Associations Between Independent Assessments of Child Appetite Self-Regulation: A Narrative Review
 Maria A. Papaioannou
Maria A. Papaioannou Nilda Micheli
Nilda Micheli Thomas G. Power
Thomas G. Power Jennifer O. Fisher
Jennifer O. Fisher Sheryl O. Hughes
Sheryl O. Hughes- 1Department of Pediatrics, United States Department of Agriculture/Agricultural Research Service (USDA/ARS) Children's Nutrition Research Center, Baylor College of Medicine, Houston, TX, United States
- 2Department of Human Development, Washington State University, Pullman, WA, United States
- 3Department of Social and Behavioral Sciences, Center for Obesity Research and Education, Temple University, Philadelphia, PA, United States
A variety of eating behaviors among children have been associated with obesity risk and are thought to broadly reflect child appetite self-regulation (ASR). While ASR is thought to occur on cognitive, emotional, motivational, biological, and behavioral levels, the inter-relatedness of ASR constructs as assessed by different methods/measures is not well-characterized. This narrative review describes the correspondence between different methods/measures of child ASR constructs as assessed by self-report questionnaires and/or observational tasks and their relationship to child standardized body mass index (BMIz). Research involving at least two different methods/measures is presented including observational tasks such as the Eating in the Absence of Hunger task, compensation trials, and eating rate, as well as various child eating behavior self-report questionnaires. Keyword searches in the PubMed and PsycINFO databases for articles published between 2000 and July 2021 identified 21,042 articles. Eighteen articles met the inclusion criteria and examined at least two of the targeted measures. Studies comparing questionnaire data with other questionnaire data showed the most evidence of significant associations (r values ranging from −0.45 to 0.49), whereas studies comparing questionnaires with observational tasks mostly showed weak (r values ranging from −0.17 to 0.19) or not significant associations, with only few studies finding moderate associations (r values ranging from −0.38 to 0.33). Studies comparing different observational tasks showed no significant associations. Overall, studies comparing self-report questionnaires showed the most correspondence, whereas those comparing observational tasks showed no correspondence. Studies across methods (questionnaires with tasks) showed less correspondence. Significant associations were found between ASR constructs and child BMIz across five studies using self-report questionnaires and two studies using observational tasks. Future research is needed to clearly define the various ASR constructs, their expected correspondence, and the strength of that correspondence, as well as the relations between ASR constructs and child weight among youth with and without overweight/obesity.
Introduction
Child appetite self-regulation (ASR) has been identified as a central mechanism in the development of childhood obesity and has been targeted as a modifiable target in childhood obesity prevention programs (1–6). Definitions of ASR span multiple disciplines including the developmental sciences, nutrition, clinical psychology, and public health. Using a biopsychosocial framework, Russell and Russell (7) recently described ASR as multidimensional latent construct that occurs at “…cognitive, emotional, motivational, biological, and behavioral levels” and can be conceptualized in at least three ways. In the first conceptualization, top-down cognitive processes of ASR, such as inhibitory control, are thought to moderate bottom-up biologically drives toward food approach and avoidance. Top-down processes reflect effortful and executive control, whereas bottom-up processes reflect reactive, automatic processes that have neural origins. A second conceptualization included behavioral manifestations of ASR such as food choices and consumption as well as regulatory elements of hunger, satiation (during eating; brings meal to end), and satiety (after end of eating; prevents eating again before hunger). Lastly, ASR can be conceptualized as a process, a trait, or a skill (7), all of which can be measured using different methods. For example, ASR as a process or a skill can be measured using observational methods (e.g., Eating in the Absence of Hunger protocol), whereas ASR as a trait can be measured using a survey (e.g., the Children's Eating Behavior Questionnaire). While these recent theoretical advances provide a robust conceptual framework, measurement of ASR remains quite varied, and the inter-relatedness of different ASR constructs as measured by the various methods and measures is not well-characterized.
The present narrative review was undertaken to evaluate the correspondence of different methods/measures that have been used to assess common ASR constructs that are relevant to obesity risk in young children. Drawing on current multidimensional conceptualizations of ASR (7) and reviews of the extant literature on child obesogenic eating behaviors (8, 9), we focused on commonly used measures of ASR constructs that reflect multiple aspects of ASR (e.g., top-down processes, satiation) but predominantly emphasize reactive bottom-up processes. The current review focused on original research studies that included self-report questionnaires and/or observational tasks to assess common ASR constructs. Observational tasks measuring ASR constructs included compensation trials, Eating in the Absence of Hunger (EAH), and eating microstructure (i.e., eating rate and bite size). ASR self-report measures included the Children's Eating Behavior Questionnaire (parent-report), the Dutch Eating Behavior Questionnaire (parent- and child-report), the Eating in the Absence of Hunger Questionnaire (parent- and child-report), and the children's Self-Regulation in Eating scale (parent-report) by Tan and Holub. A brief description of the measures is given below to illustrate the diversity of measurement approaches and operational definitions employed in the study of ASR among children.
Among observational tasks, compensation trials have been used to assess satiation in children. Specifically, compensation protocols typically characterize the extent to which children adjust food intake at an ad libitum meal in response to the energy content of a compulsory preload consumed prior to the meal (10, 11). In other words, this protocol addresses whether children overeat, undereat, or accurately compensate at meals for prior intake. The EAH task assesses satiety by measuring children's intake of palatable foods (i.e., sweet and savory snacks) provided after a meal (along with a stack of toys) (12). Finally, average eating rate and average bite size are used to assess the eating microstructure, often in the context of satiation, by characterizing the number of mouthfuls eaten per minute and by gram, respectively (13, 14). Faster average eating rates and larger average bite sizes are thought to promote excessive intake by outpacing internal satiation signals (13, 14).
