 Jana Werner
Jana Werner Giovanna Brandi
Giovanna Brandi Ilijas Jelcic
Ilijas Jelcic Marian Galovic
Marian Galovic- 1Department of Intensive Care Medicine, University Hospital Zurich, Zurich, Switzerland
- 2Department of Neurology, Clinical Neuroscience Center, University Hospital Zurich, Zurich, Switzerland
Background: Vaccination against SARS-CoV-2 has been conducted frequently to limit the pandemic but may rarely be associated with postvaccinal autoimmune reactions or disorders.
Case presentation: We present a 35-year-old woman who developed fever, skin rash, and headache 2 days after the second SARS-CoV-2 vaccination with BNT162b2 (Pfizer/Biontech). Eight days later, she developed behavioral changes and severe recurrent seizures that led to sedation and intubation. Cerebral magnetic resonance imaging showed swelling in the (para-) hippocampal region predominantly on the left hemisphere and bilateral subcortical subinsular FLAIR hyperintensities. Cerebrospinal fluid analysis revealed a lymphocytic pleocytosis of 7 cells/μl and normal protein and immunoglobulin parameters. Common causes of encephalitis or encephalopathy such as viral infections, autoimmune encephalitis with well-characterized autoantibodies, paraneoplastic diseases, and intoxications were ruled out. We made a diagnosis of new-onset refractory status epilepticus (NORSE) due to seronegative autoimmune encephalitis. The neurological deficits improved after combined antiepileptic therapy and immunomodulatory treatment including high-dose methylprednisolone and plasma exchange.
Conclusions: Although a causal relationship cannot be established, the onset of symptoms shortly after receiving the SARS-CoV-2 vaccine suggests a potential association between the vaccination and NORSE due to antibody-negative autoimmune encephalitis. After ruling out other etiologies, early immunomodulatory treatment may be considered in such cases.
Introduction
Adverse effects of SARS-CoV-2 vaccination with mRNA vaccines are rare and mostly limited to local reactions or slight systemic symptoms (1) including fatigue and headache most commonly. Generally, post-vaccination autoimmune encephalitis is rare (2, 3), but it has been reported to have an association with the adenoviral vector vaccine ChAdOx1 (Oxford-AstraZeneca) (4) as well as the mRNA vaccine (Pfizer/Biontech) for SARS-CoV-2 (3, 5).
A heterogeneous group of sporadic autoimmune encephalitis cases associated with SARS-CoV-2 infection has also been reported (6). Additionally, more and more autoimmune encephalitis cases have been linked to other viral triggers (7).
Here, we describe a case of new-onset refractory status epilepticus (NORSE) due to autoantibody-negative autoimmune encephalitis in close temporal association with the second SARS-CoV-2 vaccination dose of BNT162b2 (Pfizer/Biontech).
Case presentation
A 35-year old woman was referred to our center with recurrent focal to bilateral convulsive seizures after an episode of fever, headache, and skin rash 6 days prior. Two days before the onset of fever, she received the second dose of an mRNA-based SARS-CoV-2 vaccine (BNT162b2, Pfizer/Biontech). The first dose was well-tolerated. The patient's medical history revealed only sporadic but not recent cocaine consumption and mild SARS-CoV-2 infection a year before the vaccination.
The clinical, laboratory, and imaging findings are summarized in Table 1 and are illustrated in Figure 1. On admission, the patient presented with fever of up to 40°C, visual impairment, behavioral changes, recurrent focal to bilateral tonic-clonic seizures, reduced level of consciousness, and choreatic movements. On admission, moderately elevated TSH, normal free T3 and T4 hormone levels, and slightly elevated liver function tests possibly due to recent overuse of paracetamol were found in the blood test. Drug screening of urine was negative.
