 Mengjie Sun
Mengjie Sun Lamei Liu1*
Lamei Liu1* Ronnell Dela Rosa
Ronnell Dela Rosa- 1School of Nursing and Health, Zhengzhou University, Zhengzhou, Henan, China
- 2School of Nursing, Philippine Women's University, Manila, Philippines
Background: Chronic diseases are long-term, recurring and prolonged, requiring frequent travel to and from the hospital, community, and home settings to access different levels of care. Hospital-to-home transition is challenging travel for elderly patients with chronic diseases. Unhealthy care transition practices may be associated with an increased risk of adverse outcomes and readmission rates. The safety and quality of care transitions have gained global attention, and healthcare providers have a responsibility to help older adults make a smooth, safe, and healthy transition.
Objective: This study aims to provide a more comprehensive understanding of what may shape health transitions in older adults from multiple perspectives, including older chronic patients, caregivers, and healthcare providers.
Methods: Six databases were searched during January 2022, including Pubmed, web of science, Cochrane, Embase, CINAHL (EBSCO), and PsycINFO (Ovid). The qualitative meta-synthesis was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) recommendations. The quality of included studies was appraised using the Critical Appraisal Skills Programme (CASP) qualitative research appraisal tool. A narrative synthesis was conducted informed by Meleis's Theory of Transition.
Results: Seventeen studies identified individual and community-focused facilitators and inhibitors mapped to three themes, older adult resilience, relationships and connections, and uninterrupted care transfer supply chain.
Conclusion: This study identified potential transition facilitators and inhibitors for incoming older adults transitioning from hospital to home, and these findings may inform the development of interventions to target resilience in adapting to a new home environment, and human relations and connections for building partnerships, as well as an uninterrupted supply chain of care transfer at hospital-home delivery.
Systematic review registration: www.crd.york.ac.uk/prospero/, identifier: CRD42022350478.
Introduction
With the development of an aging population, chronic disease health problems are becoming increasingly prevalent and the coexistence of multiple diseases is becoming more severe among older adults worldwide (1). Approximately 50% of older adults are reported to have two or more chronic diseases (2). Compared to a single chronic disease, older adults with multiple diseases are associated with poorer quality of life, higher risk of adverse drug events, repeat care, and death (3), increasing the social and medical burden. In this context, with national efforts to reduce the burden of health care, coupled with increased hospital turnaround efficiency and shorter hospital stays, older adults with complex health problems often have more complex needs, requiring multiple health care providers to provide a wide range of health and geriatric care equipment in multiple care settings, as well as frequent transitions between hospital and home (4, 5). Approximately 1 in 5 older patients experienced adverse events during hospital-to-home transitions, including unplanned readmissions within a month of discharge, medication errors, and even death (6–8). These adverse events were associated with uncoordinated, discontinuous transitions of care across healthcare settings (9–12). Improving the safety and quality of care transitions had become a global concern (13, 14).
Transition is defined as the process of changing from one state, or condition to another, which is a complex, multidimensional process that encompasses awareness, engagement, and period (15, 16). Assisting patients in managing life transitions is a key function of nursing (16). The Transition from hospital to home is often a ternary process involving patients, families, and health care providers, and the common goal for the stakeholders involved is that older adults are able to make healthy transitions after discharge from the hospital in accordance with established goals or are supported in problematic transitions of care. According to Meleis' transition theory, healthy transitions are characterized by response patterns that include process indicators (e.g., coping skills) and outcome indicators (e.g., wellbeing). And some transition conditions at the individual level (e.g., cultural beliefs, attitudes, readiness and knowledge related to transition), community level (community resources and support), etc., and social level (e.g., social norms) can facilitate or inhibit healthy transitions (15).
To promote healthy and safe patient transitions, transitional care models have been developed to bridge the gap between patients in different healthcare settings and different levels of care by providing continuous, coordinated care (5, 17). However, there is some controversy about the effectiveness of implementing transitional care interventions (18, 19). Although studies have shown that transitional care has the potential to improve health system efficiency and reduce adverse events and lower patient readmission rates (20, 21), difficulties remain in improving user experience aspects and satisfaction (22, 23). User experience can improve the process and quality of healthcare delivery (4, 24–26). Several studies have focused on user experience and satisfaction in care transitions, and have received some review attention (23, 27–29). The more recent are Hestevik et al. (23), Chen et al. (29), Høy et al. (28), and Joo et al. (27). Høy et al. (28), and Hestevik et al. (23) explored the perspective of older adults and Joo et al. (27) included family caregivers in addition to patients. Chen et al. (29) reviewed the barriers and facilitators of transition care for stroke patients and their caregivers. This was a review of specific diseases. In contrast, the prevalence of multimorbidity in the elderly population is 55–98% (30), requiring us to focus on a broader population of chronic disease, not just the transition of patients with specific diseases. Høy et al. (28) drafted a protocol that focused on exploring patient preferences, challenges, and levels of involvement in care transitions. However, the protocol was only planned to include literature published after 2010. The main results of the more important his review have not been reported. Hestevik et al. (23) examined the experiences of older adults adjusting to daily life at home after discharge from the hospital, synthesizing the results of 13 studies as (i) experiencing an insecure and unsafe transition, (ii) settling into a new situation at home, (iii) what would I do without my informal caregiver? and (iv) experience of a paternalistic medical model. Joo et al. (27) reviewed seven studies to understand the experiences and perceptions of patients with chronic illnesses and their caregivers as they transitioned from a medical setting to home. They reported that the transition from hospital to home was influenced by the following barriers and facilitators: communication with multiple healthcare providers, self-management, and psychological stress and family caregiver support and nurse-provided patient-centered care. However, the study population was patients ≥18 years of age and older with chronic conditions. None of these reviews included studies of health care workers' perceptions of transitions of care for older adults. Without a doubt, patient experience is important for the quality of care during the transition and is considered one of the three cores of healthcare quality (31). Yet the transition of care is a triadic process involving patients, families, and health care professionals. Healthcare professionals, especially nurses, as the primary implementers and providers of transitional care, need to interact with other health care professionals, family members, and others in the transition of care to assess the biological, psychological, social, and emotional needs of the patient, and their perceptions and experiences also influence the patient's health transition (24, 32, 33).
Researchers have not identified a published systematic review examining the transition conditions of older adults from hospital to home that has included older adults, caregivers, and health care providers. To achieve this goal, researchers need to understand what facilitates and inhibits the transition process from the perspective of older adults, their family caregivers, and health care providers. The study aims to address this question: a more comprehensive understanding of what facilitates or inhibits the transition of older adults transitioning from hospital to home from multiple perspectives, based on Meleis' transition theory, is important for an evidence-based approach to developing interventions for care transitions.
Methods
Design
This is a systematic evaluation and meta-synthesis of qualitative research. Qualitative synthesis follows the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA).
The study aimed to address the following question: What facilitates or hinders the transition for older adults from hospital to home? We used the SPICE framework (34) to formulate the review question. “Setting (where): healthcare facility, patient's home” “Perspective (for whom?): older adults transitioning from hospital to home, their caregivers, and health care providers” “Phenomena of interest: transition from hospital to home” “Comparison: not applicable” “Evaluation (with what results?): experiences, perceptions, facilitators, inhibitors.”
