 Keeva Duffey1*
Keeva Duffey1* Ana Barbosa1,2
Ana Barbosa1,2 Stephen Whiting1,2
Stephen Whiting1,2 Romeu Mendes1,2
Romeu Mendes1,2 Isabel Yordi Aguirre1
Isabel Yordi Aguirre1 Antonina Tcymbal3
Antonina Tcymbal3 Karim Abu-Omar3
Karim Abu-Omar3 Peter Gelius3João Breda1
Peter Gelius3João Breda1- 1World Health Organization, Regional Office for Europe, Copenhagen, Denmark
- 2Epidemiology Research Unit–Instituto de Saúde Pública, Universidade do Porto, Porto, Portugal
- 3Department of Sport Science and Sport, Friedrich–Alexander University Erlangen–Nürnberg, Erlangen, Germany
Background: Persistent low physical activity (PA) levels among adolescent girls constitute a public health concern that calls for immediate and evidence-based policy action. This systematic review (SR) aimed to summarize evidence from SRs examining the barriers and facilitators of PA participation in adolescent girls. The objectives were to provide a synthesis of the available evidence and identify key areas for fostering gender-responsive action and policy implications.
Methods: A comprehensive search of relevant SR and meta-analyses were performed in PubMed and Cochrane Library, until February 2021. Studies were included if they were SRs or meta-analyses, included adolescent girls aged between 10 and 19 years, and described barriers or facilitators of PA. Two independent authors performed the screening of potentially eligible studies and both assessed the methodological quality of included studies using the AMSTAR 2 tool. The barriers and facilitators were synthesized at environmental, interpersonal, and individual levels.
Results: A total of eight SRs were included in the qualitative synthesis. The most frequent barriers identified were the lack of support from peers, family, and teachers, and the lack of time. The most reported facilitators were weight loss, and support from peers, family, and teachers. Key areas for action and policy implementation include an inclusive approach to curriculum development to address gender norms; adequate training of professionals so they have a range of skills to ensure inclusion of adolescent girls; environmental changes in and out of schools to stimulate participation, to allow adolescent girls to be active in a safe and attractive environment; multistakeholder support at local, regional, and national level in incorporating a gender-responsive approach toward PA participation.
Conclusion: The results highlight a variety of factors that influences the PA participation of adolescent girls. For the attainment of effective policies that increase PA levels in adolescent girls, it is essential to engage several stakeholders at different levels in incorporating a gender-responsive approach toward PA participation.
Systematic Review Registration: PROSPERO, identifier: CRD42020204023.
Introduction
Regular physical activity (PA) has well-known positive effects on the prevention and control of non-communicable diseases, such as cardiovascular diseases, cancer, diabetes, and depression (1–4), as well as reduced overall mortality and risk of premature death (5). In children and adolescents, adequate PA also provides benefits to cognitive development, motor skills, self-esteem, social integration (6), musculoskeletal health (7) academic achievement (8), and overall well-being (9).
The World Health Organization (WHO) recommends that children and adolescents aged 5–17 years engage in at least an average of 60 min per day of moderate to vigorous-intensity, mostly aerobic, PA across the week (10). According to a recent study on school-attending adolescents, 81.0% of adolescents aged 11–17 years are insufficiently active (not meeting current daily PA recommendations) (11). The 2020 study by Guthold et al. revealed that a higher prevalence of physical inactivity was found amongst girls in almost all countries globally (84.7%, compared with a prevalence of 77.6% for boys), with no significant changes for girls in these trends over the past decade (11).
Persistent low PA levels among adolescent girls constitute a public health concern that calls for immediate and evidence-based policy action. Increasing PA participation among adolescent girls is an important component not just because of the positive effects on health, but also because PA can play a role in economic development, education, peace-building, and trauma relief in different geographical, cultural, and political contexts (12, 13). Promoting PA contributes directly to attain many of the 2030 Sustainable Development Goals (SDG), by promoting policy actions that foster peace, tolerance, respect, and the empowerment of women (14).
Several reviews have investigated the factors that influence PA behavior in adolescent girls and highlighted complex influential factors. For example, a review of the effectiveness of school-based PA interventions on adolescent girls discovered only a small effect of these interventions, namely multicomponent interventions, on increasing PA levels due to complex social and cultural norms that play in the structures of school PA programs rendering limited flexibility in accommodating for gender differences (15). Furthermore, a review of qualitative studies on the self-perception of PA of adolescent girls identified perceived gender bias in sports, along with a limited level of competence in abilities, preference in other priorities, and differing social expectations as impediments for PA participation among adolescent girls (16). Despite the sizable evidence providing insights on the influences of PA behavior for this group, challenges continue to exist in implementing gender-responsive PA interventions (17) leaving girls enduring inequalities in access to and experiences with PA (18).
Limited research has been able to explain how policymakers and implementers can effectively cater toward adolescent girls' needs when it comes to increasing PA levels (11, 16, 19). Common theories used to explain the factors that affect the PA of adolescent girls have used the socioecological model (18, 20, 21). Bronfenbrenner's ecological model of human development describes factors that influence behavior to be linked to individual, interpersonal, and environmental levels (22). Nonetheless, previous studies lack on how to translate these factors into practice in terms of a gender-responsive approach to PA promotion in adolescent girls.
A more gender-responsive approach to PA promotion has been recommended in important policies and strategies. The United Nations and WHO have called on the Member States to act to increase gender equity in PA and sport participation. For example, Article 10 of the Convention on the Elimination of All Forms of Discrimination against Women calls on countries to ensure women have equal opportunities for participation in sport and PA (23), also contributing to achieving the SDG number five, gender equality (24). The WHO, through the Global Action Plan on Physical Activity 2018–2030 (12), also reinforces and supports gender equality and the empowerment of girls to uphold this fundamental human right, and a necessary foundation for a peaceful, prosperous, and sustainable world (24). Accordingly, actions are necessary to tackle inequalities in PA, as reflected by the Physical Activity Strategy for the WHO European Region 2016–2025 (25), by improving the availability, affordability, and acceptability of PA in some age groups. In particular, early adolescence may be an opportune transitional period to promote the development of healthy behavior and equitable gender norms early in life that can be transformative both immediately and over the life course (26, 27).
The gender disparity of PA in adolescents calls for increased efforts at the global, national, and regional levels to reduce inequalities in opportunities for PAs of adolescent girls. Providing a synthesis of the most recent evidence may assist in the development of gender-responsive recommendations, strategies, initiatives, and policies for implementers. Therefore, this systematic review (SR) of systematic reviews (SRs) aims to (i) summarize evidence from SRs examining the barriers and facilitators of PA participation in adolescent girls and (ii) identify key areas for action and policy implementation.
Methods
An adapted Preferred reporting item for systematic reviews and meta-analysis (PRISMA) reporting method was used to conduct this SRof SRs (28). The PRISMA checklist is available in Supplementary Material 1. The protocol for this review is registered in PROSPERO (reference number CRD42020204023).
Eligibility Criteria
The study eligibility criteria consisted of the type of studies (SRs and/or meta-analysis); type of participants [adolescent girls 10–19 years of age (according to WHO), or in this age range]; type of interventions (any form of PA practice); and type of outcome (barriers and/or facilitators. Studies were excluded according to study type (editorials, comments, case reports, guidelines, conference abstracts, other reviews); studies without measurement of the outcomes of interest, i.e., studies without barriers or facilitators; studies that aim to find correlations between PA and other factors; studies that aim to analyze the effectiveness of PA interventions; populations with specific conditions (e.g., pregnancy); and studies that do not provide separate data for sex or age category.
