 Henner Hanssen1*†
Henner Hanssen1*† Alice Minghetti1†
Alice Minghetti1† Stefano Magon2,3Anja Rossmeissl1Athina Papadopoulou2Christopher Klenk1
Stefano Magon2,3Anja Rossmeissl1Athina Papadopoulou2Christopher Klenk1 Arno Schmidt-Trucksäss1
Arno Schmidt-Trucksäss1 Oliver Faude1Lukas Zahner1Till Sprenger2,4
Oliver Faude1Lukas Zahner1Till Sprenger2,4 Lars Donath1,5
Lars Donath1,5- 1Department of Sport, Exercise and Health, University of Basel, Basel, Switzerland
- 2Department of Neurology, University Hospital Basel and University of Basel, Basel, Switzerland
- 3Medical Image Analysis Center, University Hospital Basel, Basel, Switzerland
- 4Department of Neurology, DKD HELIOS Klinik Wiesbaden, Wiesbaden, Germany
- 5Department of Intervention Research in Exercise Training, Institute of Exercise Training and Computer Science in Sport, German Sport University Cologne, Köln, Germany
Background: Migraine is associated with increased cardiovascular risk and vascular dysfunction. Since aerobic exercise can reduce cardiovascular risk, the present randomized controlled trail aimed at investigating the effects of high-intensity interval training (HIT) vs. moderate continuous exercise training (MCT) on arterial stiffness in migraine patients.
Methods: Forty-eight episodic migraineurs were initially enrolled in the study. 37 patients [female: 30; age: 37 (SD: 10); BMI: 23.1 (5.2); Migraine days per month: 3.7 (2.5)] completed the intervention. Central blood pressure, pulse wave reflection, and aortic pulse wave velocity (PWV) were obtained by an oscillometric monitor. Incremental treadmill exercise testing yielded maximal and submaximal fitness parameters. Participants were randomly assigned to either HIT, MCT, or a control group (CON). The intervention groups trained twice a week over a 12-week intervention period.
Results: After adjustment for between-group baseline differences, a moderate meaningful overall reduction of the augmentation index at 75 min−1 heart rate (AIx@75) was observed [partial eta squared (ηp2) = 0.16; p = 0.06]. With 91% likely beneficial effects, HIT was more effective in reducing AIx@75 than MCT [HIT: pre 22.0 (9.7), post 14.9 (13.0), standardized mean difference (SMD) = 0.62; MCT: pre 16.6 (8.5), post 21.3 (10.4), SMD −0.49]. HIT induced a relevant reduction in central systolic blood pressure [cSBP: pre 118 (23) mmHg, post 110 (16) mmHg, SMD = 0.42] with a 59% possibly beneficial effect compared to CON, while MCT showed larger effects in lowering central diastolic blood pressure [pre 78 (7) mmHg, post 74 (7) mmHg, SMD = 0.61], presenting 60% possibly beneficial effects compared to CON. Central aortic PWV showed no changes in any of the three groups. Migraine days were reduced more successfully by HIT than MCT (HIT: SMD = 1.05; MCT: SMD = 0.43).
Conclusion: HIT but not MCT reduces AIx@75 as a measure of pulse wave reflection and indirect marker of systemic arterial stiffness. Both exercise modalities beneficially affect central blood pressure. HIT proved to be an effective complementary treatment option to reduce vascular dysfunction and blood pressure in migraineurs.
Introduction
Migraine is considered a debilitating neurological disease which recurs in the form of severe headache attacks accompanied with nausea, vomiting, phonophobia, and photophobia (Jiménez Caballero and Muñoz Escudero, 2013). Despite high prevalence rates (Stovner and Andree, 2010), the complex pathogenetic mechanisms involved in migraine remain to be elucidated (Jiménez Caballero and Muñoz Escudero, 2013). Various studies have been able to link migraine to adverse vascular risk profiles (Sacco et al., 2012, 2015). Migraine is associated with an increased risk of cardiovascular disease (CVD) such as myocardial infarction and stroke (Kurth et al., 2008; Schürks et al., 2009, 2011; Spector et al., 2010). A recent study revealed that there are about 2.6 million individuals in the U.S. suffering from episodic migraine with one or more cardiovascular events or conditions (Buse et al., 2017). Migraineurs have independently been associated with increased aortic stiffness and enhanced peripheral wave reflection (Schillaci et al., 2010), endothelial dysfunction (Jiménez Caballero and Muñoz Escudero, 2013) as well as increased hypercoagulability and inflammation (Kurth et al., 2008). This evidence suggests that functional properties of large arteries are altered in migraine patients (Liman et al., 2012), leading to an overall increase in cardiovascular risk (Liew et al., 2006; Rose et al., 2007; Kurth et al., 2008, 2016; Buse et al., 2017).
Arterial stiffness is an established independent predictor of cardiovascular events and stroke in healthy patients (Mitchell et al., 2010). The augmentation index (AIx) serves as an established systemic haemodynamic marker of pulse wave reflection and is closely related to the development of atherosclerosis and incidence cardiovascular events (Vlachopoulos et al., 2010a). An increased AIx displays a greater contribution of the reflected wave to the central blood pressure, indicating increased arterial stiffness and cardiac afterload as well as an unfavorably altered central blood pressure. As the AIx is dependent on heart rate (HR) (Wilkinson et al., 2000), the corrected augmentation index calculated for a set of heart rate of 75 beats per minute (AIx@75) is usually applied for a more valid comparison in resting state. Pulse wave velocity (PWV) is a direct measure of large artery stiffness and an independent predictor of CV morbidity and mortality (Hansen, 2010; Vlachopoulos et al., 2010b; Ben-Shlomo et al., 2014).