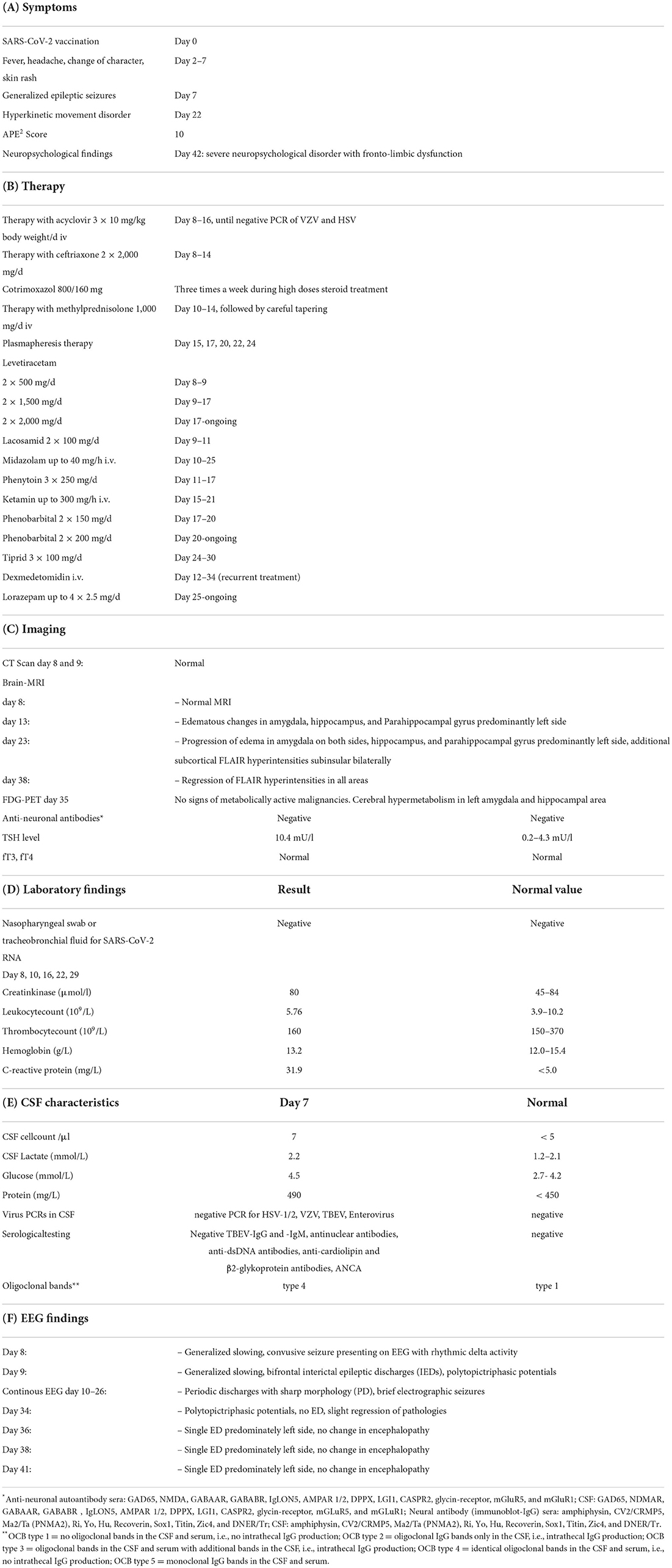
Table 1. (A) Symptoms and (B) therapy, (C) imaging, (D) laboratory, (E) CSF, and (F) EEG findings.
