Field-Based Health-Related Physical Fitness Tests in Children and Adolescents: A Systematic Review
 Adilson Marques1,2
Adilson Marques1,2  Duarte Henriques-Neto1
Duarte Henriques-Neto1  Miguel Peralta1,2*
Miguel Peralta1,2*  João Martins1,2
João Martins1,2  Fernando Gomes3
Fernando Gomes3  Stevo Popovic4
Stevo Popovic4  Bojan Masanovic4
Bojan Masanovic4  Yolanda Demetriou5
Yolanda Demetriou5  Annegret Schlund5
Annegret Schlund5  Andreas Ihle6,7,8
Andreas Ihle6,7,8- 1CIPER, Faculty of Human Kinetics, University of Lisbon, Lisbon, Portugal
- 2ISAMB, University of Lisbon, Lisbon, Portugal
- 3Faculty of Human Kinetics, University of Lisbon, Lisbon, Portugal
- 4Faculty for Sport and Physical Education, University of Montenegro, Niksic, Montenegro
- 5Department of Sport and Health Sciences, Technical University of Munich, Munich, Germany
- 6Cognitive Aging Lab, Department of Psychology, University of Geneva, Geneva, Switzerland
- 7Center for the Interdisciplinary Study of Gerontology and Vulnerability, University of Geneva, Geneva, Switzerland
- 8Swiss National Centre of Competence in Research LIVES – Overcoming Vulnerability: Life Course Perspectives, Lausanne and Geneva, Switzerland
Physical fitness (PF) is a multi-component construct and a biomarker of health. Worse PF is related to vulnerability and predicts worse academic achievements. Thus, assessing PF is important to monitor health in youth. This systematic review aimed to identify and inform physical education, health professionals and entities about existing PF batteries and field-tests that can be used in school settings. A comprehensive literature search was carried out in five electronic databases (Academic Search Complete, Education Resources Information Center, PubMed, Scopus, and Web of Science) to identify PF battery protocols that can be carried out in the school setting. Overall, 24 PF batteries were identified. Regarding the PF components assessed, only cardiorespiratory fitness and upper body strength were contemplated in all batteries. Middle-body strength and lower body strength were presented in most batteries (21 and 19 of 24, respectively). Agility (16 of 24) and body composition (16 of 24) were also considered in several batteries, although to a lesser extent. Flexibility (14 of 24) and speed (12 of 24) were the PF components less represented in the batteries. Among the 24 identified PF batteries, 81 PF tests assessing the different PF components were encountered. The advances in the PF field-based assessment in school settings and health in youth resulted in the amplification of the number of existing batteries. Considering the connection between PF and health and the opportunity that the school setting provides to assess fitness in children and adolescents, there is a need for standardization and a consensus of PF assessments in this specific setting.
Introduction
Physical fitness (PF) is a multi-component construct and a biomarker of health (1, 2). Worse PF is related to vulnerability (3) that can negatively affect human development, such as cognitive functioning (4, 5). This has important consequences children and adolescents. For instance, it has been shown that worse PF predicts substantially reduced improvements in academic achievement over time (6). PF is influenced by genetic and external factors (7). The genetic heritage has an essential role in trainability and describes the magnitude of the physiologic response to physical stress (2, 8). External factors such as regular PA, sleep, nutrition also have an impact on PF components (9–11). Assessing PF through specific and validated test protocols allows monitoring the biological and physiological adaptations that are achieved through natural development or training (12). Health-related PF components include body composition measures (i.e., body mass index [BMI], waist circumference), cardiorespiratory fitness (CRF), muscular fitness, speed, agility, balance, and coordination (13, 14). These components have been consistently associated with indicators of obesity, cardiovascular health, metabolic health, bone health, and mental health (1).
Assessing PF reflects the impact of genetic and environmental factors on health-related PF components and consequently on health indicators (15). In light of this, assessing PF is a simple, safe, and low-cost tool that allows examining several health indicators. Based on the PF level of children, pedagogical, and public health strategies and policies can be developed. However, to correctly and accurately assess PF, the validity, reliability, and feasibility of PF assessment tools are essential. This is especially true when health and government entities aim to monitor a variety of health indicators in local, regional, national, or worldwide populations to guide policy actions.
Previous systematic reviews identified a large number of test batteries available worldwide to test children's and adolescents' PF levels (16–18). These reviews showed that different tests address different components of fitness such as cardiorespiratory fitness, musculoskeletal fitness, body composition, and central body fat. Although the selected tests are extensively used and recognized, they do not determine all physical fitness aspects. Moreover, a large number of field-based fitness tests presented in these systematic reviews have limited evidence (16, 18). Furthermore, previous reviews sought to identify physical fitness tests that could be used with children and adolescents. However, some of the contexts identified for the application of some batteries were the sport context. This context is elitist because few children and adolescents practice physical activity in the sports context.
So far no systematic review that provides a summary of all existing fitness test batteries for children and adolescents that can be carried out in the school setting under the specific circumstances of the school (e.g., time constraints, equipment at schools, the scope of testing, costs) has been carried out. Therefore, this systematic review aimed to identify and summarize the existing field-based health-related PF batteries that can be performed in children and adolescents to monitor and improve their health status.
Methods
Data selection, collection, and analyses were performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (19).