Search strategy
A systematic electronic databases search was conducted during January 2022 for all English articles in six databases, including Pubmed, Web of Science, Cochrane, Embase, CINAHL (EBSCO), and PsycINFO (Ovid). There were no limitations on the year of publication. Searches were based on a combination of free-text keywords and indexed terms (MeSH) related to the terms: aged, elderly, chronic disease, transitional care, patient discharge, patient transfer, continuity of patient care, discharge, discharged home, transition, hospital-to-home, and qualitative research etc. (See Supplementary File 1 for search strategy).
Inclusion/exclusion criteria
Inclusion criteria: qualitative studies or mixed studies for which qualitative data could be extracted were included, including but not limited to phenomenological, root theory, and ethnographic studies; focus on multiple chronic conditions rather than one specific condition, as studies focusing on a single condition are too specific and not necessarily generalizable to older adults with multiple chronic conditions; all studies included older adults who were at least 60 years of age, as this is the World Health Organization definition of older adults; published in English.
Exclusion criteria: focus on the overall hospital/discharge experience rather than the transition experience from hospital to home; transition to a nursing home or specialized palliative care facility or rehabilitation center; conference proceedings or abstracts, review articles, editorials, clinical case reports, or review articles; articles collected using qualitative methods but analyzed using quantitative analysis; non-English language literature.
An initial search yielded a total of 3,129 articles. Two researchers independently screened and extracted literature by inclusion and exclusion criteria. The remaining 2,384 articles after removing duplicate literature. In addition, 117 papers remained after reading the titles and abstracts and 100 papers were deleted after reading the full text, for a total of 17 included studies. Seventeen papers were not deleted after quality assessment. The PRISMA flow chart was used in this process (Figure 1).
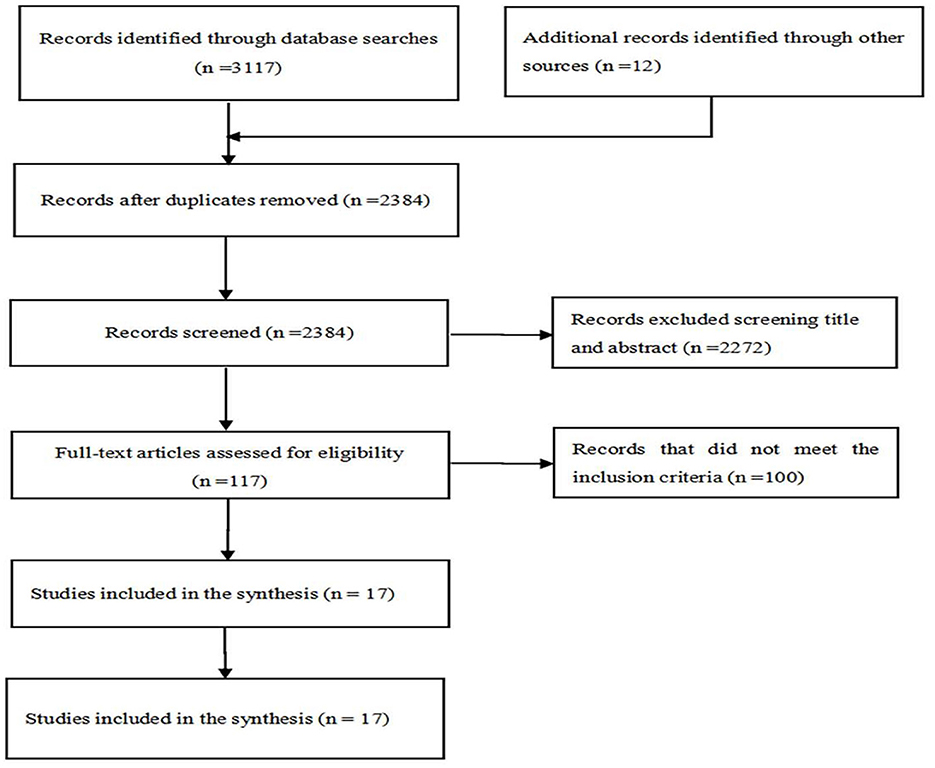
Figure 1. PRISMA flow diagram.
Quality appraisal
The Qualitative studies were appraised using The Critical Appraisal Skills Programme (2013) qualitative checklist comprising 10 items relating to rigor, credibility and relevance of qualitative studies (35). All items were scored as “yes” or “no” or “can't tell.” Studies were scored as “high” or “medium” or “low” quality. Quality evaluations were performed by two independent authors, and when disagreements were encountered, a third author moderated. The final evaluation results are shown in Table 1.
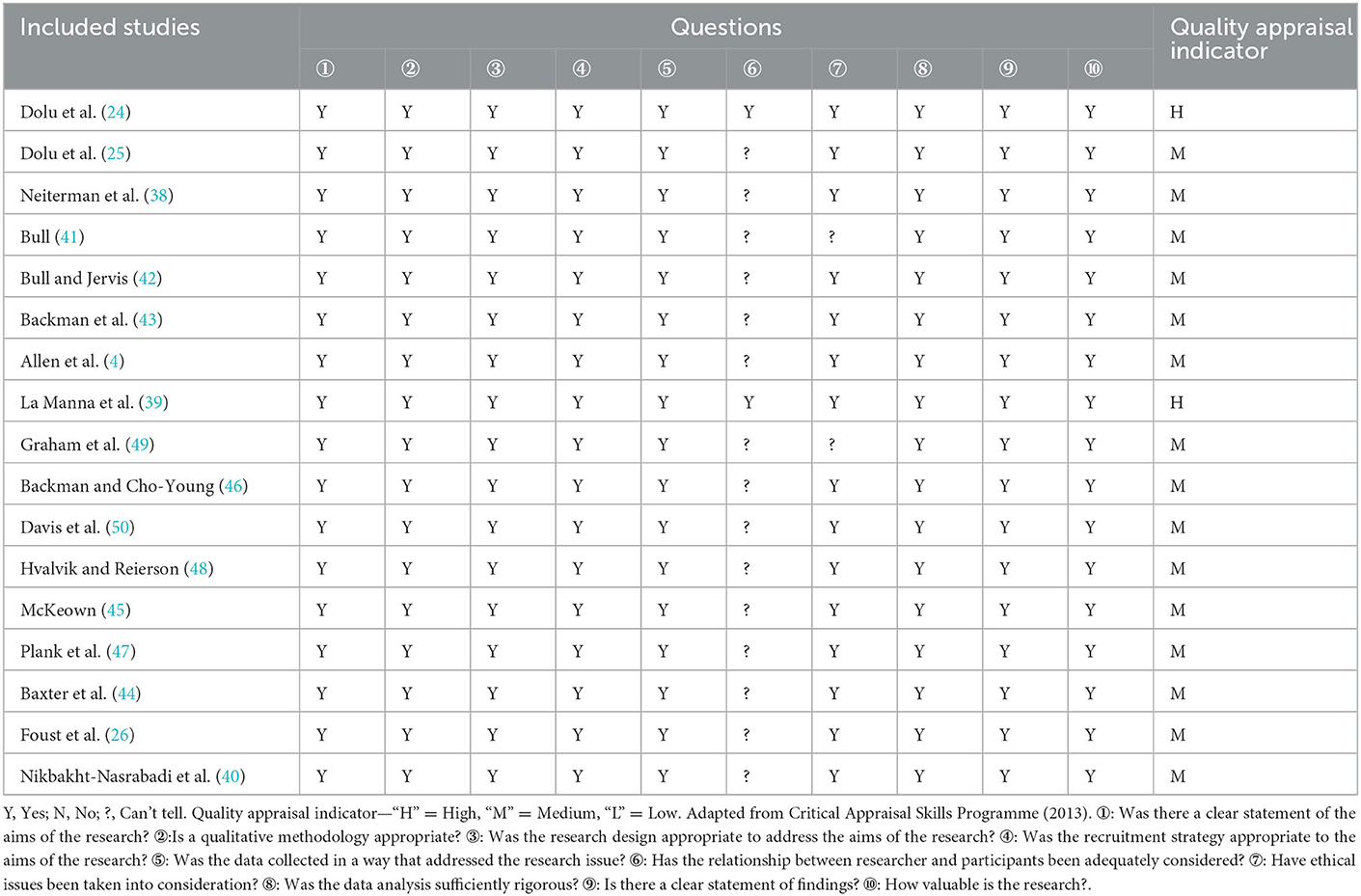
Table 1. Evaluation of methodological quality.
