 Aiyu Peng
Aiyu Peng Chunmei Gong1†
Chunmei Gong1† Wenxu Hong
Wenxu Hong Junxia Yan
Junxia Yan- 1Animal Laboratory, Shenzhen Center for Chronic Disease Control, Shenzhen, China
- 2Department of Epidemiology and Health Statistics, XiangYa School of Public Health, Central South University, Changsha, China
- 3Hunan Provincial Key Laboratory of Clinical Epidemiology, XiangYa School of Public Health, Central South University, Changsha, China
- 4Institute of Clinical Pharmacology, Central South University, Changsha, China
Background: Variants in organic cation transporter (OCT) genes play a crucial role in metformin pharmacokinetics and are critical for diabetes treatment. However, studies investigating the effect of OCT genetic polymorphisms on metformin response have reported inconsistent results. This review and meta-analysis aimed to evaluate the associations between OCT genetic polymorphisms and metformin response and intolerance in individuals with type 2 diabetes mellitus (T2DM).
Method: A systematic search was conducted on PubMed, EMBASE, CNKI, WANFANG DATA, and VIP database for identifying potential studies up to 10 November 2022. The Q-Genie tool was used to evaluate the quality of included studies. Pooled odds ratios (OR) or standardized mean differences (SMD) and 95% confidence intervals (95% CI) were calculated to determine the associations between OCT genetic polymorphisms and metformin response and intolerance that were reflected by glycemic response indexes, such as glycated hemoglobin level (HbA1c%) or change in glycated hemoglobin level (ΔHbA1c%), fasting plasma level (FPG) or change in fasting plasma glucose level (ΔFPG), the effectiveness rate of metformin treatment, and the rate of metformin intolerance. A qualitative review was performed for the variants identified just in one study and those that could not undergo pooling analysis.
Results: A total of 30 related eligible studies about OCT genes (SLC22A1, SLC22A2, and SLC22A3) and metformin pharmacogenetics were identified, and 14, 3, and 6 single nucleotide polymorphisms (SNPs) in SLC22A1, SLC22A2, and SLC22A3, respectively, were investigated. Meta-analysis showed that the SLC22A1 rs622342 polymorphism was associated with a reduction in HbA1c level (AA vs. AC: SMD [95% CI] = −0.45 [−0.73–−0.18]; p = 0.001). The GG genotype of the SLC22A1 rs628031 polymorphism was associated with a reduction in FPG level (GG vs. AA: SMD [95 %CI] = −0.60 [−1.04–0.16], p = 0.007; GG vs. AG: −0.45 [−0.67–0.20], p < 0.001). No statistical association was found between the remaining variants and metformin response and intolerance.
Conclusion: SLC22A1 rs622342 and rs628031 polymorphisms were potentially associated with glycemic response to metformin. This evidence may provide novel insight into gene-oriented personalized medicine for diabetes.
1. Introduction
Diabetes mellitus (DM) is a global prevalent chronic metabolic disease characterized by hyperglycemia (1). The prevalence of DM among people aged 20 to 70 is approximately 10.5%, meaning one in ten adults has diabetes. DM and its complications pose a significant burden on mortality and disability globally. According to the International Diabetes Federation (IDF), there will be an estimated 784 million people with diabetes by 2045, and approximately 90% of them will have type 2 diabetes mellitus (T2DM) (2). Given its global influence, it is essential to implement measures to prevent the occurrence and development of T2DM.
Lifestyle modifications, including weight loss, increased physical activity, and healthy eating, and medication are important interventions in T2DM management. Common medications for T2DM include biguanide, sulfonylureas, thiazolidinediones, glycerides, and α-glucosidase inhibitors. Metformin is the most commonly prescribed biguanide and is considered as first-line antidiabetic drug due to its low cost, hypoglycemic effect, and few adverse reactions. Its primary mechanism seems to be a decrease in blood glucose and an improvement of insulin resistance through the inhibition of gluconeogenesis. However, there are significant inter-individual differences in metformin hypoglycemic efficacy, with more than 30% of patients not reaching the target blood glucose level after treatment (3). Metformin intolerance is mainly manifested by gastrointestinal symptoms; studies have shown that approximately 30% of patients had significant gastrointestinal intolerance when taking normal doses of metformin (4). The metformin response and intolerance are affected by non-genetic factors, such as age, sex, and physiological status, while genetic factors also play a crucial role in metformin bioavailability (5). Organic cation transporters (OCTs), belonging to the SLC22 gene family, play an essential role in the pharmacokinetics of metformin. OCTs include three subtypes: OCT1, OCT2, and OCT3. These transporters widely distribute in human intestines, liver, kidney, and other organs and are responsible for metformin absorption, distribution, and elimination (6). Pharmacogenetic researchers speculated that genetic variants may alter the structure and function of organic cation transporters (OCTs), leading to inter-individual differences in responses to metformin (7). To date, a few studies have investigated the effect of polymorphisms in the OCT genes (SLC22A1, SLC22A2, and SLC22A3) on metformin response and intolerance. The current findings on the impact of genetic variants of these transporters on metformin clinical response and intolerance lack consistency, likely due to various factors, such as small sample sizes, differences in study groups, or observational endpoints. Thus, comprehensive meta-analyses are needed to characterize the role of genetic variants in these transporters on metformin clinical response and intolerance.
Previously, Dujic et al. (8) conducted a large-scale meta-analysis across the cohorts of the Metformin Genetics Consortium (MetGen) to investigate the effect of candidate variants of SLC22A1 and SLC22A2 on glycemic response to metformin. However, this meta-analysis only included patients with European ancestry who had T2DM. In recent years, a number of studies have been subsequently performed. Considering that the previous meta-analysis only included patients with European backgrounds and focused on the role of genetic variants in OCT genes on metformin response, we conducted this review and meta-analysis to estimate the association between OCT genetic polymorphisms and metformin response and intolerance in all ethnicities. This study aimed to provide more evidence and guidance for gene-oriented personalized medicine for T2DM patients.
2. Methods
2.1. Literature search strategy
Systematic searches were conducted on PubMed, Embase, China National Knowledge Infrastructure (CNKI), Wanfang database, and VIP database to retrieve potential articles up to 10 November 2022. The search strategy followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement, and it was registered in PROSPERO (https://www.crd.york.ac.uk/PROSPERO), registration number: CRD42022326203). The search strategy was conducted by the following keywords and MeSH terms: (((((((((((((((Diabetes Mellitus, Type 2 [MeSH Terms]) OR (Diabetes Mellitus, Lipoatrophic [MeSH Terms])) OR (Non-insulin Dependent Diabetes Mellitus)) OR (Ketosis Resistant Diabetes Mellitus)) OR (Type II Diabetes Mellitus)) OR (Type 2 Diabetes Mellitus)) OR (Type 2 Diabetes)) OR (Maturity Onset Diabetes)) OR (Adult Onset Diabetes Mellitus)) OR (Stable Diabetes Mellitus)) OR (Lipoatrophic Diabetes Mellitus)) OR (NIDDM)) OR (MODY) AND (((((((((Genetic Polymorphism [MeSH Terms]) OR (Gene Polymorphism)) OR (Polymorphism)) OR (Genetic)) OR (Gene)) OR (Genetic markers)) OR (Single nucleotide polymorphism)) OR (variant)) OR (allele) AND (((((Solute Carrier Family 22 Organic cation transporters) OR (Organic cation transporters)) OR (SLC22)) OR (OCTs) AND ((((((Metformin [MeSH Terms]) OR (Dimethylbiguanidine)) OR (Dimethylguanylguanidine)) OR (Glucophage)) OR (Metformin Hydrochloride)) OR (Metformin HCl) NOT ((animals [MeSH Terms]) NOT (human [MeSH Terms]). In addition, a manual search was performed to identify potential articles that were not screened in the electronic search. After removing duplication, two authors independently screened the articles by reading the title and abstract to determine whether the study met the criteria for further reading the full text.