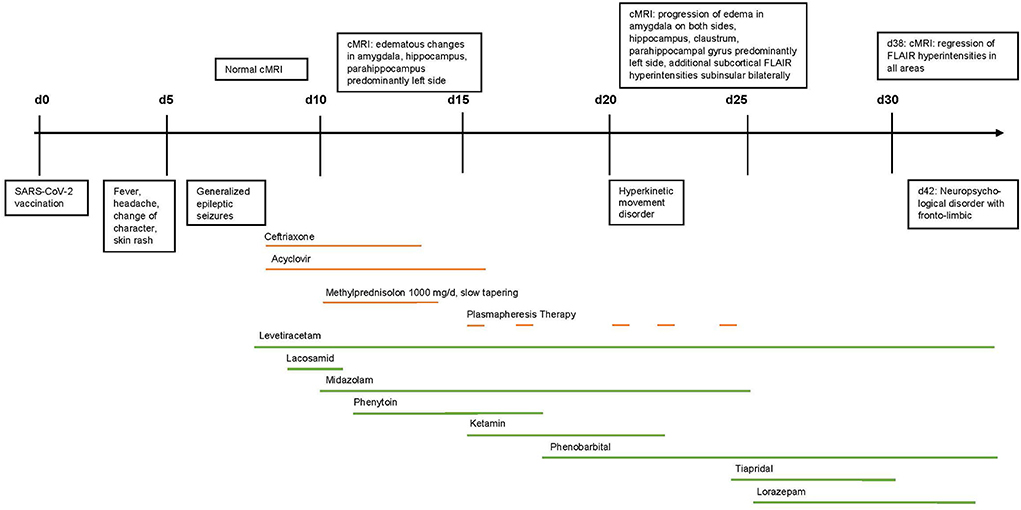
Figure 1. Timeline of clinical development, therapy, and MRI-findings.
The electroencephalogram (EEG) initially showed a generalized rhythmic delta activity with superimposed multifocal interictal epileptic discharges mainly over the frontal and right-sided leads. Frequent brief electrographic seizures were also detected (Figure 2). Initial CT and MRI scans were unremarkable. The MRI on day 5 after admission revealed edema in the left mesial temporal lobe, particularly the hippocampus, which became progressive in size 10 days later. Additionally, FLAIR hyperintensive lesions in the bilateral subinsular regions were detected (Figure 3). The FDG PET showed hypermetabolism of the left amygdala and hippocampus and basal pulmonary hypoventilation. Cerebrospinal fluid (CSF) analysis revealed lymphocytic pleocytosis (7 cells/μl), normal protein, glucose, lactate, and total immunoglobulin parameters, and matched oligoclonal bands in the serum and CSF without signs of intrathecal IgG production (Table 1). The blood and CSF screening for common viral and bacterial infections and autoimmune disorders including vasculitis was negative. The diagnostic criteria for a definite autoantibody-negative autoimmune limbic encephalitis according to established criteria were fullfilled (8). However, testing for common anti-neuronal autoantibodies in serum and CSF was negative, including indirect immunofluorescence staining of mouse brain.
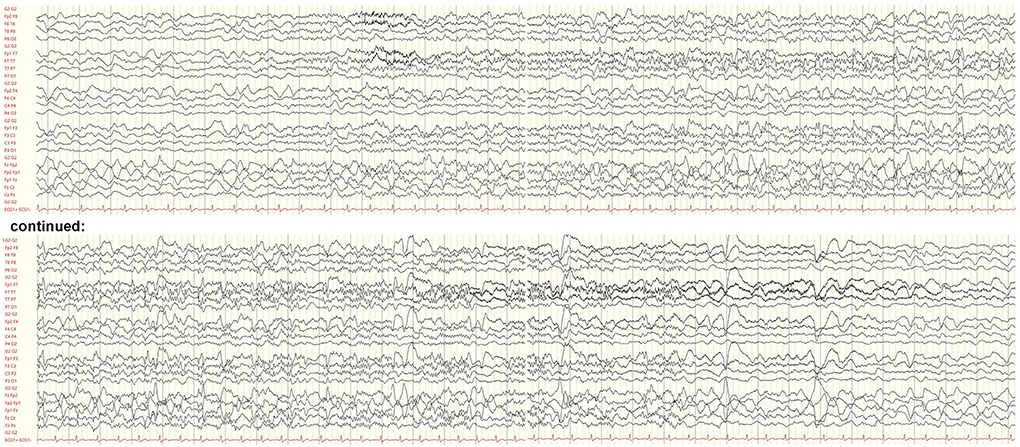
Figure 2. Electroencephalogram on day 8 after symptom onset showing a brief focal seizure. The seizure discharge begins with an evolving fast rhythm with onset in the left temporal leads and interspersed epileptic discharges. There is generalized background slowing following the seizure. Bipolar longitudinal montage, gain 70 μV/cm, base time 3 cm/s, high-pass filter. 53 Hz, low-pass filter 80 Hz, and notch filter 50 Hz.