Information Sources
A comprehensive search for relevant SRs was conducted independently by the first and second author until February 2021 using two electronic databases: PubMed and Cochrane Library.
Search Strategy
The key search terms used in each database were as follows: (“physical activity” OR exercise OR sport* OR “physical education”) AND (child* OR adolescent* OR teen* OR youth OR young) AND (female OR girl* OR women) AND (“gender gap” OR “gender differences” OR factor* OR motive* OR barrier* OR facilitator* OR perception* OR support). We limited the search to study type (SRs, meta-analysis, and reviews) and the English language. The complete search strategy for each database can be consulted in Supplementary Material 2.
Selection Process
The search results were retrieved and screened from databases by two independent authors according to predefined steps. First, articles were screened by the information from the title and abstract. Second, potentially relevant articles were retrieved for full-text review and their eligibility for the study was determined. Disagreements were resolved through discussion until consensus.
Data Collection Process
Each selected SR was independently evaluated by the two authors to extract information regarding study design, participants, number and type of included studies, outcome measures, the setting of intervention, and barriers and facilitators. If there were discrepancies in data extraction, authors discussed until consensus.
Data Items
Barriers and facilitators were identified and then synthesized in three main levels (individual, interpersonal, and environment) from Bronfenbrenner's ecological model of human development (22). The individual level refers to perceptions and attitudes of the individual; the interpersonal level refers to the relations with factors that have direct contact with the individual in their immediate environment, such as parents, siblings, teachers, and school peers; and the environment level incorporates formal and informal social structures, and cultural norms, which do not themselves contain the individual, but indirectly influence them.
Methodological Quality
Each eligible SR was evaluated regarding its methodological quality by two independent authors, using the 16-item AMSTAR 2 tool (29). Each study was classified according to critical domains that can affect the validity and conclusion of the review. The critical domains considered for this review were: protocol registered before the commencement of the review (item 2); adequacy of the literature search (item 4); justification for excluding individual studies (item 7); risk of bias from individual studies being included in the review (item 9); appropriateness of meta-analytical methods (item 11); consideration of the risk of bias when interpreting the results of the review (item 13); and assessment of the presence and likely impact of publication bias (item 15). The studies were rated as “high-quality” if there were none or there was one non-critical weakness; “moderate-quality” if more than one non-critical weakness; “low-quality” if one critical flaw with or without non-critical weaknesses; and “critically low-quality” if more than one critical flaw with or without non-critical weaknesses. Any disagreements in the classification were resolved by discussion.
Results
Study Selection
Out of the 641 references identified in the initial search in electronic databases, the study selection process resulted in the inclusion of a total of eight studies in the qualitative synthesis (Figure 1).
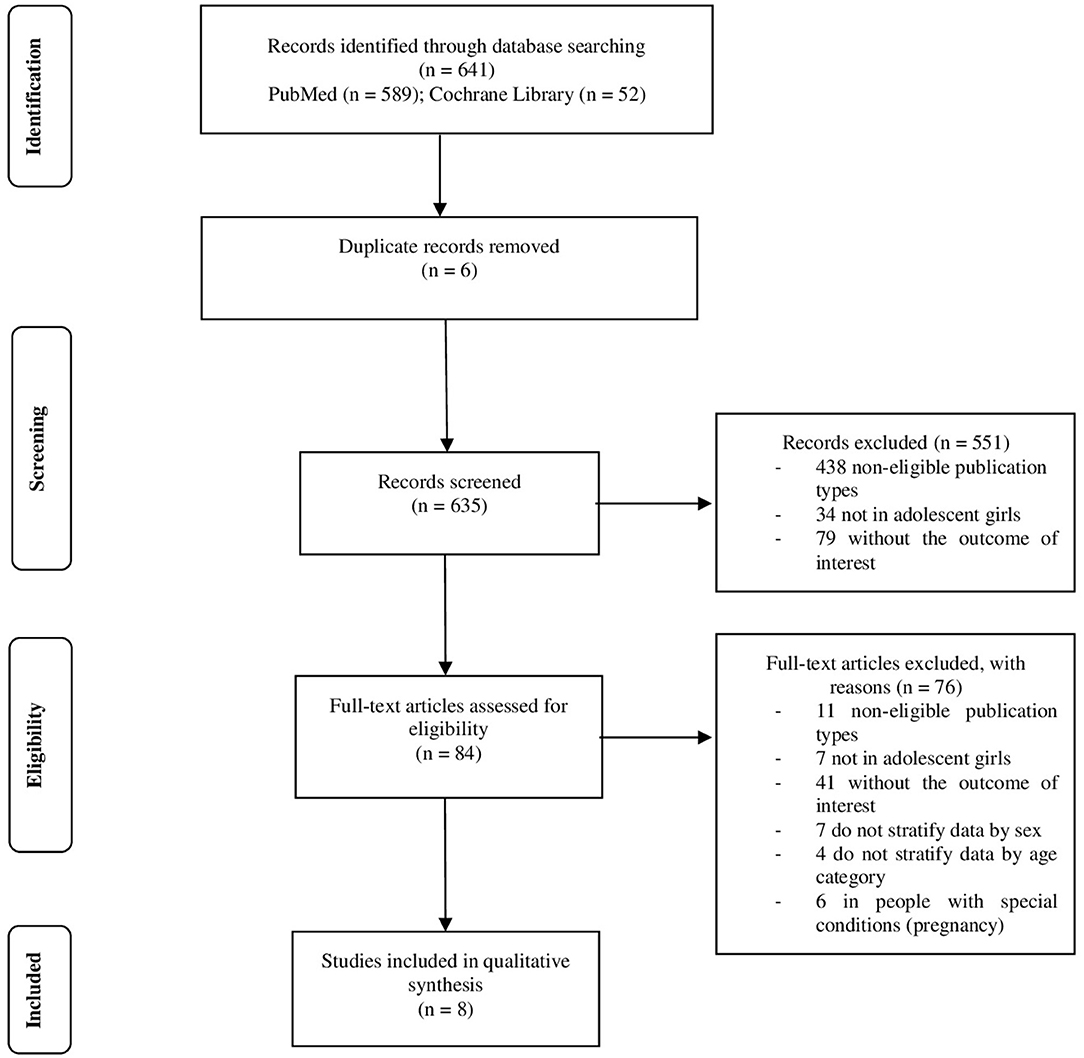
Figure 1. Flow diagram of included studies.
Study Characteristics
The study characteristics included in this review are shown in Table 1. All studies were SRs, ranging from 2006 to 2019, and published in the English language. Concerning the study design of the original studies, the majority provided qualitative designs (16, 31, 33, 35, 36). Regarding the participants, the studies included children and adolescents (30, 31, 34) or adolescents only (16, 32, 33, 35, 36) of the female sex (16, 32, 35) or both sexes (30, 31, 33, 34, 36), with ages ranging from 3 to 25 years. All the SRs included school setting, with some reviews also including community (i.e., public spaces like parks) (16, 31, 32, 36), primary care clinic/health centers (16, 31, 35), and after school hours setting (i.e., organized by school clubs, in or out of the school facilities) (33).