Among ASR self-report measures, the most commonly used are the Children's Eating Behavior Questionnaire (CEBQ; parent-report) (15) and the Dutch Eating Behavior Questionnaire [DEBQ; parent- (16) and child-report (17)]. The CEBQ measures eight appetitive traits of children 2 years old and above across 35 items using a 5-point Likert scale. Four of the eight traits are food approaching (i.e., food responsiveness or how responsive a child is to food/eating, emotional overeating, enjoyment of food, and desire to drink) and four are food avoidant (i.e., satiety responsiveness or how responsive a child is to feelings of fullness, emotional undereating, slowness in eating, and food fussiness) (15). The child-report of the DEBQ measures emotional eating, external eating, and restrained eating in children ages 7–12 years across 20 items using a 3-point scale (17). The parent-report of the DEBQ (parent report of child behaviors) measures the same constructs across 30 items on a 5-point scale (16). In addition to the CEBQ and the DEBQ, there are a number of other tools that have been used to assess ASR. For example, the Eating in the Absence of Hunger Questionnaire has two parallel versions, a parent-report of child behaviors (EAH-PC) (18), and a child-report (EAH-C) (19) used with children ages 8–18 years. Both versions assess the frequency of eating in the absence of hunger and specifically measure external eating, negative affect, and fatigue/boredom across 14 items on a 5-point Likert scale. Tan and Holub's children's Self-Regulation in Eating scale (SRES; parent-report) assesses parental beliefs regarding child's ability to self-regulate eating across 8 items on a 5-point Likert scale (20).
Considering the difficulty of operationalizing and explicitly measuring child ASR as well as the various assessment methods available, it is important for research and prevention efforts to understand how ASR constructs as assessed by different methods/measures are related (21). For example, caloric compensation, as measured by compensation trials is thought to be a behavioral analog or manifestation of satiety responsiveness, as measured by the CEBQ (22, 23). While it is not uncommon to employ multiple measures of ASR (24–27), little research to date has been undertaken with the specific goal of characterizing the correspondence of ASR constructs. Further, patterns of associations have been mixed, with some studies utilizing independent measures showing weak associations between ASR measures (25, 26) and others showing no significant associations (24, 27). While ASR is often described in general terms, it is thought to occur at multiple levels and be manifested across a wide range of dimensions. Characterizing the inter-relatedness of ASR constructs as measured by different methods/measures is critical to advance theoretical understanding of the role of ASR in obesity risk and prevention during early childhood.
In this context, the purpose of this narrative review is to describe the correspondence of methods/measures of common ASR constructs relevant to obesity risk in children and to examine the associations between different methods/measures and child standardized body mass index (BMIz). The review focuses on original research studies that included at least two ASR assessment methods (self-report questionnaires and observational tasks) as well as measures within each methodology (i.e., a study including at least two self-report questionnaires or at least two observational tasks). Measures chosen within each methodology were those that are notably related to child obesity risk in the current literature. The review also focuses on children ages 2–12 years for two reasons: (1) eating behaviors mainly develop during this period and (2) this is the time when children are still somewhat dependent on their caregivers while becoming more autonomous and independent in their food choices (28).
Methods
This narrative review of the literature involved an iterative process of searching for original research articles that included at least two assessments of child ASR constructs from self-report questionnaires and observational tasks. Self-report questionnaires included parent reports of child behaviors as well as child self-reports. We focused on the following constructs that are applicable to ASR: food responsiveness, satiety responsiveness, emotional overeating, external eating, eating in the absence of hunger, eating rate, bite size, slowness in eating, caloric or energy compensation, and satiation and satiety. During this process, additional constructs emerged (e.g., children's self-regulation in eating). Table 1 provides an overview of the constructs, their definitions, and respective assessment tools.
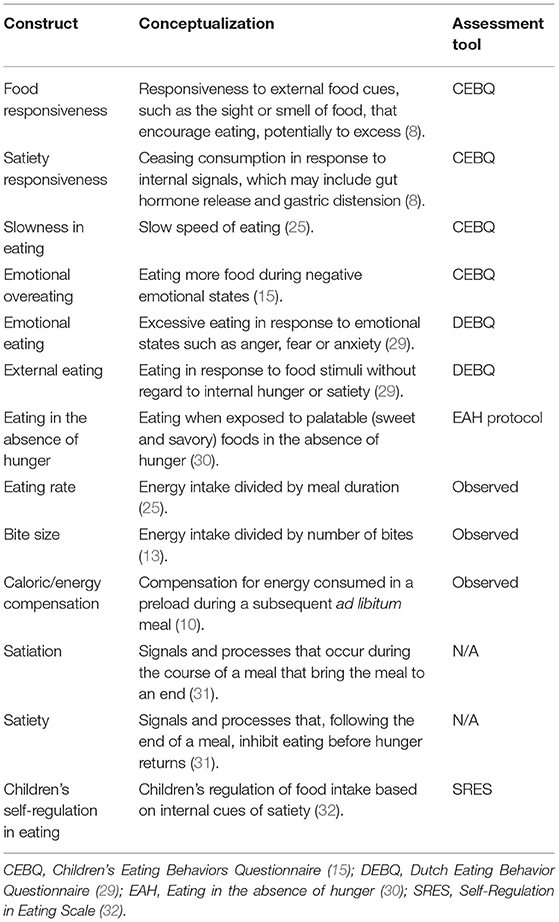
Table 1. Conceptualizations and assessment tools of constructs.
Review Question
The focus of the review was to examine correlational data between different ASR constructs among children as assessed by at least two different methods/measures (self-report questionnaires and observational tasks). We excluded reports of correlations between subscales of the same questionnaire because they do not represent independent assessments.
Search Strategy
Keyword searches were conducted in electronic databases (PubMed and PsycINFO) in July 2021 using the following terms: (appetitive traits) OR (appetite self-regulation) OR (appetite regulation) OR (child eating behaviors) OR (bite size) OR (eating in the absence of hunger) OR (energy compensation) OR (caloric compensation) OR (food responsiveness) OR (emotional overeating) OR (satiety responsiveness) OR (slowness in eating) OR (emotional eating) OR (external eating) OR (disinhibited eating) OR (satiation) OR (satiety) OR (compensation AND eating). As the focus of the review was on correlations found in the literature, the publication type was limited to original articles, and thus systematic reviews with or without meta-analysis, conceptual articles, case-studies, and dissertations were excluded. We searched for articles published between 2000 and 2021 targeting children 2–12 years old. NM conducted the search in PubMed, which resulted in 20,593 articles. MAP conducted the search in PsycINFO, which resulted in 449 articles. A total of 373 articles in the PubMed search were also found in the PsycINFO search. Relevant articles were also hand-searched to identify any studies that were not included in our search.