Higher levels of physical activity and cardiorespiratory fitness reduce all-cause mortality and CVD (Rognmo et al., 2004). Physical activity inversely correlates with an age-dependent increase of arterial stiffness (Kozakova et al., 2007) and cardiorespiratory fitness and sports-related activity are inversely correlated with arterial stiffness in younger adults (Boreham et al., 2004). More recently, higher levels of moderate-to-vigorous physical activity were independently associated with slower age-related progression of central arterial stiffness (Ahmadi-Abhari et al., 2017). Furthermore, endurance exercise training has been shown to improve arterial stiffness in patients with coronary artery disease (Edwards et al., 2004). Regular high-intensity interval training (HIT) has been shown to induce superior improvement in aerobic fitness, endothelial function, as well as other cardio-metabolic risk factors in comparison to moderate continuous exercise training (MCT) (Wisløff et al., 2007; Tjønna et al., 2008). Higher exercise intensities applied in intermittent bouts of highly intense aerobic exercise seem to affect pulse wave reflection more beneficially than moderate continuous exercise (Hanssen et al., 2015). To date, few studies have examined the effects of different exercise modalities in patients suffering from migraine (Hanssen et al., 2017). This is the first study comparing the effects of different longer term exercise training modalities on arterial stiffness and attack frequency in migraineurs. We hypothesized that regular HIT is a more beneficial means compared to MCT for the reduction of central and peripheral arterial stiffness indices, blood pressure, and migraine attack frequency.
Methods
Study Design and Participants
The present study was designed as a three-armed randomized controlled trial with a primary endpoint set on the effect of exercise training on pulse wave reflection in patients with migraine. In order to determine a clinical baseline for disease severity, patients underwent a 4-week run-in period prior to the start of the intervention period. After the run-in period and pre-testing measurements, 48 patients were randomly assigned [minimization method (Pocock and Stone, 2016), strata: age, gender, BMI, PA, migraine assessment according to MIDAS score, physical fitness determined by VO2max] to one of three groups: high intensity aerobic interval training group (HIT), moderate continuous aerobic training group (MCT), or control group (CON). Baseline parameters are depicted in Table 1. The intervention groups MCT and HIT trained twice a week over the 12-week intervention period. CON were requested to maintain their habitual daily physical activity profile and received additional standard physical activity recommendations. During the 12 weeks, a total of 11 (23%) patients dropped out due to injury, lack of motivation or personal reasons (Figure 1). Before and after 12 weeks of training, pulse wave reflection, PWV, and cardiopulmonary exercise testing were assessed in pre- and post-testing procedures. During the entire training study, patients were asked to keep a migraine and physical activity diary documenting the frequency and side effects of the attacks as well as their physical activity profiles. The study was registered in the German clinical trial register (DRKS-ID: DRKS00008015) and has been approved by the regional ethics committee (Ethical approval number: 194/13). All subjects signed an informed written consent after receiving all relevant study information.
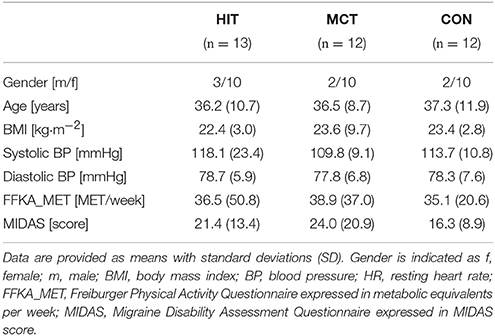
Table 1. Baseline data of the participants for both intervention groups (HIT and MCT) and the control group (CON).
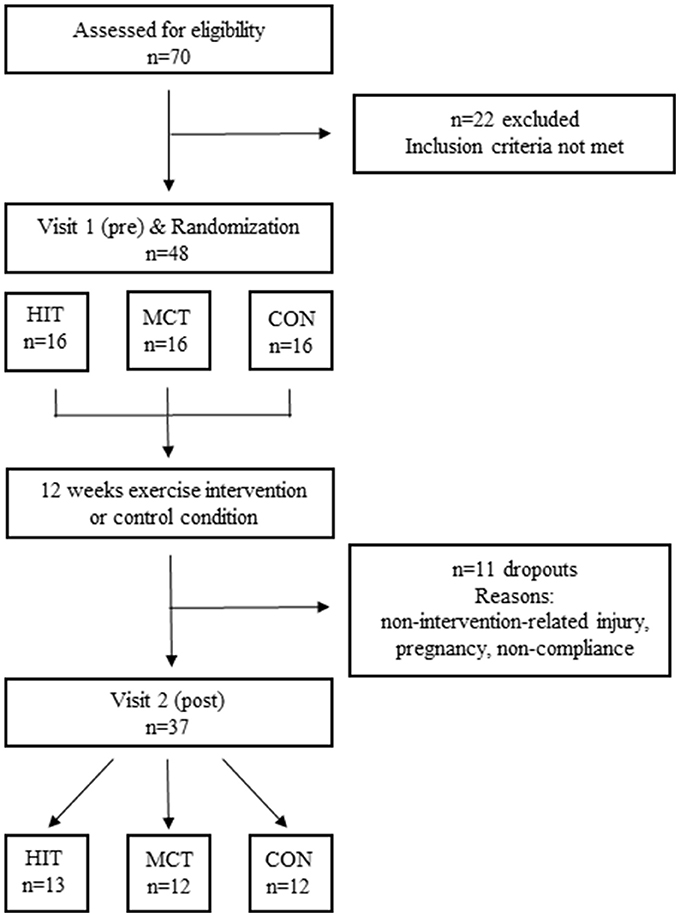
Figure 1. Flow-chart of the randomized controlled trial.
All examinations were performed at the University of Basel, Switzerland. Patients were recruited from the outpatient division of the Department of Neurology at the University Hospital Basel and via advertisements. Following the initial clinical screening, confirmation of the diagnosis was given by a neurologist. The neurological examinations were normal in all patients.
Inclusion and Exclusion Criteria
Inclusion criteria comprising the diagnosis of episodic migraine without aura were confirmed by an experienced neurologist according to the International Classification of Headache Disorders, third edition (ICHD-IIIb) (Headache Classification Committee of the International Headache Society, 2013). Exclusion criteria were (a) current medical preventive therapy (patients were included if preventive medication was stopped at least 8 weeks prior to study participation), (b) other internal or neurological diseases, and (c) regular exercise experience within the last 6 months. The ability to participate in an intense exercise program was confirmed using the physical activity readiness questionnaire (PAR-Q) and the exercise test. Patients with CVD or acute or chronic inflammatory disease were not included in the study.