2.2. Selection criteria
We included genetic studies about OCT genetic polymorphisms and metformin monotherapy (without additional hypoglycemic medication) in T2DM patients. The duration of metformin monotherapy should be more than 2 months. The inclusion criteria were as follows: (1) case–control, cohort, or cross-sectional studies investigating the association between at least one OCT genetic variant and the therapeutic effect or adverse reaction of metformin in T2DM patients; (2) the data on defined genotype and clinical outcome were available to calculate the odds ratio (OR) or standardized mean difference (SMD) and 95% confidence intervals (95% CI); (3) all variants included in the meta-analysis should be assessed in more than one original article. The exclusion criteria included non-human studies, review papers, meta-analyses, conference abstracts, case reports, unpublished articles and comments, and studies with no metformin monotherapy or metformin treatment of < 2 months. If duplicated or overlapped studies were retrieved, we chose the largest study for further analysis.
2.3. Data extraction
The data were extracted independently by two authors with a preconceived table, and disagreements were resolved by consensus. Information about the first author, published year, study design, sites, characteristics of participants (percentage of males, age), treatment duration, therapeutic dose, genotyping, and relevant genes (SNPs) were extracted. Characteristics of genetic variants and related genetic association studies were collected including gene (SNP) with its chromosome position, variant type, minor allele frequency (MAF), P-value of HWE, and clinical effect. Clinical effect was reflected by indexes of metformin response and intolerance, including HbA1c%, ΔHbA1c%, FPG, ΔFPG, postprandial plasma glucose level (PPG), change in postprandial plasma glucose level (ΔPPG), fasting insulin level (FINS), change in fasting insulin level (ΔFINS), insulin resistance index (HOMA-IR), insulin sensitivity index (HOMA-IS), the rate of metformin response or glycemic control, and the rate of metformin intolerance. Metformin intolerance was defined as individuals who stopped metformin within the first 6 months of treatment due to the gastrointestinal adverse events caused by metformin.
2.4. Quality assessment of primary studies
Q-Genie tool was used to estimate the quality of included studies by two independent researchers. This tool was created and validated to aid in the quality assessment of published genetic association studies (9). It consists of 11 items that address the following 11 issues: rationale for the study, definition of outcome, selection of control group, technical and non-technical classification of exposure, discussion of sources of bias, appropriateness of sample size and power, description of planned statistical analysis and methods, statistical methods for controlling confounding, genetic hypothesis test, and appropriateness of conclusions supported by the results (6). Each item is scored from 1 (poor) to 7 (excellent) and then the scores from each item are added. Scores of ≤ 35 are considered low-quality studies, >35 and ≤ 45 are considered middle-quality studies, and >45 are considered high-quality studies.
2.5. Statistical analysis
Meta-analysis was conducted on variants reported in at least two published studies to evaluate their association with clinical effects. For dichotomous outcomes, we calculated the pooled ORs with 95% CIs to assess the degree of associations. For continuous outcomes, the pooled SMDs with 95% CI were calculated. The I2 test and Cochran Q test were used to assess heterogeneity. When a P-value was < 0.05 or I2 > 50%, heterogeneity between studies was considered to be significant, a qualitative review was performed in such cases and the potential source of heterogeneity was discussed. Otherwise, the fixed-effect model was adopted. Forest plots were used to present findings and statistical heterogeneity. STATA12.0 software was used for meta-analysis. The variants identified in only one study were qualitatively described.
3. Results
3.1. Characteristics of the included studies
A total of 495 studies were identified from PubMed (n = 210), Embase (n = 165), CNKI (n = 98), Wanfang Database (n = 12), and VIP Database (n = 4), and nine studies were identified by manual search (Supplementary Table 1). After screening for duplication and eligibility, 30 studies were included, and 14 studies among them were available for meta-analysis with 2,791 T2DM patients (Table 1). The flow diagram of the study selection process is shown in Figure 1.
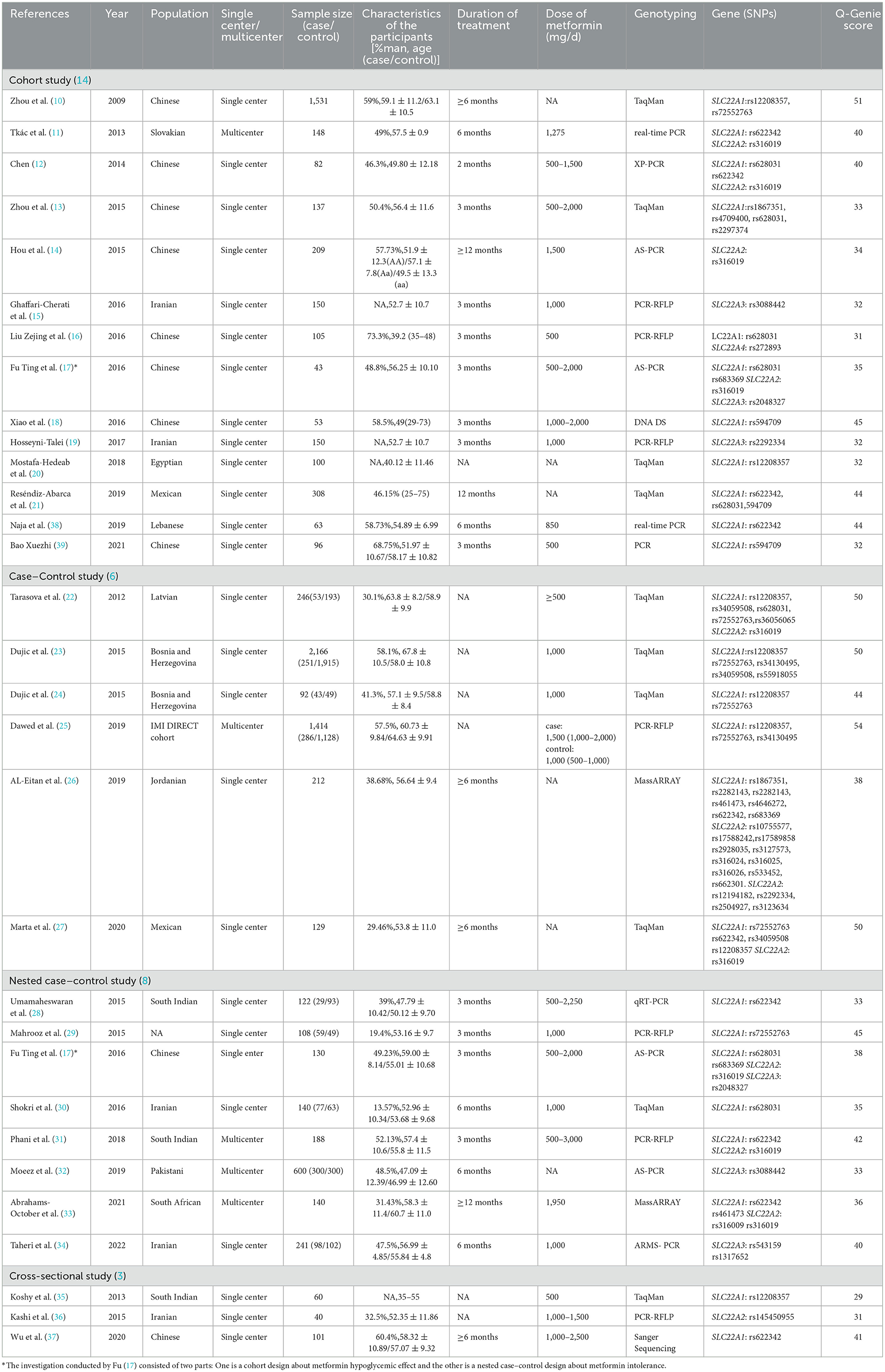
Table 1. Detailed characteristics of all eligible studies.