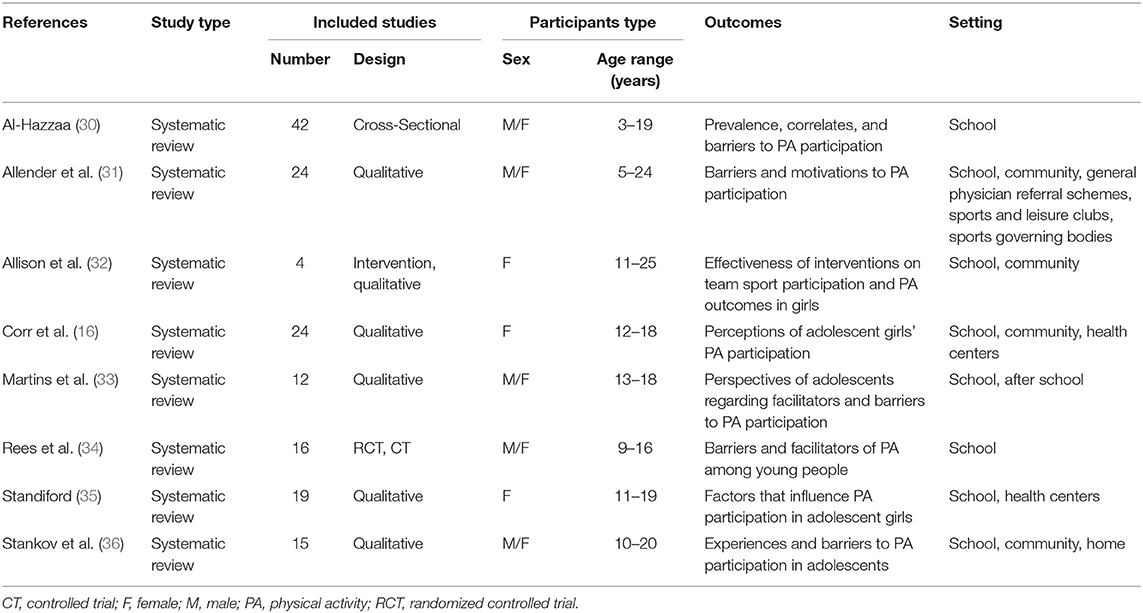
Table 1. Characteristics of the included studies.
Methodological Quality
Table 2 shows the assessment of methodological quality for each study. All studies were rated with “critically low-quality.” The critical domains where studies did not meet the quality requirements more frequently were the registration of the protocol before the commencement of the review (item 2, n = 7) and the consideration of the risk of bias when interpreting the results of the review (item 13, n = 6). In non-critical domains, all the reviews did not report the complete population, intervention, control group, and outcome (PICO) components (item 1, n = 8) and they also did not report the sources of funding of individual studies (item 10, n = 8). The reviewers were in total agreement on the methodological quality assigned to each study.
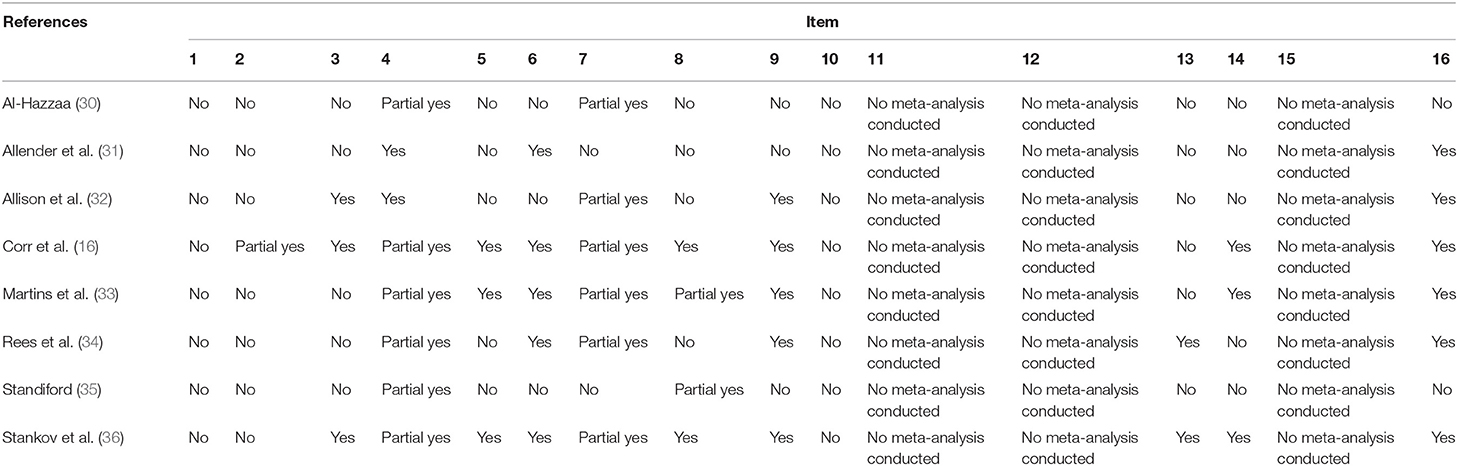
Table 2. Assessment of methodological quality of the selected systematic reviews using AMSTAR 2 tool.
Barriers and Facilitators
The barriers and facilitators that seem to have influenced PA participation among adolescent girls are described in Table 3. All the studies provided barriers, and seven studies also provided facilitators (16, 30–35). The most frequent PA barriers were the lack of support from peers (16, 32, 33, 35, 36), family (16, 33–36), and teachers (16, 31–33, 35), followed by lack of time (16, 30, 32, 33, 35). The most identified facilitators for PA were weight loss or management (30–34) and support from the peer (16, 31, 33–35), family (16, 31, 33–35), and teachers (16, 31–33, 35).
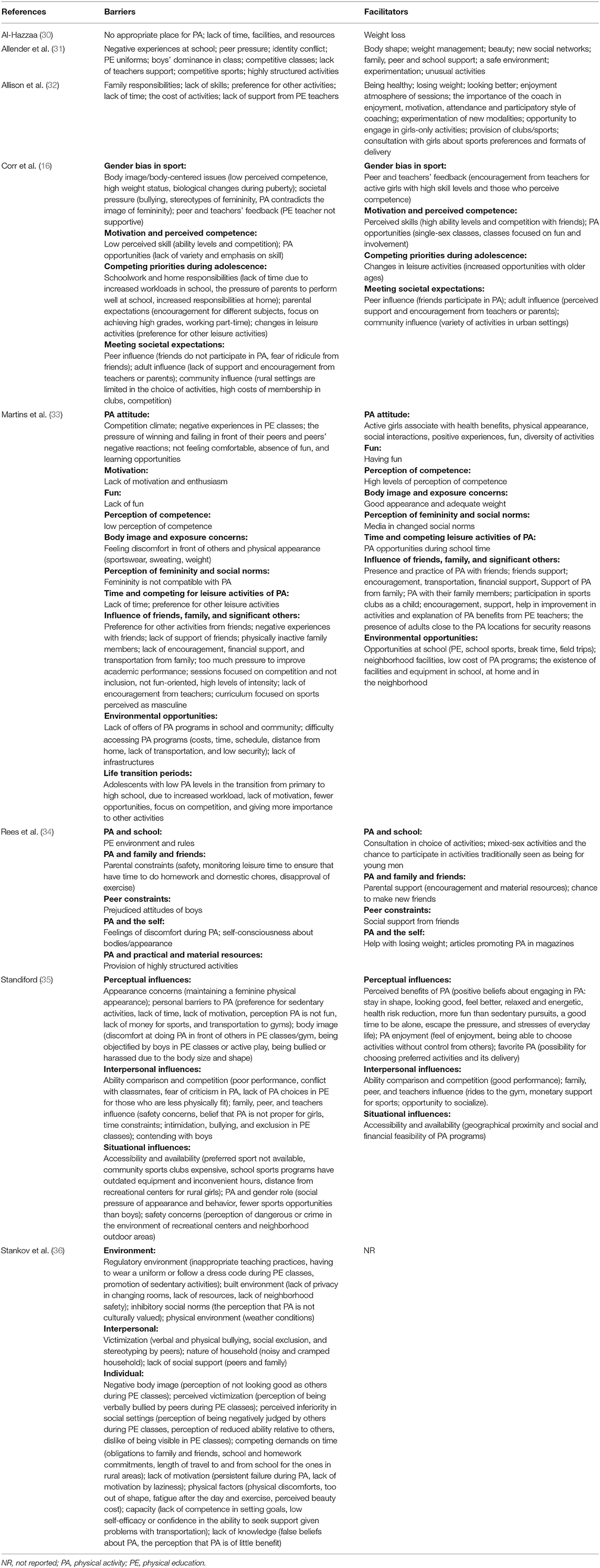
Table 3. Barriers and facilitators identified in the selected systematic reviews.