Testing Procedures
Arterial Stiffness
Arterial stiffness parameters were obtained using an oscillometric Mobil-O-Graph® PWA Monitor device (I.E.M GmbH, Stolberg, Germany) with integrated ARCSolver® software. The blood pressure cuff was placed on the left upper arm while the patient was lying in a resting supine position. The measurements of arterial stiffness and central hemodynamics using the oscillometric method stand in good agreement with the conventional tonometric method (Wassertheurer et al., 2010). The first of three measurements was performed after 5 min of resting period. The two following measurements were performed at 2-min intervals. From the measurements, central blood pressures, crude Aix, and AIx@75 as well as PWV were extracted. After data readout, every measurement was reviewed for erroneous values. The mean and standard deviation of three valid measurements were calculated.
Recording Migraine Days
Prior to training (4-week run-in period) and during the exercise intervention a standardized paper and pencil migraine diary was kept by all patients (Baos et al., 2005). The last 4 weeks of the intervention period were considered as post value.
Maximal Exercise Testing
Exercise testing was conducted on a treadmill (HP Cosmos Pulsar, H/P/COSMOS Sports & Medical, Germany) to determine the individual anaerobic lactate-threshold (LT), maximal heart rate (HRmax), and VO2max. To obtain these data within one test, incremental protocols were combined with a ramp-like protocol (Meyer et al., 2007). Patients started at 5 km/h, step duration lasted 3 min with an increment of 1 km/h and a capillary lactate withdrawal for each step. After 5 steps (9 km/h), a ramp-wise increase of 1.0 km/h per minute without lactate withdrawal was applied to assess VO2max (Scharhag-Rosenberger et al., 2012). During exercise testing, breath-by-breath spirometric gas-exchange data (Metamax 3b, Cortex, Leipzig, Germany), heart rate (HR) (Polar Electro Oy, Kempele, Finland), and ratings of perceived exertion (RPE) (Borg, 1998) were collected. The maximum of the three highest consecutive oxygen uptake and heart rate values were regarded as VO2max and HRmax, while the individual anaerobic LT was determined according to Hagberg and Coyle (1983). For the analyses, the running speed at the LT in kilometer per hour (km/h) was used.
Exercise Intervention
Both HIT and MCT were conducted individually under supervision of a sports scientists at the Department of Sports, Exercise and Health (DSBG) of the University of Basel, Switzerland, and consisted of an individual running program on a treadmill. A general warm-up of 400 m easy running followed by two skipping exercises and a cool-down period of 400 m and stretching exercises were included. MCT was performed by maintaining the calculated target heart rate of 70% (± 5 beats per minutes, bpm) of HRmax for 45 min (Helgerud et al., 2007). Exercising 45 min at this specific intensity results in similar energy expenditure as the chosen HIT program (Helgerud et al., 2007). During HIT, the target intensity of 90 to 95% HRmax (±5 bpm) was generally reached after 1 min. Each interval lasted 4 min, followed by an active rest period of 3 min at 70% of HRmax. The 4-min intervals were repeated four times (Helgerud et al., 2007). HR-monitors collected heart rate data of each training session. The total training distance was recorded for each session. In total, 24 training sessions were conducted. It was required to complete at least 20 training sessions (~80% attendance, “per protocol” analysis) during the 12-week training period. No adverse and serious adverse events were reported.
Statistics
Indices of central haemodynamics and arterial stiffness, migraine attack frequency, and maximal and submaximal fitness were given as means with standard deviations (SD).
Analyses of covariance (ANCOVA) were computed to adjust between-group effects for potential baseline differences (Vickers and Altman, 2001). To estimate practical relevance of the ANCOVA between group effects, effect sizes (partial eta squared, ) were additionally calculated. According to Cohen (Cohen et al., 2013), an ≥ 0.01 indicates a small, ≥0.06 a medium and ≥0.14 a large effect. Standardized mean differences (Cohen's d, trivial: SMD < 0.2, small: 0.2 ≤ SMD < 0.5, moderate: 0.5 ≤ SMD < 0.8, large SMD ≥ 0.8; Cohen, 1992) were calculated for each pairwise comparison for each variable.
Additionally, the absolute and percentage differences as well as the standardized mean differences (Cohen's d) in the change scores between HIT, MCT, and CON from pre- to post-testing were also calculated together with 90% confidence intervals according to the magnitude-based inference approach (Batterham and Hopkins, 2006): These calculations were adjusted for pre-test values as well. A practically worthwhile change was assumed when the difference score was at least 0.2 of the between-subject standard deviation (Hopkins et al., 2009). The probability for an effect being practically worthwhile was calculated according to the magnitude-based inference approach using the following scale: 25–75%, possibly; 75–95%, likely; 95–99.5%, very likely; >99.5%, most likely (Batterham and Hopkins, 2006). The default probabilities for declaring an effect practically beneficial were <0.5% (most unlikely) for harm and >25% (possibly) for benefit (Hopkins et al., 2009). All calculations were conducted using a published spreadsheet in Microsoft® excel (Hopkins, 2007).
Results
Arterial Stiffness
Taking baseline values into account, ANCOVA revealed a large and relevant between group effect for AIx@75 (p = 0.06, = 0.16). Pairwise comparison of AIx@75 showed moderate effects in HIT [pre: 22.0 (9.7), post: 14.9 (13.0), SMD = 0.62] with a likelihood of a meaningful effect of 85% likely beneficial compared to CON and 91% likely beneficial compared to MCT (Tables 2, 3). Figure 2 demonstrates the pairwise between group comparisons for AIx@75 change scores. Central systolic blood pressure (cSBP) was lowered in HIT [cSBP HIT: pre: 118.1 (23.4), post: 109.8 (15.7), SMD = 0.42] with a likelihood of a meaningful effect of 59% possibly beneficial compared to CON. Central diastolic blood pressure showed moderate effects in MCT [pre: 77.8 (6.8), post: 73.7 (6.6), SMD = 0.61] with a likelihood of a meaningful effect of 60% possibly beneficial compared to CON (Tables 2, 3).