Eligibility Criteria
Studies that met all the following criteria were included in the review: (1) study design (cross-sectional study, longitudinal study, randomized controlled trial), (2) population (children ages 2–12 years and/or their caregivers), (3) articles comparing results of at least two assessments that were originally designed to measure healthy ASR, and (4) article type (peer-reviewed publication). Exclusion criteria included: (1) articles focusing on children with eating disorders (e.g., loss of control of eating, binge eating) and/or developmental disorders that may affect appetite regulation (e.g., autism), (2) articles presenting research that was not original (i.e., review articles, conceptual articles, case-studies, and dissertations), (3) articles measuring child ASR constructs that are not typical/healthy (e.g., disinhibited or restrained eating due to dieting or disordered eating), (4) articles presenting data already presented in a previous publication, (5) articles that measured constructs only by a single item on a questionnaire, and (6) language (title, abstract, and/or full text not in English).
Study Selection
MAP and NM independently screened titles and abstracts of the articles identified against the study selection criteria after removal of duplicates. Specifically, MAP reviewed all articles from the PsycINFO search. NM reviewed 10,205 articles from the PubMed search, while MP reviewed the rest of the PubMed search articles. The full text of articles appearing to meet eligibility were then individually reviewed and evaluated for final eligibility by NM and MAP. To ensure quality control, approximately 37% of the articles retrieved were double coded and were in high agreement regarding inclusion or exclusion (k = 0.83). Any disagreements were resolved through discussion and TGP was consulted in the final selection stage. Eighteen articles met the inclusion criteria and are included in this review. The flow chart of the identification and selection of the reviewed articles is presented in Figure 1.
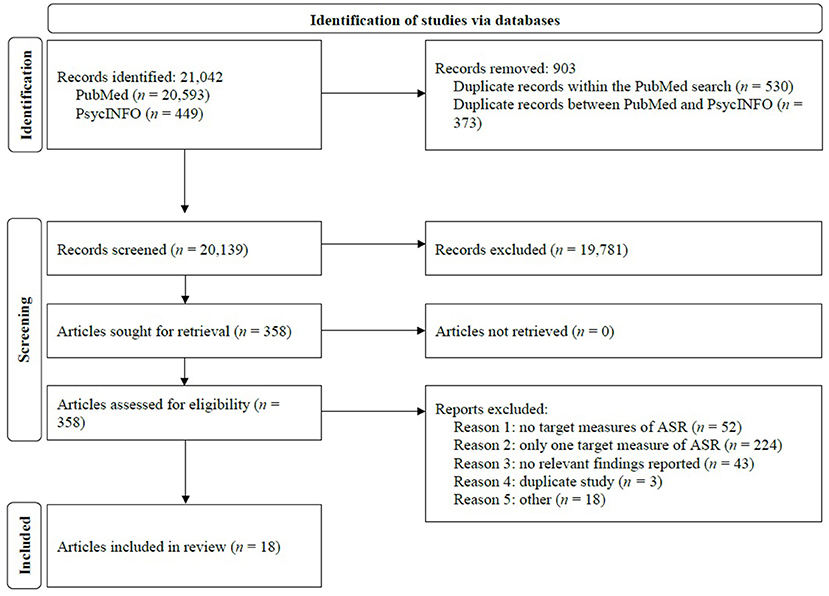
Figure 1. Flow chart of the identification, selection, and inclusion of the retrieved articles.
Data Extraction
A standardized data extraction form was used to gather the following information: (1) author(s) and publication year, (2) sample size, (3) age, (4) ethnicity/location, (5) assessment tools, (6) implementation, and (7) results/selected findings. This information was extracted to a spreadsheet by NM and checked by MP for accuracy. The results of the review are presented as a narrative summary below and in Table 2.
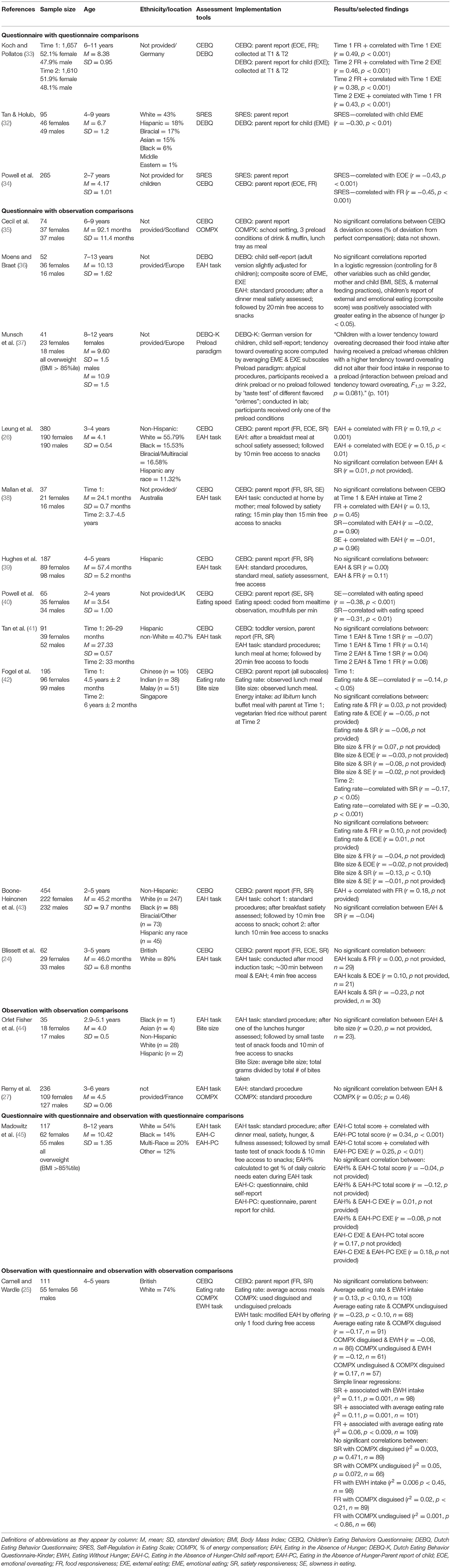
Table 2. Characteristics and selected findings of included studies.