Data extraction and synthesis
The study data extracted were: author, publication year, country, design, setting and sampling, method(s) of data collection, data analysis strategy and aims. Study findings were extracted from the findings/results section of each paper. Thematic synthesis was conducted using a three-stage process (36). Stage 1: the coding of the selected studies text line-by-line. Stage 2: a review of the coding with grouping to generate descriptive themes and subthemes. We drew upon Meleis's Transition theory (37) for data a narrative synthesis, specifically, the domain “transition conditions” to classify potential facilitators and inhibitors as personal, community or societal. Stage 3: the generation of abstract themes or analytic themes.
Results
A total of 17 studies were included, with studies from a total of nine countries: the United States (n = 7), Turkey (n = 2), Canada (n = 2), Australia (n = 1), Tran (n = 1), Norway (n = 1), Italy (n = 1), the United Kingdom (n = 1), and Ireland (n = 1). Six of the studies had theoretical or conceptual frameworks involving active recovery models, social-ecological perspectives, transition theory, social-ecological models of health behavior, positive deviance frameworks, and constructivism. The sample of participants varied across studies. Eleven of the 17 studies included older adults, 12 studies investigated the perspectives of their caregivers, and 3 studies explored the perspectives of health care providers. Each study was systematically assessed for study purpose, study methodology, sample size, study setting, and country in which the study occurred (Table 2). The methodological quality of the included studies was variable, with 2 being rated as high and 15 as moderate. None of the studies were excluded due to study quality issues.

Table 2. Summary of included studies.
In this review, Personal and community focused facilitators and inhibitors were identified that mapped to there themes: (1) Resilience in older adults; (2) Interpersonal connections and relationships; (3) Uninterrupted transfer of care supply chain (Table 3). These facilitators and inhibitors existed at the health care provider level, at the patient and family level, and at the health system level.
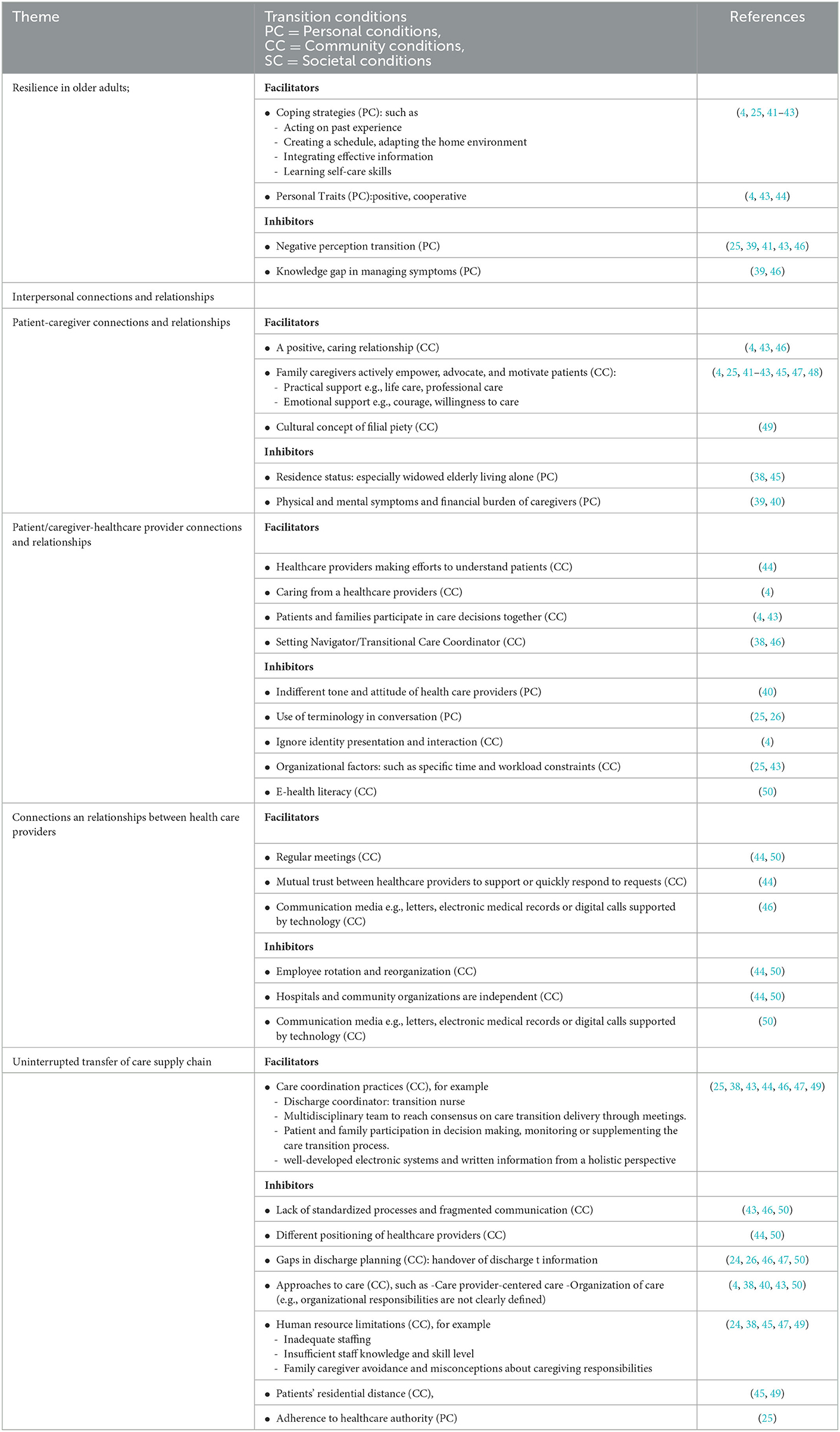
Table 3. Transition facilitators and inhibitors.
Resilience in older adults
Resilience in older adults refers to the ability of the elderly to accept the transition from hospital to home and to make sense of the benefits and losses associated with the transition. We identified several facilitators and barriers that were compatible with Meleis's personal and community transition conditions.
For older adults, the perceived benefits of going home include access to comfort, freedom (e.g., following one's own opinions in daily life without the constraints and supervision of organizations), safety (avoiding hospital-acquired infectious risks), and a sense of personal control (4, 25, 38). Care transitions can be a difficult and unsafe time for most participants (25, 38–40). Resilience as a force against adversity involves positive thinking, lifestyle changes and engagement in self-management to readjust within an unstructured family environment, become independent and re-establish new routines (4, 25, 41–43). Adapting to a new environment at home and achieving a safe transition seem to benefit from personal traits such as motivation, initiative, and cooperation (4, 43, 44). One contributing factor was the personal belief that older adults want to be independent, which motivated them to find a personal strategy and solution to the dilemma of care transition and dependency.