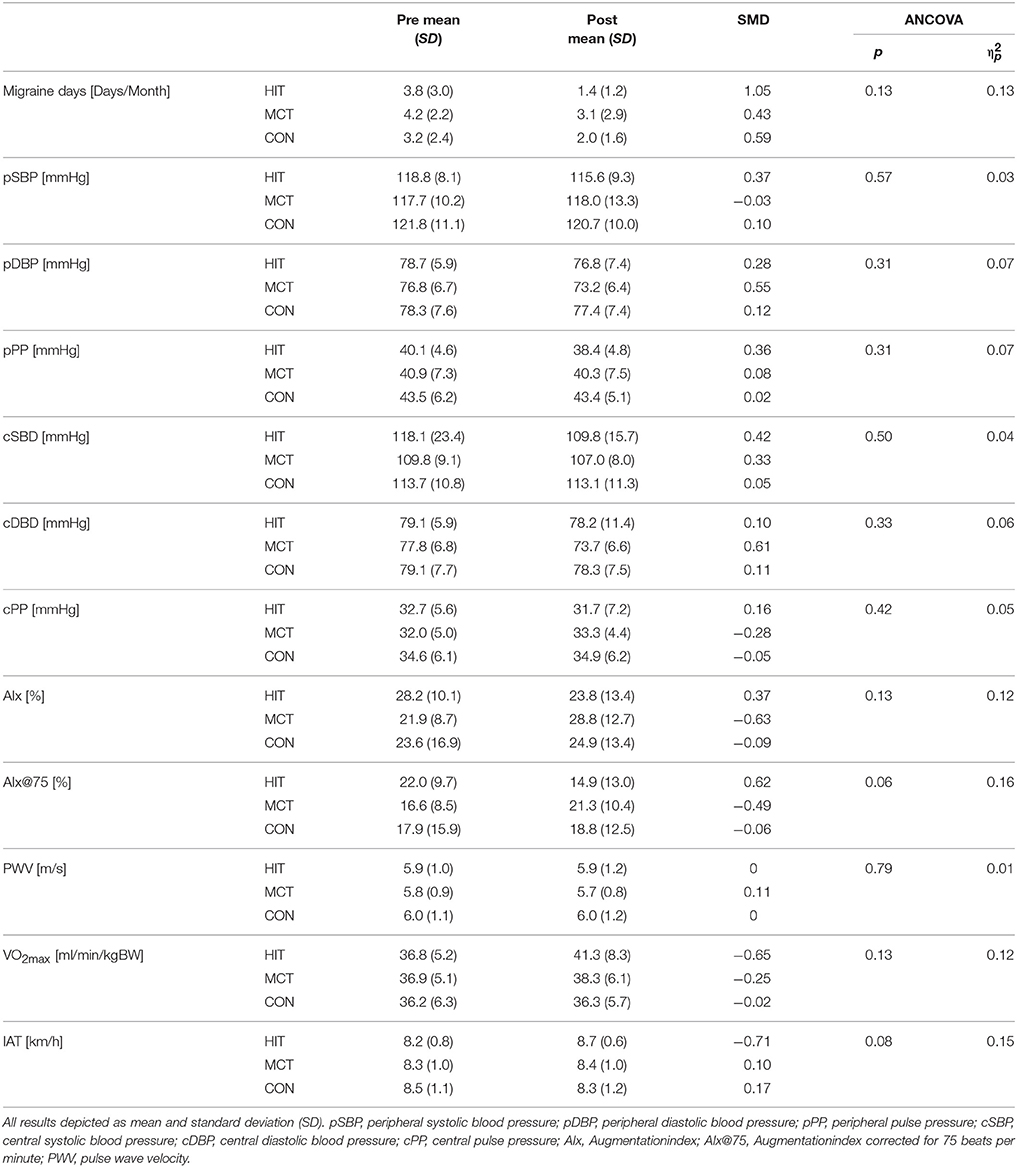
Table 2. Pre and post intervention results of all three groups for peripheral and central vessel parameters and arterial stiffness parameters.
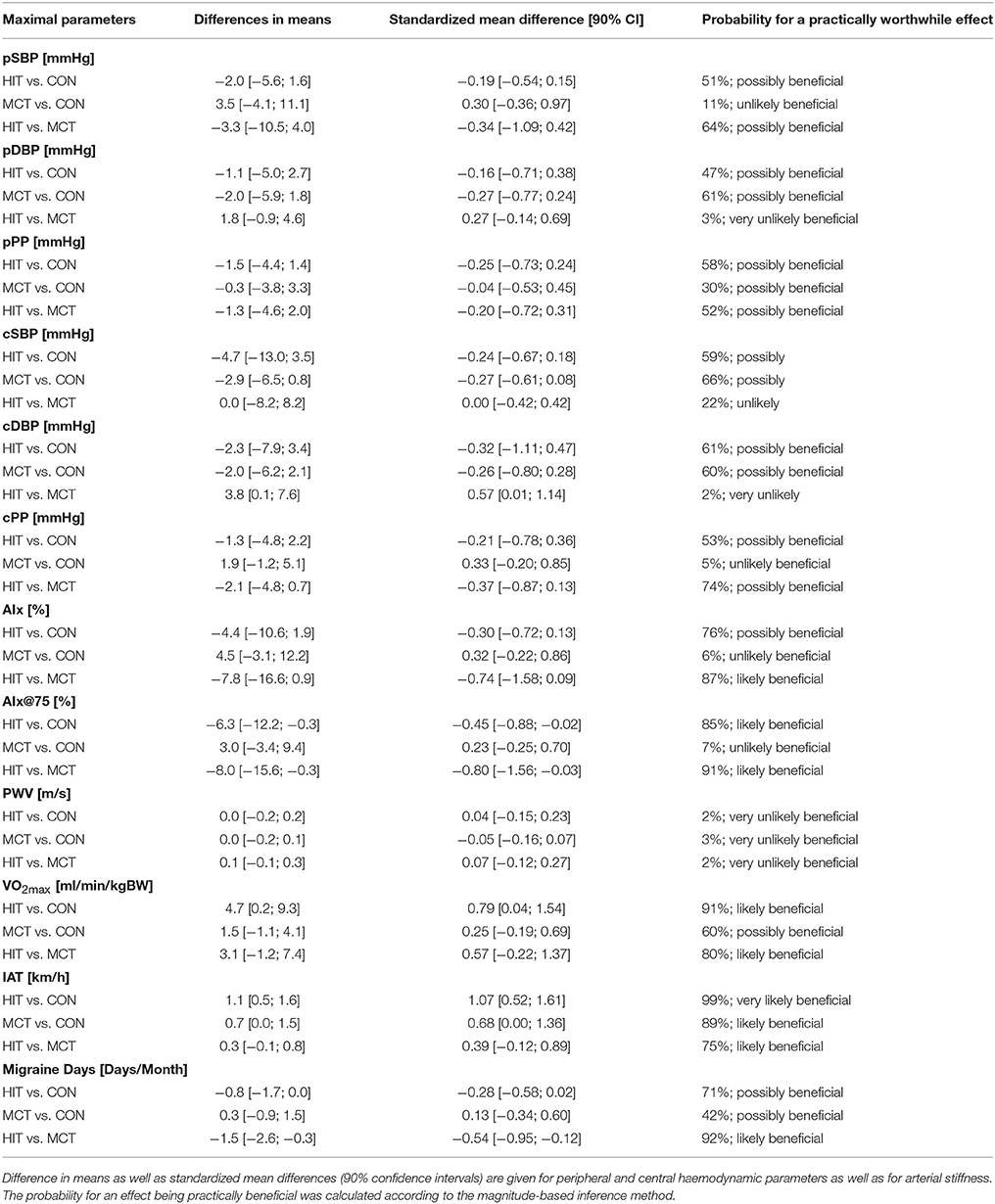
Table 3. Parallel Group Trials for HIT, MCT, and CON.