Search Strategy and Data Sources
Five international databases (Academic Search Complete [ASC], Education Resources Information Center [ERIC], PubMed, Scopus, and Web of Science) were searched for scientific articles published in peer-reviewed journals until the 30th of April 2020 containing PF battery protocols. In each database, a search was conducted taking into account a predefined combination of keywords. The combination of keywords used in each database was the following: “field-based test” OR “fit*” OR “physical performance” OR “sport performance” OR “physical condition” OR “aerobic capacity” OR “maximum oxygen consumption” OR “strength” OR “flexibility” OR “motor” OR “endurance” OR “speed” OR “agility” OR “balance” OR “body composition” OR “anthropometry” OR “body mass index” OR “BMI” OR “skinfolds” OR “waist circumference” AND “batter*” OR “protocol*” OR “assess*” OR “valid*” OR “reproduct*” OR “feasab*” OR “measur*” AND “adolescent*” OR “child*” OR “young*” OR “school age” OR “school-aged” OR “youth”. The keywords were selected and defined by consensus from all authors. Furthermore, the reference lists of individual studies that reported results or used PF batteries in their methodologies but did not present the protocol were searched for records containing those protocols. Records identified through this method were added as records identified through other sources.
Inclusion Criteria
This systematic review includes scientific articles from peer-reviewed journals that contained PF battery protocols published until the 30th of April 2020. Only records presenting PF batteries comprising field-based health-related PF tests for children and adolescents that could be performed in the school setting were included. Thus, inclusion criteria were the following: (1) presenting results on the identification, structure, validity, reliability or feasibility of PF batteries, or parts of it (including specific tests), assessing health-related PF components in children and adolescents; (2) containing PF batteries comprising field-based tests that can be performed in the school setting; (3) having a cross-sectional, prospective, observational, experimental, or narrative review study design; (4) being written in English, French, German, Spanish, or Portuguese. Records presenting findings on motor skills, other populations that were not children or adolescents, or not meeting all inclusion criteria were excluded.
Data Extraction and Selection
