 Anita J. W. M. Brouns1,2
Anita J. W. M. Brouns1,2 Ben H. De Bie3
Ben H. De Bie3 Marieke H. J. van den Beuken-van Everdingen4
Marieke H. J. van den Beuken-van Everdingen4 Anne-Marie C. Dingemans2,5
Anne-Marie C. Dingemans2,5 Lizza E. L. Hendriks2*
Lizza E. L. Hendriks2*- 1Department of Pulmonary Diseases, Zuyderland Medical Center, Sittard-Geleen, Netherlands
- 2Department of Pulmonary Diseases, GROW—School for Oncology and Developmental Biology, Maastricht University Medical Center+ (MUMC+), Maastricht, Netherlands
- 3Department of Anesthesiology, Maastricht University Medical Center+ (MUMC+), Maastricht, Netherlands
- 4Centre of Expertise for Palliative Care, Maastricht University Medical Center+ (MUMC+), Maastricht, Netherlands
- 5Department of Pulmonary Diseases, Erasmus MC, Rotterdam, Netherlands
Introduction: Cancer induced bone pain (CIBP) is frequent in patients with non-small cell lung cancer (NSCLC). Radiation therapy continues to be the gold standard for treatment of painful bone metastases, however only a limited number of metastases can be irradiated. We evaluated non-radiation based early CIBP relief options in NSCLC through a systematic review.
Methods: Systematic review including all prospective articles published between 01-1994 and 06-2020 on Pubmed, Cochrane Library and ClinicalTrials.gov database. Inclusion: non-radiation based trials evaluating CIBP early pain relief options (initially defined as pain score evaluated within two weeks, because of no randomized trials, later inclusion broadened to pain score evaluated within six weeks) in ≥10 NSCLC patients. Radioisotope trials were excluded as these treatments have interactions with systemic anticancer therapy.
Results: 188 articles were found; 10 articles (6 randomized controlled (4 double blinded), 1 phase II single-arm, and 3 prospective trials) fulfilled the inclusion criteria. Six of these trials consisted of ≥2 treatment arms, whereas the others were single-arm studies. In total, 554 NSCLC patients were evaluated in these trials. The included trials were very heterogeneous regarding evaluated treatment options, methods of pain measuring, and endpoints. No high-level evidence for specific early pain relief treatment options was found.
Discussion: Non-radiation based studies evaluating treatment options to rapidly reduce CIBP in NSCLC are scarce. This systematic review shows that there is no high-level evidence to recommend a specific treatment for early pain relief. Future research should focus on early pain relief treatment options for CIBP in NSCLC.
Introduction
Bone metastases are diagnosed in 24%–70% of patients with non-small cell lung cancer (NSCLC) during the course of the disease (1–3). Up to 80% of these patients experience cancer induced bone pain (CIBP) (4). Unfortunately, scarce data is available describing the severity of bone pain in patients with lung cancer; only the incidence of bone pain or usage of analgesics is reported (1–3, 5). In about one fifth of the patients, Quality of Life (QoL) worsens after a diagnosis of bone metastases (6). Furthermore, bone metastases are associated with lower overall survival (OS) (6).
Tumor invasion into bone causes osteoclast and osteoblast recruitment and modulation of genes and proteins involved in the bone microenvironment. Numerous factors are involved in the process of bone pain such as nociceptor activation and sensitization, ectopic sprouting of nerve fibers and central sensitization in the spinal cord and brain. Without treatment of the underlying disease and/or local treatment, no bone healing occurs in bone metastases, leading to a vicious circle of CIBP, central sensitization resulting in more pain, and the development of chronic bone pain (7). Therefore, early pain reduction is important.
Due to the high incidence, chronic character, and negative impact on QoL and OS, CIBP is an important issue that needs to be addressed in metastatic NSCLC. According to the World Health Organization (WHO) pain ladder, (bone) pain should first be treated with paracetamol and/or non-steroidal anti-inflammatory drugs (NSAIDs), followed if necessary by adding mild, and later strong opioids (8). The extended use of NSAIDs and opioids is associated with unwanted side effects (e.g., renal, hepatic or gastro-intestinal) (7). Especially in the older population (i.e., most patients with lung cancer), opioids can lead to neurological complaints such as dizziness or cognitive clouding, which in turn increases the likelihood of falling with the risk of for example bone fractures (7). Furthermore, several patients are reluctant to take opioids because of fear to become addicted, or because of the side effects (9). Radiotherapy is another effective treatment strategy for bone pain with a complete pain resolution in approximately 50% of the patients (10). Drawbacks of radiotherapy as treatment option are the time delay, as it takes up to 6 weeks before a maximum treatment effect is obtained (although ≥50% of responders have benefit within 1–2 weeks) and a frequently occurring pain flare-up in the first week after radiotherapy (10, 11). In addition, radiotherapy is only feasible in patients with a limited number of painful bone metastases.
The European Society for Medical Oncology (ESMO) guideline on metastatic NSCLC (2018) recommends denosumab or zoledronic acid in patients with NSCLC and bone metastases considered at high risk for skeletal related events (SREs) and with a life expectancy of >3 months (level of evidence I, grade of recommendation B) (12). This recommendation is based on the observation that bone targeted agents reduce SREs. Of note, pain scores are not included in the definition of SRE, although necessity for radiation because of painful bone metastases is included. For denosumab it was found that in patients with bone metastases and no/mild baseline CIBP, time to pain interference with daily life was longer compared with zoledronic acid. The ESMO advice is based on randomized phase III trials that included solid tumors (approximately 50% NSCLC) and early pain relief was not a primary objective of these trials (12). Trials including patients with bone metastases from prostate- or breast- or lung cancer (N=607 of which 1 NSCLC), which evaluated the effect of ibandronate (intravenous or oral) on bone pain showed pain relief within seven days after start of ibandronate (13–15). However, most of the patients received concomitant antineoplastic treatment, therefore a pain relief effect of the systemic anti-cancer therapy cannot be excluded and is it difficult to evaluate the therapeutic effect on CIBP of bisphosphonate therapy alone.
The ESMO guideline on bone health in patients with cancer (2020) states that multidisciplinary management (e.g., systemic treatments, radiation therapy, surgery and supportive care) is needed for effective treatment of metastatic bone disease. They suggest radiotherapy as treatment of choice in localized CIBP, but no specific treatment recommendations are made for diffuse CIBP (10). The National Comprehensive Cancer Network (NCCN) guideline on NSCLC and National Institute for Health and Care Excellence (NICE) flowcharts on lung cancer mention radiotherapy as pain relief option in CIBP (16, 17).