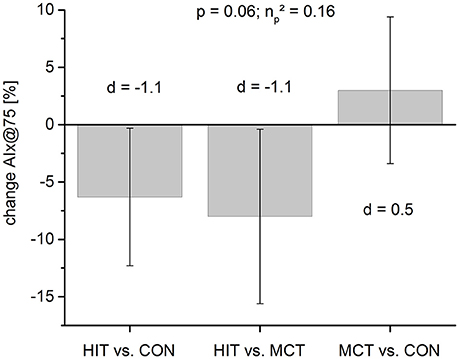
Figure 2. Mean change scores (%) for peripheral arterial stiffness (AIx@75) for pairwise between group comparison. Standardized mean differences are given as Cohen's d indicating moderate effects for HIT (0.5 < d < 0.7) compared to both groups. MCT vs. CON remains unchanged.
PWV showed no changes in any of the three groups (Tables 2, 3).
Migraine Days
ANCOVA, again taking baseline values into account, revealed moderate and relevant between group effect for migraine days (p = 0.13, = 0.13). Pairwise comparison of migraine days showed very large effects in HIT [pre: 3.8 (3.0), post: 1.4 (1.2), SMD = 1.05] with a likelihood of a meaningful effect of 71% possibly beneficial compared to CON and 92% likely beneficial compared to MCT. MCT revealed a 42% possibly beneficial effect compared to CON. Migraine days are reported as number of migraine days per month (Tables 2, 3).
Maximal and Submaximal Fitness Parameters
ANCOVA revealed a moderate but relevant between group effect for VO2max (p = 0.13, = 0.12) and IAT (p = 0.08, = 0.15). Pairwise comparison of VO2max showed moderate effects in favor of HIT [(ml/min/kg) pre: 36.8 (5.2), post: 41.3 (8.3), SMD = −0.65] and small effects for MCT [(ml/min/kg) pre: 36.9 (5.1), post: 38.3 (6.1), SMD = −0.25]. HIT showed a 91% likely beneficial effect while MCT revealed a 60% possibly beneficial effect over CON. Pairwise comparison of IAT revealed moderate effects in HIT [(km/h) pre: 8.2 (0.8), post: 8.7 (0.6), SMD = −0.71].
Discussion
The aim of the present randomized controlled trial was to investigate whether different aerobic exercise intensity modalities yield differential effects on central systolic and diastolic blood pressure, pulse wave reflection, and PWV in episodic migraineurs. To the best of our knowledge, no study to date has compared the effects of different exercise modalities and intensities on arterial stiffness and migraine. Our results show that HIT but not MCT was able to lower AIx@75 while both exercise programs were able to reduce migraine days and improve physical fitness. We could further elucidate that HIT is superior to MCT in improving AIx as an indirect marker of systemic arterial stiffness, which indicates cardiovascular risk reduction in migraineurs. The exercise-induced adaptations of arterial stiffness may be attributed in large part to an increased availability of nitric oxide (NO) and a consecutive improvement of endothelial function. Increases in shear stress during exercise induce NO production of the endothelium, which results in relaxation of vascular smooth muscle cells, arterial vasodilation, and a drop in vascular resistance (Alsop and Hauton, 2016). It has been suggested that the regulation of vascular tone in response to endothelial sheer stress stimulus is impaired in migraineurs and NO is regarded as crucial factor in the process (Buse et al., 2017). An increased nitrate-mediated response during development of migraine has been suggested, supporting the theory of overregulated NO sensitivity in migraineurs (Buse et al., 2017). Our results indirectly suggest that the improvement of NO regulation is intensity-dependent, whereby higher intensities applied in intervals compel stronger vascular adaptations. These findings correspond to previous findings comparing acute effects of HIT and MCT on arterial stiffness, which showed that AIx@75 declined significantly over time after HIT but less after MCT (Hanssen et al., 2015). HIT induces higher laminar shear stress compared to lower continuous exercise intensities and, therefore, HIT represents a stronger stimulus for shear stress-induced release of NO (Adams et al., 2017). This may, in part, explain why HIT reduced AIx@75 as well as migraine days more efficiently than MCT. Regular exercise, and HIT in particular, has the potential to improve NO production and regulation in migraineurs and reduce migraine days. Further research is needed to clarify the postulated mechanistic link and its causality.
Interestingly, PWV showed no changes in any of the three groups even though HIT reduced central systolic blood pressure while MCT reduced central diastolic blood pressure. These results are in line with the few studies which have examined the effects of exercise on PWV (Heffernan et al., 2007; Munir et al., 2008). Central arteries seem to require longer intervention periods with regular stimulus than the conduit and more peripheral vessels in order to adapt to aerobic exercise stimuli (Hanssen et al., 2015). As expected, CON underwent no changes in any arterial stiffness parameters.