Results
Eighteen studies were eligible for inclusion, representing studies measuring common ASR constructs as assessed by: (1) four unique self-report questionnaires, three of which included multiple versions: CEBQ (two versions: CEBQ and CEBQ for toddlers), DEBQ (three versions: parent-report for child behaviors, modified parent version for child self-report, German version for child self-report), SRES, EAH (parent-report for child behaviors and child self-report); and (2) four unique observational tasks, two of which were implemented slightly differently across studies: compensation trials/preload paradigm, EAH/Eating Without Hunger (EWH) tasks, eating rate/speed, and bite size. Implementation information and deviations from typical procedures are presented in Table 2.
Characteristics of the Included Studies
Table 2 also presents study characteristics and selected findings of the included articles [i.e., author(s) and publication year, sample size, age, ethnicity/location, assessment tools, assessment implementation, and results/selected findings]. Most of the included studies were conducted outside the United States (n = 10), with eight conducted in Europe, one in Australia, and one in Singapore. Seven were conducted within the United States and one did not report location of their subjects. Of the studies conducted outside of the United States, only three reported information on race/ethnicity. Of the studies conducted within the US, most included participants from differing ethnic/racial backgrounds, although the majority was comprised of predominantly White participants. Gender distribution was approximately equal throughout all studies and child ages ranged from 2 to 13 years.
Methodologies Used to Assess ASR Constructs
Of the 18 studies that met eligibility, three studies compared data between different self-report questionnaires: Koch and colleagues (33) compared the CEBQ and the DEBQ; Tan and Holub (32) compared the SRES and the DEBQ; and Powell and colleagues (34) compared the SRES and the CEBQ. Regarding comparisons of questionnaires with observational tasks, nine studies compared the CEBQ with various tasks: compensation trials (35); eating rate/speed (40, 42) and bite size (42); or EAH (24, 26, 38, 39, 41, 43). One study compared the DEBQ (child self-report) with the EAH task (36) and another compared the DEBQ-K (child self-report; German version) with a preload paradigm (37). Three studies compared data between different observational tasks: the EAH was compared to bite size (44) and compensation trials (27); Carnell and Wardle (25) compared the following tasks to each other, compensation trials (disguised and undisguised), eating rate, and EWH. This latter study also compared all observational tasks to the CEBQ. Finally, one study conducted by Madowitz and colleagues (45), using the EAH task and EAH questionnaires (parent- and child-report), compared both versions of the EAH questionnaire to the task as well as to one another.
Inter-relatedness of ASR Constructs
Overall, the majority of significant associations were seen in cohort studies involving multiple self-report questionnaires of ASR. Specifically, in the Koch and colleagues (33) study, food responsiveness (CEBQ) was positively associated with external eating (DEBQ) at the 1st time point of the study (r = 0.49, p < 0.001) and remained significant at the 2nd time point (r = 0.46, p <0.001). Additionally, significant positive associations were found for these constructs across time points with Time 2 food responsiveness correlating positively with external eating at Time 1 (r = 0.38, p <0.001) and Time 2 external eating positively correlating with Time 1 food responsiveness (r = 0.43, p <0.001). Powell and colleagues (34) also found strong associations between subscales of two questionnaires. Child eating self-regulation (SRES) was negatively associated with both emotional overeating (r = −0.43, p <0.001) and food responsiveness (r = −0.45, p <0.001) from the CEBQ. The SRES was also negatively associated with emotional eating from the DEBQ (r = −0.30, p <0.01) in the Tan and Holub (32) study, but the association was moderate.
Most of the 11 studies comparing self-report questionnaires to observational tasks showed either no significant associations (4 studies) (24, 35, 39, 41) or weak and no associations (3 studies) (26, 38, 43). Two of the 11 studies showed moderate associations only between eating rate/speed and CEBQ subscales: negative association with slowness in eating (r = −0.30, p <0.001) (42); and negative association with both slowness in eating and satiety responsiveness (r = −0.38, p <0.001, r = −0.31, p <0.01, respectively) (40). Between the two studies comparing observational tasks to other tasks, none showed significant associations (27, 44).
Carnell and Wardle (25) and Madowitz et al. (45) found some significant moderate associations in their studies that used mixed methods and more than one ASR observational task or self-report questionnaire. Carnell and Wardle (25) showed that satiety responsiveness was positively associated with both EWH and average eating rate (r = 0.33, p = 0.001, r = 0.33, p = 0.01, respectively), and that food responsiveness was also positively associated with average eating rate (r = 0.25, p = 0.009). However, no significant associations were shown between observational tasks. On the other hand, Madowitz and colleagues (45) found significant associations only between the parent- and child-report versions of the same questionnaire (EAH). The total scores of the child self-report were moderately associated with those of the parent-report of child behaviors (r = 0.34, p <0.001), and weakly to moderately associated to the external eating subscale of the parent-report (r = 0.25, p <0.01).
Within the studies comparing ASR questionnaires (32–34, 45), only Madowitz et al. (45) used different raters (i.e., parent and child) for children's behaviors with moderate and weak to moderate associations (r = 0.34, p <0.001, r = 0.25, p <0.01, respectively). The strength of these associations is lower than those found in the other three studies that compared data from the same rater (i.e., parent-report). Moreover, the evidence of association strength in the Madowitz and colleagues (45) study matches the strength of association strength (i.e., moderate) in three studies that compared data from self-report questionnaires and observational tasks (25, 40, 42). On the other hand, the moderate associations were found in these three studies, while the majority of the studies comparing self-report questionnaire with observational task data showed either weak or no significant associations. In contrast, within studies comparing data from several self-report questionnaires, all four studies showed significant associations.