The data extraction process was conducted based on PRISMA guidelines (19). After downloading the records from the databases to a reference managing software and integrating further records identified through other sources, duplicates were removed. Two authors (DHN and MP) screened the remaining records for title and abstract to identify studies that met the inclusion criteria. Relevant articles were retrieved for a full read. Then, the two authors reviewed the full text of potential studies, and decisions to include or exclude studies in the review were made by consensus. Disagreements were solved by consensus and, when necessary, a third reviewer served as a judge (AM). Agreement between reviewers was assessed using k statistics (k=0.96) for full-text screening and rating of relevance.
Data Analysis
Each identified PF battery was entered into a Microsoft Excel (Microsoft Corp., Redmond, Washington, DC, USA) spreadsheet, including information on author and year of publication; country; setting and age range of application; PF components assessed, and the PF tests used for each assessed component. The considered components of PF were body composition, CRF, upper body strength, lower body strength, middle-body strength, speed, agility, and flexibility. Also, a narrative synthesis was performed to describe each field-based health-related PF test in the identified PF batteries.
Results
Study Selection
A total of 10223 records (1506 from ASC; 167 from ERIC; 1559 from PubMed; 2610 from Scopus; 4358 from Web of Science; and 23 from other sources) were identified. After removing duplicates (n=5,838), 4,385 records were screened based on title and abstract, resulting in 4,154 records excluded. A total of 231 records were assessed for eligibility by full-text reads. Finally, 33 articles matched all inclusion criteria and were included in the qualitative synthesis. The flow chart of records selection is presented in Figure 1.
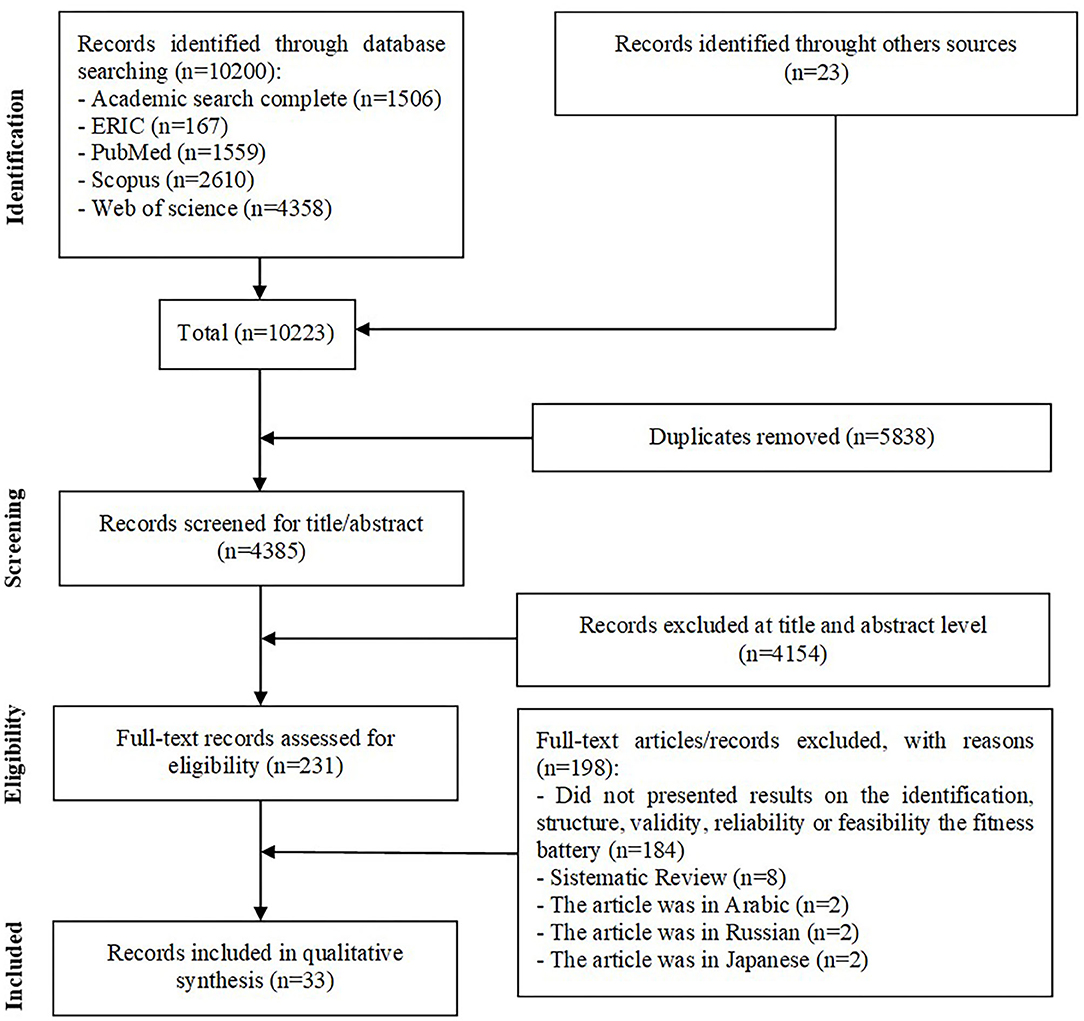
Figure 1. Flow diagram of study selection.
Summary of the Identified Physical Fitness Batteries
Table 1 presents a summary of the PF batteries identified in the included records, showing author, year, country, setting, age-range, and test for the following PF components: body composition, CRF, upper body, middle-body and lower body strength, endurance and power, speed, agility, and flexibility. From the 33 included records, 25 PF batteries were identified. Nine PF batteries were from America (six from the United States, two from Canada, one from Brazil) (20–28), nine were from Europe (two from the Czech Republic, one from each of the following countries Norway, Slovenia, Portugal, Italy, France, and Spain, one from the European Union) (15, 23, 24, 27, 28, 30, 32, 41, 42), four were from Asia (one from each of the following countries: Japan, Singapore, China, and Russia) (33, 34, 38, 40), two were from Oceania (one from Australia, one from New Zealand) (22, 36), and one from the Middle East (Bahrain) (31).
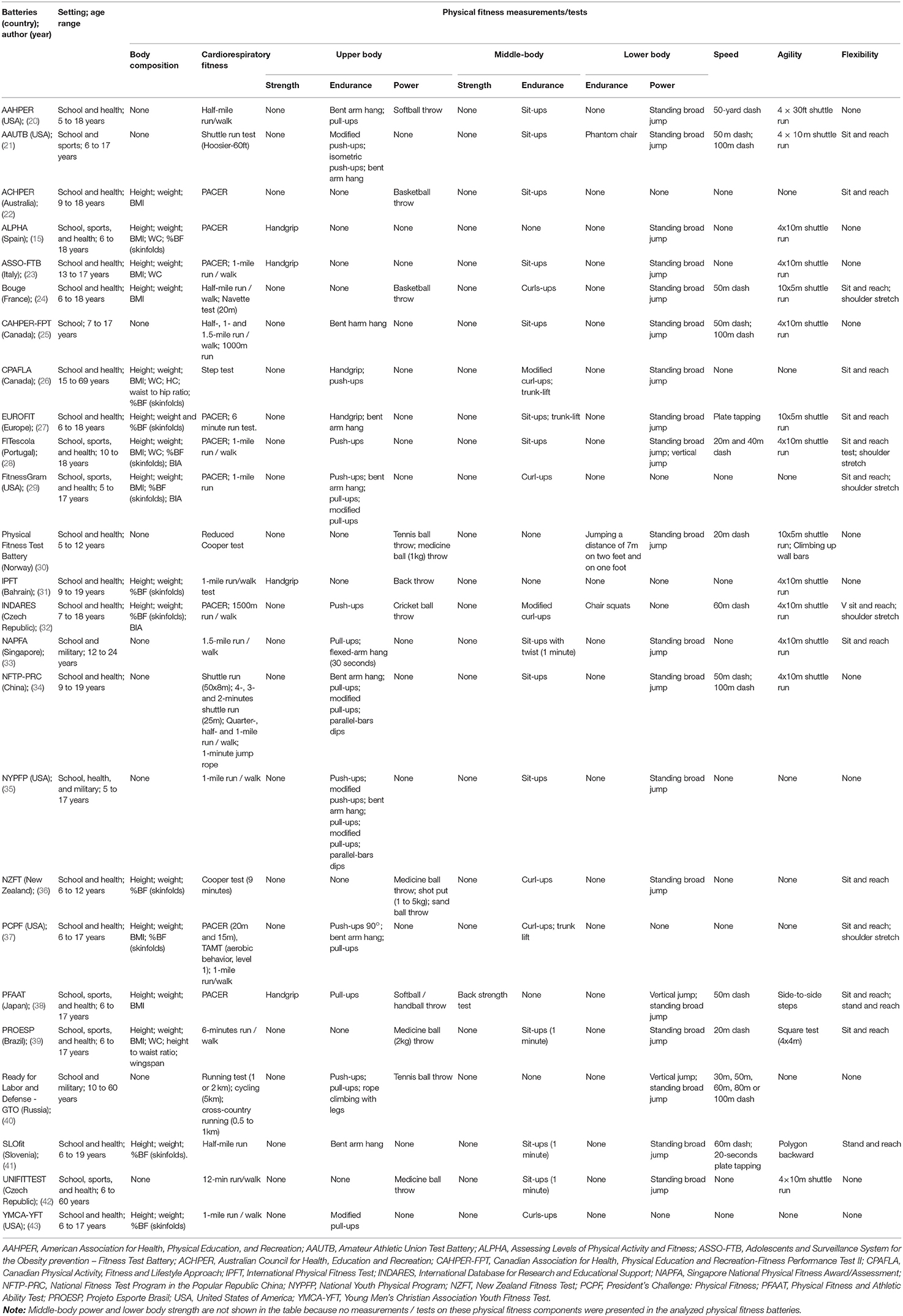
Table 1. Presentation and summary of the physical fitness batteries identified in the included records.