Migraine attacks are accompanied by repeated spells of vascular inflammation and repeated attacks of migraine have been suggested to induce inflammatory changes of cranial arteries (Bolay et al., 2002). These recurring inflammatory processes may predispose to vascular endothelial dysfunction (Schillaci et al., 2010). In previous studies, HIT has been shown to be superior to MCT in reducing arterial stiffness over a 24 h period in normotensive patients (Hanssen et al., 2015) as well as reducing cardio-metabolic risk in patients with CVD (Wisløff et al., 2007). The improvement of AIx@75 following HIT in our study indicates the potential to reduce cardiovascular risk in migraineurs, as a decrease in AIx is associated with a decreased cardiac afterload and left ventricular burden long-term (Vlachopoulos et al., 2012; Hanssen et al., 2015). A 10% increase of AIx is associated with a 30% increased relative risk for cardiovascular events (Vlachopoulos et al., 2010b). Therefore, HIT may prove to be an effective therapy for the reduction of migraine symptoms, improving vascular function and integrity as well as reducing cardiovascular risk. We would like to postulate that interval-like application of high intensities evoke patterns of wave reflection that improve vascular function more than continuous lower intensity applications. Increased NO bioavailability evoked by the HIT protocol is one of the most likely mechanisms that help explain these findings.
The study comprises some limitations that need to be mentioned. The sample size of the pilot study might be considered low. In our group analysis, we refrained from interpreting our data on the basis of mere conventional p-values to estimate relevant between-group effects, as p-values do not sufficiently allow for continuous estimation of relevant interventional effect sizes (Pocock and Stone, 2016). Indeed, these would have failed to reach significance due to the relatively small sample size of this study. Although increased arterial stiffness and cardiovascular risk has been reported in migraine, the patients in our study did not have impaired baseline levels of AIx or PWV according to the current recommendations for normal values (Hansen, 2010; Janner et al., 2010). A selection bias may have occurred whereby healthier and physically fitter patients were motivated to participate in the exercise intervention trial. In addition, despite group allocation based on physical fitness and migraine days per month, notable baseline differences in migraine days as well as arterial stiffness parameters AIx and AIX@75 need to be addressed. These findings might further be caused by the dropouts. We applied fitness and the MIDAS (migraine disability assessment) questionnaire as strata for group allocation. Moreover, we included baseline values and age as covariates. Thus, our results are adjusted for potential baseline differences.
Conclusion
Regular aerobic exercise has beneficial effects on blood pressure, vascular function, and cardiovascular risk. Since HIT was more effective in reducing systemic arterial stiffness and migraine days than MCT, we postulate that the exercise effects in migraine patients depend on intensity and modality of the exercise therapy. HIT should be considered as a complementary treatment strategy for migraine treatment and prevention. It is all the more important since drug treatment of migraine is oftentimes addressed with precautions in the presence of cardiovascular comorbidities. Exercise therapy seems to have the potential to play a crucial role in future preventive strategies to combat migraine complaints and development of associated CVD.
Author Contributions
Study design: HH, TS, and LD; data collection: AM, SM, AR, AP, and CK; statistical analysis: AM and LD; manuscript preparation: HH, AM, TS, and LD; manuscript revision: OF, AS-T, and LZ.
Funding
This study was funded by the Research Fund of the University of Basel.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We cordially thank all participants for their confidence and compliance in taking part in our research. We wish to thank the Neurology Department of the University Hospital of Basel (Alain Thoeni, Elena Gross) for their collaboration and flexibility. Furthermore, we would like to thank the students who were involved in data acquisition and conduction of measurements as well as coordination with the patients and supervision of training sessions.
References
Adams, V., Reich, B., Uhlemann, M., and Niebauer, J. (2017). Molecular effects of exercise training in patients with cardiovascular disease: focus on skeletal muscle, endothelium, and myocardium. Am. J. Physiol. Heart Circ. Physiol. 313, H72–H88. doi: 10.1152/ajpheart.00470.2016
Ahmadi-Abhari, S., Sabia, S., Shipley, M. J., Kivimäki, M., Singh-Manoux, A., Tabak, A., et al. (2017). Physical activity, sedentary behavior, and long-term changes in aortic stiffness: the whitehall II study. J. Am. Heart Assoc. 6:e005974. doi: 10.1161/JAHA.117.005974
Alsop, P., and Hauton, D. (2016). Oral nitrate and citrulline decrease blood pressure and increase vascular conductance in young adults: a potential therapy for heart failure. Eur. J. Appl. Physiol. 116, 1651–1661. doi: 10.1007/s00421-016-3418-7
Baos, V., Ester, F., Castellanos, A., Nocea, G., Caloto, M. T., and Gerth, W. C. (2005). Use of a structured migraine diary improves patient and physician communication about migraine disability and treatment outcomes. Int. J. Clin. Pract. 59, 281–286. doi: 10.1111/j.1742-1241.2005.00469.x
Batterham, A. M., and Hopkins, W. G. (2006). Making meaningful inferences about magnitudes. Int. J. Sports Physiol. Perform. 1, 50–57. doi: 10.1123/ijspp.1.1.50
Ben-Shlomo, Y., Spears, M., Boustred, C., May, M., Anderson, S. G., Benjamin, E. J., et al. (2014). Aortic pulse wave velocity improves cardiovascular event prediction: an individual participant meta-analysis of prospective observational data from 17,635 subjects. J. Am. Coll. Cardiol. 63, 636–646. doi: 10.1016/j.jacc.2013.09.063
Bolay, H., Reuter, U., Dunn, A. K., Huang, Z., Boas, D. A., and Moskowitz, M. A. (2002). Intrinsic brain activity triggers trigeminal meningeal afferents in a migraine model. Nat. Med. 8, 136–142. doi: 10.1038/nm0202-136
Boreham, C. A., Ferreira, I., Twisk, J. W., Gallagher, A. M., Savage, M. J., and Murray, L. J. (2004). Cardiorespiratory fitness, physical activity, and arterial stiffness: the Northern Ireland young hearts project. Hypertension 44, 721–726. doi: 10.1161/01.HYP.0000144293.40699.9a
Buse, D. C., Reed, M. L., Fanning, K. M., Kurth, T., and Lipton, R. B. (2017). Cardiovascular events, conditions, and procedures among people with episodic migraine in the US Population: results from the American migraine prevalence and prevention (AMPP) study. Headache 57, 31–44. doi: 10.1111/head.12962
Cohen, J., Cohen, P., West, S. G., and Aiken, L. S. (2013). Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences. Mahwah, NJ: Routledge.