ASR and Child BMIz
Of the 18 studies included in this review, 11 examined associations between at least one measure of ASR constructs and child BMIz or an equivalent score. Most studies used standard methods for calculating child BMIz (e.g., CDC standards) except three studies: weight-for-length z score (WLZ) (41) and similar procedures (35, 37). Henceforth, BMIz will be used to describe child weight status scores. Of the 11 studies, four used self-report questionnaires to measure ASR (32, 33, 36, 37), three used observational tasks (27, 35, 44), and four used both questionnaires and tasks (24, 38, 39, 41).
Among the four studies examining associations between self-report questionnaires and child BMIz, only two studies found associations (32, 33). Emotional overeating and food responsiveness (CEBQ) were positively associated with BMIz (r = 0.17, p <0.001 and r = 0.45, p <0.001, respectively) (33); external eating (DEBQ) was also positively associated with BMIz (r = 0.21, p <0.001) (33). It should be noted that these associations were found in a larger sample [n = 1,657 (33)]. Self-regulation in eating (SRES) was negatively associated with BMIz (r = −0.30, p <0.01) (32). The other two studies which measured external and emotional eating (DEBQ) found no associations (36, 37).
Among the three studies examining associations between observational tasks and child BMIz, only one study found an association—bite size was positively associated with BMIz (r = 0.55, p <0.01) (44). No associations were found between the EAH task (27) or the compensation trials (27, 35) with BMIz.
All four studies that examined associations between both self-report questionnaires and observational tasks with child BMIz, used the CEBQ and the EAH task to measure ASR (24, 38, 39, 41). Of the four studies, three found associations: a negative association with satiety responsiveness [r = −0.42, p = 0.015 (38); r = −0.24, p <0.01 (39); r = −0.28, p <0.01 (41)] was found in all three studies; a positive association with food responsiveness (r = 0.15, p <0.05) (39) was found in one study. The EAH task was associated with BMIz in one of the four studies (r = 0.20, p <0.01) (39).
Discussion
This narrative review was aimed at examining associations between of common child ASR constructs as assessed by at least two methods/measures. The aim was to examine these constructs both within and across self-report questionnaires and/or observational tasks. A total of 18 studies met eligibility criteria and were included in the review. The three studies comparing constructs using self-report questionnaires showed the most correspondence between different ASR constructs. In contrast, the two studies comparing ASR constructs using different observational tasks showed no correspondence. Furthermore, among the 11 studies comparing self-report questionnaires to observational tasks, two studies showed moderate correspondence and nine studies showed weak and/or no associations. As mentioned previously, the remaining two studies compared constructs within and across methodologies and showed weak and/or no associations.
Among the three studies using self-report questionnaires, three questionnaires were used to measure correspondence between constructs—emotional overeating (CEBQ) positively associated with external eating (DEBQ) (33); self-regulation of eating (SRES) negatively associated with emotional eating (DEBQ) (32); and self-regulation of eating (SRES) negatively associated with emotional overeating and food responsiveness (CEBQ) (34). That emotional overeating and external eating were positively associated could be explained by the shared elements of eating without regard to hunger and satiety cues. This correspondence is in line with the construct definitions provided in Table 1. Similarly, the negative association between self-regulation of eating as measured by the SRES and emotional overeating/emotional eating may reflect that responsiveness to internal cues of hunger is diminished by emotional overeating. The negative association found between SRES and food responsiveness could reflect the idea that response to external cues (e.g., sight and smell) and the response to internal cues represent opposite ends of a continuum.
However, the correspondence between these constructs, as measured by self-report questionnaires, could partly be due to method biases that can result when the data is provided by the same source/rater or by the measurement context in which the data was obtained. Apart from the Madowitz and colleagues (45) study, the studies reporting on associations within questionnaires gathered data from the same rater (32–34). When the same source provides data, an “artifactual covariance” can be created between the variables in an effort to create a consistent “story” (or consistency motif) between the rater's cognitions and responses (46). Additionally, the use of the same rater can generate an implicit theory which may “affect attention to and encoding of ratee behaviors as well as later recall” (p. 599) (47). For example, a parent completing questionnaires on their child's eating behaviors may bias their responses based on an overall view they have of their child, which may not necessarily be specific to eating. If a child is difficult, the parent may be biased to create a consistent “story” of their child's eating as being difficult. The measurement context in which the raters provide responses can also be a source of bias. For example, the current mood state of the rater as well as the time of day and location of assessment may impact responses (46). Specifically, a rater's retrieval of information may affect questionnaire completion because of the presence of “common contextual cues” influencing their memory and thus, associations between variables (46).
Among the two studies comparing constructs using only observational tasks (27, 44) and one study that examined constructs within and across methods (25), four assessments tools were used including the eating in the absence of hunger task, various types of compensation trials, and the measurements of eating rate and bite size. Across these different observational tasks, none of the constructs showed correspondence. One reason for the lack of correspondence across observations could stem from the nature of observations—the capture or snapshot of behavior at a single point in time. It is possible that observed data capture state-based behaviors, whereas self-report questionnaire data capture behaviors that parents observe or children engage in across multiple occasions and over an extended period of time—trait-based behaviors.
Among the 11 studies comparing self-report questionnaires and observational tasks of ASR, assessment tools included observations of eating rate, bite size, EAH, and compensation trials as well as the CEBQ (i.e., satiety responsiveness, food responsiveness, slowness in eating, and emotional overeating), and the DEBQ (i.e., emotional and external eating). Two additional studies examining constructs within and across methods also used most of these measures as well as the EAH questionnaire. Of these 13 studies, the most common association found was between eating rate and the CEBQ subscales of satiety responsiveness, food responsiveness, and slowness in eating (25, 40, 42). This common finding may be explained by the simplicity of the eating rate observations. Measuring eating rate can be considered fairly simple, direct, and practical compared to other observational assessments involving multiple steps over a longer period of time. In addition to the eating rate finding, mixed results (weak or no associations) were found across seven studies comparing EAH and the CEBQ subscales (24–26, 38, 39, 41, 43), while no associations were found between compensation trials (25, 35), bite size (44) and the CEBQ subscales, and between the DEBQ and a preload paradigm [a modified form of the compensation trials] (37). Interestingly, neither the parent- nor the child-report of the EAH questionnaire were associated with the EAH task.