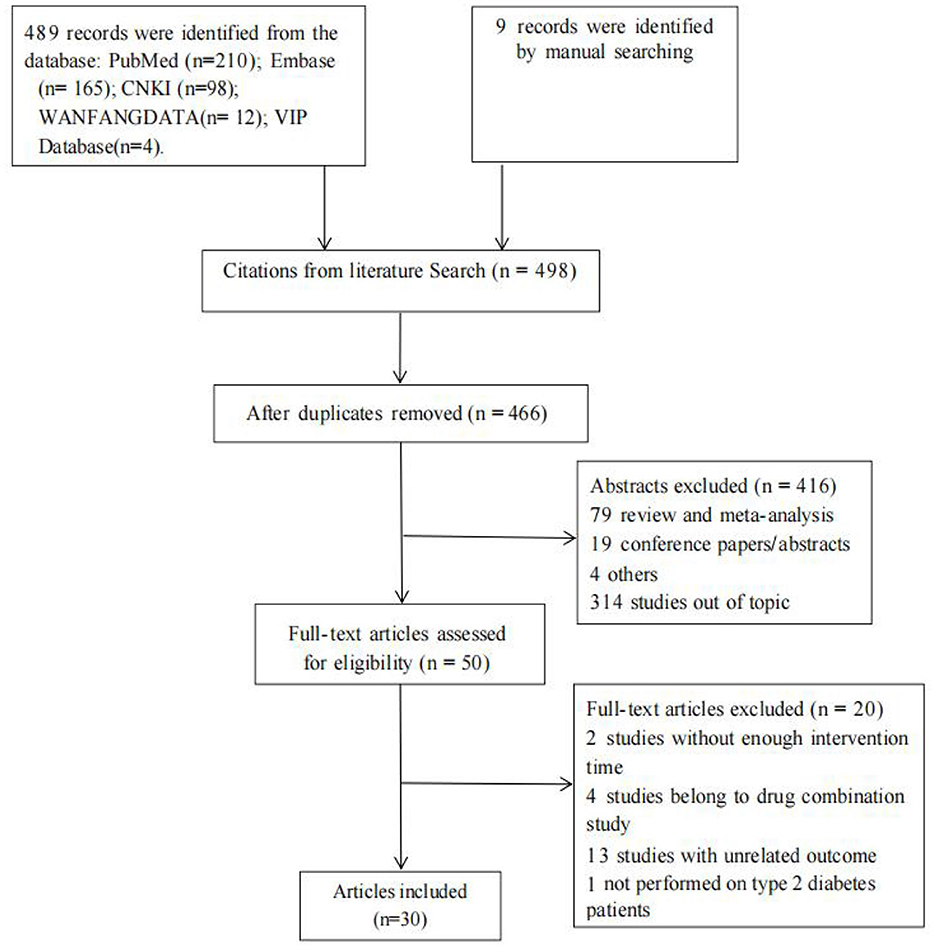
Figure 1. PRISMA flow diagram for the process of study selection.
Of these studies, 14 studies were cohort studies (10–21), six were case–control studies (22–27), eight were nested case–control studies (17, 28–34), and three were cross-sectional studies (35–37). The investigation conducted by Fu (17) consisted of two parts, one is a cohort design about metformin hypoglycemic effect, and the other is a nested case–control design about metformin intolerance. Thus, we divided this investigation into two different studies in the following qualitative description and meta-analysis. Characteristics of individual studies were described in Table 1.
A total of 14, 3, and 6 single nucleotide polymorphisms (SNPs) in SLC22A1, SLC22A2, and SLC22A3, respectively, were investigated for their association with metformin response and intolerance. These studies were mostly conducted in Caucasian and Asian populations. The Q-Genie tool indicated that 5 studies were of high quality, 13 were of moderate quality, and 13 were of low quality (Supplementary Table 3). The details of genetic variants and relevant genetic association studies are shown in Table 2.
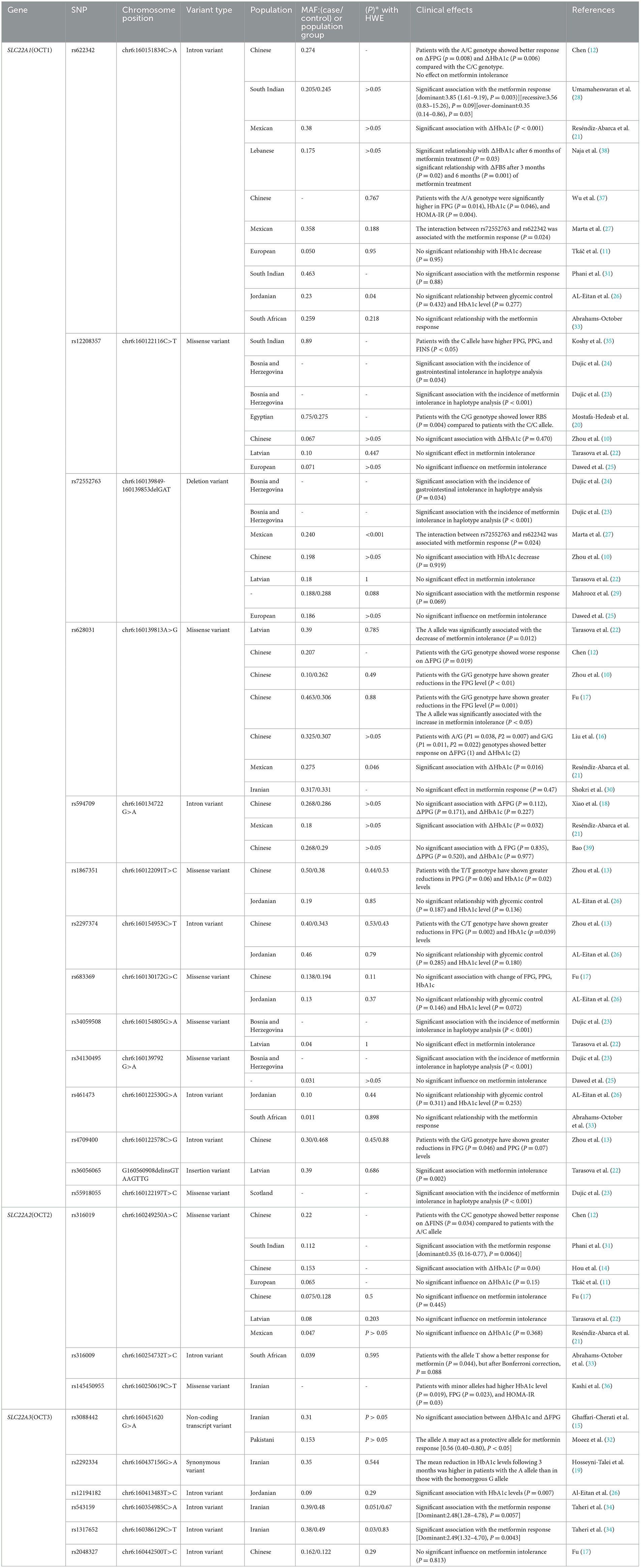
Table 2. Characteristics of genetic variants and related genetic association study.
3.2. Genetic effects of SLC22A1 polymorphisms on metformin response and intolerance
A total of 25 studies evaluated the genetic effects of 14 polymorphisms of SLC22A1 on metformin response and intolerance. These studies were mainly performed in nine countries: five countries in Asia, two in Europe, one in Latin America, and one in Africa. There were 11 cohort studies, 6 case–control studies, 6 nested case–control studies, and 2 cross-sectional studies, respectively. All details are presented in Table 1.
rs622342 is the most commonly studied SLC22A1 variant, and 10 studies (11, 12, 21, 26–28, 31, 33, 37, 38) assessed the association between rs622342 polymorphism and metformin responses. Six studies (12, 21, 27, 28, 37, 38) found a significant association with metformin responses in East Asian, South Asian, Middle Eastern, and Latin American populations, which was reflected by the change in HbA1c and FPG levels. While four studies (11, 26, 31, 33) found no association in South Asian, African, European, and Middle Eastern populations, one study found that rs622342 polymorphism was not associated with metformin intolerance in Chinese people. After further meta-analysis, rs622342 polymorphism was found to be substantially related to the change of HbA1c level (AA vs. AC: SMD [95% CI] = −0.45 [−0.73−0.18]; P = 0.001; PQ = 0.742, I2 = 0.0%) (Table 3, Figure 2). But no association was found between rs622342 polymorphism and the effectiveness rate of metformin response (Supplementary Table 4).