Edwards, D. G., Schofield, R. S., Magyari, P. M., Nichols, W. W., and Braith, R. W. (2004). Effect of exercise training on central aortic pressure wave reflection in coronary artery disease. Am. J. Hypertens. 17, 540–543. doi: 10.1016/j.amjhyper.2003.12.001
Hagberg, J. M., and Coyle, E. F. (1983). Physiological determinants of endurance performance as studied in competitive racewalkers. Med. Sci. Sports Exerc. 15, 287–289. doi: 10.1249/00005768-198315040-00006
Hansen, T. W. (2010). Determinants of pulse wave velocity in healthy people and in the presence of cardiovascular risk factors:'establishing normal and reference values'. Eur. Heart J. 31, 2338–2350. doi: 10.1093/eurheartj/ehq165
Hanssen, H., Minghetti, A., Magon, S., Rossmeissl, A., Rasenack, M., Papadopoulou, A., et al. (2017). Effects of different endurance exercise modalities on migraine days and cerebrovascular health in episodic migraineurs: A randomized controlled trial. Scand. J. Med. Sci. Sports. doi: 10.1111/sms.13023. [Epub ahead of print].
Hanssen, H., Nussbaumer, M., Moor, C., Cordes, M., Schindler, C., and Schmidt-Trucksäss, A. (2015). Acute effects of interval versus continuous endurance training on pulse wave reflection in healthy young men. Atherosclerosis 238, 399–406. doi: 10.1016/j.atherosclerosis.2014.12.038
Headache Classification Committee of the International Headache Society, IHS. (2013). The international classification of headache disorders, 3rd edition (beta version). Cephalalgia 33, 629–808. doi: 10.1177/0333102413485658
Heffernan, K. S., Collier, S. R., Kelly, E. E., Jae, S. Y., and Fernhall, B. (2007). Arterial stiffness and baroreflex sensitivity following bouts of aerobic and resistance exercise. Int. J. Sports Med. 28, 197–203. doi: 10.1055/s-2006-924290
Helgerud, J., Hoydal, K., Wang, E., Karlsen, T., Berg, P., Bjerkaas, M., et al. (2007). Aerobic high-intensity intervals improve VO2 max more than moderate training. Med. Sci. Sports Exerc. 39, 665–671. doi: 10.1249/mss.0b013e3180304570
Hopkins, W. G. (2007). A spreadsheet for deriving a confidence interval, mechanistic inference and clinical inference from a P value. Sportscience 11, 16–21.
Hopkins, W. G., Marshall, S. W., Batterham, A. M., and Hanin, J. (2009). Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 41, 3–13. doi: 10.1249/MSS.0b013e31818cb278
Janner, J. H., Godtfredsen, N. S., Ladelund, S., Vestbo, J., and Prescott, E. (2010). Aortic augmentation index: reference values in a large unselected population by means of the SphygmoCor device. Am. J. Hypertens. 23, 180–185. doi: 10.1038/ajh.2009.234
Jiménez Caballero, P. E., and Muñoz Escudero, F. (2013). Peripheral endothelial function and arterial stiffness in patients with chronic migraine: a case-control study. J. Headache Pain 14:8. doi: 10.1186/1129-2377-14-8
Kozakova, M., Palombo, C., Mhamdi, L., Konrad, T., Nilsson, P., Staehr, P. B., et al. (2007). Habitual physical activity and vascular aging in a young to middle-age population at low cardiovascular risk. Stroke 38, 2549–2555. doi: 10.1161/STROKEAHA.107.484949
Kurth, T., Schürks, M., Logroscino, G., Gaziano, J. M., and Buring, J. E. (2008). Migraine, vascular risk, and cardiovascular events in women: prospective cohort study. BMJ 337:a636. doi: 10.1136/bmj.a636
Kurth, T., Winter, A. C., Eliassen, A. H., Dushkes, R., Mukamal, K. J., Rimm, E. B., et al. (2016). Migraine and risk of cardiovascular disease in women: prospective cohort study. BMJ 353:i2610. doi: 10.1136/bmj.i2610
Liew, G., Mitchell, P., Wong, T. Y., and Wang, J. J. (2006). Retinal vascular caliber and migraine: the Blue Mountains eye study. Headache 46, 997–1004. doi: 10.1111/j.1526-4610.2006.00364.x
Liman, T. G., Neeb, L., Rosinski, J., Wellwood, I., Reuter, U., Doehner, W., et al. (2012). Peripheral endothelial function and arterial stiffness in women with migraine with aura: a case-control study. Cephalalgia 32, 459–466. doi: 10.1177/0333102412444014
Meyer, T., Auracher, M., Heeg, K., Urhausen, A., and Kindermann, W. (2007). Effectiveness of low-intensity endurance training. Int. J. Sports Med. 28, 33–39. doi: 10.1055/s-2006-924037
Mitchell, G. F., Hwang, S. J., Vasan, R. S., Larson, M. G., Pencina, M. J., Hamburg, N. M., et al. (2010). Arterial stiffness and cardiovascular events: the Framingham heart study. Circulation 121, 505–511. doi: 10.1161/CIRCULATIONAHA.109.886655
Munir, S., Jiang, B., Guilcher, A., Brett, S., Redwood, S., Marber, M., et al. (2008). Exercise reduces arterial pressure augmentation through vasodilation of muscular arteries in humans. Am. J. Physiol. Heart Circ. Physiol. 294, H1645–H1650. doi: 10.1152/ajpheart.01171.2007
Pocock, S. J., and Stone, G. W. (2016). The primary outcome fails - what next? N. Engl. J. Med. 375, 861–870. doi: 10.1056/NEJMra1510064
Rognmo, Ø., Hetland, E., Helgerud, J., Hoff, J., and Slørdahl, S. A. (2004). High intensity aerobic interval exercise is superior to moderate intensity exercise for increasing aerobic capacity in patients with coronary artery disease. Eur. J. Cardiovasc. Prev. Rehabil. 11, 216–222. doi: 10.1097/01.hjr.0000131677.96762.0c