During the care transition, older adults had difficulties with self-management in daily living, professional care and follow-up care, such as dressing, eating, bathing and transportation, medications, wounds, follow-up visits (4, 24, 38, 39, 41, 42, 45). Potential facilitators of transition were reinvention strategies used by older adults to meet independence and personal care needs, such as self-motivation, acting on previous experiences, developing schedules, engaging in activities of daily living and co-learning, proactively seeking help from others, integrating valid information, and mastering self-care skills (e.g., complex medication management) (4, 25, 41–43).
Inhibiting factors were negative perceived transitions as discontinuity and powerlessness, loss (25, 39, 41, 43, 46), which were related to the patient's health status, roles and relationships, daily life and hobbies, and gaps in self-care knowledge. Fear of leaving the hospital exacerbates disease progression in older adults due to unresolved physical symptoms (25). Patients with delayed self-recovery feel depressed and frustrated (39). Older adults presented a strong care dependency during transition. Participants indicated that maintaining daily life and managing complex health issues after returning home was a challenge (4, 24, 38, 39, 41, 42, 45) and that daily management and hobbies required forced changes (38, 41, 45). Gaps in knowledge when dealing with physical changes and adverse reactions can leave participants will be in a difficult situation (38, 39, 46).
Interpersonal connections and relationships
Interpersonal relationships and connections among older adults concentrated among family caregivers (including spouses, children, neighbors, friends, etc.), and health care providers. We identified several facilitators and barriers that were compatible with Meleis's personal and community transition conditions.
Patient-caregiver connections and relationships: a positive and strong relationship with caregivers was an important factor for a smooth transition for older patients. Caregivers actively empowered, advocated, and motivated patients in care transitions (4, 41–43, 45, 47, 48), including closely monitoring older adults' health status; facilitating communication between older adults and health care providers; helping older adults improve their self-management; and focusing on the care delivery process to ensure a smooth transition. In addition, caregivers provided emotional support, such as hope, courage, and willingness to enter the caregiver role, so that patients felt dependent and confident as well as unabandoned (4, 43, 47). In some cultural settings, the value of filial piety became a double-edged sword and caregivers and patients had to live together. Cultural values and practices that do not allow elderly people to be sent to nursing homes constitute, at another level, a barrier to the use of formal care (49).
Caregivers experienced physical and emotional and financial stress when confronted with the complexity and number of chronic illnesses suffered by family members, combined with their own physical condition and work and patient cooperation, which may result in burnout and avoidance (39, 40). In addition, An important inhibiting factor was the patient's residential status (38, 45). Older adults who were widowed, especially those who live alone, were vulnerable to the loss of basic social relationships and connections, which not only exacerbated depression and isolation (45); they also tended to miss out on the symptom monitoring and care support provided by their families and put themselves at a disadvantage (38).
Interpersonal relationships and connections between older patients and families and healthcare providers was identified as potential facilitators and inhibitors of health transitions (4, 25, 38, 43, 44, 48). The nature of the relationship between older adults and health care providers was diverse and was described as collaborative and supportive (43), caring (4), trusting rapport (44), and skeptical (47, 48). Promoting meaningful patient/caregiver-provider relationships was a way for healthcare providers proactively spend more time with patients or families in an effort to understand the health status and care needs (44); to involve patients and families in healthcare decisions (4); to conduct regular follow-up visits (46); and, especially in cross-border situations, to establish intermediaries to navigate relationships, organize contacts to ensure patients know when problems arise whom to contact (38, 46).
Inhibiting factors were included: indifferent tone and attitude of medical provision (40); use of medical jargon in conversations; giving verbal information that may be forgotten and written information that is not readable (25, 26); neglected identity presentations and interactions (4); poor previous care and medical records (47); and organizational factors such as specific working hours and workload limitations (25, 43). A potential inhibiting factor lay in electronic communication devices (50). Older adults with limited e-health literacy had difficulty staying in communication with health professionals in digitally supported conversation and appointment systems and felt separated and alienated from their interpersonal relationships.
Establishing or maintaining valuable relationships among health care providers appeared to be important in facilitating the transition of older adults (44, 45). One barrier factor was the instability of relationships between healthcare providers, which was a matter of systems and organizational processes, such as regular staff rotation and reorganization, which meant that old familiar partnerships were broken up and had to be regrouped; the independence of hospitals and community health organizations from each other lacking feedback on patient transition status, channels for sharing and opportunities for cross-border learning, which reduced interpersonal interactions and contacts among healthcare providers and thus may not allow for timely tracking of patient transition status (44, 50). Communication media such as letters, electronic medical records, or digital calls supported by technology were considered potential facilitators or inhibitors that helped facilitate valuable contact between healthcare providers regarding patient follow-up care services (46) or relyed solely on electronic cases to convey information or discharge processes, neglecting interpersonal communication (50). Trust was a cornerstone of many relationships among healthcare teams and an important facilitator of maintaining connections. Mutual support or rapid response to requests among healthcare members across settings helps strengthen relationships and connections (44). Regular meetings brought members of teams together, and such multidisciplinary meetings provided opportunities for socialization and interaction, not only to maintain contact and relationships, but also to support patients through verbal communication (44, 50).
Uninterrupted transfer of care supply chain
The theme of uninterrupted transfer of care supply chain centered on care coordination, approaches to care, and workforce factors. Potential facilitators and inhibitors corresponded with Meleis's personal and community transition conditions.
Care coordination was a facilitator of hospital-home care delivery for patients (25, 38, 43, 44, 46, 47, 49). An important manifestation of care coordination was the discharge coordinator, who was the central point of contact between the hospital and the community agency or family physician or general practitioner, especially the transition nurse, who was familiar with the way the health system works and provided a liaison for care coordination across hospitals/communities (25, 38, 43, 44, 46, 49). Whereas, communication was considered an important means of care coordination, multidisciplinary teams share information seamlessly between different team members and/or specialists through formal or informal meetings, raised relevant issues, and set transition goals and priorities to reach consensus on care delivery to avoid inconsistency and loss of trust (47). Other facilitators included involving patients and families in discharge planning decisions and discussions, the ability of patients and families to add and share more nuanced information as they move across health care settings to help care providers better understand the situation and make decisions (25, 46), or monitoring the entire care delivery process so that information was not misplaced (46, 48). Potential facilitators included well-developed electronic systems and written information with a holistic perspective so that staff in care transition delivery act on established plans and relevant symptom management knowledge and information (24).
Factors impeding care coordination included: lack of standardized processes and fragmented communication (43, 46, 50) differences in the positioning of hospital and community care providers' roles and thus priorities and goals, and possible conflicting values and understandings that impede care coordination (44, 50); other inhibiting factors included: gaps in discharge planning, where patients and caregivers were often passive and hastily accepted discharge plans (26); arbitrary and incomplete handover of discharge information, e.g., care provides giving verbal information that may be forgotten, and primary care providers or family physicians do not receive or delay receiving or receive incorrect, unclear discharge information or letters (24, 26, 46, 47, 50).