Compensation trials did not reveal any significant associations with any ASR measures. One possible reason for this lack of findings is that the percent of compensation shown by children in these tasks usually shows a wide range of values and it is not clear how much of this variation (based on only a single pair of meals) represents stable individual differences in children's ASR vs. variability due to the many situational factors that can affect children's consumption on a single pair of occasions (time of day, child hunger, child mood, child food preferences, etc.). As part of an evaluation of a childhood obesity prevention program, Hughes and colleagues (48) found that although the COMPX scores (i.e., % of energy compensation) showed the expected relationships with child weight status, there was no significant stability in this variable over a 9- to 10-week period in either their prevention or control groups. This suggests that although this variable may be useful in the comparison of groups of children, a single pair of meals may not be sufficient to yield stable measure of individual differences in ASR. Additionally, the lack of findings with the EAH task, may stem from socialization influences that could be affecting children's behaviors during this task. Hughes and colleagues (48) have suggested that tasks, such as compensation trials and EAH, may not be effective measures of ASR with certain samples (i.e., Hispanic children from low-income backgrounds) for various reasons. For example, it is highly likely that these children experience high food insecurity at home, or the foods provided during the tasks are unfamiliar or not culturally congruent to the children. Moreover, children show wide variability in their responses to the EAH task, and individual differences may reflect both situational factors as well as individual differences in ASR. In the Hughes and colleagues (48) study, however, significant stability was shown over a 9- to 10-week period in both the prevention (r = 0.50) and control (r = 0.32) groups.
The lack of associations between ASR constructs as measured by self-report questionnaires and observational tasks has been shown in studies of adults as well (49). Interestingly, similar to the findings from this narrative review, Creswell et al. (49) found that associations between self-report questionnaires and observed computerized tasks were either weak or non-significant. Additionally, the self-report questionnaires showed associations with outcomes, whereas the computerized tasks showed weak or no associations with outcomes. This is in line with findings from the current review showing significant associations between ASR constructs and child weight outcomes across five studies using self-report questionnaires. Specifically, these studies showed significant associations between ASR constructs and child BMIz across five studies using self-report questionnaires. Specifically, satiety responsiveness, food responsiveness, and emotional overeating from the CEBQ (33, 38, 39, 41), external eating from the DEBQ (33), and child self-regulation in eating (32) were associated with child BMIz. In contrast, only two studies showed significant associations with child BMIz using observational tasks (39, 44). The findings from this review are consistent with a recent systematic review of the CEBQ subscales and child weight (50). Among studies comparing observational tasks and child BMIz, only two constructs showed associations—bite size (44) and EAH (39). Interestingly, EAH was associated with child BMIz in only one (39) of five studies (24, 27, 41, 44), despite the fact that EAH has consistently been shown to be associated with child weight status (51). These associations were specific to studies that involved more than one ASR measure and constitutes a small subset of studies looking at associations of ASR measures with weight status. The association found by Hughes et al. (39) is consistent with previous reports among these constructs in young children (51).
Findings from this narrative review should be considered in light of its limitations. Inclusion in his review required that each study assessed at least two ASR measures and reported associations. Furthermore, although many factors impact ASR in children, including biopsychological (e.g., genes, hormones, executive functioning) and family and community processes (7, 21), the current review focused on the intrapersonal factors of common ASR constructs. Moreover, only a subset of published articles (i.e., the 18 included in this review) reported associations between the measured ASR constructs with over 40 identified that did not present associations. This limits the interpretation of the findings, because if more data were available, the relationship between the targeted measures may have presented differently.
Future Research and Implications
It is thought that questionnaire-based measures have clear advantages over observational tasks for a number of reasons. Specifically, questionnaires (1) involve little participant burden for young children as parents often report on child behaviors, (2) present relatively low participant burden for parents, and (3) are more feasible to administer compared to many observational protocols that involve multiple steps administered by trained research staff. In this sense, questionnaires have obvious advantages for measurement in large epidemiological studies and interventions as well as for rapid identification of at-risk children in healthcare settings.
Future research is needed to more clearly define the various ASR constructs, their expected correspondence, as well as the strength of that correspondence. Additionally, as other scholars have suggested, current literature would benefit from studies considering the biology of the child as well as the child's immediate and more distal environments (7). The use of mixed methods comprised of existing tools, as well as conducting the same assessments over a shorter period of time (e.g., across 10 days) will better determine whether these constructs measure a state vs. a trait. Longitudinal research will provide evidence of predictability. Taken together, this additional information and identifying which ASR constructs are most effective can inform efforts toward successful childhood obesity programs that promote healthful eating behaviors in families. Further, investigating the relations between ASR constructs and child weight, among youth with and without overweight/obesity and their parents, fosters a better understanding for predicting obesity risk in children.
Author Contributions
MP, SH, TP, and JF contributed to conception and design of the review. MP and NM conducted the article search and review and organized the database. TP approved the final list of articles. MP wrote the first draft of the manuscript. SH, TP, and JF wrote sections of the manuscript. All authors contributed to the revision of the manuscript and read and approved the submitted version.
Funding
This work is a publication of the United States Department of Agriculture (USDA/ARS) Children's Nutrition Research Center, Department of Pediatrics, Baylor College of Medicine (Houston, TX) funded in part by the USDA/ARS (Cooperative Agreement 58-3092-0-001).
