randomised, cross-over study. BMC Pulm. Med. 2015, 15, 47. [Google Scholar] [CrossRef] [Green Version]
- Davidson, H.E.; Radlowski, P.; Han, L.; Shireman, T.I.; Dembek, C.; Niu, X.; Gravenstein, S. Clinical Characterization of Nursing Facility Residents With Chronic Obstructive Pulmonary Disease. Sr. Care Pharm. 2021, 36, 248–257. [Google Scholar] [CrossRef]
- Al-Showair, R.A.; Tarsin, W.Y.; Assi, K.H.; Pearson, S.B.; Chrystyn, H. Can all patients with COPD use the correct inhalation flow with all inhalers and does training help? Respir. Med. 2007, 101, 2395–2401. [Google Scholar] [CrossRef] [Green Version]
- Represas-Represas, C.; Aballe-Santos, L.; Fernandez-Garcia, A.; Priegue-Carrera, A.; Lopez-Campos, J.L.; Gonzalez-Montaos, A.; Botana-Rial, M.; Fernandez-Villar, A. Evaluation of Suboptimal Peak Inspiratory Flow in Patients with Stable COPD. J. Clin. Med. 2020, 9, 3949. [Google Scholar] [CrossRef]
- Sharma, G.; Mahler, D.A.; Mayorga, V.M.; Deering, K.L.; Harshaw, O.; Ganapathy, V. Prevalence of Low Peak Inspiratory Flow Rate at Discharge in Patients Hospitalized for COPD Exacerbation. Chronic Obstr. Pulm. Dis. J. COPD Found. 2017, 4, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Farkas, A.; Szipocs, A.; Horvath, A.; Horvath, I.; Galffy, G.; Varga, J.; Galambos, K.; Kugler, S.; Nagy, A.; Szalai, Z. Establishment of relationships between native and inhalation device specific spirometric parameters as a step towards patient tailored inhalation device selection. Respir. Med. 2019, 154, 133–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chua, J.R.; Albay, A.B., Jr.; Tee, M.L. Body Composition of Filipino Chronic Obstructive Pulmonary Disease (COPD) Patients in Relation to Their Lung Function, Exercise Capacity and Quality of Life. Int. J. Chronic Obstr. Pulm. Dis. 2019, 14, 2759–2765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Visser, F.J.; Ramlal, S.; Dekhuijzen, P.N.; Heijdra, Y.F. Pursed-lips breathing improves inspiratory capacity in chronic obstructive pulmonary disease. Respiration 2011, 81, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Tout, R.; Tayara, L.; Halimi, M. The effects of respiratory muscle training on improvement of the internal and external thoraco-pulmonary respiratory mechanism in COPD patients. Ann. Phys. Rehabil. Med. 2013, 56, 193–211. [Google Scholar] [CrossRef] [Green Version]
- Magnussen, H.; Watz, H.; Zimmermann, I.; Macht, S.; Greguletz, R.; Falques, M.; Jarreta, D.; Garcia Gil, E. Peak inspiratory flow through the Genuair® inhaler in patients with moderate or severe COPD. Respir. Med. 2009, 103, 1832–1837. [Google Scholar] [CrossRef] [Green Version]
- Chodosh, S.; Flanders, J.S.; Kesten, S.; Serby, C.W.; Hochrainer, D.; Witek, T.J., Jr. Effective delivery of particles with the HandiHaler® dry powder inhalation system over a range of chronic obstructive pulmonary disease severity. J. Aerosol Med. 2001, 14, 309–315. [Google Scholar] [CrossRef]
- Stanescu, D.; Veriter, C.; Van de Woestijne, K.P. Maximal inspiratory flow rates in patients with COPD. Chest 2000, 118, 976–980. [Google Scholar] [CrossRef] [Green Version]
- Anderson, M.; Collison, K.; Drummond, M.B.; Hamilton, M.; Jain, R.; Martin, N.; Mularski, R.A.; Thomas, M.; Zhu, C.Q.; Ferguson, G.T. Peak Inspiratory Flow Rate in COPD: An Analysis of Clinical Trial and Real-World Data. Int. J. Chronic Obstr. Pulm. Dis. 2021, 16, 933–943. [Google Scholar] [CrossRef]