Most PF batteries (21 of 25) are exclusively for children and adolescents, while four of them are also extended to young adults (33) and adults (26, 40, 42). Also, even though all PF batteries can be performed in the school setting with the purpose of monitoring health-related indicators, some of them can be used in other settings such as sports and the army to assess physical performance. Two examples are the National Youth Physical Program from the United States Marines Youth Foundation (NYPFP) and the Ready for Labour and Defense (GTO) from Russia that is usually used to monitor PF for military purposes.
Regarding the PF components assessed in the batteries, only the CRF and the upper body strength, endurance and power were contemplated in all PF batteries. Middle-body and lower body strength, endurance and power were presented in most of the PF batteries, 21 of 25 and 20 of 25, respectively. Other components as agility (17 of 25) and body composition (16 of 25) were also contemplated in most PF batteries, although to a lesser extent. Flexibility (14 of 25) and speed (13 of 25) were the PF components less represented in the batteries, notwithstanding they were present in at least 50% of the identified PF batteries.
Among 25 identified PF batteries, a total of 87 PF tests, assessing the different PF components, were encountered. The PF component with the widest variety of different tests, that is, with 23, was CRF. It was followed by upper body strength, endurance and power with 21, speed with 10, middle-body strength and endurance with nine, body composition with eight, agility with seven, lower body endurance and power with five and flexibility with four different tests.
Discussion
This systematic review provides a summary of existent PF batteries from around the world containing field-based health-related tests that can be performed by children and adolescents and used to monitor health status. A total of 25 different PF batteries from European, American, Asian, and Oceanian countries were identified. This knowledge can be useful for selecting standardized and validated PF tests and batteries, adjusted for the school setting and considering different PF components, and simultaneously, allows direct comparison between peers of the same age from different geographic locations.
Among children and adolescents, PF is associated with numerous health indicators, thus assessing PF has been suggested to be a reliable tool to monitor health in youth (1). Furthermore, PF batteries are considered a valid, simple, precise, and low-cost health monitoring tool (44). Given that in several countries, such as Australia, Bahrain, Brazil, Canada, Czech Republic, China, France, Italy, Japan, Norway, Portugal, New Zealand, Russia, Singapore, Slovenia, Spain, and the USA, the military, sport, health, and education sectors have been implementing and using PF batteries. Findings from this review corroborate the popularity of PF assessments, once 25 PF batteries from four different continents were identified.
Being a multi-component construct, examining PF as a whole, using only one or two tests is a misconception, as different associations between PF components and health indicators are observed (1, 45). Because of that, the existence of detailed PF batteries is of importance. Such batteries allow taking into account a cluster of PF tests that are validated for each PF component, and that together it is possible to monitor complementing indicators of health and vulnerability. In this review, body composition, CRF, and muscular fitness (MF) were identified as the components of PF most frequently assessed in PF batteries.
Assessing body composition is usually the result of different anthropometric measures and their relation, such as height, weight, or waist circumference, as well as methodologies to analyse the % of body fat, muscle mass, and hydration (44). The measures of body composition, used in PF batteries, identified in this review were BMI, waist circumference, % of body fat (skinfolds), height to waist ratio, waist to hip ratio, wingspan, and bioelectrical impedance analysis. Requiring only height and weight, the BMI is a non-invasive, inexpensive, practical, and a largely applicable anthropometric indicator of obesity (48, 49). On the other hand, BMI does not differentiate fat mass from lean mass and is thus an insufficient indicator of body fat or abdominal adiposity (50). In this line, to avoid misclassifications international experts have been suggesting waist circumference, which is a better indicator of central adiposity, as an alternative to BMI (50, 51). More precise measures of body composition, namely the % of body fat were also present in some batteries, assessed by skinfolds or bioelectrical impedance analysis. Skinfolds allow calculating the % of fat mass and fat-free mass, through specific equations and are a low-cost methodology but specific and intensive training is required to minimize potential measurement error (52). Bioelectrical impedance analysis is more precise and allows to examine the % of fat mass, muscle mass or hydration status, however, it requires specific equipment, individual calibration and is more difficult to operationalize (53).