Approaches to care had the potential to inhibit transition. This included: approaches to care that promoted resident care dependence rather than greater patient self-management (4); care provider-centered care that did not take into account patient preferences and uniqueness (40, 43); and care organization (e.g., organizational responsibilities were not clearly defined (50), multiple care providers emerged in a confusing manner after discharge, and patients did not know who to contact when problems arose (38).
A potential inhibiting factor was human resources. With inadequate staffing, patients felt abandoned and helpless by the organization as they were unable to receive accurate care and assistance from medical staff at the right time or when they needed it most (38, 45). The limited level of knowledge and skills in the hospital-to-home delivery process, e.g., home health care providers were powerless in the face of new medical equipment due to gaps in continuing education (24). And family caregivers' ambiguous answers to questions about symptoms, questioning their ability to provide home care, and thus avoiding responsibility for home care or the misperception that it should be borne entirely by the health care provider, were often associated with limited discharge planning (24, 47).
In addition, other inhibiting factors including the distance patients live (45, 49) and adherence to medical authority (25) also hindered care delivery. If older adults were afraid to question care delivery methods and questions or live far from hospitals, communities, or in rural areas where there was a lack of primary care organizations, the lack of continuous supply of care services may affect patient transition.
Discussions
The ideal outcome for older adults transitioning from hospital to home is a healthy transition in which the physical, psychological, and emotional needs of older adults with follow-up care services are met and independence is gradually achieved. Our systematic review identified factors that may facilitate or inhibit healthy transitions from hospital to home for older adults, with implications for the development of transitional care services. Facilitators and barriers were mapped to three themes with an individual and community focus: Resilience in older adults; Interpersonal connections and relationships; Uninterrupted transfer of care supply chain. These themes resonate with the broader international literature (30, 51–54) on the losses and gains of care transitions (51, 52), elements that reduce readmission rates for older patients with chronic conditions (30, 53), and competencies needed for transitional care providers (54), such as: education and promotion of self-management, maintenance of relationships and promotion of coordination, communication and health care provider training.
For the topic of resilience in older adults, person-centered transition facilitators included older adults' values, positive personal attributes, and personal coping strategies in the face of self-management barriers. Chronic illness is a problem-based endeavor in which participants, with limited medical resources, often act on previous experiences, struggle to seek help, and employ self-management strategies to deal with health issues. Older adults want to be as independent as possible and stay at home for as long as possible. Personal strategies driven by beliefs to cope with self-management barriers emerge to make a smooth transition possible. Previous research had also found that older adults were struggling to find ways to master new situations that were useful and not burdensome for others (55). However, in the actual transition, there is a gap between the self-management performed by older adults and the self-management imagined in the discharge instructions (56). The lack of knowledge and self-management skills led to uncertainty and anxiety in some participants. In addition, unresolved somatic symptoms, delayed recovery from self-care, difficulties in daily management and processing of information, and inadequate social support also had an impact on patients' psychological mood. These physically, psychologically, and socially diverse factors contribute to the uncertainty and powerlessness of patients' transitions. This is consistent with studies by Joo et al. (27) and Hardy et al. (57). MacLeod et al. (58) reported that resilience interventions currently designed for older adults are often not available per se, but seem to show life for resilience building by improving adaptive coping, changing complex emotional responses (e.g., anxiety, depression), and social support. Patients with chronic illness often need knowledge in order to objectively interpret the illness and cope effectively. In this context, patient education before discharge and intensive self-management training after discharge seem to facilitate patients' adaptation to the transition (30, 59, 60). Furthermore, in the theme of uninterrupted care supply transfer chain we mentioned the impediment of caregiver (family caregivers and medical caregivers) incompetence to care transition. Therefore, in addition to patients, formal and informal caregivers need to develop competencies to help patients with self-management education and training.
The two mindsets of older chronically ill patients regarding care transition gains and losses are intertwined and constantly dynamic. Participants can be seen to have gained some important developments in their care transitions, such as: regaining independence, sense of personal control, etc. However, unsurprisingly, some participants appeared to experience fewer gains, and their journeys contained more pronounced losses than others, reporting strong feelings of anxiety, depression, and becoming barriers to transition. Notably, although psychological problems such as anxiety and depression are common in patients after discharge, screening is not routinely performed at discharge. Common outcome indicators for most transitional care interventions remain objective indicators such as readmission rates and mortality (61), with limited attention to patient-related outcomes, such as complex emotional problems. A prospective study reported (62) that hospital-home transition, as a period when older adults are at high risk for depressive symptoms, screening for identification of depressive symptoms and assessment of coping skills at discharge may be a potentially preventive intervention. Esche et al. (52) showed that resilience, as a factor that must be considered when transitioning older adults from hospital home, requires early identification by nurses and help those patients with low resilience to succeed in the home environment. Thus, these facilitators and barriers have the potential to inform the development of resilience-specific interventions to promote the psychological, social, and physical wellbeing of older patients with chronic conditions during transitions of care. Furthermore, intervention development has to consider the potential contribution of conceptual models such as Meleis' transition theory, the active recovery model, and the social ecology of health promotion.
Connections and relationships between the elderly and their caregivers, healthcare providers, and healthcare workers play an important role in facilitating and inhibiting patient transition and engagement in care. Our study suggests that patient and family caregiver partnerships that fill supply gaps, navigate the health care system, and advocate on behalf of patients can improve the health wellbeing of older adults. Findings also highlight that contextual factors (e.g., cultural attributes, roles and responsibilities of family members, residential status, etc.) must be considered to support these important relationships. There is a link between interpersonal continuity and patient satisfaction with health care (63). The medical staff can act as a barrier or facilitator, depending on his communication skills and ability to involve patients in decision making. Our study showed that a cordial, trusting relationship with the provider was an important factor in facilitating transition and supporting patient involvement, which is consistent with a study by Stolee et al. (64), which reported similar characteristics of a beneficial patient-provider relationship, including trust and respect, and guided patient and family involvement in decision making related to treatment during the transition. Moreover, a study by Mitchell et al. found that cold, brief discourse was detrimental to the establishment and maintenance of the relationship. This is consistent with our study's findings. To facilitate communication and connection and improve relationships with healthcare professionals, information communicated verbally and in writing must be shared in language that is jargon-free and easily understood by service users and caregivers. Health care workers need biopsychosocial training including communication skills, the need to consider the risk of giving inadequate or marginalized elderly wellness, and the need to assess the ability and understanding of older adults to understand information to ensure that both parties are working at a uniform level and to correct inequalities in power between service users and providers, which is particularly important in the new person-centered care model promulgated by WHO and other health agencies (65, 66).
Our study also highlights the importance of maintaining relationships and connections among HCPs. Previous studies have shown that healthcare providers establish cross-border relationships that can overcome discontinuous letters and uncertainty at transition (67). Healthcare providers have also indicated that regular meeting interactions (formal or informal) provide opportunities and channels for knowledge sharing, information feedback, and interpersonal communication that not only help healthcare providers gain knowledge of each other's work environment and develop interpersonal relationships, but also build trust and mutual understanding of each other's roles of responsibility, thereby maintaining organizational stability and continuity of patient care treatment during hospital-to-home transitions and consistency of patient care during the hospital-to-home transition (68, 69). Participants perceived that healthcare professionals build trusting relationships that allow for rapid response to each other during care transitions. A previous study by Bryn et al. (70) demonstrated little effective tools to support trust among HCPs when collaborating across borders when in different locations and lacking shared electronic health records, and at the broader health care system level. Baxter et al. (44) suggested that supporting staff to build and maintain relationships should be prioritized from an organizational systems perspective, such as minimizing staff rotation or having the same values and beliefs among staff.