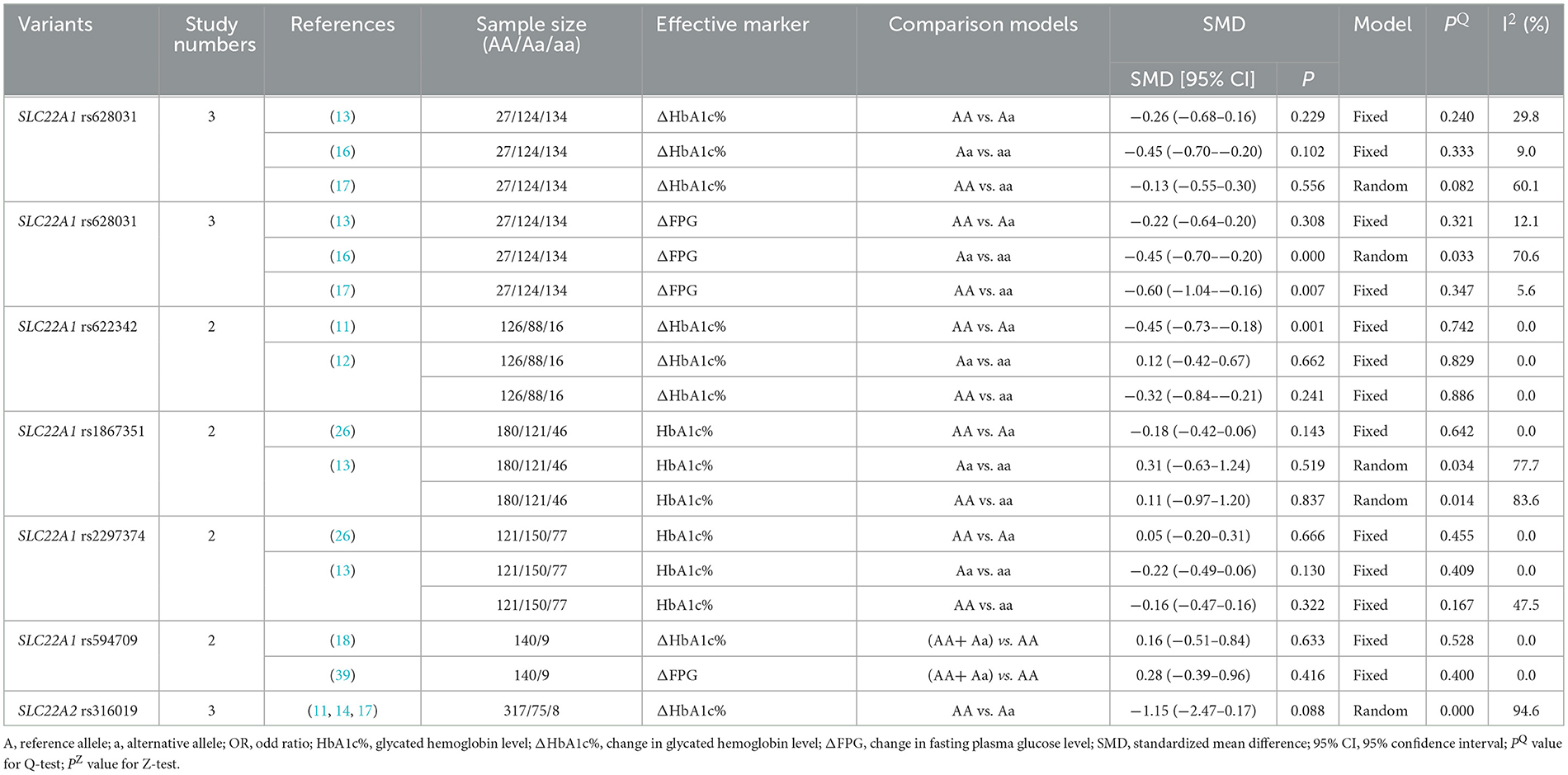
Table 3. The pooled SMD (95% CIs) in meta-analysis for the association between potential SNPs and glycemic response.
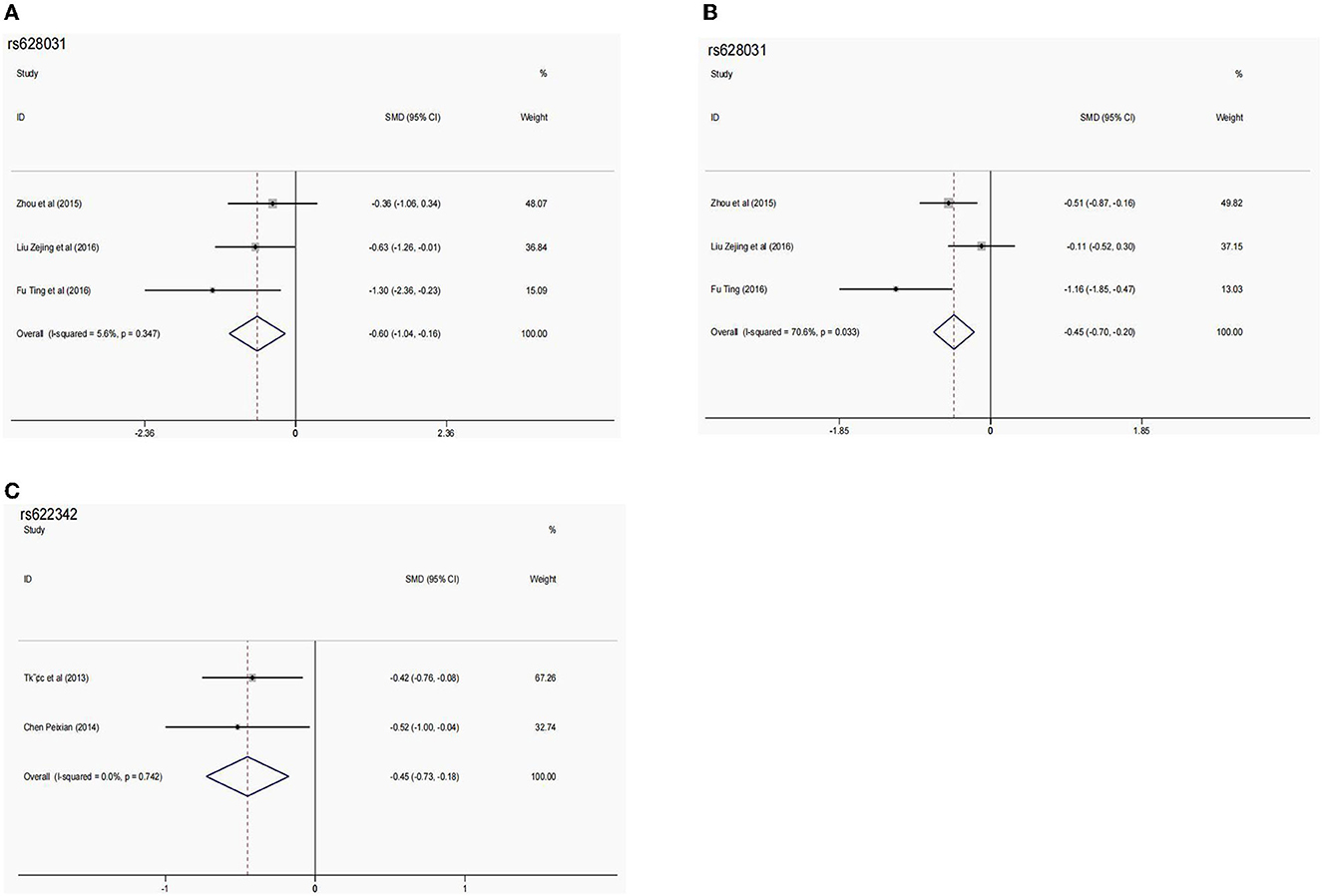
Figure 2. The forest plots for the association between SNPs and the metformin effect. (A) Forest plots of SLC22A1 rs628031 and ΔFPG (AA vs. aa). (B) Forest plots of SLC22A1 rs628031 and ΔFPG (Aa vs. aa). (C) Forest plots of SLC22A1 rs622342 and ΔHbA1c% (AA vs. Aa).