The CRF is the most studied component of PF among children and adolescents (54), and not surprisingly was assessed in each of the PF batteries identified in this systematic review. Higher levels of CRF are associated with a lower risk of several health outcomes, namely obesity, cardiovascular diseases, and mental health (1). The importance of assessing CRF was also reflected in a large number of tests observed, and among these tests, the PACER and the 1-mile run/walk seemed to be present in the most PF batteries. Both, the PACER and 1-mile run /walk are widely validated and reliable for assessing the CRF in young populations (15, 55). From these test results, maximum aerobic capacity can be estimated. From all equations to estimate maximum aerobic capacity through these field-based PF tests, the equations proposed by Cureton et al. (56) for the 1-mile run/walk test and Barnet et al. (57) for the PACER had the strongest evidence of validity with Léger equation (56–59). However, recently some issues have been raised regarding the estimation of maximum aerobic capacity considering that a multitude of factors (e.g., sex, adiposity) have an influence, emphasizing that estimations should be carefully interpreted to avoid misconceptions (60–62). Also, using test results in terms of the number of laps, stages, or time may provide a clearer picture of the individual's CRF.
Muscular fitness, another important PF component, was also assessed in each of the PF batteries identified. However, different components of MF (i.e., upper body, middle-body and lower body strength, endurance and power, agility, speed, and flexibility) were assessed across the batteries. Similar to CRF, MF is also associated with several health outcomes in youth (45, 46). A total of 56 different tests to assess the several components of MF were identified. For the upper body, the most common tests were the handgrip, push-ups or bent arm hang test, which assessed endurance and power. Regarding the lower body, the standing broad jump and the vertical jump, both assessing power, were the most usual tests. Lastly, for the middle-body, curl-ups and sit-ups were the most common tests, assessing endurance. Most of these tests require minimum equipment and are easily applied within a school or class setting. Agility, speed, and flexibility were present in fewer PF batteries than the other components of muscular fitness. This may be because there is more evidence observing the associations of lower, upper, and middle body strength with health indicators (47).
A total of 25 PF batteries were identified in this systematic review and across them 87 different PF tests for body composition, CRF, and MF. A previous systematic review focused on PF tests indicated that the PACER (or 20-meter shuttle run), the handgrip strength and standing broad jump tests, the 4 × 10m shuttle run test, weight, BMI, skinfolds, circumferences, and % body fat estimated from skinfold thickness were the most reliable field-based PF tests for children and adolescents (63). In this review, the aforementioned tests are among the most used in the identified PF batteries, which also corroborates previous research on this topic (17). Notwithstanding, when selecting a measurement/ protocol test of body composition, CRF or MF to perform factors such as staff training, equipment cost and time should be considered, as they heavily influence data collection, validity, and feasibility. Also, to avoid data contamination and misinterpretations, all protocols should be clear and performed by trained personnel, such as physical education teachers and other specialists (44). Despite being beyond the scope of this paper, it is important to acknowledge that physical education, sport, and health professionals should have a pedagogical approach in the application of PF batteries. This means that the application of the PF batteries must be aligned with the promotion of meaningful, relevant, and positive experiences for children and adolescents (64).
This systematic review is not without some limitations. Firstly, the large number of articles and protocols for the same PF test may have resulted in an overlap of tests. Secondly, the terms selected to identify investigations and other documents describing the PF batteries, although highly thorough nevertheless may have excluded documents not matching the inclusion criteria. Also, the search was conducted in only five databases. Lastly, because of the different study designs and the integration of gray literature (not following a scientific structure, such as protocols) the risk of bias and study quality assessment was unfeasible. Yet, most importantly, the major strength of this review is the ample number of articles reviewed and time interval search, which resulted in the identification of a rich set of PF batteries from around the globe.
Conclusion
The advances in the PF field-based assessment on school settings and health in youth resulted in the amplification of the number of existing batteries. On the one hand, diversity allows choosing the battery that most fits the specific purpose and setting of the assessment. On the other hand, it somehow complicates the comparability of data from different contexts, countries, or regions. Therefore, considering the connection between PF and health and the opportunity that the school setting provides to assess fitness in children and adolescents, we highlight the need for standardization and a consensus of PF assessments in this specific setting. In the European Union, a unique and actualized European PF battery would allow comparisons between European children and adolescents from different countries, to contribute to adequate and specific education and health public policies in the future.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Author Contributions
AM and MP: conception and design and drafting the manuscript. DH-N, MP, JM, and FG: data acquisition. AM, SP, and BM: data analysis and interpretation. YD, AS, JM, DH-N, and AI: critical revision for intellectual content. DH-N and FG: administrative, technical or material support. All authors read and approved the final manuscript.