Survival is improving in patients with NSCLC, partly because of the survival benefit seen with immune checkpoint inhibitors for a large proportion of patients and partly due to the availability of tyrosine kinase inhibitors for the group of patients with an oncogenic driver. As it is possible that these patients live longer with CIBP, effective, preferably early pain reducing treatments might be more relevant. We performed a systematic review specifically focusing on early non-radiation based pain relief options for NSCLC patients with CIBP.
Materials and Methods
Search Strategy and Selection Criteria
A systematic search of the literature published between January 1994 and June 2020 was performed using the PubMed, the Cochrane Library and the ClinicalTrials.gov database. Published studies were identified using a search strategy based on the Patient-Intervention-Control-Outcome (PICO) method (shown in Table 1 in the Supplementary Material) (18). PRISMA 2009 checklist for systematic reviews is shown in Table 3 in the Supplemental Material. Our clinical question was to assess the efficacy of CIBP relief treatment options in patients with NSCLC. Initially, we defined early pain relief as pain reduction within two weeks. As we identified only one trial, and to be as inclusive as possible, we expanded the time to six weeks because in this period the maximum effect of radiotherapy occurs. We excluded radiotherapy because of the aforementioned drawbacks, and radioisotopes since the possible interaction with systemic treatment which is the mainstay of treatment for the majority of patients with NSCLC (19). The main inclusion criteria were 1) prospective trials focusing on treatment options for early pain relief, 2) inclusion of a minimum of 10 patients with NSCLC and with at least one bone metastasis. All inclusion criteria for this systematic review are summarized in Table 2 in the Supplementary Material.
Study Selection
Two authors (AB and BB) independently screened the titles of the selected studies and subsequently the abstracts of the eligible studies. The same authors independently examined the full texts of the selected articles regarding the inclusion criteria. Studies were included if they met the eligibility criteria. To complete the search, the references of all eligible articles were manually searched for additional relevant articles. Also, the excluded review articles were screened for relevant studies which were not represented in the original search. The entire search and selection were independently checked by a third reviewer (LH). In case of disagreement during study inclusion, consensus was sought.
Data Selection
When available and applicable, the following data were extracted from eligible studies by one author (AB) and independently by another author (BB): year of publication, number of study arms, randomization method, duration of study and follow-up, histological diagnosis, intervention (i.e., type, dose, duration, route and frequency), method of pain score (e.g., bone pain inventory [BPI]), timing of pain score, efficacy of intervention on pain relief, whether results were specifically for NSCLC or for all included patients, and primary and secondary objectives of the trials. Final approval of the extracted data was performed by LH.
The Jadad scale was used to assess the methodological quality of the included trials (20). We did not perform a formal test of heterogeneity because of the heterogeneous type of trials included in the systemic review, with one third of the included trials being single arm (i.e., per definition high risk of bias).
Results
Study Selection
The literature search identified 186 articles in total without duplicates. As mentioned in the inclusion criteria, reviews were excluded in the search strategy, but to broaden the search results these reviews were manually searched for relevant studies. After checking the reference list of the reviews identified with the systematic search, 2 additional relevant articles were included. Of these 188 articles, 151 were excluded because of non-relevant titles. 18 of the 37 remaining articles were excluded because they did not fulfill the inclusion criteria based on the abstract. After screening of the full text of the remaining 19 articles, 14 articles were excluded because of: no answer on the clinical question (N = 4), radiotherapy as treatment modality (N = 1), radioisotopes as treatment modality (N = 1), retrospective study or case report (N = 2), and a language barrier (e.g., Chinese, Japanese or Serbian language, N = 6). After manual search of the reference list of included articles 5 other relevant articles were included. The flowchart for article selection is shown in Figure 1.
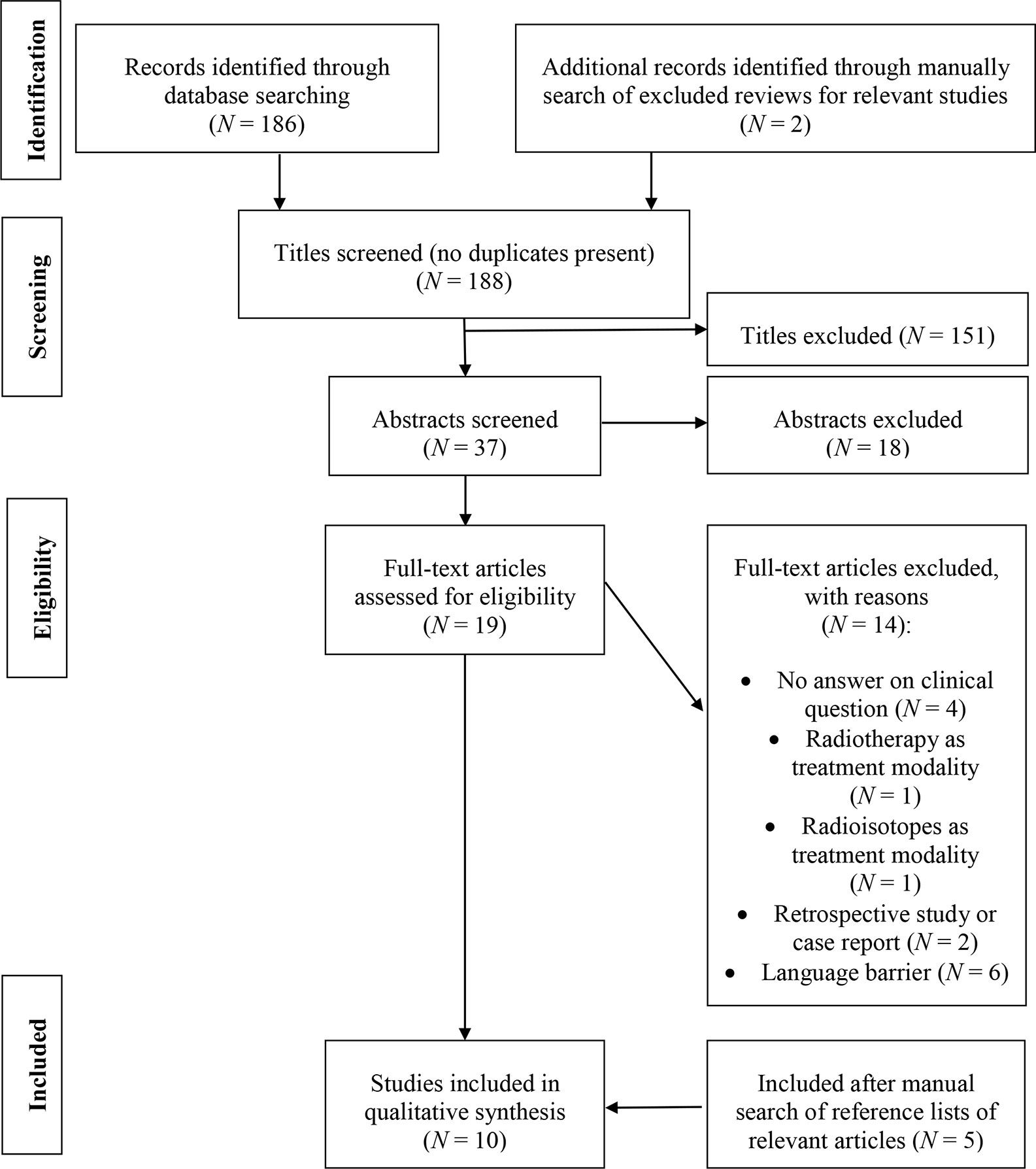
Figure 1 Flowchart for article selection.