Individual
The most commonly mentioned barriers at the individual level were lack of time (16, 30, 32, 33, 35), lack of perceived competence (16, 32, 33, 36), discomfort during and after PA (33–36), increased obligations and responsibilities toward family and friends (16, 32, 34, 36), and preference for other leisure activities (16, 32, 33, 35). Regarding the facilitators for PA, the results show that the most reported in the individual level were weight loss or management (30–34), looking good and beauty perceptions (31–33, 35), perceived competencies (16, 33, 35), benefits of PA (33, 35), and enjoyment (33, 35).
Interpersonal
The most commonly mentioned barriers at the interpersonal level were the lack of support from family (16, 33–36), peers (16, 32, 33, 35, 36), and teachers (16, 31–33, 35). The most commonly mentioned facilitators at the interpersonal level were family (16, 31, 33–35), peer (16, 31, 33–35), and teachers (16, 31–33, 35), and the opportunity to socialize (31, 33–35).
Environmental
The most commonly mentioned barriers at the environmental level were the costs of activities available (16, 32, 33, 35), and safety concerns of the neighborhood outdoor areas and environment (33, 35, 36). The most commonly mentioned facilitators in the environmental level were the accessibility and availability of recreational centers (16, 32, 35), the opportunity to explore new activities (31, 32, 35), the consultation with girls about sports preferences and formats of delivery (32, 34), and the role of media have on influencing change in social norms (33, 34).
The distribution of the barriers and facilitators among the three levels (individual, interpersonal, and environment) is presented in Table 4.
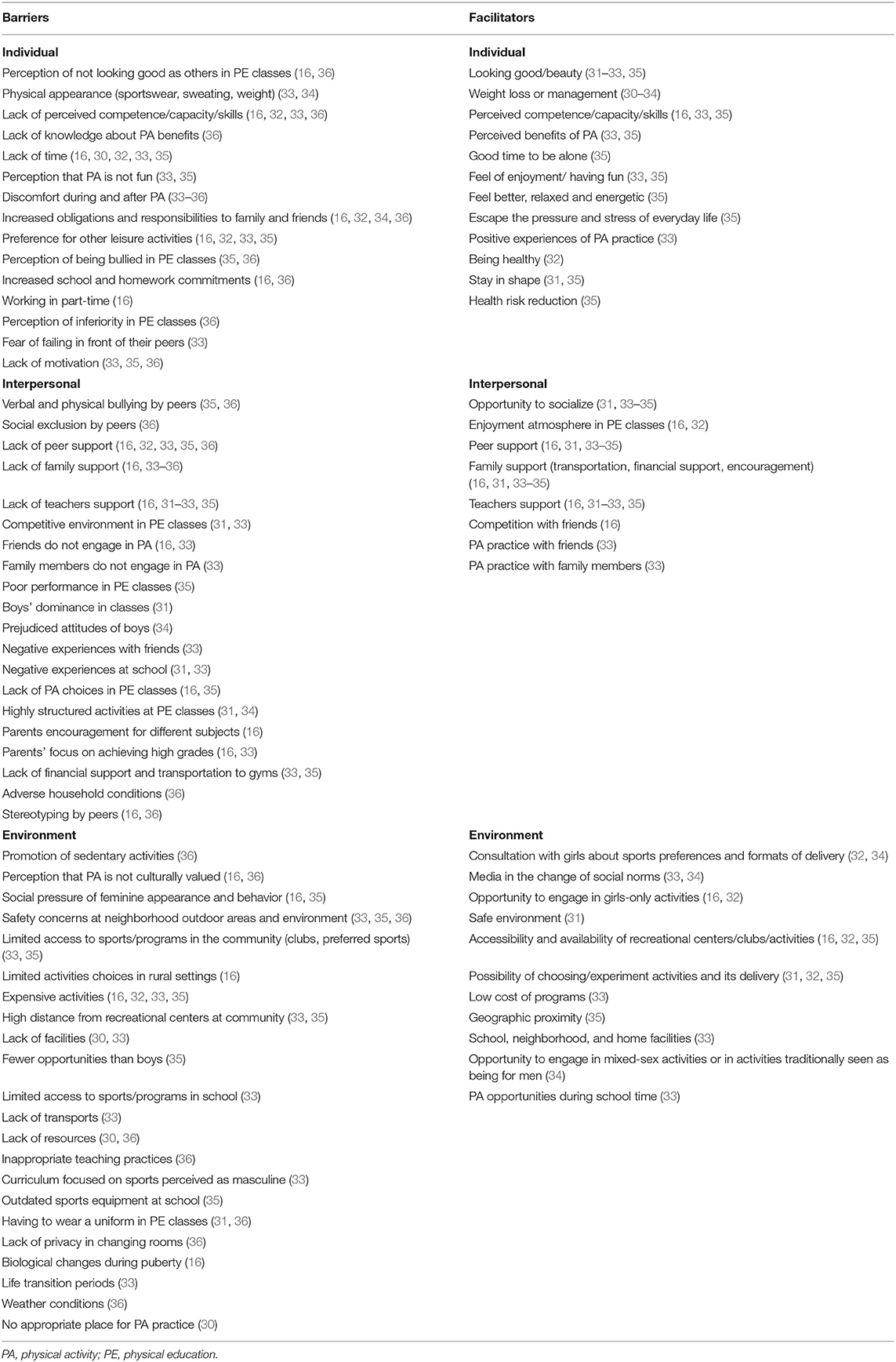
Table 4. Summary of barriers and facilitators in the selected systematic reviews.
Discussion
Summary of Main Findings
This SR of SRs summarizes the evidence of eight studies examining the barriers and facilitators of PA in adolescent girls. This synthesis has highlighted that the most frequent PA barriers reported in adolescent girls were found to be the lack of support from peers, family, and teachers, followed by the lack of time; the most identified facilitators reported for the PA of adolescent girls were weight loss/management, and peer, family, and teachers support (16, 31–33, 35). The majority of reported factors of influence hindering and/or supporting PA gathered in this review were mainly located in the individual and interpersonal levels.