Funding
This work was supported by the Swiss National Centre of Competence in Research LIVES – Overcoming vulnerability: life course perspectives, granted by the Swiss National Science Foundation (grant number: 51NF40-185901). AI acknowledges support from the Swiss National Science Foundation (grant number: 10001C_189407). The funder had no role in the collection of data, their analysis and interpretation, and in the right to approve or disapprove publication of the finished manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Ortega FB, Ruiz JR, Castillo MJ, Sjostrom M. Physical fitness in childhood and adolescence: a powerful marker of health. Int J Obes. (2008) 32:1–11. doi: 10.1038/sj.ijo.0803774
3. Spini D, Bernardi L, Oris M. Toward a Life Course Framework for Studying Vulnerability. Research in Human Development. (2017) 14:5–25. doi: 10.1080/15427609.2016.1268892
4. Ihle A, Gouveia ER, Gouveia BR, Freitas DL, Jurema J, Odim AP, et al. The relation of education, occupation, and cognitive activity to cognitive status in old age: the role of physical frailty. Int Psychogeriatr. (2017) 29:1469–74. doi: 10.1017/S1041610217000795
5. Ihle A, Gouveia ER, Gouveia BR, Freitas DL, Jurema J, Ornelas RT, et al. The relation of education and cognitive activity to mini-mental state in old age: the role of functional fitness status. Eur J Ageing. (2018) 15:123–31. doi: 10.1007/s10433-017-0441-4
6. Gouveia ER, Gouveia BR, Marques A, Lopes H, Rodrigues A, Peralta M, et al. Physical Fitness Predicts Subsequent Improvement in Academic Achievement: Differential Patterns Depending on Pupils' Age. Sustainability. (2020) 12. Artn 8874 10.3390/Su12218874
7. Yan X, Papadimitriou I, Lidor R, Eynon N. Nature versus Nurture in Determining Athletic Ability. Genet Sports. (2016) 61:15–28. doi: 10.1159/000445238
8. Ahmetov II, Fedotovskaya ON. Sports genomics: current state of knowledge and future directions. Cell Mol Exerc Physiol. (2012) 1. doi: 10.7457/cmep.v1i1.e1
9. Freitas D, Maia J, Beunen G, Claessens A, Thomis M, Marques A, et al. Socio-economic status, growth, physical activity and fitness: The Madeira Growth Study. Ann Hum Biol. (2009) 34:107–22. doi: 10.1080/03014460601080983
10. Sheldon SH. The function, phylogeny and ontogeny of sleep. In: Sheldon S, Ferber R, Kryger M, Gozal D, editors. Principles and Practice of Pediatric Sleep Medicine. Philadelphia, PA: Content Repository Only (2014). p. 3–11.
11. Bergeron MF, Mountjoy M, Armstrong N, Chia M, Côté J, Emery CA, et al. International Olympic Committee consensus statement on youth athletic development. Br J Sports Med. (2015) 49:843–51. doi: 10.1136/bjsports-2015-094962
12. Schutte N, Bartels M, Geus E. Genetics of physical activity and physical fitness. In: Armstrong N, Van Mechelen W, editors. Oxford Textbook of Children's Sport and Exercise Medicine. 3 ed. Oxford: Oxford University Press (2017). p. 293–302.
13. Ortega FB, Ruiz JR, Castillo MJ. Physical activity, physical fitness, and overweight in children and adolescents: Evidence from epidemiologic studies. Endocrinol Nutr. (2013) 60:458–69. doi: 10.1016/j.endoen.2013.10.007
14. Tayo BO, Li Y, Zou Z, Luo J, Ma J, Ma Y, et al. The predictive value of anthropometric indices for cardiometabolic risk factors in Chinese children and adolescents: a national multicenter school-based study. Plos ONE. (2020) 15:e0227954. doi: 10.1371/journal.pone.0227954
15. Ortega FB, Artero EG, Ruiz JR, Vicente-Rodriguez G, Bergman P, Hagstromer M, et al. Reliability of health-related physical fitness tests in European adolescents. The HELENA Study Int J Obes. (2008) 32:S49–S57. doi: 10.1038/ijo.2008.183
16. Castro-Pinero J, Artero EG, Espana-Romero V, Ortega FB, Sjostrom M, Suni J, et al. Criterion-related validity of field-based fitness tests in youth: a systematic review. Br J Sports Med. (2010) 44:934–43. doi: 10.1136/bjsm.2009.058321
17. Bianco A, Jemni M, Thomas E, Patti A, Paoli A, Ramos Roque J, et al. A systematic review to determine reliability and usefulness of the field-based test batteries for the assessment of physical fitness in adolescents—The ASSO Project. Int J Occup Med Environ Health. (2015) 28:445–78. doi: 10.13075/ijomeh.1896.00393
18. Tabacchi G, Lopez Sanchez GF, Nese Sahin F, Kizilyalli M, Genchi R, Basile M, et al. Field-Based Tests for the Assessment of Physical Fitness in Children and Adolescents Practicing Sport: A Systematic Review within the ESA Program. Sustainability. (2019) 11. doi: 10.3390/su11247187
19. Moher D. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann Intern Med. (2009) 151:264. doi: 10.7326/0003-4819-151-4-200908180-00135
20. Hunsicker P, Reiff G. AAPHER Youth Fitness Test Manual. Washington, DC: American Alliance for Health, Physical Education, and Recreation (1976).
21. Chrysler Corporation AAU. 1992–93 Testing Packet: Chrysler Fund-AAU Physical Fitness Program. Bloomington, IN: Amateur Athletic Union (1993).
22. Walkley J, ACHPER ACC. Australian Fitness Education Award. Hindmarsh, SA: Australian Council for Health, Physical Education and Recreation (1988).