Description of Studies
One phase II trial (21), six randomized controlled trials (22–27) and three other prospective series (28–30) were included in this review. The randomized controlled trials were double-blinded in four trials (24–27) (of which one was placebo-controlled) and open label in two (22, 23). Three studies were single-arm (21, 28, 29) six were 2-arm (22, 24–27, 30) and one 3-arm (23). In the study of Zarogoulidis et al., the selection was made on the presence of bone pain (30). The main characteristics of the included studies are shown in Table 1. Four studies included only patients with NSCLC, with a minimum of one bone metastasis (21, 22, 28, 30). The other studies included also patients with CIBP caused by bone metastases of solid malignancies (256 out of 978 patients in total had NSCLC) (23–27, 29). The number of patients with NSCLC enrolled in the studies ranged from 14 (24, 28) to 144 (30), leading to in total 554 patients with NSCLC included in this review. Only in five trials patients received pain modifying therapy alone (23–25, 27, 28), in all other trials, other anticancer treatment (mainly chemotherapy) was given (21, 22, 26, 29, 30). The inclusion criteria were quite similar across the included trials. The only difference was the treatment history of the patients, e.g., pre-treated with radiotherapy (28), chemonaïve (29) and presumably chemonaïve (22, 30) and pre-treated with chemotherapy and/or radiotherapy (21, 26). In the other trials, no information about previous therapy is provided (23–27). The exclusion criteria concerning comorbidities were comparable among eight studies (21–27, 29). In two other studies, no exclusion criteria were mentioned (28, 30).
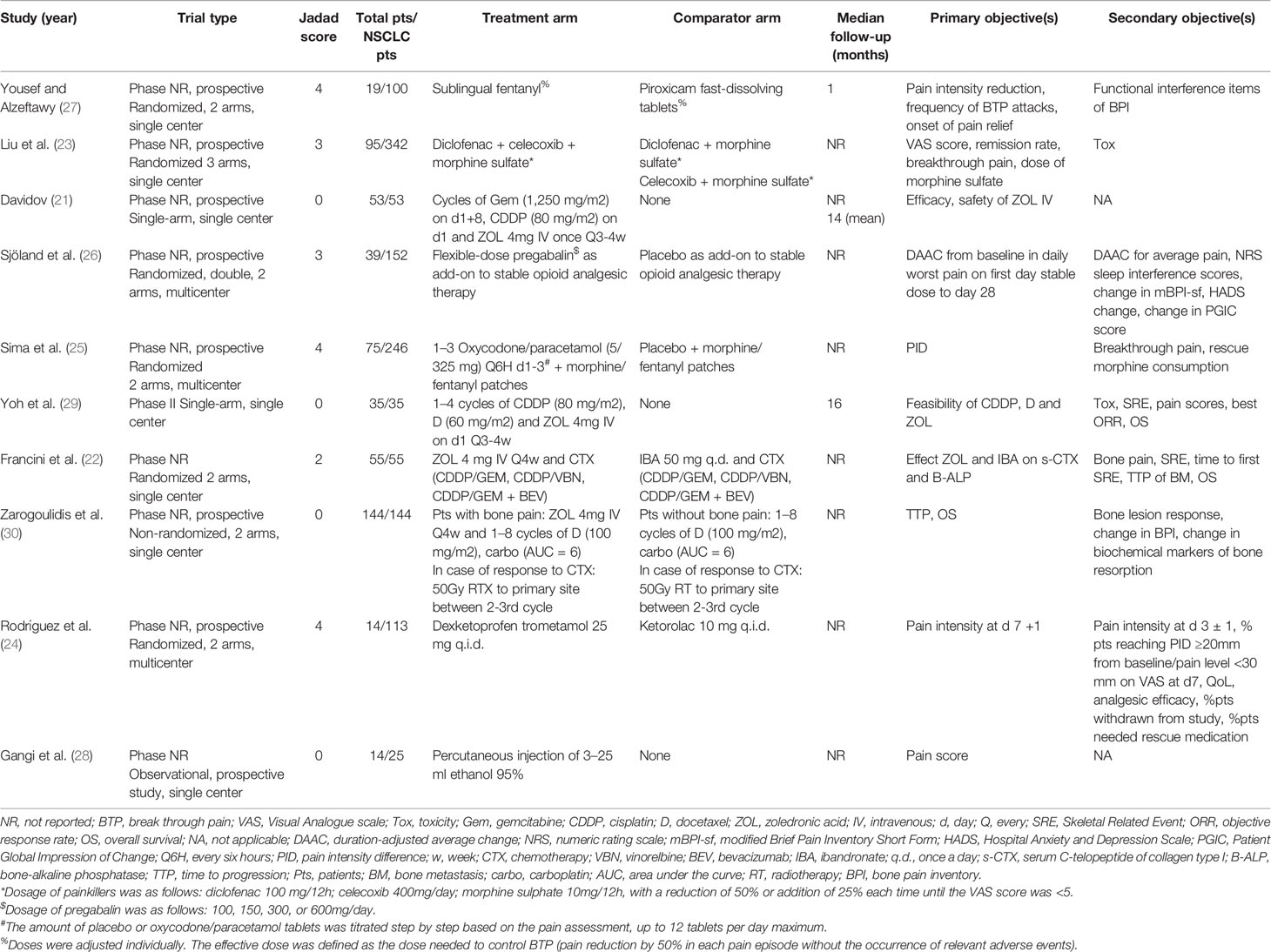
Table 1 Main characteristics of included studies.
The primary objectives of the included trials varied from efficacy and safety of combined treatment of chemotherapy and zoledronic acid (21, 29) effects of zoledronic acid on bone resorption or formation markers (22), efficacy of treatment on time to progression (TTP), OS (30), reduction in pain intensity (24–27), frequency of breakthrough pain (24, 27), remission rate (24), dose of morphine sulfate (24), and duration-adjusted average change (DAAC) from baseline in the daily NRS worst pain score (26). Six studies had (reduction in) pain score as primary or secondary objective (23–28). Three studies assessed bone pain or change in BPI from baseline as secondary objectives (22, 29, 30). The study of Davidov et al. measured pain scores as an exploratory objective (21). Table 1 provides a detailed summary of all outcome variables of the included studies.