rs12208357 and rs72552763 polymorphisms were assessed in nine studies (10, 20, 22–25, 27, 29, 35). Three studies (20, 27, 35) demonstrated that rs12208357 and rs72552763 were significantly associated with metformin response in South Asian, African, and Latin American populations. Two studies (23, 24) reported that these two variants were associated with metformin intolerance in haplotype analysis in West European populations. Four studies (10, 22, 25, 29) showed no association in European and East Asian populations. Due to differences in study design and outcome indicators, data from related studies cannot be combined for meta-analysis.
rs628031 polymorphism was assessed by seven studies (12, 13, 16, 17, 21, 22, 30); six of them (12, 13, 16, 17, 21, 30) performed in Chinese people found significant associations between rs628031 polymorphism and metformin response, and two of them (17, 22) found that rs628031 polymorphism was significantly associated with metformin intolerance. Our meta-analysis showed that the GG genotype mediated a significantly increased change in FPG compared with AA genotype (SMD [95% CI] = −0.60 [−1.04–−0.16]; P = 0.007; PQ = 0.347; I2 = 5.6%) and AG genotype (−0.45 [−0.70–−0.20]; p = 0.000; PQ = 0.033, I2 = 70.6%) (Table 3, Figure 2). However, the result of the meta-analysis showed no association between this variant and metformin intolerance (Supplementary Table 4).
rs594709 polymorphism was evaluated by three studies (18, 21, 39) in East Asian and Latin American populations. The Latin American study found a significant correlation between rs594709 polymorphism and metformin hypoglycemic effect, while two studies conducted in China and our meta-analysis did not find such a correlation (Table 3). No studies have researched the relationship between rs594709 and metformin intolerance.
rs1867351, rs2297374, rs683369, rs34059508, rs34130495, and rs461473 polymorphisms were respectively assessed in two studies (13, 17, 22, 23, 25, 26, 33) in East Asian, European, and South African populations. rs1867351 and rs2297374 polymorphisms were reported to be associated with metformin for reducing blood glucose, but the results were the opposite in relevant research studies (13, 26). rs34059508 (22, 23) and rs34130495 polymorphisms (23, 25) were also reported with inconsistent results on the effect of these genetic variants on metformin intolerance. Studies showed that rs683369 (17, 26) and rs461473 polymorphisms (26, 33) were unrelated to metformin response. The pooled results showed that rs1867351 and rs2297374 polymorphisms were uncorrelated with the metformin hypoglycemic effect (Table 3). Other variants were not included in the meta-analysis due to the difference in clinical endpoints or insufficiency of genotype data. The remaining SLC22A1 polymorphisms (rs4709400, rs36056065, and rs55918055) were assessed only in a single study in East Asian and European populations. The rs4709400 (13) polymorphism was reported to be related to hypoglycemic response and rs36056065 (22) and rs55918055 polymorphisms (23) were associated with metformin intolerance.
3.3. Genetic effects of SLC22A2 polymorphisms on metformin response and intolerance
Ten studies assessed the effect of SLC22A2 polymorphisms (rs316019, rs316009, and rs145450955) on metformin response and intolerance in six countries involving Asian and Caucasian populations.
The rs316019 polymorphism is the most studied SLC22A2 variant, and seven studies (11, 12, 14, 17, 21, 22, 31) evaluated genetic association with metformin response or intolerance. Three studies reported that rs316019 polymorphism was associated with metformin response in East Asian (12, 14) and South Asian populations (31). The remaining studies showed that this variant was unrelated to metformin response (11, 21) and intolerance (17, 22) in East Asian, Latin American, and European populations. The heterogeneity test displayed high heterogeneity among studies (PQ < 0.001, I2 = 94.6%) (Table 3).
The rs316009 polymorphism was only evaluated in African populations (33), and the study showed that the T allele has a better effect on metformin response. rs145450955 polymorphism was reported in Middle Eastern populations (36) in which patients with minor alleles exhibited worse metformin response. The results of these two variants were not pooled as they did not meet the criteria of meta-analysis.
3.4. Genetic effects of SLC22A3 polymorphisms on metformin response and intolerance
Six studies (15, 17, 19, 26, 32, 34) reported the associations between SLC22A3 polymorphisms (rs3088442, rs2292334, rs12194182, rs543159, rs1317652, and rs2048327) and metformin response or intolerance in Middle Eastern and East Asian populations.
The rs3088442 polymorphism has been investigated in two studies, which have reached opposite conclusions regarding metformin response in Middle Eastern populations (15, 32). rs2292334 (19), rs12194182 (26), rs543159 (34), and rs1317652 (34) were identified as being related to metformin response in Middle Eastern populations, respectively; in one study, rs2048327 polymorphism was reported to be unrelated to metformin intolerance in East Asian populations (17). The meta-analysis was not conducted due to the limited studies and different clinical outcomes.
4. Discussion
Metformin is a first-line hypoglycemic agent for T2DM patients; however, the individual metformin bioavailability is highly variable (39), which results in variation in metformin response and intolerance. The OCT genetic polymorphisms have been be considered as contributing factors to these variations. This review qualitatively and quantitatively summarized the genetic effect of SLC22A1, SLC22A2, and SLC22A3 polymorphisms, respectively, on metformin response and intolerance. The pooled result showed that SLC22A1 rs628031 and rs622342 polymorphisms were associated with hypoglycemic response to metformin, suggesting that SLC22A1 polymorphisms play a vital role in metformin pharmacokinetics. Most of the studies were rated as low to moderate in quality due to inadequacies in identifying bias sources, sample size, power analysis, and statistical methods for controlling confounding. More high-quality studies are needed to verify these associations.
OCT1 (SLC22A1) is mainly expressed on the basolateral side of hepatocytes and intestinal epithelial cells, and many studies have testified that OCT1 was involved in metformin transport in the intestine and liver (40, 41). In recent years, the effect of SLC22A1 polymorphisms on metformin treatment has been extensively studied with inconsistent outcomes. rs622342 is the most common SLC22A1 intronic variant (42). Numerous studies have reported that the C allele mediated a diminished metformin glucose-lowering effect (27, 37, 42). The rs622342 polymorphism, although not changing the amino acid sequence, may affect the gene expression of OCT1 transport function. Our meta-analysis found that the AC genotype had a higher HbA1c reduction than the CC genotype with no significant heterogeneity. However, conflicting with these results, Dujic et al. suggested that rs622342 polymorphism has contributed little to variability in glycemic response to metformin monotherapy in T2DM patients of European ancestry (8). The discrepancy in these findings may be due to the differences in study ethnicity, sample size, and the definition of glycemic response, leading to different conclusions. rs628031 is a frequent missense variant that changes methionine to valine at position 408 (Met408Val) in the OCT1 functional protein (42), which was reported to be associated with decreased OCT1 mRNA expression in enterocytes and subsequently decreased intestinal metformin absorption and plasma concentration (43). rs628031 variant was reported with different effects on metformin response across various populations (12, 16, 17, 21, 30, 42, 44). Our meta-analysis specifically focusing on the Chinese population showed that variant homozygous exhibited greater reductions in FPG level compared with wild homozygous and variant heterozygous after metformin monotherapy. However, as only three primary studies were included in the meta-analysis, with small sample size and considerable heterogeneity, this conclusion should be cautiously drawn. There are still many SLC22A1 polymorphisms (e.g., rs12208357, rs72552763, and rs34130495) reported to be associated with metformin response in small studies (13, 16–18, 26, 39). However, the meta-analysis of the MetGen cohort showed no significant association between SLC22A1 variants (rs12208357 and rs72552763) and glycemic response to metformin monotherapy in European populations (8). Given the heterogeneity from the clinic and methodology in different studies reflected by the Q-Genie tool, definite conclusions about associations of the above-mentioned variants with metformin response could not be drawn. Clinical heterogeneity can be attributed to differences in inclusion and exclusion criteria, ethnicity, and intervention, such as therapeutic dose, treatment course, dosage form, and patient compliance. Methodology heterogeneity is mainly from study design, sample size, and genotyping technology. Additionally, the result of the heterogeneity test may be imprecise and biased when there were few studies included in the meta-analysis (45). Morphine is another good substrate of OCT1, and gene variants related to morphine have also been widely studied (46, 47). More research studies are required to clarify the roles of pharmacogenomic variants on metformin in certain ethnic groups.