Barriers and Facilitators
The socio-ecological model is one approach commonly mentioned as the most suitable method to illustrate complexities of examining the individual, physical, and social environmental factors when explaining PA behavior in general, therefore can be viewed as applicable for illustrating PA behavior of adolescent girls. Although the data were aggregated according to the three main levels, it is essential to note that there is a dynamic cross-over of barriers and facilitators, as one facilitator and/or barrier may be linked to another on a different level. For example, limited social support by a coach/teacher may occur due to the limited physical ability/skill of an individual leading to an overall negative experience, as mentioned in one review (35).
Although the barriers and facilitators by level can be seen separately, it is important to acknowledge the interplay and complexity of each and how they affect the participation of adolescent girls in PA overall when targeting within interventions. Further research is needed in terms of appropriate theoretical frameworks that can provide a clearer way to illustrate such complex intertwined factors that influence the PA participation of adolescent girls. This, in turn, can provide improved guidance when designing multicomponent interventions to target multiple influential factors that address these complex factors affecting PA participation of adolescent girls.
Approaches that can transform the role and relationship of harmful gender norms should be an aim of PA promotion (37). Gender norms have been known to play a significant role not only in the diverse exposure levels to the risk factors of non-communicable diseases in men and women but also in the access to and the use of services and resources (37). Gender norms and stereotypes have a specific influence on PA participation by creating societal expectations of what it means to be feminine/masculine that may limit the access to and use of PA opportunities available. For adolescent girls, gender stereotypes are seen as a barrier toward PA participation. With PA opportunities seen as socially appropriate to boys only, a perceived gender dominance occurs, which decreases the value and access to PA opportunities for girls (16, 30, 33, 35, 36). Not only do these norms hinder access to opportunities, but they also play a significant role in body image concerns. Although, body image was perceived as a facilitator in this synthesis (30–35) warrants should be made regarding the potential to negatively reinforce gender stereotypes that could be harmful to the physical and mental health of girls. Additionally, challenges exist in implementing gender-responsive PA interventions aimed at adolescent girls, calling for increased research and mechanisms on how to effectively respond (17).
Individual
Examples of individual barriers common across the reviews were associated with body image perceptions, such as feeling uncomfortable while participating in PA due to the concerns of appearance and discomfort that for example, were linked to the type of clothing worn and/or perceived skill level (16, 31–36). Consistent with previous research, negative body image and dissatisfaction have been associated with the age of adolescent girls which can contribute to the negative perceptions and experiences around PA participation (18, 38). Interventions that can increase the perceived competencies of girls could be considered one way of which to target negative self-ideals such as PA opportunities that focus on individual progression (18). However, self-perception has been considered largely influenced by the interpersonal and greater social contexts of cultural/gender ideals reinforced by family and peer groups (39). Evidence has suggested that mothers' conversation with adolescent girls around positive body image to be one way to foster improved body satisfaction (40), which may also aid in improved experiences with PA participation.
Adolescence is often marked as a highly sensitive and complex period of transition from childhood to adulthood (16). Further heightening vulnerabilities, biological changes experienced by adolescent girls during puberty can lead to discomfort while menstruating and combined with a heightened sense of self-consciousness which may, in fact, discourage participation in this age group (16). Research has suggested early maturing girls to be particularly prone to develop negative body images as they experience contradictions to the cultural ideals placed on them (39). Limited research has explored the role menstruation may play in hindering PA participation of adolescent girls since only one review in this synthesis mentioned menstruation as a barrier (16). Thus, further research should explore mechanisms to combat potential barriers of menstruation around PA participation as this review found limited evidence suggesting such implications.
Interpersonal
Interpersonal facilitators and barriers most commonly reported in this SR were the variety of and/or lack of support providers for PA of adolescent girls (16, 31–35). Support by peers, family, and teachers was mentioned evenly amongst the included reviews in this synthesis, potentially suggesting that each provider of support may have an equivalent influence on the PA of girls. A qualitative study that attempted to provide mechanisms for social support in PA for adolescents observed that receiving reinforcement and praise for PA, providing opportunities to practice and improve performance, and providing the practical support necessary to participate (equipment/money/transport) were key forms of support (41).
It is important to note that each support provider may play a different role in influencing the participation of girls in different settings. For example, supportive parents were found in this synthesis to play an essential role for adolescent girls by promoting PA time outside of school through means, such as financial support for the activities, transportation to activities, or overall encouragement to participate (16, 31, 33, 34). Similar research has acknowledged the influential support by parents toward PA of adolescent girls, especially young adolescents who may be more reliant on parents' ability to provide access to PA opportunities (i.e., equipment, cost of activity, and transportation) (42, 43).
This form of support places a burden on the financial ability and time of parents to provide the necessary access to resources and transportation to PA facilities, which may foster the potential inequalities from socioeconomic classes unable to provide the financial support required for adolescent girls to participate. Such disparities can also be seen within ethnic/minority PA participation of adolescent girls (18, 44, 45). Other forms of social support may provide a greater influence in PA participation less contingent on the family. For instance, social support by friends discovered in previous research was to be a greater predictor of meeting the daily PA recommendations for those with low access to PA resources (43). Teacher support, especially important in terms of school PA participation, influences adolescent girls from this synthesis mirrors existing research as well. Evidence has suggested that teacher support in the form of providing encouragement, praise, feedback, and enthusiasm directly targeting adolescent girls can provide increased positive dialog and engagement, which has been reportedly inexperienced by this group (41, 42).
Environmental
Most of the SRs in this synthesis focused on the school setting PA and reported barriers across all three levels: be it the teachers, social or physical environment, or the activity/curriculum. While numerous efforts have been made in the past decade to increase PA and sport participation of adolescent girls in this setting, many interventions have been found to have only small to limited effects (15). This may be due to the multidimensional barriers that span across the three levels, making it difficult to accurately address existing interventions targeting adolescent girls. Despite this, schools may be an important entry point for improved PA promotion among girls, especially if they are effective in changing the traditional structure of PE that hinders participation. This is consistent with existing literature that has made claims of gender biases in the PE curriculum calling for new ways of developing a more inclusive approach (46).
Considerations should be made to the social and built environment of the setting that offers PA in schools to be appropriate to gender preferences and needs. For instance, this synthesis found that some girls may prefer enjoyable activities that are non-skill-based, provide social opportunities, along with having a variety of activities to choose from, and the autonomy of which activity to participate in (16, 31–35). Alternatives to competitive sports with a focus on physical fitness and enjoyment could help adolescent girls develop positive PA habits according to their abilities and skills, which could, in turn, increase the likelihood of lifelong engagement in PA (16, 33).
Environments outside of the school setting, such as the constructed setting of parks, sidewalks, street lights, distance to school, and the neighborhood that one lives in have found an influence on the PA levels in adolescent girls (42, 47, 48), which is in accordance with findings from this review.
Limitations
Notwithstanding, there are limitations that must be considered when interpreting the findings from this synthesis. Although this SR aimed to identify key barriers and facilitators for adolescent girls on a global level, we acknowledge that adolescent girls may face different obstacles unique to their social, cultural, and regional contexts that cannot be generalized in this review.
A major gap highlighted in this review is that most of the SRs included studies that were primarily conducted in high-income settings. As the global disparities of PA continue to rise in adolescent girls, additional interventions and research is needed throughout diverse regional settings due to the potential contextual variances in PA norms and environmental situations (15, 16, 49).