Results of Individual Studies
Method and Timing of Pain Score
The studies of Yoh et al. and Zarogoulidis et al. used the BPI as method of measuring pain score (29, 30). In Zarogoulidis’s study, the BPI was scored each clinical visit (the interval between study visits was not further specified) (30), whereas in Yoh’s et al. study this assessment was performed at baseline and after six weeks of treatment (29). Three studies used the visual analogue scale (VAS) expressed in figures or millimeters as method of measuring pain score (23, 24, 27). The pain assessments took place within the first week of treatment (23, 24, 26, 27) till four weeks (23, 26, 27). Two other studies were not focused on a direct pain score, they evaluated pain response indirectly with the use of analgesics (21, 28). This was evaluated after one and three cycles of chemotherapy (e.g., first measurement at three-four weeks after start of anticancer treatment) (21) and within 48 h after the intervention with a re-evaluation after two weeks (28). One study used the McGill-Melzack pain score, which was performed at baseline and after one and three months of treatment (22). The numeric rating scale (NRS) as method of measuring pain score was used by two trials (25, 26), one double blind randomized trial only recorded till day three of treatment (25), whereas the other recorded daily till day 35. Details on methods and timing of pain score are in Table 2.
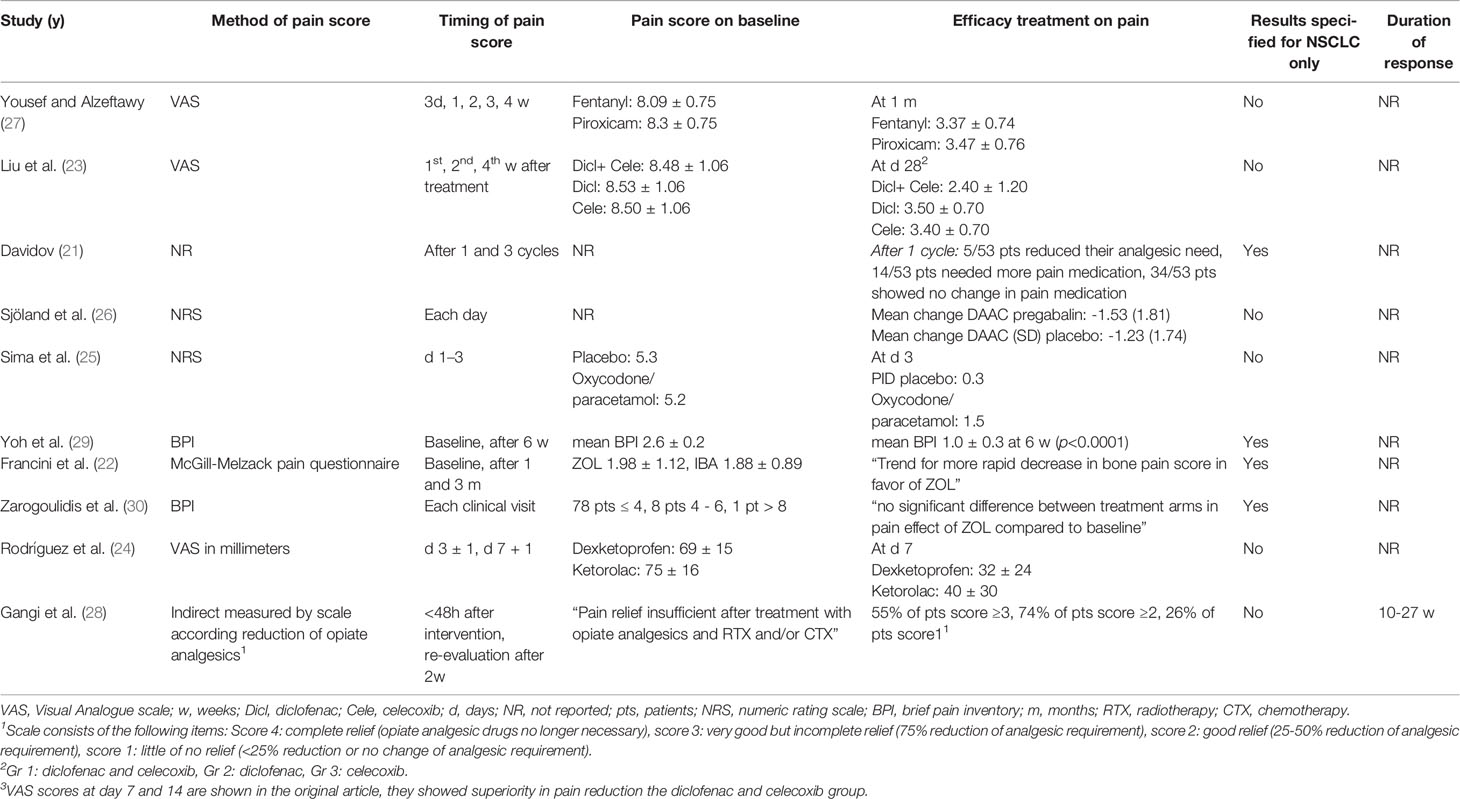
Table 2 Overview of reported items on early bone pain relief.