23. Bianco A, Mammina C, Jemni M, Filippi AR, Patti A, Thomas E, et al. A Fitness Index model for Italian adolescents living in Southern Italy: the ASSO project. J Sports Med Phys Fit. (2016) 56:1279–88.
24. Vanhelst J, Béghin L, Czaplicki G, Ulmer Z. BOUGE-fitness test battery: Health-related field-based fitness tests assessment in children and adolescents. Revue Medicale de Bruxelles. (2014) 35:483–90.
25. CAHPER. The CAHPER Fitness-Performance Test Manual for Boys and Girls 7 to 17 Years of Age. Ottawa: Canadian Association for Health, Physical Education and Recreation (1966).
26. CSEP The Canadian Physical Activity Fitness and Lifestyle Approach (CPAFLA): CSEP—Health and Fitness Program's Health-Related Appraisal and Counselling Strategy. Canadian Society for Exercise Physiology (2003).
27. Lovecchio N, Bussetti M, Eid L. Flexibility and abdominal strength among young student: Eurofit protocol. Eur J Phys Health Educ. (2009) 1:19–24.
28. Henriques-Neto D, Minderico C, Peralta M, Marques A, Sardinha LB. Test–retest reliability of physical fitness tests among young athletes: The FITescola® battery. Clin Physiol Funct Imaging. (2020). doi: 10.1111/cpf.12624
29. Laurson KR, Saint-Maurice PF, Karsai I, Csányi T. Cross-validation of FITNESSGRAM® health-related fitness standards in Hungarian youth. Res Q Exerc Sport. (2015) 86:S13–S20. doi: 10.1080/02701367.2015.1042800
30. Fjortoft I, Pedersen AV, Sigmundsson H, Vereijken B. Measuring physical fitness in children who are 5 to 12 years old with a test battery that is functional and easy to administer. Phys Ther. (2011) 91:1087–95. doi: 10.2522/ptj.20090350
32. Chmelík F, Frömel K, Kren F, Fical P. Indares.com: International database for research and educational support. Procedia - Social and Behavioral Sciences. (2013) 83:328–31. doi: 10.1016/j.sbspro.2013.06.064
34. Zhu Z, Yang Y, Kong Z, Zhang Y, Zhuang J. Prevalence of physical fitness in Chinese school-aged children: Findings from the 2016 Physical Activity and Fitness in China—The Youth Study. J Sport Health Sci. (2017) 6:395–403. doi: 10.1016/j.jshs.2017.09.003
35. Department of the Navy Marine Corps Physical Fitness Test and Body Composition Program Manual. D.o.t. Navy, editor. Washington, DC: Department of the Navy (2002).
36. Russell DG, Isaac A, Wilson PG. New Zealand Fitness Test Handbook. Wellington: Department of Education (1989).
37. Winnick J, Short F. Profile, Test Selection Guides, Standards, and Fitness Zones. In: Winnick J, Short F, editors. Brockport Physical Fitness Test Manual. Champaign, IL: Human Kinectis (2014).
38. Shingo N, Takeo M. The educational experiments of school health promotion for the youth in Japan: analysis of the 'sport test' over the past 34 years. Health Promot Int. (2002) 17:147–60. doi: 10.1093/heapro/17.2.147
39. Lima FEB, Coco MA, Pellegrinotti IL, Lima WF, Lima SB, Lima FB. Physical fitness related to motor performance and health of adolescents of the southwest region of the state of São Paulo and north pioneer of the state of Parana. Rbone-Revista Brasileira de Obesidade Nutricao e Emagrecimento. (2018) 12:908–19.
40. Howell R. The Soviet Physical Fitness Tests: An Essential Aspect of the Soviet organizational Plan. San Diego, CA: AAHPER (1976).
41. Jurak G, Kovac M, Sember V, Starc G. 30 years of SLOfit: Its legacy and perspective. Turk J Sports Med. (2019) 54:23–7. doi: 10.5152/tjsm.2019.148
42. Kopecky M, Kusnierz C, Kikalova K, Charamza J. Comparison of the somatic state and the level of motor performance of boys between the ages of seven and fifteen in the Olomouc region (Czech Republic) and in Opole (Poland). Acta Universitatis Palackianae Olomucensis Gymnica. (2013) 43:53–65. doi: 10.5507/ag.2013.024
44. Pate R, Oria M, Pillsbury L. Fitness Measures and Health Outcomes in Youth. Washington, DC: National Academies Press (2012).