Despite that general implications can continue to be warranted to an extent, it is important to also note that differences in perceptions of barriers and facilitators in adolescent girls could relate to how active or inactive a girl is, as some evidence discovered not all girls prefer the same type of activities (16, 33). In addition, some barriers and facilitators explicitly mentioned for adolescent girls in this review may also affect adolescent boys to some extent, given the adolescent period of social pressures and norms.
One limitation worth noting is that the SRs included in this review did not exclusively reflect adolescent girls aged 10–19, as some reviews reported on both sex and a variety of age ranges. Therefore, some barriers and facilitators may not be representative for adolescence, but also for transition periods, such as childhood and early adulthood. By including studies in both sexes, it allowed us to highlight the limitation that barriers and facilitators mentioned in this review may not only affect adolescent girls, thereby highlighting the difficulties placed in providing a clear gender-responsive direction in targeting interventions. For example, SRs included in this study that investigated both genders identified a few common barriers across genders, such as lack of time (30, 33), perceived skill level (33, 36), and family support (33, 34, 36).
Furthermore, included SRs were ranked as having low methodological quality. However, besides the AMSTAR 2 Tool being described as adequate for the assessment of the methodological quality of SR of SRs, this tool is more appropriate for healthcare interventions and not for studies of a qualitative nature. Therefore, results should be interpreted with caution.
Implications for Action
The findings of this review aimed to provide a backdrop of considerations for policymakers and implementers when taking a gender-responsive approach to the promotion of PA in adolescent girls. Based on the evidence synthesized in this review, key courses of action can be applied in practice.
Inclusive Approach to Curriculum Development to Address Gender Norms
It is necessary to have an inclusive approach to curriculum development for adolescent girls to address their specific needs. An Intersectoral approach involving education, sports, and health sectors should be considered in designing PE curricula that place a gender-responsive view of preferences of adolescent girls. This may require policies within the education and sports sector that can hold accountable the gender-responsive targeted action required in these modifications.
More dialog addressing harmful gender norms in the settings where PA takes place may help identify and address the barriers that discourage participation (33). Examples may include involving institutions, teachers, and boys in recognizing and addressing their own contribution to enabling these norms and encourage fostering a supportive environment for PA participation of girls. A curriculum that is non-competitive, flexible, individually created with a variety of opportunities, and the time to perform PA are some examples of how to adapt to the preferences of adolescent girls. Policies and initiatives that can support PA outside the traditional PE setting in schools, such as active breaks and active extracurricular activities are additional ways to encourage increase PA opportunities.
Adequate Training of Professionals to Ensure Inclusion of Adolescent Girls
Adequate training of professionals is required to equip them with the knowledge and skills to provide an inclusive PA environment for adolescent girls. Trained professionals should possess the understanding of the negative implications of lack of support provided to PA of girls, regardless of skill level and strategies on how to be more gender-responsive in their support provided specifically to girls. Qualified professionals should consider focusing on increasing physical literacy at earlier ages to build the confidence and skills required to maintain adequate PA levels throughout adolescence (50). Policies should be in place to ensure continued professional development and the availability of appropriate resources and material to provide gender-responsive PA strategies in school and sports club settings. Strategies and proper training of parents and peers to provide support for the PA participation of girls should also be considered due to its strong influence in facilitating PA (16, 31, 33–35). Examples of ways in which parents and peers can encourage PA support in girls include participating in PA with adolescent girls and providing positive reinforcement for conducting PA (41). Interventions that can provide family participation and engagement in PA should also be considered.
Environmental Changes in and Out of Schools to Stimulate Participation, to Allow Adolescent Girls to Be Active in a Safe and Attractive Environment
It is essential to stimulate PA participation with environmental modifications. Increasing access to safe and comfortable physical infrastructures and facilities for the use of adolescent girls should be a priority within and outside the school setting. Cost-effective PA interventions are needed so that they can be delivered with limited resources with little to no cost to families and increasing family support and participation of all children and adolescents, but with special attention toward techniques that can encourage adolescent girls specifically (33).
Policies that aim to provide equal opportunities regardless of gender and financial resources to tackle the larger structural barriers toward PA participation in adolescent girls are required. At the local level, policies and initiatives should address how public open spaces can be rendered more appealing to girls regarding safety and accessibility by addressing their specific concerns.
Community mobilization and engagement are necessary to foster a conducive environment supportive for the participation of adolescent girls in these spaces. Schemes that can encourage active travel to and from school are other ways in which schools and local authorities can work together toward increasing PA opportunities. In addition, recreational PA initiatives that can encourage peer engagement of adolescent girls should also be considered.
Multistakeholder Support at the Local, Regional, and National Level in Incorporating a Gender-Responsive Approach Toward PA Participation
For the promotion of PA to be effective, it is essential for multistakeholder engagement at the individual, community, cultural, political, and environmental levels (51). Investing in policies that encourage PA for adolescent girls across these levels in and outside the school setting is deemed necessary for taking a gender-responsive action toward PA promotion. For example, active commuting to and from school has been described as a way to enhance PA practice, but this can be compromised if other measures are not implemented, such as safe sidewalks and cycle paths that provide routes to school along with neighborhood safety (8, 52, 53).
At the country level, leadership and coordination across sectors are fundamental to maximize the response required to address low levels of PA of adolescent girls. Ensuring national measures are taken to promote gender equality in PA can be reflected in policies that support gender-relevant forms of activity, particularly in school and recreational time, which can decrease sedentary leisure time activities (25).
The attainment of effective policies that increase PA levels in adolescent girls will contribute to meeting SDG number five, by promoting gender equality and the empowerment of girls at all levels, both essential for a peaceful, prosperous, and sustainable world (24). Gender equality and norms are strengthened and integrated during the adolescence period, when transitions to individualized identities, sexual activity, labor force participation, and marriage may occur. Interventions in the early stage in patterns of health behaviors, such as PA, will influence health trajectories over the life course (27).
Future Research
Despite the available evidence on the multiple barriers and facilitators that influence the PA of adolescent girls, research is required in terms of appropriate theoretical frameworks that can provide a clearer way to illustrate the multifaceted factors that influence the PA participation of adolescent girls. Such evidence can guide intervention designs aimed to target the multiple influential factors for PA promotion of adolescent girls and provide a clearer picture of what a gender-responsive approach toward action can look like.
Future research on PA should explore the factors for increasing PA among specific subgroups of adolescent girls (e.g., low socioeconomic status, migrant, transgender, girls living with disability, and pregnant/post-partum adolescent girls) along with the barriers and facilitators of transition periods (childhood to adolescence and adolescence to adulthood) longitudinally, to further promote PA in a life-course approach. Further research should also explore developing and testing gender-specific and gender-transformative PA programs for this population to gain effective and evidence-based PA programs, good practices and policies, at local, regional and national levels, as well as its proper monitoring and evaluation. Such evidence is needed to disseminate practical recommendations from research for policymakers at different levels.
Conclusion
This SR of SRs highlights the collected evidence that there is a variety of factors that influence the PA of adolescent girls. Lack of support from peers, family, and teachers, and the lack of time were among the most frequent barriers for adolescent girls while the motivation for weight loss and support from peers, family, and teachers were the most frequent facilitators toward PA participation.