- Malmberg, L.P.; Pelkonen, A.S.; Vartiainen, V.; Vahteristo, M.; Lahelma, S.; Jogi, R. Patients with asthma or chronic obstructive pulmonary disease (COPD) can generate sufficient inspiratory flows via Easyhaler® dry powder inhaler: A pooled analysis of two randomized controlled trials. J. Thorac. Dis. 2021, 13, 621–631. [Google Scholar] [CrossRef]
- Erdelyi, T.; Lazar, Z.; Odler, B.; Tamasi, L.; Muller, V. The Repeatability of Inspiration Performance Through Different Inhalers in Patients with Chronic Obstructive Pulmonary Disease and Control Volunteers. J. Aerosol Med. Pulm. Drug Deliv. 2020, 33, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Jogi, R.; Lahelma, S.; Vahteristo, M.; Happonen, A.; Haikarainen, J. In Vitro Flow Rate Dependency of Delivered Dose and Fine Particle Dose of Salmeterol/Fluticasone Propionate Easyhaler and Seretide Diskus with Patient Flow Rates Collected in a Randomized Controlled Trial. J. Aerosol Med. Pulm. Drug Deliv. 2019, 32, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Altman, P.; Wehbe, L.; Dederichs, J.; Guerin, T.; Ament, B.; Moronta, M.C.; Pino, A.V.; Goyal, P. Comparison of peak inspiratory flow rate via the Breezhaler®, Ellipta® and HandiHaler® dry powder inhalers in patients with moderate to very severe COPD: A randomized cross-over trial. BMC Pulm. Med. 2018, 18, 100. [Google Scholar] [CrossRef] [PubMed]
- Prime, D.; de Backer, W.; Hamilton, M.; Cahn, A.; Preece, A.; Kelleher, D.; Baines, A.; Moore, A.; Brealey, N.; Moynihan, J. Effect of Disease Severity in Asthma and Chronic Obstructive Pulmonary Disease on Inhaler-Specific Inhalation Profiles Through the ELLIPTA® Dry Powder Inhaler. J. Aerosol Med. Pulm. Drug Deliv. 2015, 28, 486–497. [Google Scholar] [CrossRef] [Green Version]
- Canonica, G.W.; Arp, J.; Keegstra, J.R.; Chrystyn, H. Spiromax, a New Dry Powder Inhaler: Dose Consistency under Simulated Real-World Conditions. J. Aerosol Med. Pulm. Drug Deliv. 2015, 28, 309–319. [Google Scholar] [CrossRef] [Green Version]
- Broeders, M.E.; Molema, J.; Hop, W.C.; Folgering, H.T. Inhalation profiles in asthmatics and COPD patients: Reproducibility and effect of instruction. J. Aerosol Med. 2003, 16, 131–141. [Google Scholar] [CrossRef]
- Nsour, W.M.; Alldred, A.; Corrado, J.; Chrystyn, H. Measurement of peak inhalation rates with an In-Check Meter® to identify an elderly patient’s ability to use a Turbuhaler®. Respir. Med. 2001, 95, 965–968. [Google Scholar] [CrossRef] [Green Version]
- Chen, R.; Chen, R.; Chen, X.; Chen, L. Effect of endurance training on expiratory flow limitation and dynamic hyperinflation in patients with stable chronic obstructive pulmonary disease. Intern. Med. J. 2014, 44, 791–800. [Google Scholar] [CrossRef]
- Quanjer, P.; Tammeling, G.; Cotes, J.; Pedersen, O.; Perlin, R.; Yernault, J. Lung volumes and forced ventilatory flows. Report working party. Standardization of lung function test European Community for steel and oral official statement of the European Respiratory Society. Eur. Respir. J. 1993, 6, 40. [Google Scholar]
- Rau, J.L. Practical problems with aerosol therapy in COPD. Respir. Care 2006, 51, 158–172. [Google Scholar] [PubMed]
- Lavorini, F.; Mannini, C.; Chellini, E.; Fontana, G.A. Optimising Inhaled Pharmacotherapy for Elderly Patients with Chronic Obstructive Pulmonary Disease: The Importance of Delivery Devices. Drugs Aging 2016, 33, 461–473. [Google Scholar] [CrossRef] [PubMed]