Transitions are uncertain and complex (37), and the transition of older adults from hospital to home is not a linear process, but one of cross-cultural challenges for two organizations with different values and priorities. Some participants indicated that the different positioning and nature of services between hospitals and community agencies influence Healthcare workers' perceptions, expectations, and priorities for care transitions (25, 44, 50). Healthcare professionals need to be familiar with each other's roles and functions and clearly position themselves to minimize professional, cultural, and organizational differences (71). In fact, care plans and instructions between providers still conflict with each other. Previously Naylor et al.'s (11) transitional care model utilized transitional care coaches to facilitate care coordination through the advanced practice nurse and Coleman et al.'s (60) transitional care intervention model. Participants (25, 38, 43, 44, 46, 49) also reported that roles in the nursing process can facilitate care transitions and ensure an uninterrupted supply chain of care delivery. The importance of nurses as core healthcare practitioners and facilitators of transitional care continues to emerge. This is due to the professional status of nurses and their close interaction with patients, their familiarity with the way health systems work, and their leadership in collaboration. In the past few years, several Meta-analyses have shown that nurse-led transitional care, which respects patients' independence and decision-making power in care, is effective in increasing satisfaction, improving health status, reducing readmission rates, and is cost-effective and economically efficient (72, 73). Despite these developments, the inclusion of 17 studies in our review, only 3 of which investigated the views of medical caregivers, and no qualitative studies of transition nurses have been included, is a weakness of the existing literature. This supports our call for all stakeholders to be involved. Future research could therefore explore how nurses face barriers and experiences in collaborating across organizations.
Limitation
A systematic review of multiple perspectives of older patients, caregivers, and health professionals using Meleis' transition theory constructed our conceptualization of situational transitions and helped us classify facilitative and barrier factors with the help of the transition condition domain. However, we only included studies published in English in our review, so we may have missed relevant studies from non-English speaking countries, a potential language bias; there was a little theoretical framework in the studies and the timeline of the transition process varied, with some studies collected from the day patients were discharged and some 1 month or more after, and the heterogeneity of patient experiences and feelings limits the generalizability of the study to some extent. Finally, as this was a secondary analysis, we were unable to confirm our themes and consequences with the study participants.
Implications for practice
Identify individual and community-focused facilitators and inhibitors to inform the development of interventions to promote healthy transitions in older adults.
• Assess the psychological status of older adults at discharge in addition to the physical status of the patient.
• Healthcare staff need to improve capacity in addition to enhancing patient and family education.
• Build trusting relationships between health care providers, professionals, and older adults and their caregivers.
• Further explore the perceptions of health care workers, especially transition nurses, regarding transitions of care in order to improve transition care at the organizational system level.
Conclusions
This study identified potential transition facilitators and inhibitors for incoming older adults transitioning from hospital to home, and these findings may inform the development of interventions to target key areas of resilience in adapting to a new home environment, and human relations and connections for building partnerships, as well as an uninterrupted supply chain of care transfer at hospital-home delivery.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
MS and JW were responsible for the conception, design of the review, literature search and screening, analysis and interpretation of data, and drafted the manuscript. LL contributed to the data acquisition and interpretation and revised the paper. MZ, TX, and YQ contributed to data analysis and interpretation. RD contributed to the design of the review and revised of the manuscript. All authors approved the final version of the manuscript for submission and the type of the magazine.
Funding
This report was independent research funded by the 2021 Henan Province Science and Technology Research Project, 212102310665; 2020 Training Program for Young Backbone Teachers of Higher Colleges in Henan Province, 2020GGJS001; and 2019 Training Program for Young Backbone Teachers of Zhengzhou University, 2019ZDGGJS012.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1047723/full#supplementary-material
References
1. The Lancet GBD. 2017: a fragile world. Lancet. (2018) 392:1683. doi: 10.1016/S0140-6736(18)32858-7
2. Islam MM, Valderas JM, Yen L, Dawda P, Jowsey T, McRae IS. Multimorbidity and comorbidity of chronic diseases among the senior Australians: prevalence and patterns. PLoS ONE. (2014) 9:e83783. doi: 10.1371/journal.pone.0083783
3. Yarnall AJ, Sayer AA, Clegg A, Rockwood K, Parker S, Hindle JV. New horizons in multimorbidity in older adults. Age Ageing. (2017) 46:882–8. doi: 10.1093/ageing/afx150
4. Allen J, Hutchinson AM, Brown R, Livingston PM. User experience and care for older people transitioning from hospital to home: patients' and carers' perspectives. Health Expect. (2018) 21:518–27. doi: 10.1111/hex.12646
5. Coleman EA, Boult C. Improving the quality of transitional care for persons with complex care needs. J Am Geriatr Soc. (2003) 51:556–7. doi: 10.1046/j.1532-5415.2003.51186.x
6. Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. (2003) 138:161–7. doi: 10.7326/0003-4819-138-3-200302040-00007
7. Tsilimingras D, Schnipper J, Duke A, Agens J, Quintero S, Bellamy G, et al. Post-discharge adverse events among urban and rural patients of an urban community hospital: a prospective cohort study. J Gen Intern Med. (2015) 30:1164–71. doi: 10.1007/s11606-015-3260-3
8. Forster AJ, Clark HD, Menard A, Dupuis N, Chernish R, Chandok N, et al. Adverse events among medical patients after discharge from hospital. CMAJ. (2004) 170:345–9. doi: 10.1053/cmaj.1040215
9. Poldervaart JM, van Melle MA, Reijnders LJ, de Wit NJ, Zwart DL. Transitional safety incidents as reported by patients and healthcare professionals in the Netherlands: a descriptive study. Eur J Gen Pract. (2019) 25:77–84. doi: 10.1080/13814788.2018.1543396
10. Waring J, Bishop S, Marshall F. A qualitative study of professional and carer perceptions of the threats to safe hospital discharge for stroke and hip fracture patients in the English National Health Service. BMC Health Serv Res. (2016) 16:297. doi: 10.1186/s12913-016-1568-2
11. Naylor MD. Advancing high value transitional care: the central role of nursing and its leadership. Nurs Adm Q. (2012) 36:115–26. doi: 10.1097/NAQ.0b013e31824a040b
12. Brunner-La Rocca HP, Peden CJ, Soong J, Holman PA, Bogdanovskaya M, Barclay L. Reasons for readmission after hospital discharge in patients with chronic diseases-information from an international dataset. PLoS ONE. (2020) 15:e0233457. doi: 10.1371/journal.pone.0233457
13. WHO. Transitions of Care: Technical Series on Safer Primary Care. (2016). Available online at: https://apps.who.int/iris/handle/10665/252272 (accessed January 10, 2022).
14. NHS Digital UK. Hospital Admitted Patient Care Activity, 2015–16. Government Statistical Service (2016). Available online at: https://digital.nhs.uk/data-and-information/publications/statistical/hospital-admitted-patient-care-activity/2015-16 (accessed January 10, 2022).