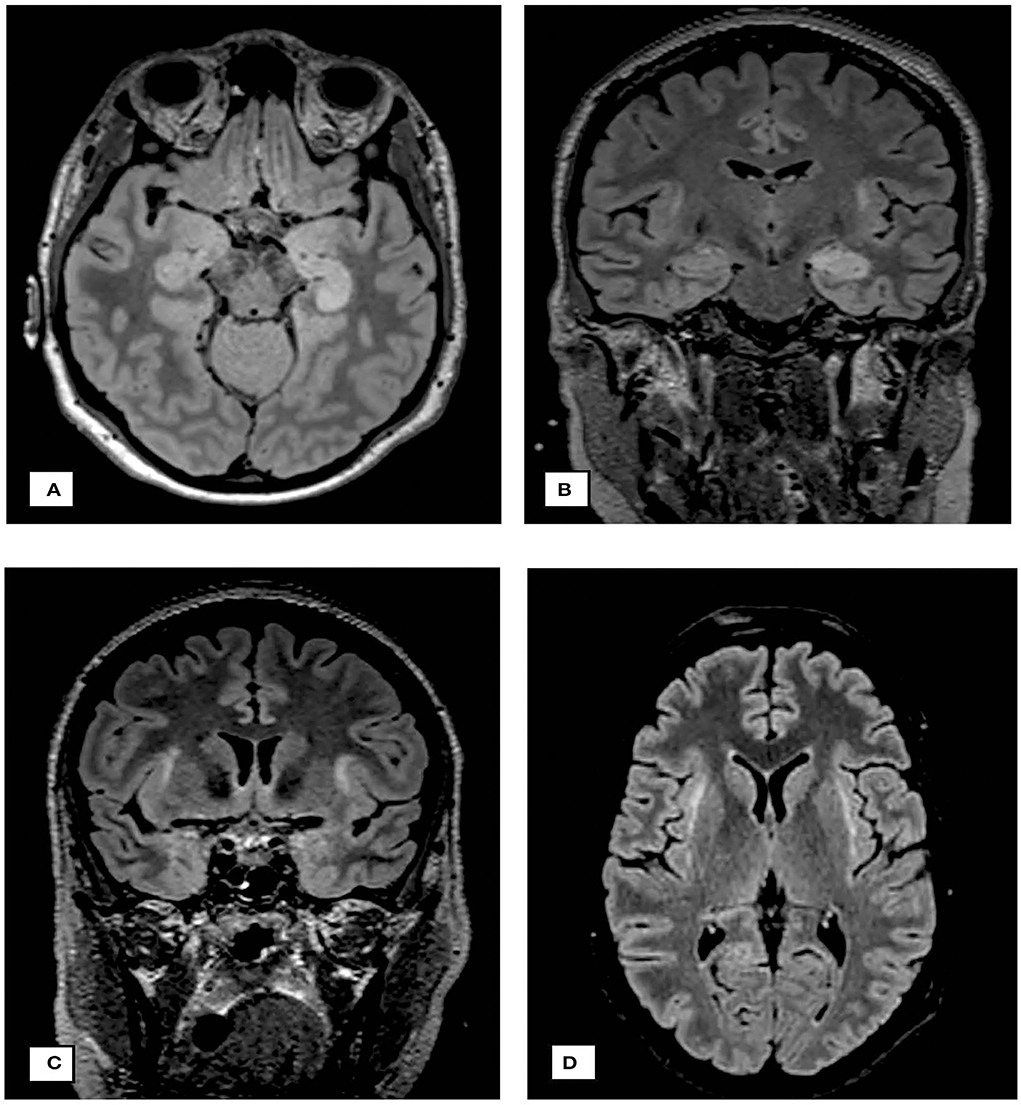
Figure 3. Neuroimaging findings. (A) cMRI on day 13: axial FLAIR sequence demonstrating edematous changes in hippocampus and parahippocampal gyrus predominantly on the left side. (B) cMRI on day 23: coronary FLAIR sequence demonstrating progression of edema on both sides, the hippocampus and parahippocampal gyrus, additional subcortical FLAIR hyperintensities subinsular on both sides. (C,D) demonstrate the claustra hyperintensities.