- Ciciliani, A.M.; Langguth, P.; Wachtel, H. Handling forces for the use of different inhaler devices. Int. J. Pharm. 2019, 560, 315–321. [Google Scholar] [CrossRef]
- Leving, M.; Wouters, H.; de la Hoz, A.; Bosnic-Anticevich, S.; Dekhuijzen, R.; Gardev, A.; Lavorini, F.; Meijer, J.; Price, D.; Rodriguez, M.R.; et al. Impact of PIF, Inhalation Technique and Medication Adherence on Health Status and Exacerbations in COPD: Protocol of a Real-World Observational Study (PIFotal COPD Study). Pulm. Ther. 2021, 7, 591–606. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Papers Evaluating Characteristic, n/Total Papers included in Review | Papers Supporting an Association between Characteristic and PIF, n/Total for Characteristic (% of Total for Characteristic) | Nature of Association Where Correlation is Observed | Papers not Supporting an Association Between Characteristic and PIF, n/Total for Characteristic (% of Total for Characteristic) | |
|---|---|---|---|---|
| Patient Characteristic | ||||
| Age | 17/35 | 12/17 (71%) [11,17,21,22,25,28,30,32,34,35,44,47]  | Age ↑; PIF ↓ 1 (r ranging from −0.19 to −0.84; odds ratio ranging from 1.05 to 1.07) | 5/17 (29%) [18,19,29,36,46]  |
| Gender | 14/35 | 10/14 (71%) [16,17,18,19,22,26,32,35,36,47]  | Female gender; PIF ↓ 2 (odds ratio ranging from 0.28 to 2.41) | 4/14 (29%) [11,21,29,34]  |
| Height | 11/35 | 8/11 (73%) [16,17,18,19,22,28,32,44]  | Height ↓; PIF ↓ 3 (r ranging from 0.26 to 0.44) | 3/11 (27%) [11,25,35]  |
| Body weight/body mass index/body composition | 12/35 | 2/12 (17%) [17,37]  | Body weight ↓; PIF ↓ [17] 4 (r 0.22) Fat-free mass ↓ [37]; PIF ↓ (rpb −0.58) | 10/12 (83%) [11,18,19,22,28,29,32,34,36,44]  |
| Handgrip strength/inspiratory muscle strength | 4/35 | 4/4 (100%) [21,26,27,28]  | Handgrip strength ↓; PIF ↓ [21] (effect size in adjusted model: 0.49 [95% CI 0.08, 0.90]) Maximal inspiratory mouth pressure (a measure of inspiratory muscle strength) ↓; PIF ↓ [26,27,28] 5 (r ranging from 0.42 to 0.91) | 0/4 (0%) |
| Comorbidities | 4/35 | 3/4 (75%) [21,32,35]  Note: While these papers each include a correlation between PIF and at least one comorbidity, they also contain data showing no correlation between PIF and other comorbidities | Asthma [21]; anemia and coronary artery disease [32]; pneumonia and ischemic heart disease [35]; PIF ↓ | 1/4 (25%) [11]  |
| Smoking status | 5/35 | 1/5 (20%) [35]  | Current smoker; PIF ↓ (Odds ratio: 2.06) | 4/5 (80%) [21,29,34,36]  |
| Ethnicity | 3/35 | 0/3 (0%) | N/A | 3/3 (100%) [11,21,32]  |
| Disease characteristics | ||||
| IC | 2/35 | 2/2 (100%) [16,27]  | IC ↓; PIF ↓ (r ranging from 0.40 to 0.52) | 0/2 (0%) |
| IC% pred. | 4/35 | 3/4 (75%) [11,16,22]  | IC% pred ↓; PIF ↓ (r ranging from 0.21 to 0.35) | 1/4 (25%) [27]  |
| FEV1 | 14/35 | 9/14 (64%) [16,17,19,25,32,34,36,44,48] 6  | FEV1 ↓; PIF ↓ (r ranging from 0.29 to 0.73) | 5/14 (35%) [18,28,29,35,41]  |
| FEV1% pred. | 16/35 | 3/16 (19%) [30,32,44]  | FEV1 % pred ↓; PIF ↓ (r ranging from 0.22 to 0.68) | 13/16 (81%) [11,16,17,19,22,27,28,29,34,35,36,41,43]  |
| FVC | 10/35 | 7/10 (70%) [16,25,28,32,34,36,44] 6,7  | FVC ↓; PIF ↓ [16,25,28,32,36,44] 6,7 (r ranging from 0.29 to 0.48; odds ratio: 0.961) [34] | 3/10 (30%) [18,19,35]  |
| FVC% pred. | 11/35 | 3/11 (27%) [16,22,34]  | % pred FVC ↓; PIF ↓ (r 0.37) | 8/11 (73%) [11,19,27,28,29,35,36,44]  |
| PEF | 5/35 | 5/5 (100%) [17,19,28,44,48]  | PEF ↓; PIF ↓ (r ranging from 0.32 to 0.80) | 0/5 (0%) |