Author Disclaimer
The contents of this publication do not necessarily reflect the views or policies of the USDA, nor does mention of trade names, commercial products, or organizations imply endorsement from the US government.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Hayes JF, Eichen DM, Barch DM, Wilfley DE. Executive function in childhood obesity: promising intervention strategies to optimize treatment outcomes. Appetite. (2018) 124:10–23. doi: 10.1016/j.appet.2017.05.040
2. Hughes SO, Power TG, Beck A, Betz D, Calodich S, Goodell LS, et al. Strategies for effective eating development-SEEDS: design of an obesity prevention program to promote healthy food preferences and eating self-regulation in children from low-income families. J Nutr Educ Behav. (2016) 48:405–18. doi: 10.1016/j.jneb.2016.04.388
3. Miller AL, Gearhardt AN, Fredericks EM, Katz B, Shapiro LF, Holden K, et al. Targeting self-regulation to promote health behaviors in children. Behav Res Ther. (2018) 101:71–81. doi: 10.1016/j.brat.2017.09.008
4. Miller AL, Horodynski MA, Herb HEB, Peterson KE, Contreras D, Kaciroti N, et al. Enhancing self-regulation as a strategy for obesity prevention in head start preschoolers: the growing healthy study. BMC Public Health. (2012) 12:1040. doi: 10.1186/1471-2458-12-1040
5. Russell CG, Russell A. “Food” and “non-food” self-regulation in childhood: a review and reciprocal analysis. Int J Behav Nutr Phys Act. (2020) 17:33. doi: 10.1186/s12966-020-00928-5
6. van der Veek SMC, de Graaf C, de Vries JHM, Jager G, Vereijken C, Weenen H, et al. Baby's first bites: a randomized controlled trial to assess the effects of vegetable-exposure and sensitive feeding on vegetable acceptance, eating behavior and weight gain in infants and toddlers. BMC Pediatr. (2019) 19:266. doi: 10.1186/s12887-019-1627-z
7. Russell A, Russell CG. Appetite self-regulation declines across childhood while general self-regulation improves: a narrative review of the origins and development of appetite self-regulation. Appetite. (2021) 162:105178. doi: 10.1016/j.appet.2021.105178
8. Carnell S, Benson L, Pryor K, Driggin E. Appetitive traits from infancy to adolescence: using behavioral and neural measures to investigate obesity risk. Physiol Behav. (2013) 121:79–88. doi: 10.1016/j.physbeh.2013.02.015
9. Kral TVE, Moore RH, Chittams J, Jones E, O'Malley L, Fisher JO. Identifying behavioral phenotypes for childhood obesity. Appetite. (2018) 127:87–96. doi: 10.1016/j.appet.2018.04.021
10. Birch LL, Deysher M. Conditioned and unconditioned caloric compensation: evidence for self-regulation of food intake in young children. Learn Motiv. (1985) 16:341–55. doi: 10.1016/0023-9690(85)90020-7
11. Birch LL, Deysher M. Caloric compensation and sensory specific satiety: evidence for self regulation of food intake by young children. Appetite. (1986) 7:323–31. doi: 10.1016/S0195-6663(86)80001-0
12. Fisher JO, Birch LL. Restricting access to palatable foods affects children's behavioral response, food selection, and intake. Am J Clin Nutr. (1999) 69:1264–72. doi: 10.1093/ajcn/69.6.1264
13. Blundell JE, Bellisle F. Satiation, Satiety and the Control of Food Intake: Theory and Practice. Cambridge: Woodhead Publishing Ltd (2013).
14. Zijlstra N, de Wijk RA, Mars M, Stafleu A, de Graaf C. Effect of bite size and oral processing time of a semisolid food on satiation. Am J Clin Nutr. (2009) 90:269–75. doi: 10.3945/ajcn.2009.27694
15. Wardle J, Guthrie CA, Sanderson S, Rapoport L. Development of the children's eating behaviour questionnaire. J Child Psychol Psychiatry. (2001) 42:963–70. doi: 10.1111/1469-7610.00792
16. Braet C, Van Strien T. Assessment of emotional, externally induced and restrained eating behaviour in nine to twelve-year-old obese and non-obese children. Behav Res Ther. (1997) 35:863–73. doi: 10.1016/S0005-7967(97)00045-4
17. van Strien T, Oosterveld P. The children's DEBQ for assessment of restrained, emotional, and external eating in 7- to 12-year-old children. Int J Eat Disord. (2008) 41:72–81. doi: 10.1002/eat.20424
18. Shomaker LB, Tanofsky-Kraff M, Elliott C, Wolkoff LE, Columbo KM, Ranzenhofer LM, et al. Salience of loss of control for pediatric binge episodes: does size really matter? Int J Eat Disord. (2010) 43:707–16. doi: 10.1002/eat.20767
19. Tanofsky-Kraff M, Ranzenhofer LM, Yanovski SZ, Schvey NA, Faith M, Gustafson J, et al. Psychometric properties of a new questionnaire to assess eating in the absence of hunger in children and adolescents. Appetite. (2008) 51:148–55. doi: 10.1016/j.appet.2008.01.001
20. Tan CC, Holub SC. Children's self-regulation in eating: associations with inhibitory control and parents' feeding behavior. J Pediatr Psychol. (2011) 36:340–5. doi: 10.1093/jpepsy/jsq089
21. Faith MS, Carnell S, Kral TVE. Genetics of food intake self-regulation in childhood: literature review and research opportunities. Human Heredity. (2013) 75:80–9. doi: 10.1159/000353879
22. Carnell S, Wardle J. Appetitive traits and child obesity: measurement, origins and implications for intervention. Proc Nutr Soc. (2008) 67:343–55. doi: 10.1017/S0029665108008641
23. Carnell S, Wardle J. Appetitive traits in children. New evidence for associations with weight and a common, obesity-associated genetic variant. Appetite. (2009) 53:260–3. doi: 10.1016/j.appet.2009.07.014
24. Blissett J, Farrow C, Haycraft E. Relationships between observations and parental reports of 3-5 year old children's emotional eating using the children's eating behaviour questionnaire. Appetite. (2019) 141:104323. doi: 10.1016/j.appet.2019.104323
25. Carnell S, Wardle J. Measuring behavioural susceptibility to obesity: validation of the child eating behaviour questionnaire. Appetite. (2007) 48:104–13. doi: 10.1016/j.appet.2006.07.075