Gastrointestinal metformin intolerance is the most frequent side effect associated with metformin usage, and several studies have used its occurrence to evaluate metformin safety. OCT1 is partly responsible for metformin absorption from the intestinal lumen, and it has been suggested that reduced OCT1 could increase intestine local metformin concentration, leading to gastrointestinal intolerance (48). Common genetic polymorphisms associated with reduced-function of OCT1 include rs12208357, rs72552763, rs34130495, and rs3405950 (49). Several population observational studies (22–25) have explored the association between these polymorphisms and metformin intolerance in European populations, but the results obtained are not always consistent. However, due to limited studies, we were unable to perform a meta-analysis on these polymorphisms. In addition, we observed significant heterogeneity among these studies regarding sample size, definition of metformin intolerance, and analytical methods. Furthermore, larger multicenter studies are needed to clarify the associations between OCT1 polymorphisms and metformin intolerance.
OCT2 (SLC22A2), another isoform of the OCT family, is highly expressed at the basolateral membrane of renal tubule epithelium and is mainly engaged in metformin excretion in the kidney (50). A number of SLC22A2 variants that can alter OCT2 transport function and affect glycemic response to metformin have been screened out in different populations (51). rs316019 is the most studied SLC22A2 polymorphism. According to the pharmacokinetics study (14), the mutant allele of rs316019 may enhance the metformin glucose-lowering effect by delaying elimination. In this review, seven studies (11, 12, 14, 17, 21, 22, 31) evaluated the effect of rs316019 on metformin response or intolerance. However, our meta-analysis suggested that the rs316019 variant is not related to metformin response with significant population heterogeneity, which is in keeping with the result of the MetGen cohort performed in European populations (8). Moreover, the association between rs316019 polymorphisms and cisplatin-induced nephrotoxicity was reported extensively in clinical studies on genotype-guided prescribing (52–54). rs316009 and rs145450955 polymorphisms were reported in one study, respectively, in African (33) and Middle Eastern populations (36), and further genetic association studies are needed in the future.
OCT3 (SLC22A3), distributed widely in the intestine, muscle, and adipose tissue, also has a certain effect on metformin transport (55). A pharmacologic study (56) showed that SLC22A3 variants were correlated with reduced uptake activity of metformin. However, SLC22A3 variants have only been reported in a few population studies so far, and the result of the Q-Genie assessment suggested that the existing studies lack discussion of sources of bias and statistical methods for controlling confounding factors. Moreover, the sample size and power were not large enough to obtain statistically significant results. Therefore, it is difficult to assume an association between SLC22A3 polymorphisms and metformin response and intolerance at present. More pharmacologic studies are required to characterize the molecular mechanism of OCT3 for transporting metformin, and well-designed multicenter RCTs should be conducted to confirm relevant findings.
There are several limitations in this review. First, due to differences in study design and outcome measures, there were limited studies accessible for meta-analysis, making it unable to further perform subgroup analysis, and meta-regression analysis to explore the source of heterogeneity. Second, variations in ethnic background and study quality were significant in studies on certain variants, so the conclusion should be cautiously drawn. Furthermore, we were unable to exclude the effect of diet and lifestyle modifications on metformin response on account of insufficient information provided by primary studies. Finally, articles written in other languages and unpublished articles with negative results were not included, which may lead to unavoidable selection bias and publication bias. Meanwhile, we were unable to check publication bias with Egger's and/or Begg–Mazumdar's test and Funnel plot due to the limited number of articles. Despite these limitations, we have summarized the effect of OCT genetic variants on metformin monotherapy as comprehensively as possible and discussed the limitations and shortcomings of current genetic association studies, which provide steering suggestions for follow-up research.
In conclusion, SLC22A1 rs622342 and rs628031 polymorphisms were associated with metformin response, but these associations should be confirmed in more high-quality studies. Further research is also required to confirm the physiological function of OCTs and how it relates to clinical outcomes. Knowledge of the genetic effects of OCT genetic polymorphisms may provide new insights into gene-oriented personalized medicine for diabetes. With increasing international cooperation and accumulating metformin pharmacogenetic data, we hope to see uncontested data converted into clinical practice.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
Author contributions
JY and WH designed the entire study. YX, XL, and XC collected and analyzed the data. AP and CG wrote the manuscript. All authors read and approved the final manuscript.
Funding
This study was supported by the Sanming Project of Medicine of Shenzhen (SZSM201811057), the National Natural Science of Guang Dong province (2019A1515010358), Guangdong Medical Research Fund Project (2017196), and the Central South University Graduate Research Innovation Program (1053320215942).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1183879/full#supplementary-material
References
1. Zheng Y, Ley SH, Hu FB. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat Rev Endocrinol. (2018) 14:88–98. doi: 10.1038/nrendo.2017.151
2. Sun H, Saeedi P, Karuranga S, Pinkepank M, Ogurtsova K, Duncan BB, et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. (2022) 183:109119. doi: 10.1016/j.diabres.2021.109119
3. Cook MN, Girman CJ, Stein PP, Alexander CM. Initial monotherapy with either metformin or sulphonylureas often fails to achieve or maintain current glycaemic goals in patients with Type 2 diabetes in UK primary care. Diabet Med. (2007) 24:350–8. doi: 10.1111/j.1464-5491.2007.02078.x
4. Ieiri I, Takane H, Hirota T, Otsubo K, Higuchi S. Genetic polymorphisms of drug transporters: pharmacokinetic and pharmacodynamic consequences in pharmacotherapy. Expert Opin Drug Metab Toxicol. (2006) 2:651–74. doi: 10.1517/17425255.2.5.651
5. Adak T, Samadi A, Ünal AZ, Sabuncuoglu S. A reappraisal on metformin. Regulat Toxicol Pharmacol. (2018) 92:324–32. doi: 10.1016/j.yrtph.2017.12.023
6. Graham GG, Punt J, Arora M, Day RO, Doogue MP, Duong JK, et al. Clinical pharmacokinetics of metformin. Clin Pharmacokinet. (2011) 50:81–98. doi: 10.2165/11534750-000000000-00000
7. Fahrmayr C, Fromm MF, König J. Hepatic OATP and OCT uptake transporters: Their role for drug-drug interactions and pharmacogenetic aspects. Drug Metab Rev. (2010) 42:380–401. doi: 10.3109/03602530903491683
8. Dujic T, Zhou K, Yee SW, van Leeuwen N, de Keyser CE, Javorský M, et al. Variants in pharmacokinetic transporters and glycemic response to metformin: a metgen meta-analysis. Clin Pharmacol Ther. (2017) 101:763–72. doi: 10.1002/cpt.567
9. Sohani ZN, Meyre D, de Souza RJ, Joseph PG, Gandhi M, Dennis BB, et al. Assessing the quality of published genetic association studies in meta-analyses: the quality of genetic studies (Q-Genie) tool. BMC Genet. (2015) 16:50. doi: 10.1186/s12863-015-0211-2
10. Zhou K, Donnelly LA, Kimber CH, Donnan PT, Doney AS, Leese G, et al. Reduced-function SLC22A1 polymorphisms encoding organic cation transporter 1 and glycemic response to metformin: a GoDARTS study. Diabetes. (2009) 58:1434–9. doi: 10.2337/db08-0896
11. Tkáč I, Klimčáková L, Javorský M, Fabianová M, Schroner Z, Hermanová H, et al. Pharmacogenomic association between a variant in SLC47A1 gene and therapeutic response to metformin in type 2 diabetes. Diabetes Obes Metab. (2013) 15:189–91. doi: 10.1111/j.1463-1326.2012.01691.x
12. Chen P. Effect of SLC22A1, SLC22A2, SLC47A1, SLC47A2, ATM gene polymorphism on response of the efficacy the adverse reaction of metformin in type 2 diabetes. Shantou University, (2014). Available online at: https://d.wanfangdata.com.cn/thesis/ChJUaGVzaXNOZXdTMjAyMjAzMjMSB0Q1OTgxMDUaCGJ6MmptbWZm (accessed December 26, 2022).