| PEF% pred. | 2/35 | 0/2 (0%) | N/A | 2/2 (100%) [17,27]  |
| TLC | 2/35 | 2/2 (100%) [16,48]  | TLC ↓; PIF ↓ (r 0.27) | 0/2 (0%) |
| TLC% pred. | 2/35 | 0/2 (0%) | N/A | 2/2 (100%) [16,27]  |
| DLCO | 1/35 | 1/1 (100%) [48]  | DLCO ↓; PIF ↓ (r 0.79) | 0/1 (0%) |
| VC | 1/35 | 1/1 (100%) [27]  | VC ↓; PIF ↓ (r ranging from 0.42 to 0.51) | 0/1 (0%) |
| VC% pred. | 1/35 | 0/1 (0%) | N/A | 1/1 (100%) [27]  |
| MEP | 2/35 | 1/2 (50%) [28]  | MEP ↓; PIF ↓ (r 0.5) | 1/2 (50%) [27]  |
| FIV | 1/35 | 1/1 (100%) [19]  | FIV ↓; PIF ↓ (r not stated) | 0/1 (0%) |
| FIVC | 2/35 | 2/2 (100%) [19,44]  | FIVC ↓; PIF ↓ (r 0.63) | 0/2 (0%) |
| MVV | 1/35 | 1/1 (100%) [19]  | MVV ↓; PIF ↓ (r not stated) | 0/1 (0%) |
| FIFmax | 1/35 | 1/1 (100%) [16]  | FIFmax ↓; PIF ↓ (r 0.65) | 0/1 (0%) |
| RV% pred. | 2/35 | 0/2 (0%) | N/A | 2/2 (100%) [16,27]  |
| RV/TLC ratio | 1/35 | 1/1 (100%) [16]  | RV/TLC ratio ↑; PIF ↓ (r −0.19) | 0/1 (0%) |
| Disease severity | 11/35 | 9/11 (82%) [19,26,30,33,40,41,47,48,50] 8  | Disease severity ↑; PIF ↓ | 2/11 (18%) [18,36]  |
| Exacerbations | 3/35 | 1/3 (33%) [34]  | ≥2 exacerbations in previous year; PIF ↓ | 2/3 (67%) [32,45]  |
| Symptoms (CAT, mMRC) | 7/35 | 2/7 (29%) [11,19]  | CAT scores ↑; PIF ↓ [11,19] | 5/7 (71%) [18,21,32,34,35]  |
| Other factors | ||||
| Enhanced educational training/instruction/verbal training/counseling | 5/35 | 5/5 (100%) [31,33,49,50,51] 9  | Enhanced educational training/instruction/verbal training/counseling ↑; PIF ↑ | 0/5 (0%) |
| Exercise training/inspiratory muscle training/respiratory physiotherapy | 3/35 | 2/3 (67%) [26,52]  | Exercise training ↑; PIF ↑ [52] Inspiratory muscle training ↑; PIF ↑ [26] | 1/3 (33%) [39]  |
| Critical errors in inhalation technique/non-adherence | 1/35 | 1/1 (100%) [34]  | Inhalation technique errors ↑; PIF ↓ Unconscious non-adherence ↑; PIF ↓ Deliberate non-adherence ↓; PIF ↓ Erratic non-adherence ↓; PIF ↓ | 0/1 10 (0%) |
| ADL score | 1/35 | 1/1 (100%) [32]  | ADL score ↑; PIF ↓ | 0/1 (0%) |
| Length of stay | 1/35 | 0/1 (0%) | N/A | 1/1 (100%) [11]  |
| ICS use | 1/35 | 0/1 (0%) | N/A | 1/1 (100%) [11]  |
| Primary education | 1/35 | 0/1 (0%) | N/A | 1/1 (100%) [34]  |
| FSI-10 | 1/35 | 0/1 (0%) | N/A | 1/1 (100%) [34]  |
| Pursed lip breathing | 1/35 | 0/1 (0%) | N/A | 1/1 (100%) [38]  |
| LVEF | 1/35 | 0/1 (0%) | N/A | 1/1 (100%) [11]  |
| Airway conductance | 1/35 | 0/1 (0%) | N/A | 1/1 (100%) [42]  |
| Arterial pH, PO2/FiO2 | 1/35 | 0/1 (0%) | N/A | 1/1 (100%) [29]  |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leving, M.T.; Kocks, J.; Bosnic-Anticevich, S.; Dekhuijzen, R.; Usmani, O.S. Relationship between Peak Inspiratory Flow and Patient and Disease Characteristics in Individuals with COPD—A Systematic Scoping Review. Biomedicines 2022, 10, 458. https://doi.org/10.3390/biomedicines10020458
Leving MT, Kocks J, Bosnic-Anticevich S, Dekhuijzen R, Usmani OS. Relationship between Peak Inspiratory Flow and Patient and Disease Characteristics in Individuals with COPD—A Systematic Scoping Review. Biomedicines. 2022; 10(2):458. https://doi.org/10.3390/biomedicines10020458
Chicago/Turabian StyleLeving, Marika T., Janwillem Kocks, Sinthia Bosnic-Anticevich, Richard Dekhuijzen, and Omar S. Usmani. 2022. "Relationship between Peak Inspiratory Flow and Patient and Disease Characteristics in Individuals with COPD—A Systematic Scoping Review" Biomedicines 10, no. 2: 458. https://doi.org/10.3390/biomedicines10020458