Efficacy of Treatment on Pain and Duration of Response
Five studies (including 217 patients with NSCLC, out of 554 patients included in total) showed a significant treatment effect on pain score (23–25, 27, 29). One double blind randomized controlled trial, including 14 patients with NSCLC out of 113 included patients (10%) evaluating dexketoprofen trometamol versus ketorolac showed superior of the former on pain rating index (secondary outcome, p = 0.04) (24). One open label, randomized controlled trial, showed that diclofenac combined with celecoxib and morphine sulfate was superiority to NSAID monotherapy combined with morphine sulfate in CIBP reduction, measured with VAS (average VAS score at 28 days: 2.40 ± 1.20 vs 3.50 ± 0.70 (diclofenac monotherapy plus morphine) or 3.40 ± 0.70 (celecoxib monotherapy plus morphine), p = 0.006) (23). Another double blind randomized controlled trial, including 75 patients with NSCLC out of 246 included patients (30%) showed an additional effect of the combination of short acting oxycodone/paracetamol versus placebo, added to standard long-acting opioids on reducing bone pain (pain intensity difference (PID) after three days in the placebo group 0.3, compared with 1.5 in the oxycodone/paracetamol group, p<0.001) (25). One, double blind randomized controlled, trial, including 19 patients with NSCLC out of 100 included patients (19%), evaluating fentanyl versus piroxicam for CIBP reduction, reported for both drugs a significant decrease in VAS score at 1 month. No significant difference in efficacy was found between the treatment arms (27). The only study with bisphosphonates, which found a significant effect of treatment on pain score was the single-arm study of Yoh et al. (29). They showed that treatment of both chemotherapy and zoledronic acid reduced pain score at six weeks compared to baseline. In another study, no significant difference in pain effect of zoledronic acid between the treatment arms (docetaxel and carboplatin +/- zoledronic acid) was observed (30). Another double blind randomized controlled trial, including 39 patients with NSCLC out of 152 included patients (26%), reported a non-significant effect of pregabalin treatment on pain compared placebo (DAAC from baseline in the daily NRS worst pain score -1.53 vs. -1.23). The study of Francini et al. showed a trend for more rapid decrease in bone pain score at one month in favor of zoledronic acid compared to oral ibandronate (22). Davidov et al. found only a reduced analgesic need in five out of 53 patients (10%), whereas most of the patients (34 out of 53 patients [64%]) had no change in pain medication after one treatment cycle (21). One study showed a reduction of minimal 25%–50% of analgesic requirement in 74% of the patients and 55% of the patients had a reduction of 75% of analgesic requirement after treatment with ethanol injections (28). The duration of treatment response was only reported in one study and was ten to 27 weeks (28).
Of note, none of the studies including patients with different primary tumor histologies reported results for the subgroup of patients with NSCLC. Table 2 provides an overview for reported items on bone pain relief.
Discussion
CIBP is a clinically relevant problem in metastatic NSCLC due to the high prevalence of bone metastases, the chronic character and the negative impact on QoL and OS (6). Survival is improving for NSCLC: five-year survival improved from 5% to 16%–31% for patients without targetable mutations, treated with immune checkpoint inhibitors and five-year survival rates are over 40% in patients with an EGFR mutation or ALK fusion (31–37). It is possible that some of these patients survive a prolonged time with CIBP that impairs QoL, making effective pain reducing strategies necessary.
To obtain more insight in possible treatment options for early pain relief in patients with NSCLC with bone metastases and CIBP, we performed a systematic review on this topic excluding radioisotopes and radiotherapy for the reasons mentioned above. The initial scope of this review was early pain relief (pain relief evaluated within two weeks of start of treatment), but this resulted in limited number of eligible trials. To be more inclusive, we broadened the time of “early pain relief” to a maximum of six weeks. Even then, only ten studies were eligible. Of note, the included trials were very heterogeneous regarding treatments evaluated, primary endpoints, methods of pain measurement and timing of assessment. Importantly, the randomized trials included patients with different histologies, and patients with NSCLC only comprised a subgroup in these randomized trials (554 [44%] of included patients). Importantly, not all treatments evaluated are comparable with recommended pain treatment in clinical guidelines. For example, according to international and national guidelines for breakthrough cancer pain, shorting-acting morphine should be added to standard dose long-acting morphine to treat breakthrough pain (38). Three of the included studies indeed underscore the importance of adding breakthrough medication to continuous release medication (23, 25, 27). As the comparator arms of these trials included a non-optimal treatment according to current guidelines, the results found in these trials have limited value in daily clinical practice. Another study excluded patients previously or currently treated with a scheduled regimen of painkillers, except acetaminophen and acetylsalicylic acid, which is also not according to the WHO pain ladder (8, 24).
In most other studies (21, 22, 29, 30), systemic therapy and pain relief therapy were administered concurrently, therefore conclusions on the specific efficacy of pain relief therapy were difficult as it cannot be excluded that the systemic therapy also causes a reduction in pain. For zoledronic acid, only one study showed an early pain reduction, but this pain reduction disappeared at three months despite continuous bone targeted agent use (22). While out of the scope of this review, information on long-term pain reduction is also particularly important. Only two studies provided follow-up of more than one year (21, 29). As CIBP is a chronic problem, it is also of interest to know information about the pain efficacy in the long term. However, only the studies of Davidov and Yoh had a follow-up of more than a year (21, 29). Duration of pain response and the recurrence rate of CIBP was lacking.
What are other possible treatment options for CIBP in NSCLC? The first step to achieve early pain relief in CIBP is analgesics according the WHO pain ladder (8). This advice is based on general pain management recommendations for patients with cancer. As was found in this review, opioids are indeed effective in the treatment of CIBP. Palliative radiotherapy is frequently used in the treatment of CIBP, because of the high response rate (around 85%). Drawbacks are the possibility of a pain flare-up and the limited use in multiple painful bone metastases (10). Besides that there are disparities in the access to radiotherapy facilities in high and low-income countries. For example, in Central Africa 0.05 machines are available per million people versus 11.4 machines in North-America (39). Furthermore, even if there is access, older, multi-fractionated radiotherapy schedules for treatment of painful bone metastases are often used, instead of the recommended single-fraction radiotherapy, as was shown in a survey on radiation facilities in African countries (40). This further limits the access to (up-to-date) radiotherapy facilities and strengthens the need for other early pain relief options for patients with NSCLC”. Bisphosphonates and denosumab are also used to tread CIBP. Trials including patients with breast and prostate cancer with uncontrolled CIBP indeed showed a reduction in pain scores with (loading doses) of bisphosphonates. However, data in NSCLC is scarce and results found in our systematic review do not show a clear reduction in CIBP in NSCLC. After our search, the NVALT-9 trial was published, and in contrast to the studies including patients with breast- or prostate cancer, loading doses of ibandronate did not lead to rapid bone pain relief in patients with NSCLC and uncontrolled bone pain (41). Denosumab was compared with zoledronic acid in a randomized phase III trial (1596 patients with solid tumors and at least one bone metastasis, 702 patients had NSCLC, patients with breast or prostate cancer were excluded). Primary endpoint was time to first on-study SRE, pain worsening was one of the other endpoints. Denosumab significantly delayed the time to pain worsening (HR, 0.83; 95% confidence interval, 0.71–0.97) in patients with no/mild baseline pain, compared to zoledronic acid (42). Results regarding early pain reduction in patients with baseline CIBP are not available. Unfortunately, the recently published randomized phase III Splendour trial, including only patients with advanced NSCLC (inclusion irrespective of presence of bone metastases), did not report data on the effect of denosumab on pain relief in the subgroup of patients with painful bone metastases (43). The trial design was to evaluate whether the addition of denosumab to standard first-line treatment improved OS; the primary endpoint was not met (12).