15. Meleis AI, Sawyer LM, Im EO, Hilfinger Messias DK, Schumacher K. Experiencing transitions: an emerging middle-range theory. ANS Adv Nurs Sci. (2000) 23:12–28. doi: 10.1097/00012272-200009000-00006
16. Schumacher KL, Meleis AI. Transitions: a central concept in nursing. Image J Nurs Sch. (1994) 26:119–27. doi: 10.1111/j.1547-5069.1994.tb00929.x
17. Naylor M, Keating SA. Transitional care. J Soc Work Educ. (2008) 44:65–73. doi: 10.5175/JSWE.2008.773247714
18. Lee JY, Yang YS, Cho E. Transitional care from hospital to home for frail older adults: a systematic review and meta-analysis. Geriatr Nurs. (2022) 43:64–76. doi: 10.1016/j.gerinurse.2021.11.003
19. O'Donnell R, Savaglio M, Skouteris H, Banaszak-Holl J, Moranl C, Morris H, et al. The effectiveness of transition interventions to support older patients from hospital to home: a systematic scoping review. J Appl Gerontol. (2021) 40:1628–36. doi: 10.1177/0733464820968712
20. Fønss Rasmussen L, Grode LB, Lange J, Barat I, Gregersen M. Impact of transitional care interventions on hospital readmissions in older medical patients: a systematic review. BMJ Open. (2021) 11:e040057. doi: 10.1136/bmjopen-2020-040057
21. Zou D, Wang L, Li J, Li L, Wei X, Huang L. The benefits of transitional care in older patients with chronic diseases: a systematic review and meta-analysis. Aging Clin Exp Res. (2021). doi: 10.1007/s40520-021-01973-1
22. Bauer M, Fitzgerald L, Haesler E, Manfrin M. Hospital discharge planning for frail older people and their family. Are we delivering best practice? a review of the evidence. J Clin Nurs. (2009) 18:2539–46. doi: 10.1111/j.1365-2702.2008.02685.x
23. Hestevik CH, Molin M, Debesay J, Bergland A, Bye A. Older persons' experiences of adapting to daily life at home after hospital discharge: a qualitative metasummary. BMC Health Serv Res. (2019) 19:224. doi: 10.1186/s12913-019-4035-z
24. Dolu I, Naharci M, Logan PA, Paal P, Vaismoradi M. Transitional 'hospital to home' care of older patients: healthcare professionals' perspectives. Scand J Caring Sci. (2021) 35:871–80. doi: 10.1111/scs.12904
25. Dolu I, Naharci M, Logan PA, Paal P, Vaismoradi M. A qualitative study of older patients' and family caregivers' perspectives of transitional care from hospital to home. Res Theory Nurs Pract. (2021) 35:168–88. doi: 10.1891/RTNP-D-20-00067
26. Foust JB, Vuckovic N, Henriquez E. Hospital to home health care transition: patient, caregiver, and clinician perspectives. West J Nurs Res. (2012) 34:194–212. doi: 10.1177/0193945911400448
27. Joo JY, Liu MF. The experience of chronic illness transitional care: a qualitative systematic review. Clin Nurs Res. (2022) 31:163–73. doi: 10.1177/10547738211056166
28. Høy B, Ludvigsen MS. Older adults' experiences of patient involvement in transitional care: a qualitative systematic review protocol. JBI Database System Rev Implement Rep. (2018) 16:860–6. doi: 10.11124/JBISRIR-2017-003440
29. Chen LD, Xiao LD, Chamberlain D, Newman P. Enablers and barriers in hospital-to-home transitional care for stroke survivors and caregivers: a systematic review. J Clin Nurs. (2021) 30:2786–807. doi: 10.1111/jocn.15807
30. Morkisch N, Upegui-Arango LD, Cardona MI, van den Heuvel D, Rimmele M, Sieber CC, et al. Components of the transitional care model (TCM) to reduce readmission in geriatric patients: a systematic review. BMC Geriatr. (2020) 20:345. doi: 10.1186/s12877-020-01747-w
31. Institute of Medicine (US) Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academies Press (2001).
32. Lima M, Magalhães AMM, Oelke ND, Marques GQ, Lorenzini E, Weber LAF, et al. Care transition strategies in Latin American countries: an integrative review. Rev Gaucha Enferm. (2018) 39:e20180119. doi: 10.1590/1983-1447.2018.20180119
33. Camicia M, Lutz BJ. Nursing's role in successful transitions across settings. Stroke. (2016) 47:e246–9. doi: 10.1161/STROKEAHA.116.012095
34. Booth A. Clear and present questions: formulating questions for evidence based practice. Library Hi Tech. (2006) 24:355–68. doi: 10.1108/07378830610692127
35. Critical Appraisal Skills Programme. CASP Qualitative Checklist.(2018). Available online at: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Qualitative-Checklist-2018.pdf (accessed January 10, 2022).
36. Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. (2008) 8:45. doi: 10.1186/1471-2288-8-45
37. Meleis AI. Transitions Theory Middle-Range and Situation-Specific Theories in Nursing Research and Practice. New York, NY: Springer Publishing Company (2010).
38. Neiterman E, Wodchis WP, Bourgeault IL. Experiences of older adults in transition from hospital to community. Can J Aging. (2015) 34:90–9. doi: 10.1017/S0714980814000518
39. La Manna JB, Bushy A, Gammonley D. Post-hospitalization experiences of older adults diagnosed with diabetes: “it was daunting!”. Geriatric Nurs. (2018) 39:103–11. doi: 10.1016/j.gerinurse.2017.07.005
40. Nikbakht-Nasrabadi A, Mardanian-Dehkordi L, Taleghani F. Abandonment at the transition from hospital to home: family caregivers' experiences. Ethiop J Health Sci. (2021) 31:525–32. doi: 10.4314/ejhs.v31i3.9
41. Bull MJ. Managing the transition from hospital to home. Qual Health Res. (1992) 2:27–41. doi: 10.1177/104973239200200103
42. Bull MJ, Jervis LL. Strategies used by chronically ill older women and their caregiving daughters in managing posthospital care. J Adv Nurs. (1997) 25:541–7. doi: 10.1046/j.1365-2648.1997.1997025541.x
43. Backman C, Stacey D, Crick M, Cho-Young D, Marck PB. Use of participatory visual narrative methods to explore older adults' experiences of managing multiple chronic conditions during care transitions. BMC Health Serv Res. (2018) 18:482. doi: 10.1186/s12913-018-3292-6
44. Baxter R, Shannon R, Murray J, O'Hara JK, Sheard L, Cracknell A, et al. Delivering exceptionally safe transitions of care to older people: a qualitative study of multidisciplinary staff perspectives. BMC Health Serv Res. (2020) 20:780. doi: 10.1186/s12913-020-05641-4
45. McKeown F. The experiences of older people on discharge from hospital following assessment by the public health nurse. J Clin Nurs. (2007) 16:469–76. doi: 10.1111/j.1365-2702.2006.01556.x
46. Backman C, Cho-Young D. Engaging patients and informal caregivers to improve safety and facilitate person- and family-centered care during transitions from hospital to home - a qualitative descriptive study. Patient Prefer Adherence. (2019) 13:617–26. doi: 10.2147/PPA.S201054
47. Plank A, Mazzoni V, Cavada L. Becoming a caregiver: new family carers' experience during the transition from hospital to home. J Clin Nurs. (2012) 21:2072–82. doi: 10.1111/j.1365-2702.2011.04025.x