Due to recurrent convulsive seizures without regaining consciousness, a diagnosis of new-onset refractory status epilepticus (NORSE) was made. Levetiracetam up to 4 g/d and lacosamide up to 200 mg/d were started. Under continuous EEG monitoring, phenytoin up to 750 mg/d, midazolam up to 0.57 mg/kg/h, and ketamine up to 4 mg/kg/h were added. Phenytoin was later replaced by phenobarbital. Initially, acyclovir 3 × 10 mg/kg body weight/day and ceftriaxone were given until the CSF and serum testing for herpes viral and bacterial CNS infections turned negative. Immunomodulatory treatment with high-dose methylprednisolone (5 days of 1,000 mg/d IV) was started 2 days after hospital admission with subsequent slow tapering over 8 weeks. Because of continued seizures, plasma exchange for over 10 days starting on day 7 after the admission was performed.
Subsequently, the patient's condition rapidly improved beginning on day 12 after the admission; she regained full consciousness and had only infrequent seizures. The follow-up MRI 1 month after the hospital admission showed edema reduction in the hippocampal, amygdala, and external capsule. On discharge, she had persisting moderate mnestic deficits and infrequent seizures (2–3/month). However, after 2 months, the patient was readmitted to our hospital because of deterioration in seizure frequency (2–3 serial seizures) and neuropsychological deficits. She again received high-dose methylprednisolone for 5 days, which led to significant reduction in seizure frequency.
Discussion and conclusions
We report the first case, to our knowledge, of NORSE due to seronegative autoimmune encephalitis 8 days after vaccination with the mRNA SARS-CoV-2 vaccine. A causal relationship between vaccination and autoimmune encephalitis with NORSE is not established with certainty. Nevertheless, the onset of neurological symptoms 8 days following the vaccination suggests a potential association as well as the hyperintensities of the claustrum as a common finding in NORSE and autoimmune encephalitis (9, 10).
Given the assumed low incidence of autoimmune reactions and their favorable outcome, benefits of vaccination far outweigh the risk of side effects. Importantly, SARS-CoV-2 infection itself may trigger a heterogeneous group of autoimmune encephalitis. Hence, the observation of SARS-CoV-2 vaccine-associated NORSE does not argue against the broad use of SARS-CoV-2 vaccines.
Whether the patient's history of SARS-CoV-2 infection approximately 1 year before the encephalitis may have played a role remains unknown. Our findings should encourage clinicians to consider SARS-CoV-2 vaccination or infection as a potential trigger for autoimmune encephalitis.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
JW collected and interpreted the clinical and radiological data and was a major contributor in the writing and revision of the manuscript. IJ collected and interpreted the clinical and laboratory data and revised the manuscript. GB interpreted the clinical findings and revised the manuscript. MG interpreted the clinical and electroencephalographic findings and revised the manuscript. All authors read and approved the final version of the manuscript.
Funding
This study was partly supported by the SNF (Grant No: 4078P0_198345, title: Protective and Pathogenic T Cell Immunity During SARS-CoV-2 Infection) and the Loop Zurich, COVID-19 project (Title: SARS-CoV-2-Induced Immune Alterations and their Role in Post-COVID Syndrome).