To the best of our knowledge, there is no explanation why for example bisphosphonates showed a reduction of CIBP in some malignancies but not in lung cancer (13–15, 41, 44, 45). Possible explanations are; differences in tumor histology/biology or bone metastasis metabolism [although bone turnover markers are comparable between for example breast and lung cancer (46)], which leads to different response on bone pain relief options, are probably the most obvious. Also the usage of different concomitant (systemic) therapies, which differs among malignancies, could strengthen pain control (47). Therefore, specific recommendations for (bone) pain relief are needed for different malignancies and findings cannot be extrapolated.
Radioisotopes (e.g., samarium, strontium, and rhenium) are an alternative treatment for CIBP. Radioisotopes have a rapid onset of action, but data on NSCLC are limited and consist only of subgroup analyses (19). Zoledronic acid combined with radioisotopes is another treatment option. The efficacy of adding a radioisotope (choice at discretion of investigator) to zoledronic acid was evaluated in the randomized phase III RTOG 0517 trial (26/262 included patients had lung cancer). (48). Primary endpoint was time to SRE development, pain control was a secondary endpoint. Only patients with stable or no bone pain were included. As a subgroup of patients did not have CIBP, and one of the treatment arms consisted of radioisotopes, we excluded this study in our article selection. The addition of radioisotopes resulted in superior pain control at one month, compared with zoledronic acid alone (median pain score of 0 versus 1, p=0.02). Subgroup analysis regarding the primary tumor histology or the presence of baseline CIBP were not performed (48). Because the relatively short duration of action of radioisotopes, it is expected that this treatment must be repeated several times if the patient has a prolonged survival.
Immune checkpoint inhibitors have become standard of care treatment for most patients with advanced NSCLC and result in durable responses in a subgroup of patients. For the subgroup of patients with oncogenic drivers, tyrosine kinase inhibitors often result in early and prolonged responses. For both classes of drugs, effects on CIBP have not been specifically reported. It is possible that in some patients, immune checkpoint inhibitors will not be very active in pain relief for CIBP, as Schmid et al. reported that efficacy of immunotherapy depends on the metastatic location: the treatment efficacy is less in bone lesions compared to lymph nodes (49). However, CIBP related outcomes have not been reported. Denosumab in combination with nivolumab, a programmed death-1 (PD-1) inhibitor, is currently under evaluation in patients with NSCLC and bone metastases (NCT03669523) with the overall response rate as primary outcome measurement. Time to first SRE is one of the secondary outcome measurements but there is no specific focus on pain relief. A phase II study with AL2846, a multi-target tyrosine kinase receptor inhibitor versus zoledronic acid in bone metastasized NSCLC (NCT04325776) is not yet recruiting. The primary endpoint is time to first SRE, and effectiveness of improving average daily pain (not specifically CIBP) is one of the secondary outcomes. Another, not yet recruiting, phase IV, study is zoledronic acid combined with radiotherapy for bone metastasis of NSCLC (NCT02480634). The primary outcome of this study is the percentage of patients who reach objective bone pain response.
Experimental studies in animal models of CIBP have shown alterations in, e.g., astrocytes or in the sphingolipid metabolism in the spinal cord or showed the importance of connexins in the cell-cell communication with probable effects on CIBP. Recently, different studies focused on therapeutic options to block or alter these pathophysiological changes. Blockade of interleukine-6 signaling is promising as it could lead to prevention or delay of bone remodeling as well as decreased pain intensity (4).
Some possible drawbacks for this systematic review exist. A point for discussion could be the chosen definition of early pain reduction (pain reduction within six weeks). We chose this upper limit to be as inclusive as possible to include treatment options that resulted in pain reduction within a relatively short term. Of note, for pain reduction treatment options within a shorter time frame (e.g., one or two weeks), even less data is available. As discussed above, bisphosphonates have different activity on early CIBP reduction in breast- and prostate cancer compared with NSCLC, we did not broaden our inclusion criteria to include other tumor types (13–15, 41).
Furthermore, as expected with over half of the included trials being single arm and/or not blinded and as shown by the Jadad score the methodological quality of most included trials is poor. Last, we did not include a formal test of heterogeneity, as only very heterogeneous trials met our inclusion criteria.
Conclusion
In conclusion, despite the frequent occurrence of CIBP combined with the negative effects on QoL and OS, literature on the optimal treatment of CIBP in NSCLC is lacking. Most of the recommendations given in current guidelines are mainly based on data obtained in other tumors such as breast and prostate. Therefore, randomized trials evaluating treatment options with early pain relief for CIBP are necessary in lung cancer patients.
Data Availability Statement
No datasets were generated or analyzed for this study.
Author Contributions
Conceptualization: AB, BB, MB-E, LH. Formal Analysis: AB, BB. Writing—Original Draft Preparation: AB. Writing—Review and Editing: BB, MB-E, A-MD, LH. All authors agree to be accountable for the content of the work. All authors contributed to the article and approved the submitted version.
Conflict of Interest
A-MD has taken part on an advisory board for Roche.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2020.509297/full#supplementary-material
References
1. Hendriks LE, Smit EF, Vosse BA, Mellema WW, Heideman DA, Bootsma GP, et al. EGFR mutated non-small cell lung cancer patients: more prone to development of bone and brain metastases? Lung Cancer (2014) 84(1):86–91. doi: 10.1016/j.lungcan.2014.01.006
2. Oliveira M, Mello F, Paschoal M. The relationship between lung cancer histology and the clinicopathological characteristics of bone metastasis. Lung Cancer (2016) 96:10–24. doi: 10.1016/j.lungcan.2016.03.014
3. Silva GT, Silva LM, Bergmann A, Thuler LC. Bone metastases and skeletal-related events: incidence and prognosis according to histological subtype of lung cancer. Future Oncol (2019) 15(5):485–94. doi: 10.2217/fon-2018-0613
4. Zajaczkowska R, Kocot-Kepska M, Leppert W, Wordliczek J. Bone Pain in Cancer Patients: Mechanisms and Current Treatment. Int J Mol Sci (2019) 20(23):1–20. doi: 10.3390/ijms20236047
5. Kuchuk M, Addison CL, Clemons M, Kuchuk I, Wheatley-Price P. Incidence and consequences of bone metastases in lung cancer patients. J Bone Oncol (2013) 2(1):22–9. doi: 10.1016/j.jbo.2012.12.004
6. Santini D, Barni S, Intagliata S, Falcone A, Ferrau F, Galetta D, et al. Natural History of Non-Small-Cell Lung Cancer with Bone Metastases. Sci Rep (2015) 5:18670. doi: 10.1038/srep18670
7. Mantyh PW. Mechanisms that drive bone pain across the lifespan. Br J Clin Pharmacol (2018) 85(6):1103–13. doi: 10.1111/bcp.13801