This study provided key areas for policy action to promote PA in adolescent girls, based on the most frequent barriers and facilitators experienced. For the attainment of effective policies and practices that increase PA levels in adolescent girls, a multisectoral and multilevel gender-responsive response is necessary.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author Contributions
KD, AB, SW, RM, IA, AT, KA-O, PG, and JB: conceptualization and writing—original draft preparation. KD, AB, SW, and RM: methodology. KD, AB, and RM: formal analysis. KD and AB: interpretation of data for the work. SW, RM, IA, AT, KA-O, PG, and JB: writing—review and editing and supervision. All authors have read and agreed to the published version of the manuscript.
Funding
This work was support by a grant from the Government of the Russian Federation in the context of the WHO European Office for the Prevention and Control of Non-communicable Diseases.
Author Disclaimer
The authors alone are responsible for the views expressed in this publication, and they do not necessarily represent the views, decisions, or policies of the institutions with which they are affiliated.
Conflict of Interest
SW, IA, and JB are staff members of the WHO. KD, AB, and RM are WHO consultants.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2021.743935/full#supplementary-material
References
1. Colberg SR, Sigal RJ, Yardley JE, Riddell MC, Dunstan DW, Dempsey PC, et al. Physical activity/exercise and diabetes: a position statement of the american diabetes association. Diabetes Care. (2016) 39:2065–79. doi: 10.2337/dc16-1728
2. Anderson L, Oldridge N, Thompson DR, Zwisler A-D, Rees K, Martin N, et al. Exercise-Based cardiac rehabilitation for coronary heart disease: cochrane systematic review and meta-analysis. J Am Coll Cardiol. (2016) 67:1–12. doi: 10.1002/14651858.CD001800.pub3
3. Hu MX, Turner D, Generaal E, Bos D, Ikram MK, Ikram MA, et al. Exercise interventions for the prevention of depression: a systematic review of meta-analyses. BMC Public Health. (2020) 20:1255. doi: 10.1186/s12889-020-09323-y
4. Rezende LFM de, Sá TH de, Markozannes G, Rey-López JP, Lee I-M, Tsilidis KK, et al. Physical activity and cancer: an umbrella review of the literature including 22 major anatomical sites and 770 000 cancer cases. Br J Sports Med. (2018) 52:826–33. doi: 10.1136/bjsports-2017-098391
5. Lear SA, Hu W, Rangarajan S, Gasevic D, Leong D, Iqbal R, et al. The effect of physical activity on mortality and cardiovascular disease in 130 000 people from 17 high-income, middle-income, and low-income countries: the PURE study. Lancet Lond Engl. (2017) 390:2643–54. doi: 10.1016/S0140-6736(17)31634-3
6. Biddle SJH, Asare M. Physical activity and mental health in children and adolescents: a review of reviews. Br J Sports Med. (2011) 45:886–95. doi: 10.1136/bjsports-2011-090185
7. Shiri R, Falah-Hassani K. Does leisure time physical activity protect against low back pain? Systematic review and meta-analysis of 36 prospective cohort studies. Br J Sports Med. (2017) 51:1410–8. doi: 10.1136/bjsports-2016-097352
8. Barbosa A, Whiting S, Simmonds P, Scotini Moreno R, Mendes R, Breda J. Physical activity and academic achievement: an umbrella review. Int J Environ Res Public Health. (2020) 17:5972. doi: 10.3390/ijerph17165972
9. Penedo FJ, Dahn JR. Exercise and well-being: a review of mental and physical health benefits associated with physical activity. Curr Opin Psychiatry. (2005) 18:189–93. doi: 10.1097/00001504-200503000-00013
10. Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, et al. World health organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. (2020) 54:1451–62. doi: 10.1136/bjsports-2020-102955
11. Guthold R, Stevens GA, Riley LM, Bull FC. Global trends in insufficient physical activity among adolescents: a pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc Health. (2020) 4:23–35. doi: 10.1016/S2352-4642(19)30323-2
12. World Health Organization. More Active People for a Healthier World: Global Action Plan on Physical Activity 2018-2030. (2018). Available online at: https://apps.who.int/iris/bitstream/handle/10665/272722/9789241514187-eng.pdf (accessed January 15, 2021).
13. Brown WJ, Mielke GI, Kolbe-Alexander TL. Gender equality in sport for improved public health. Lancet Lond Engl. (2016) 388:1257–8. doi: 10.1016/S0140-6736(16)30881-9
14. United Nations. Seventy-Fifth Session of the General Assembly. Item 11 of the Preliminary List*Sport for Development and Peace; Sport: A Global Accelerator of Peace and Sustainable Development for all. Report of the Secretary-General. United Nations (2020). Available online at: https://www.un.org/development/desa/dspd/wp-content/uploads/sites/22/2020/09/A75155-Sport-SG-report-ENG.pdf (accessed January 15, 2021).
15. Owen MB, Curry WB, Kerner C, Newson L, Fairclough SJ. The effectiveness of school-based physical activity interventions for adolescent girls: a systematic review and meta-analysis. Prev Med. (2017) 105:237–49. doi: 10.1016/j.ypmed.2017.09.018
16. Corr M, McSharry J, Murtagh EM. Adolescent girls' perceptions of physical activity: a systematic review of qualitative studies. Am J Health Promot. (2018) 33:806–19. doi: 10.1177/0890117118818747
17. Okely AD, Lubans DR, Morgan PJ, Cotton W, Peralta L, Miller J, et al. Promoting physical activity among adolescent girls: the girls in sport group randomized trial. Int J Behav Nutr Phys Act. (2017) 14:81. doi: 10.1186/s12966-017-0535-6
18. Cowley ES, Watson PM, Foweather L, Belton S, Thompson A, Thijssen D, et al. “Girls aren't meant to exercise”: perceived influences on physical activity among adolescent girls-the HERizon project. Child Basel Switz. (2021) 8:31. doi: 10.3390/children8010031
19. Bagby K, Adams S. Evidence-based practice guideline: increasing physical activity in schools–kindergarten through 8th grade. J Sch Nurs. (2007) 23:137–43. doi: 10.1177/10598405070230030301
20. Casey MM, Eime RM, Payne WR, Harvey JT. Using a socioecological approach to examine participation in sport and physical activity among rural adolescent girls. Qual Health Res. (2009) 19:881–93. doi: 10.1177/1049732309338198
21. Elder JP, Lytle L, Sallis JF, Young DR, Steckler A, Simons-Morton D, et al. A description of the social-ecological framework used in the trial of activity for adolescent girls (TAAG). Health Educ Res. (2007) 22:155–65. doi: 10.1093/her/cyl059
23. United Nations. United Nations: convention on the elimination of all forms of discrimination against women. Int Leg Mater. (2010) 19:33–45. doi: 10.1017/S0020782900043448
24. United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development. New York, NY (2015). Available online at: https://sustainabledevelopment.un.org/post2015/transformingourworld/publication (accessed January 15, 2021).
25. WHO Regional Office for Europe. Physical Activity Strategy for the WHO European Region 2016–2025. Vilnius: World Health Organization Regional Office For Europe (2015). Available online at: http://www.euro.who.int/__data/assets/pdf_file/0010/282961/65wd09e_PhysicalActivityStrategy_150474.pdf (accessed January 20, 2021).