Rose, K. M., Wong, T. Y., Carson, A. P., Couper, D. J., Klein, R., and Sharrett, A. R. (2007). Migraine and retinal microvascular abnormalities: the atherosclerosis risk in communities study. Neurology 68, 1694–1700. doi: 10.1212/01.wnl.0000261916.42871.05
Sacco, S., Ornello, R., Ripa, P., Tiseo, C., Degan, D., Pistoia, F., et al. (2015). Migraine and risk of ischaemic heart disease: a systematic review and meta-analysis of observational studies. Eur. J. Neurol. 22, 1001–1011. doi: 10.1111/ene.12701
Sacco, S., Ricci, S., and Carolei, A. (2012). Migraine and vascular diseases: a review of the evidence and potential implications for management. Cephalalgia 32, 785–795. doi: 10.1177/0333102412451361
Scharhag-Rosenberger, F., Walitzek, S., Kindermann, W., and Meyer, T. (2012). Differences in adaptations to 1 year of aerobic endurance training: individual patterns of nonresponse. Scand. J. Med. Sci. Sports 22, 113–118. doi: 10.1111/j.1600-0838.2010.01139.x
Schillaci, G., Sarchielli, P., Corbelli, I., Pucci, G., Settimi, L., Mannarino, M. R., et al. (2010). Aortic stiffness and pulse wave reflection in young subjects with migraine: a case-control study. Neurology 75, 960–966. doi: 10.1212/WNL.0b013e3181f25ecd
Schürks, M., Rist, P. M., Bigal, M. E., Buring, J. E., Lipton, R. B., and Kurth, T. (2009). Migraine and cardiovascular disease: systematic review and meta-analysis. BMJ 339:b3914. doi: 10.1136/bmj.b3914
Schürks, M., Rist, P. M., Shapiro, R. E., and Kurth, T. (2011). Migraine and mortality: a systematic review and meta-analysis. Cephalalgia 31, 1301–1314. doi: 10.1177/0333102411415879
Spector, J. T., Kahn, S. R., Jones, M. R., Jayakumar, M., Dalal, D., and Nazarian, S. (2010). Migraine headache and ischemic stroke risk: an updated meta-analysis. Am. J. Med. 123, 612–624. doi: 10.1016/j.amjmed.2009.12.021
Stovner, L. J., and Andree, C. (2010). Prevalence of headache in Europe: a review for the eurolight project. J. Headache Pain 11, 289–299. doi: 10.1007/s10194-010-0217-0
Tjønna, A. E., Lee, S. J., Rognmo, O., Stolen, T. O., Bye, A., Haram, P. M., et al. (2008). Aerobic interval training versus continuous moderate exercise as a treatment for the metabolic syndrome: a pilot study. Circulation 118, 346–354. doi: 10.1161/CIRCULATIONAHA.108.772822
Vickers, A. J., and Altman, D. G. (2001). Statistics notes: analysing controlled trials with baseline and follow up measurements. BMJ 323, 1123–1124. doi: 10.1136/bmj.323.7321.1123
Vlachopoulos, C., Aznaouridis, K., O'Rourke, M. F., Safar, M. E., Baou, K., and Stefanadis, C. (2010a). Prediction of cardiovascular events and all-cause mortality with central haemodynamics: a systematic review and meta-analysis. Eur. Heart J. 31, 1865–1871. doi: 10.1093/eurheartj/ehq024
Vlachopoulos, C., Aznaouridis, K., and Stefanadis, C. (2010b). Prediction of cardiovascular events and all-cause mortality with arterial stiffness: a systematic review and meta-analysis. J. Am. Coll. Cardiol. 55, 1318–1327. doi: 10.1016/j.jacc.2009.10.061
Vlachopoulos, C., Aznaouridis, K., Terentes-Printzios, D., Ioakeimidis, N., and Stefanadis, C. (2012). Prediction of cardiovascular events and all-cause mortality with brachial-ankle elasticity index: a systematic review and meta-analysis. Hypertension 60, 556–562. doi: 10.1161/HYPERTENSIONAHA.112.194779
Wassertheurer, S., Kropf, J., Weber, T., van der Giet, M., Baulmann, J., Ammer, M., et al. (2010). A new oscillometric method for pulse wave analysis: comparison with a common tonometric method. J. Hum. Hypertens. 24, 498–504. doi: 10.1038/jhh.2010.27
Wilkinson, I. B., MacCallum, H., Flint, L., Cockcroft, J. R., Newby, D. E., and Webb, D. J. (2000). The influence of heart rate on augmentation index and central arterial pressure in humans. J. Physiol. 525(Pt 1), 263–270. doi: 10.1111/j.1469-7793.2000.t01-1-00263.x
Wisløff, U., Stoylen, A., Loennechen, J. P., Bruvold, M., Rognmo, O., Haram, P. M., et al. (2007). Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients: a randomized study. Circulation 115, 3086–3094. doi: 10.1161/CIRCULATIONAHA.106.675041
Keywords: migraine, exercise, high intensity interval training, arterial stiffness, cardiovascular risk, randomized controlled trial
Citation: Hanssen H, Minghetti A, Magon S, Rossmeissl A, Papadopoulou A, Klenk C, Schmidt-Trucksäss A, Faude O, Zahner L, Sprenger T and Donath L (2017) Superior Effects of High-Intensity Interval Training vs. Moderate Continuous Training on Arterial Stiffness in Episodic Migraine: A Randomized Controlled Trial. Front. Physiol. 8:1086. doi: 10.3389/fphys.2017.01086
Received: 10 October 2017; Accepted: 11 December 2017;
Published: 19 December 2017.
Edited by:
Jun Sugawara, National Institute of Advanced Industrial Science and Technology, JapanReviewed by:
Takanobu Okamoto, Nippon Sport Science University, JapanMasato Nishiwaki, Osaka Institute of Technology, Japan
Copyright © 2017 Hanssen, Minghetti, Magon, Rossmeissl, Papadopoulou, Klenk, Schmidt-Trucksäss, Faude, Zahner, Sprenger and Donath. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Henner Hanssen, henner.hanssen@unibas.ch
†These authors have contributed equally to this work.