8. WHO’s cancer pain ladder for adults [12-12-2018]. . https://www.who.int/cancer/palliative/painladder/en/.
9. Makhlouf SM, Pini S, Ahmed S, Bennett MI. Managing Pain in People with Cancer-a Systematic Review of the Attitudes and Knowledge of Professionals, Patients, Caregivers and Public. J Cancer Educ (2019) 35(2):214–40. doi: 10.1007/s13187-019-01548-9
10. Coleman R, Hadji P, Body JJ, Santini D, Chow E, Terpos E, et al. Bone Health in Cancer: Esmo Clinical Practice Guidelines. Ann Oncol (2020). doi: 10.1016/j.annonc.2020.07.019
11. Gomez-Iturriaga A, Cacicedo J, Navarro A, Morillo V, Willisch P, Carvajal C, et al. Incidence of pain flare following palliative radiotherapy for symptomatic bone metastases: multicenter prospective observational study. BMC Palliat Care (2015) 14:48. doi: 10.1186/s12904-015-0045-8
12. Planchard D, Popat S, Kerr K, Novello S, Smit EF, Faivre-Finn C, et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol (2018) 29(Supplement_4):iv192–237. doi: 10.1093/annonc/mdy275
13. Body JJ, Diel IJ, Bell R, Pecherstorfer M, Lichinitser MR, Lazarev AF, et al. Oral ibandronate improves bone pain and preserves quality of life in patients with skeletal metastases due to breast cancer. Pain (2004) 111(3):306–12. doi: 10.1016/j.pain.2004.07.011
14. Heidenreich A, Elert A, Hofmann R. Ibandronate in the treatment of prostate cancer associated painful osseous metastases. Prostate Cancer Prostatic Dis (2002) 5(3):231–5. doi: 10.1038/sj.pcan.4500574
15. Mancini I, Dumon JC, Body JJ. Efficacy and safety of ibandronate in the treatment of opioid-resistant bone pain associated with metastatic bone disease: a pilot study. J Clin Oncol (2004) 22(17):3587–92. doi: 10.1200/JCO.2004.07.054
16. NICE Guidance [NG 122]. Lung cancer: diagnosis and management. NICE (National Institute for Health and Care excellence) (2019). Available at: https://www.nice.org.uk/guidance/ng122.
17. Ettinger DS, Wood DE, Aisner DL, Akerley W, Bauman J, Bharat A, et al. NCCN Guidelines Version 8.2020 Non-Small Cell Lung Cancer. NCCN (National Comprehensive Cancer Network) (2020). Available at: https://www.nccn.org/professionals/physician_gls/default.aspx.
18. da Costa Santos CM, de Mattos Pimenta CA, Nobre MR. The PICO strategy for the research question construction and evidence search. Rev Lat Am Enfermagem (2007) 15(3):508–11. doi: 10.1590/S0104-11692007000300023
19. Hendriks LE, Hermans BC, van den Beuken-van Everdingen MH, Hochstenbag MM, Dingemans AM. Effect of Bisphosphonates, Denosumab, and Radioisotopes on Bone Pain and Quality of Life in Patients with Non-Small Cell Lung Cancer and Bone Metastases: A Systematic Review. J Thorac Oncol (2016) 11(2):155–73. doi: 10.1016/j.jtho.2015.10.001
20. Olivo SA, Macedo LG, Gadotti IC, Fuentes J, Stanton T, Magee DJ. Scales to assess the quality of randomized controlled trials: a systematic review. Phys Ther (2008) 88(2):156–75. doi: 10.2522/ptj.20070147
21. Davidov D. Our experience with zoledronix acid in the treatment of patients with non-small cell lung cancer and bone metastases. J IMAB (2013) 19(1):391–95. doi: 10.5272/jimab.2013191.391
22. Francini F, Pascucci A, Bargagli G, Francini E, Conca R, Miano ST, et al. Effects of intravenous zoledronic acid and oral ibandronate on early changes in markers of bone turnover in patients with bone metastases from non-small cell lung cancer. Int J Clin Oncol (2011) 16(3):264–9. doi: 10.1007/s10147-010-0179-x
23. Liu Z, Xu Y, Liu ZL, Tian YZ, Shen XH. Combined application of diclofenac and celecoxib with an opioid yields superior efficacy in metastatic bone cancer pain: a randomized controlled trial. Int J Clin Oncol (2017) 22(5):980–5. doi: 10.1007/s10147-017-1133-y
24. Rodriguez MJ, Contreras D, Galvez R, Castro A, Camba MA, Busquets C, et al. Double-blind evaluation of short-term analgesic efficacy of orally administered dexketoprofen trometamol and ketorolac in bone cancer pain. Pain (2003) 104(1-2):103–10. doi: 10.1016/S0304-3959(02)00470-0
25. Sima L, Fang WX, Wu XM, Li F. Efficacy of oxycodone/paracetamol for patients with bone-cancer pain: a multicenter, randomized, double-blinded, placebo-controlled trial. J Clin Pharm Ther (2012) 37(1):27–31. doi: 10.1111/j.1365-2710.2010.01239.x
26. Sjolund KF, Yang R, Lee KH, Resnick M. Randomized study of pregabalin in patients with cancer-induced bone pain. Pain Ther (2013) 2(1):37–48. doi: 10.1007/s40122-013-0009-8
27. Yousef AA, Alzeftawy AE. The efficacy of oral piroxicam fast-dissolving tablets versus sublingual fentanyl in incident breakthrough pain due to bone metastases: a double-blinded randomized study. Support Care Cancer (2019) 27(6):2171–7. doi: 10.1007/s00520-018-4469-6
28. Gangi A, Kastler B, Klinkert A, Dietemann JL. Injection of alcohol into bone metastases under CT guidance. J Comput Assist Tomogr (1994) 18(6):932–5. doi: 10.1097/00004728-199411000-00016
29. Yoh K, Kubota K, Ohmatsu H, Goto K, Niho S, Ohe Y. Feasibility study of zoledronic acid plus cisplatin-docetaxel as first-line treatment for advanced non-small cell lung cancer with bone metastases. Anticancer Res (2012) 32(9):4131–5.