Acknowledgments
We would like to extend our acknowledgment to Giselle Golby who revised the manuscript for medical English.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
COVID-19, coronavirus disease 2019; CSF, cerebrospinal fluid; CNS, central nervous system; EEG, electroencephalogram; ED, epileptic discharge; FDG-PET, 2-fluor-2-desoxy-D-glucose positron emission tomography; FLAIR, fluid-attenuated inversion recovery; HSV-1/2, herpes simplex virus type 1 or 2; IED, interictal epileptic discharge; MRI, magnetic resonance imaging; NORSE, new onset refractory status epilepticus; PCR, polymerase chain reaction; PD, periodic discharge with sharp morphology; RNA, ribonucleic acid; SARS-CoV-2, severe acute respiratory syndrome virus 2; VZV, varicella zoster virus.
References
1. Thomas SJ, Thomas SJ, Kitchin N, Absalon J, Gurtman A, Lockhart S, et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine through 6 months. N Engl J Med. (2021) 385:1761–73. doi: 10.1056/NEJMoa2110345
2. Tian M, Yang J, Li L, Li J, Lei W, Shu X. Vaccine-associated neurological adverse events: a case report and literature review. Curr Pharm Des. (2020) 25:4570–8. doi: 10.2174/1381612825666191119095132
3. Kaulen LD, Doubrovinskaia S, Mooshage C, Jordan B, Purrucker J, Haubner C, et al. Neurological autoimmune diseases following vaccinations against SARS-CoV-2: a case series. Eur J Neurol. (2022) 29:555–63. doi: 10.1111/ene.15147
4. Zuhorn F, Graf T, Klingebiel R, Schäbitz WR, Rogalewski A. Postvaccinal encephalitis after ChAdOx1 nCov-19. Ann Neurol. (2021) 90:506–11. doi: 10.1002/ana.26182
5. Zlotnik Y, Gadoth A, Abu-Salameh I, Horev A, Novoa R, Ifergane G. Case report: anti-LGI1 encephalitis following COVID-19 vaccination. Front Immunol. (2021) 12:813487. doi: 10.3389/fimmu.2021.813487
6. Valencia Sanchez C, Theel E, Binnicker M, Toledano M, McKeon A. Autoimmune encephalitis after SARS-CoV-2 infection: case frequency, findings, and outcomes. Neurology. (2021) 97:e2262–8. doi: 10.1212/WNL.0000000000012931
7. Joubert,B, Dalmau J. The role of infections in autoimmune encephalitides. Rev Neurol (Paris). (2019) 175:420–6. doi: 10.1016/j.neurol.2019.07.004
8. Graus F, Titulaer MJ, Balu R, Benseler S, Bien CG, Cellucci T, et al. A clinical approach to diagnosis of autoimmune encephalitis. Lancet Neurol. (2016) 15:391–404. doi: 10.1016/S1474-4422(16)30130-2
9. Meletti S, Giovannini G, d'Orsi G, Toran L, Monti G, Guha R, et al. New-Onset refractory status epilepticus with claustrum damage: definition of the clinical and neuroimaging features. Front Neurol. (2017) 8:111. doi: 10.3389/fneur.2017.00111
Keywords: new-onset refractory epileptic state, NORSE, SARS-CoV-2 vaccination, BNT162b2, seronegative autoimmune encephalitis, postvaccinal encephalitis
Citation: Werner J, Brandi G, Jelcic I and Galovic M (2022) New-onset refractory status epilepticus due to autoimmune encephalitis after vaccination against SARS-CoV-2: First case report. Front. Neurol. 13:946644. doi: 10.3389/fneur.2022.946644
Received: 17 May 2022; Accepted: 21 July 2022;
Published: 16 August 2022.
Edited by:
Fernando Cendes, State University of Campinas, BrazilReviewed by:
Felipe von Glehn, University of Brasilia, BrazilLécio Figueira Pinto, University of São Paulo, Brazil
Copyright © 2022 Werner, Brandi, Jelcic and Galovic. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jana Werner, jana.werner@usz.ch