26. Blum RW, Mmari K, Moreau C. It begins at 10: how gender expectations shape early adolescence around the world. J Adolesc Health. (2017) 61 (4. Suppl):S3–4. doi: 10.1016/j.jadohealth.2017.07.009
27. Lane C, Brundage CL, Kreinin T. Why we must invest in early adolescence: early intervention, lasting impact. J Adolesc Health. (2017) 61:S10–1. doi: 10.1016/j.jadohealth.2017.07.011
28. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
29. Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. (2017) 358:j4008. doi: 10.1136/bmj.j4008
30. Al-Hazzaa HM. Physical inactivity in Saudi Arabia revisited: a systematic review of inactivity prevalence and perceived barriers to active living. Int J Health Sci. (2018) 12:50–64. doi: 10.2196/preprints.9883
31. Allender S, Cowburn G, Foster C. Understanding participation in sport and physical activity among children and adults: a review of qualitative studies. Health Educ Res. (2006) 21:826–35. doi: 10.1093/her/cyl063
32. Allison R, Bird E, Mcclean S. Is team sport the key to getting everybody active, every day? A systematic review of physical activity interventions aimed at increasing girls' participation in team sport. AIMS Public Health. (2017) 4:202–20. doi: 10.3934/publichealth.2017.2.202
33. Martins J, Marques A, Sarmento H, Carreiro da Costa F. Adolescents' perspectives on the barriers and facilitators of physical activity: a systematic review of qualitative studies. Health Educ Res. (2015) 30:742–55. doi: 10.1093/her/cyv042
34. Rees R, Kavanagh J, Harden A, Shepherd J, Brunton G, Oliver S, et al. Young people and physical activity: a systematic review matching their views to effective interventions. Health Educ Res. (2006) 21:806–25. doi: 10.1093/her/cyl120
35. Standiford A. The secret struggle of the active girl: a qualitative synthesis of interpersonal factors that influence physical activity in adolescent girls. Health Care Women Int. (2013) 34:860–77. doi: 10.1080/07399332.2013.794464
36. Stankov I, Olds T, Cargo M. Overweight and obese adolescents: what turns them off physical activity? Int J Behav Nutr Phys Act. (2012) 9:53. doi: 10.1186/1479-5868-9-53
37. World Health Organization. Why using a gender approach can accelerate noncommunicable disease prevention and control in the who european region. In: WHO European High-Level Conference on Noncommunicable Diseases. Time to Deliver: Meeting NCD Targets to Achieve Sustainable Development Goals in Europe 9-10 April 2019, Ashgabat, Turkmenistan. Turkmenistan: WHO Regional Office for Europe (2019). Available online at: https://www.euro.who.int/__data/assets/pdf_file/0003/399063/GenderApproachAndNCDsPreventionAndControl-eng.PDF (accessed January 20, 2021).
38. Fernández-Bustos JG Infantes-Paniagua Á Cuevas R Contreras OR. Effect of physical activity on self-concept: theoretical model on the mediation of body image and physical self-concept in adolescents. Front Psychol. (2019) 10:1537. doi: 10.3389/fpsyg.2019.01537
39. Voelker DK, Reel JJ, Greenleaf C. Weight status and body image perceptions in adolescents: current perspectives. Adolesc Health Med Ther. (2015) 6:149–58. doi: 10.2147/AHMT.S68344
40. Hart E, Chow CM. “I just don't want to be fat!”: body talk, body dissatisfaction, and eating disorder symptoms in mother-adolescent girl dyads. Eat Weight Disord. (2020) 25:1235–42. doi: 10.1007/s40519-019-00756-y
41. Laird Y, Fawkner S, Niven A. A grounded theory of how social support influences physical activity in adolescent girls. Int J Qual Stud Health Well-Being. (2018) 13:1435099. doi: 10.1080/17482631.2018.1435099
42. Budd EL, McQueen A, Eyler AA, Haire-Joshu D, Auslander WF, Brownson RC. The role of physical activity enjoyment in the pathways from the social and physical environments to physical activity of early adolescent girls. Prev Med. (2018) 111:6–13. doi: 10.1016/j.ypmed.2018.02.015
43. Gill M, Chan-Golston AM, Rice LN, Roth SE, Crespi CM, Cole BL, et al. Correlates of social support and its association with physical activity among young adolescents. Health Educ Behav. (2017) 45:207–16. doi: 10.1177/1090198117714826
44. Singh GK, Yu SM, Siahpush M, Kogan MD. High levels of physical inactivity and sedentary behaviors among US immigrant children and adolescents. Arch Pediatr Adolesc Med. (2008) 162:756–63. doi: 10.1001/archpedi.162.8.756
45. Priest N, Armstrong R, Doyle J, Waters E. Interventions implemented through sporting organisations for increasing participation in sport. Cochrane Database Syst Rev. (2008) 16:CD004812. doi: 10.1002/14651858.CD004812.pub3
46. Bailey R. Evaluating the relationship between physical education, sport and social inclusion. Educ Rev. (2005) 57:71–90. doi: 10.1080/0013191042000274196
47. Van Hecke L, Verhoeven H, Clarys P, Van Dyck D, Van de Weghe N, Baert T, et al. Factors related with public open space use among adolescents : a study using GPS and accelerometers. Int J Health Geogr. (2018) 17:3. doi: 10.1186/s12942-018-0123-2
48. Martins J, Marques A, Rodrigues A, Sarmento H, Onofre M, Carreiro da Costa F. Exploring the perspectives of physically active and inactive adolescents: how does physical education influence their lifestyles? Sport Educ Soc. (2018) 23:505–19. doi: 10.1080/13573322.2016.1229290
49. Camacho-Miñano MJ, LaVoi NM, Barr-Anderson DJ. Interventions to promote physical activity among young and adolescent girls: a systematic review. Health Educ Res. (2011) 26:1025–49. doi: 10.1093/her/cyr040
50. Faigenbaum AD, Rebullido TR, MacDonald JP. Pediatric inactivity triad: a risky PIT. Curr Sports Med Rep. (2018) 17:45–7. doi: 10.1249/JSR.0000000000000450
51. Rigby BP, van der Graaf P, Azevedo LB, Hayes L, Gardner B, Dodd-Reynolds CJ. Challenges, opportunities and solutions for local physical activity stakeholders: an implementation case study from a cross-sectoral physical activity network in Northeast England. BMC Public Health. (2020) 20:1760. doi: 10.1186/s12889-020-09847-3
52. Kerr J, Rosenberg D, Sallis JF, Saelens BE, Frank LD, Conway TL. Active commuting to school: associations with environment and parental concerns. Med Sci Sports Exerc. (2006) 38:787–94. doi: 10.1249/01.mss.0000210208.63565.73
Keywords: adolescence, gender, exercise, physical activity, public health, policy
Citation: Duffey K, Barbosa A, Whiting S, Mendes R, Yordi Aguirre I, Tcymbal A, Abu-Omar K, Gelius P and Breda J (2021) Barriers and Facilitators of Physical Activity Participation in Adolescent Girls: A Systematic Review of Systematic Reviews. Front. Public Health 9:743935. doi: 10.3389/fpubh.2021.743935
Received: 19 July 2021; Accepted: 17 September 2021;
Published: 15 October 2021.
Edited by:
Germán Vicente-Rodriguez, University of Zaragoza, SpainReviewed by:
Ivana I. Kavecan, University of Novi Sad, SerbiaKatalin Dr. Papp, University of Debrecen, Hungary
Copyright © 2021 Duffey, Barbosa, Whiting, Mendes, Yordi Aguirre, Tcymbal, Abu-Omar, Gelius and Breda. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Keeva Duffey, keeva.duffey@gmail.com