45. Garcia-Hermoso A, Ramirez-Campillo R, Izquierdo M. Is Muscular Fitness Associated with Future Health Benefits in Children and Adolescents? A Systematic Review and Meta-Analysis of Longitudinal Studies. Sports Med. (2019) 49:1079–94. doi: 10.1007/s40279-019-01098-6
46. Petrigna L, Karsten B, Marcolin G, Paoli A, D'Antona G, Palma A, et al. A Review of Countermovement and Squat Jump Testing Methods in the Context of Public Health Examination in Adolescence: Reliability and Feasibility of Current Testing Procedures. Front Physiol. (2019) 10:1384. doi: 10.3389/fphys.2019.01384
47. Smith JJ, Eather N, Morgan PJ, Plotnikoff RC, Faigenbaum AD, Lubans DR. The health benefits of muscular fitness for children and adolescents: a systematic review and meta-analysis. Sports Med. (2014) 44:1209–23. doi: 10.1007/s40279-014-0196-4
48. de Onis M, Lobstein T. Defining obesity risk status in the general childhood population: which cut-offs should we use? Int J Pediatr Obes. (2010) 5:458–60. doi: 10.3109/17477161003615583
49. Grossman D, Bibbins-Domingo K, Curry S, Barry MJ, Davidson K, Doubeni C, et al. Screening for obesity in children and adolescents: US Preventive Services Task Force recommendation statement. J Am Med Assoc. (2017) 317:2417–26. doi: 10.1001/jama.2017.6803
50. Ross R, Neeland IJ, Yamashita S, Shai I, Seidell J, Magni P, et al. Waist circumference as a vital sign in clinical practice: a Consensus Statement from the IAS and ICCR Working Group on Visceral Obesity. Nat Rev Endocrinol. (2020) 16:177–89. doi: 10.1038/s41574-019-0310-7
51. Bovet P, Magnussen CG, Zhao M, Dwyer T, Venn AJ, Khadilkar V, et al. International Waist Circumference Percentile Cutoffs for Central Obesity in Children and Adolescents Aged 6 to 18 Years. J Clin Endocrinol Metab. (2020) 105:e1569–e1583. doi: 10.1210/clinem/dgz195
52. Moreno LA, Joyanes M, Mesana M, González-Gross M, Gil CM, Sarría A, et al. Harmonization of anthropometric measurements for a multicenter nutrition survey in Spanish adolescents. Nutrition. (2003) 19:481–6. doi: 10.1016/s0899-9007(03)00040-6
53. Dehghan M, Merchant AT. Is bioelectrical impedance accurate for use in large epidemiological studies? Nutr J. (2008) 7:26. doi: 10.1186/1475-2891-7-26
54. Falk B, Klentrou P, Armstrong N, Rowland T, Kemper H. A Brief History of Pediatric Exercise Physiology. Pediatr Exerc Sci. (2018) 30:1–10. doi: 10.1123/pes.2017-0246
55. Castro-Piñero J, Mora J, Gonzalez-Montesinos JL, Sjöström M, Ruiz JR. Criterion-related validity of the one-mile run/walk test in children aged 8–17 years. J Sports Sci. (2009) 27:405–13. doi: 10.1080/02640410802603889
56. Cureton KJ, Sloniger MA, O'Bannon JP, Black DM, McCormack WP. A generalized equation for prediction of VO2peak from 1-mile run/walk performance. Med Sci Sports Exerc. (1995) 27:445–51.
57. Barnett A, Chan L, Bruce L. A preliminary study of the 20-m multistage shuttle run as a predictor of peak VO2 in Hong Kong Chinese students. Pediatr Exerc Sci. (1993) 5:42–50. doi: 10.1123/pes.5.1.42
58. Léger LA, Mercier D, Gadoury C, Lambert J. The multistage 20 metre shuttle run test for aerobic fitness. J Sports Sci. (1988) 6:93–101. doi: 10.1080/02640418808729800
59. Batista MB, Romanzini CLP, Castro-Piñero J, Ronque E. Validade de testes de campo para estimativa da aptidão cardiorrespiratória em crianças e adolescentes: uma revisão sistemática. Revista Paulista de Pediatria. (2017) 35:222–33. doi: 10.1590/1984-0462/;2017;35;2;00002
60. Armstrong N, Welsman J. Clarity and confusion in the development of youth aerobic fitness. Front Physiol. (2019) 10:979. doi: 10.3389/fphys.2019.00979
61. Armstrong N, Welsman J. Youth cardiorespiratory fitness: evidence, myths and misconceptions. Bull World Health Org. (2019) 97:777–82. doi: 10.2471/blt.18.227546
62. Welsman J, Armstrong N. Children's fitness and health: an epic scandal of poor methodology, inappropriate statistics, questionable editorial practices and a generation of misinformation. BMJ Evid Based Med. (2019) 26:12–3. doi: 10.1136/bmjebm-2019-111232
63. Artero EG, Espana-Romero V, Castro-Pinero J, Ortega FB, Suni J, Castillo-Garzon MJ, et al. Reliability of field-based fitness tests in youth. Int J Sports Med. (2011) 32:159–69. doi: 10.1055/s-0030-1268488
Keywords: body composition, cardiorespirarory fitness, fitness testing, musculoskeletal, physical education, vulnerability
Citation: Marques A, Henriques-Neto D, Peralta M, Martins J, Gomes F, Popovic S, Masanovic B, Demetriou Y, Schlund A and Ihle A (2021) Field-Based Health-Related Physical Fitness Tests in Children and Adolescents: A Systematic Review. Front. Pediatr. 9:640028. doi: 10.3389/fped.2021.640028
Received: 10 December 2020; Accepted: 15 February 2021;
Published: 05 March 2021.
Edited by:
Antonino Bianco, University of Palermo, ItalyReviewed by:
Brigita Mieziene, Lithuanian Sports University, LithuaniaVedrana Sember, University of Ljubljana, Slovenia
Dario Novak, University of Zagreb, Croatia
Copyright © 2021 Marques, Henriques-Neto, Peralta, Martins, Gomes, Popovic, Masanovic, Demetriou, Schlund and Ihle. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Miguel Peralta, mperalta@fmh.ulisboa.pt