13. Zhou Y, Ye W, Wang Y, Jiang Z, Meng X, Xiao Q, et al. Genetic variants of OCT1 influence glycemic response to metformin in Han Chinese patients with type-2 diabetes mellitus in Shanghai. Int J Clin Exp Pathol. (2015) 8:9533–42.
14. Hou W, Zhang D, Lu W, Zheng T, Wan L, Li Q, et al. Polymorphism of organic cation transporter 2 improves glucose-lowering effect of metformin via influencing its pharmacokinetics in Chinese type 2 diabetic patients. Mol Diagn Ther. (2015) 19:25–33. doi: 10.1007/s40291-014-0126-z
15. Ghaffari-Cherati M, Mahrooz A, Hashemi-Soteh MB, Hosseyni-Talei SR, Alizadeh A, Nakhaei SM. Allele frequency and genotype distribution of a common variant in the 3'-untranslated region of the SLC22A3 gene in patients with type 2 diabetes: Association with response to metformin. J Res Med Sci. (2016) 21:92. doi: 10.4103/1735-1995.192508
16. Liu Z, Liu X, Li J, Wang J, Liu Q. association between SLC22A1,SLC22A4 gene polymorphisms and therapeutic efficacy of metformin in type 2 diabetes mellitus. J Clin Lab Sci. (2016) 34:564–8. doi: 10.13602/j.cnki.jcls.2016.07.07
17. Fu T. Correlations between genetic variations of transports with the gastrointestinal side effect and therapeutic efficacy of metformin in patients with type 2 diabetes. Hebei Medical University (2016).
18. Xiao D, Guo Y, Li X, Yin JY, Zheng W, Qiu XW, et al. The impacts of SLC22A1 rs594709 and SLC47A1 rs2289669 polymorphisms on metformin therapeutic efficacy in Chinese type 2 diabetes patients. Int J Endocrinol. (2016) 2016:4350712. doi: 10.1155/2016/4350712
19. Hosseyni-Talei SR, Mahrooz A, Hashemi-Soteh MB, Ghaffari-Cherati M, Alizadeh A. Association between the synonymous variant organic cation transporter 3 (OCT3)-1233G>A and the glycemic response following metformin therapy in patients with type 2 diabetes. Iran J Basic Med Sci. (2017) 20:250–5. doi: 10.22038/IJBMS.2017.8351
20. Mostafa-Hedeab G, Mohamed AA, Ebid GT, Sabry D, Salam RF, Hassen ME. Effect of MATE 1, MATE 2 and OCT1 single nucleotide polymorphisms on metformin action in recently diagnosed egyptian type-2 diabetic patients. Biomed Pharmacol J. (2018) 11:149–57. doi: 10.13005/bpj/1356
21. Reséndiz-Abarca CA, Flores-Alfaro E, Suárez-Sánchez F, Cruz M, Valladares-Salgado A, del Carmen Alarcón-Romero L, et al. Altered glycemic control associated with polymorphisms in the SLC22A1 (OCT1) gene in a mexican population with type 2 diabetes mellitus treated with metformin: a cohort study. J Clin Pharmacol. (2019) 59:1384–90. doi: 10.1002/jcph.1425
22. Tarasova L, Kalnina I, Geldnere K, Bumbure A, Ritenberga R, Nikitina-Zake L, et al. Association of genetic variation in the organic cation transporters OCT1, OCT2 and multidrug and toxin extrusion 1 transporter protein genes with the gastrointestinal side effects and lower BMI in metformin-treated type 2 diabetes patients. Pharmacogenet Genomics. (2012) 22:659–66. doi: 10.1097/FPC.0b013e3283561666
23. Dujic T, Zhou K, Donnelly LA, Tavendale R, Palmer CN, Pearson ER. Association of Organic Cation Transporter 1 With Intolerance to Metformin in Type 2 Diabetes: A GoDARTS Study. Diabetes. (2015) 64:1786–93. doi: 10.2337/db14-1388
24. Dujic T, Causevic A, Bego T, Malenica M, Velija-Asimi Z, Pearson ER, et al. Organic cation transporter 1 variants and gastrointestinal side effects of metformin in patients with Type 2 diabetes. Diabet Med. (2016) 33:511–4. doi: 10.1111/dme.13040
25. Dawed AY, Zhou K, van Leeuwen N, Mahajan A, Robertson N, Koivula R, et al. Variation in the plasma membrane monoamine transporter (PMAT) (Encoded by SLC29A4) and organic cation transporter 1 (OCT1) (Encoded by SLC22A1) and gastrointestinal intolerance to metformin in type 2 diabetes: An IMI DIRECT study. Diabetes Care. (2019) 42:1027–33. doi: 10.1101/436980
26. Al-Eitan LN, Almomani BA, Nassar AM, Elsaqa BZ, Saadeh NA. Metformin pharmacogenetics: effects of SLC22A1, SLC22A2, and SLC22A3 polymorphisms on glycemic control and HbA1c Levels. J Pers Med. (2019) 9:17. doi: 10.3390/jpm9010017
27. Marta M, Sánchez-Pozos K, Jaimes-Santoyo J, Monroy-Escutia J, Rivera-Santiago C, de Los Ángeles Granados-Silvestre M, et al. Pharmacogenetic evaluation of metformin and Sulphonylurea response in Mexican mestizos with type 2 diabetes. Curr Drug Metab. (2020) 21:291–300. doi: 10.2174/1389200221666200514125443
28. Umamaheswaran G, Praveen RG, Damodaran SE, Das AK, Adithan C. Influence of SLC22A1 rs622342 genetic polymorphism on metformin response in South Indian type 2 diabetes mellitus patients. Clin Exp Med. (2015) 15:511–7. doi: 10.1007/s10238-014-0322-5
29. Mahrooz A, Parsanasab H, Hashemi-Soteh MB, Kashi Z, Bahar A, Alizadeh A, et al. The role of clinical response to metformin in patients newly diagnosed with type 2 diabetes: a monotherapy study. Clin Exp Med. (2015) 15:159–65. doi: 10.1007/s10238-014-0283-8
30. Shokri F, Ghaedi H, Ghafouri Fard S, Movafagh A, Abediankenari S, Mahrooz A, et al. Impact of ATM and SLC22A1 polymorphisms on therapeutic response to metformin in Iranian diabetic patients. Int J Mol Cell Med. (2016) 5:1–7.