30. Zarogoulidis K, Boutsikou E, Zarogoulidis P, Eleftheriadou E, Kontakiotis T, Lithoxopoulou H, et al. The impact of zoledronic acid therapy in survival of lung cancer patients with bone metastasis. Int J Cancer (2009) 125(7):1705–9. doi: 10.1002/ijc.24470
31. Garon EB, Hellmann MD, Rizvi NA, Carcereny E, Leighl NB, Ahn MJ, et al. Five-Year Overall Survival for Patients With Advanced NonSmall-Cell Lung Cancer Treated With Pembrolizumab: Results From the Phase I KEYNOTE-001 Study. J Clin Oncol (2019) 37(28):2518–27. doi: 10.1200/JCO.19.00934
32. Gettinger S, Horn L, Jackman D, Spigel D, Antonia S, Hellmann M, et al. Five-Year Follow-Up of Nivolumab in Previously Treated Advanced Non-Small-Cell Lung Cancer: Results From the CA209-003 Study. J Clin Oncol (2018) 36(17):1675–84. doi: 10.1200/JCO.2017.77.0412
33. Okamoto I, Morita S, Tashiro N, Imamura F, Inoue A, Seto T, et al. Real world treatment and outcomes in EGFR mutation-positive non-small cell lung cancer: Long-term follow-up of a large patient cohort. Lung Cancer (2018) 117:14–9. doi: 10.1016/j.lungcan.2018.01.005
34. Yamamoto N, Seto T, Nishio M, Goto K, Okamoto I, Yamanaka T. Erlotinib plus bevacizumab (EB) versus erlotinib alone (E) as first-line treatment for advanced EGFR mutation–positive non-squamous non–small-cell lung cancer (NSCLC): Survival follow-up results of JO25567. J Clin Oncol (2018) 36. doi: 10.1200/JCO.2018.36.15_suppl.9007
35. Peters S, Mok TSK, Gadgeel SM, Rosell R, Dziadziuszko R, Kim D-W, et al. Updated overall survival (OS) and safety data from the randomized, phase III ALEX study of alectinib (ALC) versus crizotinib (CRZ) in untreated advanced ALK+ NSCLC. J Clin Oncol (2020) 38. doi: 10.1200/JCO.2020.38.15_suppl.9518
36. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin (2020) 70(1):7–30. doi: 10.3322/caac.21590
37. Brahmer J, Rodriguez-Azbreu D, Robinson AG, Hui R, Csöszi T, Fülöp A, et al. KEYNOTE-024 5-year OS update: First-line (1L) pembrolizumab (pembro) vs platinum-based chemotherapy (chemo) in patients (pts) with metastatic NSCLC and PD-L1 tumour proportion score (TPS) ≥50%. Ann Oncol (2020) 31(suppl_4):S1142–215. doi: 10.1016/annonc/annonc325
38. Davies AN, Elsner F, Filbet MJ, Porta-Sales J, Ripamonti C, Santini D, et al. Breakthrough cancer pain (BTcP) management: a review of international and national guidelines. BMJ Support Palliat Care (2018) 8(3):241–9. doi: 10.1136/bmjspcare-2017-001467
39. Elmore SNC, Grover S, Bourque JM, Chopra S, Nyakabau AM, Ntizimira C, et al. Global palliative radiotherapy: a framework to improve access in resource-constrained settings. Ann Palliat Med (2019) 8(3):274–84. doi: 10.21037/apm.2019.02.02
40. Jeremic B, Vanderpuye V, Abdel-Wahab S, Gaye P, Kochbati L, Diwani M, et al. Patterns of practice in palliative radiotherapy in Africa - case revisited. Clin Oncol (R Coll Radiol) (2014) 26(6):333–43. doi: 10.1016/j.clon.2014.03.004
41. Brouns A, Hendriks LEL, van der Noort V, van de Borne B, Schramel F, Groen HJM, et al. Efficacy of Ibandronate Loading Dose on Rapid Pain Relief in Patients With Non-Small Cell Lung Cancer and Cancer Induced Bone Pain: The NVALT-9 Trial. Front Oncol (2020) 10:890. doi: 10.3389/fonc.2020.00890
42. Henry D, Vadhan-Raj S, Hirsh V, von Moos R, Hungria V, Costa L, et al. Delaying skeletal-related events in a randomized phase 3 study of denosumab versus zoledronic acid in patients with advanced cancer: an analysis of data from patients with solid tumors. Support Care Cancer (2014) 22(3):679–87. doi: 10.1007/s00520-013-2022-1
43. Peters S, Danson S, Hasan B, Dafni U, Reinmuth N, Majem M, et al. A randomised open-label phase III trial evaluating the addition of denosumab to standard first-line treatment in advanced NSCLC - the ETOP and EORTC SPLENDOUR trial. J Thorac Oncol (2020) 15(10):1647–56. doi: 10.1016/j.jtho.2020.06.011
44. Saad F, Sternberg CN, Mulders PFA, Niepel D, Tombal BF. The role of bisphosphonates or denosumab in light of the availability of new therapies for prostate cancer. Cancer Treat Rev (2018) 68:25–37. doi: 10.1016/j.ctrv.2018.04.014
45. Wong MH, Stockler MR, Pavlakis N. Bisphosphonates and other bone agents for breast cancer. Cochrane Database Syst Rev (2012) 2):CD003474. doi: 10.1002/14651858.CD003474.pub3
46. Shih LY, Shih HN, Chen TH. Bone resorption activity of osteolytic metastatic lung and breast cancers. J Orthop Res (2004) 22(6):1161–7. doi: 10.1016/j.orthres.2003.03.004
47. Lopez-Olivo MA, Shah NA, Pratt G, Risser JM, Symanski E, Suarez-Almazor ME. Bisphosphonates in the treatment of patients with lung cancer and metastatic bone disease: a systematic review and meta-analysis. Support Care Cancer (2012) 20(11):2985–98. doi: 10.1007/s00520-012-1563-z
48. Seider MJ, Pugh SL, Langer C, Wyatt G, Demas W, Rashtian A, et al. Randomized phase III trial to evaluate radiopharmaceuticals and zoledronic acid in the palliation of osteoblastic metastases from lung, breast, and prostate cancer: report of the NRG Oncology RTOG 0517 trial. Ann Nucl Med (2018) 32(8):553–60. doi: 10.1007/s12149-018-1278-4
Keywords: non-small cell lung cancer, bone metastases, cancer induced bone pain, pain relief, bisphosphonates, systematic review
Citation: Brouns AJWM, De Bie BH, van den Beuken-van Everdingen MHJ, Dingemans A-MC and Hendriks LEL (2020) Non-Radiation Based Early Pain Relief Treatment Options for Patients With Non-Small Cell Lung Cancer and Cancer Induced Bone Pain: A Systematic Review. Front. Oncol. 10:509297. doi: 10.3389/fonc.2020.509297
Received: 07 November 2019; Accepted: 30 September 2020;
Published: 22 October 2020.
Edited by:
Ibiayi Dagogo-Jack, Massachusetts General Hospital Cancer Center, United StatesReviewed by:
Valerio Gristina, University of Palermo, ItalyBen Walker Fischer-Valuck, Emory University, United States
Copyright © 2020 Brouns, De Bie, van den Beuken-van Everdingen, Dingemans and Hendriks. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lizza E. L. Hendriks, lizza.hendriks@mumc.nl