48. Hvalvik S, Reierson I. Striving to maintain a dignified life for the patient in transition: next of kin's experiences during the transition process of an older person in transition from hospital to home. Int J Qual Stud Health Well-being. (2015) 10:26554. doi: 10.3402/qhw.v10.26554
49. Graham CL, Ivey SL, Neuhauser L. From hospital to home: assessing the transitional care needs of vulnerable seniors. Gerontologist. (2009) 49:23–33. doi: 10.1093/geront/gnp005
50. Davis MM, Devoe M, Kansagara D, Nicolaidis C, Englander H. Did I do as best as the system would let me? Healthcare professional views on hospital to home care transitions. J Gen Intern Med. (2012) 27:1649–56. doi: 10.1007/s11606-012-2169-3
51. Walker R, Johns J, Halliday D. How older people cope with frailty within the context of transition care in Australia: implications for improving service delivery. Health Soc Care Commun. (2015) 23:216–24. doi: 10.1111/hsc.12142
52. Esche CA, Tanner EK. Resiliency: a factor to consider when facilitating the transition from hospital to home in older adults. Geriatric Nurs. (2005) 26:218–22. doi: 10.1016/j.gerinurse.2005.05.007
53. Leithaus M, Beaulen A, de Vries E, Goderis G, Flamaing J, Verbeek H, et al. Integrated care components in transitional care models from hospital to home for frail older adults: a systematic review. Int J Integr Care. (2022) 22:28. doi: 10.5334/ijic.6447
54. Agomoh CJ, Brisbois MD, Chin E. A mapping review of clinical nurse leader and nurse educator transitional care skills and competencies. Nurs Outlook. (2020) 68:504–16. doi: 10.1016/j.outlook.2020.02.003
55. Ebrahimi Z, Wilhelmson K, Moore CD, Jakobsson A. Frail elders' experiences with and perceptions of health. Qual Health Res. (2012) 22:1513–23. doi: 10.1177/1049732312457246
56. Werner NE, Tong M, Borkenhagen A, Holden RJ. Performance-shaping factors affecting older adults' hospital-to-home transition success: a systems approach. Gerontologist. (2019) 59:303–14. doi: 10.1093/geront/gnx199
57. Hardy MS, Dallaire C. [Using lived experiences and theoretical insights to gain a better understanding of the adaptation difficulties encountered by elderly patients with chronic heart failure during the hospital-to-home transition]. Rech Soins Infirm. (2020) 38–48. doi: 10.3917/rsi.141.0038
58. MacLeod S, Musich S, Hawkins K, Alsgaard K, Wicker ER. The impact of resilience among older adults. Geriatr Nurs. (2016) 37:266–72. doi: 10.1016/j.gerinurse.2016.02.014
59. Aboumatar H, Naqibuddin M, Chung S, Chaudhry H, Kim SW, Saunders J, et al. Effect of a hospital-initiated program combining transitional care and long-term self-management support on outcomes of patients hospitalized with chronic obstructive pulmonary disease: a randomized clinical trial. JAMA. (2019) 322:1371–80. doi: 10.1001/jama.2019.11982
60. Coleman EA, Smith JD, Frank JC, Min SJ, Parry C, Kramer AM. Preparing patients and caregivers to participate in care delivered across settings: the care transitions intervention. J Am Geriatr Soc. (2004) 52:1817–25. doi: 10.1111/j.1532-5415.2004.52504.x
61. Markle-Reid M, McAiney C, Ganann R, Fisher K, Gafni A, Gauthier AP, et al. Study protocol for a hospital-to-home transitional care intervention for older adults with multiple chronic conditions and depressive symptoms: a pragmatic effectiveness-implementation trial. BMC Geriatr. (2020) 20:240. doi: 10.1186/s12877-020-01638-0
62. Brown A, Peres L, Brown T, Haines T, Stolwyk R. A prospective investigation of factors associated with depressive symptoms in older adults' post-hospitalisation. Int J Geriatr Psychiatry. (2020) 35:671–82. doi: 10.1002/gps.5285
63. Saultz JW, Albedaiwi W. Interpersonal continuity of care and patient satisfaction: a critical review. Ann Fam Med. (2004) 2:445–51. doi: 10.1370/afm.91
64. Stolee P, Elliott J, Byrne K, Sims-Gould J, Tong C, Chesworth B, et al. A framework for supporting post-acute care transitions of older patients with hip fracture. J Am Med Dir Assoc. (2019) 20:414–9.e1. doi: 10.1016/j.jamda.2019.01.147
65. World Health Organization. Regional Office for the Western P. People-Centred Health care: Technical Papers: International Symposium on People-Centred Health Care: Reorienting Health Systems in the 21st Century, The Tokyo International Forum, 25 November 2007. Manila: WHO Regional Office for the Western Pacific (2008).
66. Kim MY, Oh S. Nurses' perspectives on health education and health literacy of older patients. Int J Environ Res Public Health. (2020) 17:6455. doi: 10.3390/ijerph17186455
67. Sims-Gould J, Byrne K, Hicks E, Khan K, Stolee P. Examining “success” in post-hip fracture care transitions: a strengths-based approach. J Interprof Care. (2012) 26:205–11. doi: 10.3109/13561820.2011.645090
68. Eika M, Hvalvik S. Municipal healthcare professionals' interprofessional collaboration during older patients' transitions in the municipal health and care services: a qualitative study. BMC Health Serv Res. (2022) 22:918. doi: 10.1186/s12913-022-08226-5
69. Baillie L, Gallini A, Corser R, Elworthy G, Scotcher A, Barrand A. Care transitions for frail, older people from acute hospital wards within an integrated healthcare system in England: a qualitative case study. Int J Integr Care. (2014) 14:e009. doi: 10.5334/ijic.1175
70. Sutherland B, Pecanac K, LaBorde T, Bartels C, Brennan M. Good working relationships: how healthcare system proximity influences trust between healthcare workers. J Interprof Care. (2021) 36:1–9. doi: 10.1080/13561820.2021.1920897
71. Heskestad RN, Aase K. The meeting point: organising for knowledge transfer. In:Aase K, Waring J, Schibevaag L, , editors. Researching Quality in Care Transitions: International Perspectives. Cham: Springer International Publishing (2017). p. 239–57. doi: 10.1007/978-3-319-62346-7_13
72. Bryant-Lukosius D, Carter N, Reid K, Donald F, Martin-Misener R, Kilpatrick K, et al. The clinical effectiveness and cost-effectiveness of clinical nurse specialist-led hospital to home transitional care: a systematic review. J Eval Clin Pract. (2015) 21:763–81. doi: 10.1111/jep.12401
Keywords: older patients, chronic diseases, transitional care, discharge, qualitative research
Citation: Sun M, Liu L, Wang J, Zhuansun M, Xu T, Qian Y and Dela Rosa R (2023) Facilitators and inhibitors in hospital-to-home transitional care for elderly patients with chronic diseases: A meta-synthesis of qualitative studies. Front. Public Health 11:1047723. doi: 10.3389/fpubh.2023.1047723
Received: 18 September 2022; Accepted: 26 January 2023;
Published: 13 February 2023.
Edited by:
Waqas Sami, Azra Naheed Medical College, PakistanReviewed by:
Wanich Suksatan, Chulabhorn Royal Academy, ThailandSimin Jahani, Ahvaz Jundishapur University of Medical Sciences, Iran
Copyright © 2023 Sun, Liu, Wang, Zhuansun, Xu, Qian and Dela Rosa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lamei Liu,  liulamei2005@126.com
liulamei2005@126.com