31. Phani NM, Vohra M, Kakar A, Adhikari P, Nagri SK, D'Souza SC, et al. Implication of critical pharmacokinetic gene variants on therapeutic response to metformin in Type 2 diabetes. Pharmacogenomics. (2018) 19:905–11. doi: 10.2217/pgs-2018-0041
32. Moeez S, Riaz S, Masood N, Kanwal N, Arif MA, Niazi R, et al. Evaluation of the rs3088442 G>A SLC22A3 Gene polymorphism and the role of microRNA 147 in groups of adult Pakistani populations with type 2 diabetes in response to metformin. Can J Diabetes. (2019) 43:128–135.e3. doi: 10.1016/j.jcjd.2018.07.001
33. Abrahams-October Z, Xhakaza L, Pearce B, Mandisa Masilela C, Benjeddou M, Vincent Adeniyi O, et al. Genetic association of solute carrier transporter gene variants with metformin response. Balkan J Med Genet. (2021) 24:47–56. doi: 10.2478/bjmg-2021-0004
34. Taheri R, Kazerouni F, Mirfakhraei R, Kalbasi S, Shahrokhi SZ, Rahimipour A. The influence of SLC22A3 rs543159 and rs1317652 genetic variants on metformin therapeutic efficacy in newly diagnosed patients with type 2 diabetes mellitus: 25 weeks follow-up study. Gene. (2022) 823:146382. doi: 10.1016/j.gene.2022.146382
35. Koshy M, Sethupathy S, Annamalai PT, Renju VC, Santha K. Association of oct1 gene polymorphism with glycemic status and serum metformin levels in type ii diabetes mellitus patients. Int J Pharmac Sci Res. (2013) 4:1940–5. Available online at: www.ijpsr.com
36. Kashi Z, Masoumi P, Mahrooz A, Hashemi-Soteh MB, Bahar A, Alizadeh A. The variant organic cation transporter 2 (OCT2)-T201M contribute to changes in insulin resistance in patients with type 2 diabetes treated with metformin. Diabetes Res Clin Pract. (2015) 108:78–83. doi: 10.1016/j.diabres.2015.01.024
37. Wu K, Li X, Xu Y, Zhang X, Guan Z, Zhang S, et al. SLC22A1 rs622342 polymorphism predicts insulin resistance improvement in patients with type 2 diabetes mellitus treated with metformin: a cross-sectional study. Int J Endocrinol. (2020) 2020:2975898. doi: 10.1155/2020/2975898
38. Naja K, El Shamieh S, Fakhoury R. rs622342A>C in SLC22A1 is associated with metformin pharmacokinetics and glycemic response. Drug Metab Pharmacokinet. (2020) 35:160–4. doi: 10.1016/j.dmpk.2019.10.007
39. Bao X. Study on transporter gene polymorphism metformin individ ualized medication in Mongolian type 2 diabetes patients in Tong liao area, Inner Mongolia. Inner Mongolia Nationality University (2021). Available online at: https://d.wanfangdata.com.cn/thesis/ChJUaGVzaXNOZXdTMjAyMjAzMjMSCUQwMjQ3NjU5NBoINzhrbHh0ams= (accessed January 5, 2023).
40. Kimura N, Masuda S, Tanihara Y, Ueo H, Okuda M, Katsura T, et al. Metformin is a superior substrate for renal organic cation transporter OCT2 rather than hepatic OCT1. Drug Metab Pharmacokinet. (2005) 20:379–86. doi: 10.2133/dmpk.20.379
41. Koehler MR, Wissinger B, Gorboulev V, Koepsell H, Schmid M. The two human organic cation transporter genes SLC22A1 and SLC22A2 are located on chromosome 6q26. Cytogenet Cell Genet. (1997) 79:198–200. doi: 10.1159/000134720
42. Becker ML, Visser LE, van Schaik RH, Hofman A, Uitterlinden AG, Stricker BH. Genetic variation in the organic cation transporter 1 is associated with metformin response in patients with diabetes mellitus. Pharmacogenomics J. (2009) 9:242–7. doi: 10.1038/tpj.2009.15
43. Semiz S, Dujic T, Causevic A. Pharmacogenetics and personalized treatment of type 2 diabetes. Biochem Med (Zagreb). (2013) 23:154–71. doi: 10.11613/BM.2013.020
44. Chen L, Takizawa M, Chen E, Schlessinger A, Segenthelar J, Choi JH, et al. Genetic polymorphisms in organic cation transporter 1 (OCT1) in Chinese and Japanese populations exhibit altered function. J Pharmacol Exp Ther. (2010) 335:42–50. doi: 10.1124/jpet.110.170159
45. von Hippel PT. The heterogeneity statistic I(2) can be biased in small meta-analyses. BMC Med Res Methodol. (2015) 15:35. doi: 10.1186/s12874-015-0024-z
46. Tzvetkov MV, dos Santos Pereira JN, Meineke I, Saadatmand AR, Stingl JC, Brockmöller J. Morphine is a substrate of the organic cation transporter OCT1 and polymorphisms in OCT1 gene affect morphine pharmacokinetics after codeine administration. Biochem Pharmacol. (2013) 86:666–78. doi: 10.1016/j.bcp.2013.06.019
47. Venkatasubramanian R, Fukuda T, Niu J, Mizuno T, Chidambaran V, Vinks AA, et al. ABCC3 and OCT1 genotypes influence pharmacokinetics of morphine in children. Pharmacogenomics. (2014) 15:1297–309. doi: 10.2217/pgs.14.99
48. Wilcock C, Bailey CJ. Accumulation of metformin by tissues of the normal and diabetic mouse. Xenobiotica. (1994) 24:49–57. doi: 10.3109/00498259409043220
49. Shu Y, Brown C, Castro RA, Shi RJ, Lin ET, Owen RP, et al. Effect of genetic variation in the organic cation transporter 1, OCT1, on metformin pharmacokinetics. Clin Pharmacol Ther. (2008) 83:273–80. doi: 10.1038/sj.clpt.6100275
50. Jonker JW, Schinkel AH. Pharmacological and physiological functions of the polyspecific organic cation transporters: OCT1, 2, and 3 (SLC22A1-3). J Pharmacol Exp Ther. (2004) 308:2–9. doi: 10.1124/jpet.103.053298
51. Leabman MK, Huang CC, Kawamoto M, Johns SJ, Stryke D, Ferrin TE, et al. Polymorphisms in a human kidney xenobiotic transporter, OCT2, exhibit altered function. Pharmacogenetics. (2002) 12:395–405. doi: 10.1097/00008571-200207000-00007
52. Filipski KK, Mathijssen RH, Mikkelsen TS, Schinkel AH, Sparreboom A. Contribution of organic cation transporter 2 (OCT2) to cisplatin-induced nephrotoxicity. Clin Pharmacol Ther. (2009) 86:396–402. doi: 10.1038/clpt.2009.139
53. Yanagisawa R, Kubota N, Hidaka E, Sakashita K, Tanaka M, Nakazawa Y, et al. Cisplatin-induced nephrotoxicity in patients with advanced neuroblastoma. Pediatr Blood Cancer. (2018) 65:e27253. doi: 10.1002/pbc.27253
54. Iwata K, Aizawa K, Kamitsu S, Jingami S, Fukunaga E, Yoshida M, et al. Effects of genetic variants in SLC22A2 organic cation transporter 2 and SLC47A1 multidrug and toxin extrusion 1 transporter on cisplatin-induced adverse events. Clin Exp Nephrol. (2012) 16:843–51. doi: 10.1007/s10157-012-0638-y
55. DeGorter MK, Kim RB. Hepatic drug transporters, old and new: pharmacogenomics, drug response, and clinical relevance. Hepatology. (2009) 50:1014–6. doi: 10.1002/hep.23233
Keywords: organic cation transporters, genetic polymorphisms, type 2 diabetes mellitus, metformin response, metformin intolerance
Citation: Peng A, Gong C, Xu Y, Liang X, Chen X, Hong W and Yan J (2023) Association between organic cation transporter genetic polymorphisms and metformin response and intolerance in T2DM individuals: a systematic review and meta-analysis. Front. Public Health 11:1183879. doi: 10.3389/fpubh.2023.1183879
Received: 10 March 2023; Accepted: 30 June 2023;
Published: 21 July 2023.
Edited by:
Mohammad Safiqul Islam, Noakhali Science and Technology University, BangladeshReviewed by:
Md. Mustafizur Rahman, Khulna University, BangladeshBrendon Pearce, Stellenbosch University, South Africa
Copyright © 2023 Peng, Gong, Xu, Liang, Chen, Hong and Yan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Junxia Yan, 20457456@qq.com; Wenxu Hong, szbloodcenter@hotmail.com
†These authors have contributed equally to this work