26. Leung CY, Lumeng JC, Kaciroti NA, Chen YP, Rosenblum K, Miller AL. Surgency and negative affectivity, but not effortful control, are uniquely associated with obesogenic eating behaviors among low-income preschoolers. Appetite. (2014) 78:139–46. doi: 10.1016/j.appet.2014.03.025
27. Remy E, Issanchou S, Chabanet C, Boggio V, Nicklaus S. Impact of adiposity, age, sex and maternal feeding practices on eating in the absence of hunger and caloric compensation in preschool children. Int J Obes. (2015) 39:925–30. doi: 10.1038/ijo.2015.30
28. Ek A, Sorjonen K, Eli K, Lindberg L, Nyman J, Marcus C, et al. Associations between parental concerns about preschoolers' weight and eating and parental feeding practices: results from analyses of the child eating behavior questionnaire, the child feeding questionnaire, and the lifestyle behavior checklist. PLoS ONE. (2016) 11:e0147257. doi: 10.1371/journal.pone.0147257
29. Van Strien T, Frijters JE, Bergers GP, Defares PB. The dutch eating behavior questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behavior. Int J Eat Disord. (1986) 5:295–315. doi: 10.1002/1098-108X(198602)5:2<295::AID-EAT2260050209>3.0.CO;2-T
30. Fisher JO, Birch LL. Eating in the absence of hunger and overweight in girls from 5 to 7 y of age. Am J Clin Nutr. (2002) 76:226–31. doi: 10.1093/ajcn/76.1.226
31. Blundell J, de Graaf C, Hulshof T, Jebb S, Livingstone B, Lluch A, et al. Appetite control: methodological aspects of the evaluation of foods. Obes Rev. (2010) 11:251–70. doi: 10.1111/j.1467-789X.2010.00714.x
32. Tan CC, Holub SC. Emotion regulation feeding practices link parents' emotional eating to children's emotional eating: a moderated mediation study. J Pediatr Psychol. (2015) 40:657–63. doi: 10.1093/jpepsy/jsv015
33. Koch A, Pollatos O. Interoceptive sensitivity, body weight and eating behavior in children: a prospective study. Front Psychol. (2014) 5:1003. doi: 10.3389/fpsyg.2014.01003
34. Powell EM, Frankel LA, Umemura T, Hazen N. The relationship between adult attachment orientation and child self-regulation in eating: the mediating role of persuasive-controlling feeding practices. Eat Behav. (2017) 26:121–8. doi: 10.1016/j.eatbeh.2017.02.006
35. Cecil JE, Palmer CN, Wrieden W, Murrie I, Bolton-Smith C, Watt P, et al. Energy intakes of children after preloads: adjustment, not compensation. Am J Clin Nutr. (2005) 82:302–8. doi: 10.1093/ajcn/82.2.302
36. Moens E, Braet C. Predictors of disinhibited eating in children with and without overweight. Behav Res Ther. (2007) 45:1357–68. doi: 10.1016/j.brat.2006.10.001
37. Munsch S, Hasenboehler K, Michael T, Meyer AH, Roth B, Biedert E, et al. Restrained eating in overweight children: does eating style run in families? Int J Pediatr Obes. (2007) 2:97–103. doi: 10.1080/17477160701369191
38. Mallan KM, Nambiar S, Magarey AM, Daniels LA. Satiety responsiveness in toddlerhood predicts energy intake and weight status at four years of age. Appetite. (2014) 74:79–85. doi: 10.1016/j.appet.2013.12.001
39. Hughes SO, Power TG, O'Connor TM, Orlet Fisher J. Executive functioning, emotion regulation, eating self-regulation, and weight status in low-income preschool children: how do they relate? Appetite. (2015) 89:1–9. doi: 10.1016/j.appet.2015.01.009
40. Powell F, Farrow C, Meyer C, Haycraft E. The stability and continuity of maternally reported and observed child eating behaviours and feeding practices across early childhood. Int J Environ Res Public Health. (2018) 15:1017. doi: 10.3390/ijerph15051017
41. Tan CC, Walczak M, Roach E, Lumeng JC, Miller AL. Longitudinal associations between eating and drinking engagement during mealtime and eating in the absence of hunger in low income toddlers. Appetite. (2018) 130:29–34. doi: 10.1016/j.appet.2018.07.029
42. Fogel A, Fries LR, McCrickerd K, Goh AT, Quah PL, Chan MJ, et al. Oral processing behaviours that promote children's energy intake are associated with parent-reported appetitive traits: results from the GUSTO cohort. Appetite. (2018) 126:8–15. doi: 10.1016/j.appet.2018.03.011
43. Boone-Heinonen J, Weeks HM, Sturza J, Miller AL, Lumeng JC, Bauer KW. Prenatal predictors of objectively measured appetite regulation in low-income toddlers and preschool-age children. Pediatr Obes. (2019) 14:e12554. doi: 10.1111/ijpo.12554
44. Orlet Fisher J, Rolls BJ, Birch LL. Children's bite size and intake of an entrée are greater with large portions than with age-appropriate or self-selected portions. Am J Clin Nutr. (2003) 77:1164–70. doi: 10.1093/ajcn/77.5.1164
45. Madowitz J, Liang J, Peterson CB, Rydell S, Zucker NL, Tanofsky-Kraff M, et al. Concurrent and convergent validity of the eating in the absence of hunger questionnaire and behavioral paradigm in overweight children. Int J Eat Disord. (2014) 47:287–95. doi: 10.1002/eat.22213
46. Podsakoff PM, MacKenzie SB, Lee JY, Podsakoff NP. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. (2003) 88:879–903. doi: 10.1037/0021-9010.88.5.879
47. Smither JW, Buda R, Collins H. When ratee satisfaction influences performance evaluations: a case of illusory correlation. J Appl Psychol. (1989) 74:599. doi: 10.1037/0021-9010.74.4.599
48. Hughes SO, Power TG, Beck A, Betz D, Goodell LS, Hopwood V, et al. Short-term effects of an obesity prevention program among low-income hispanic families with preschoolers. J Nutr Educ Behav. (2020) 52:224–39. doi: 10.1016/j.jneb.2019.12.001
49. Creswell KG, Wright AGC, Flory JD, Skrzynski CJ, Manuck SB. Multidimensional assessment of impulsivity-related measures in relation to externalizing behaviors. Psychol Med. (2019) 49:1678–90. doi: 10.1017/S0033291718002295
50. Kininmonth A, Smith A, Carnell S, Steinsbekk S, Fildes A, Llewellyn C. The association between childhood adiposity and appetite assessed using the child eating behavior questionnaire and baby eating behavior questionnaire: a systematic review and meta-analysis. Obes Rev. (2021) 22:e13169. doi: 10.1111/obr.13169
Keywords: appetite self-regulation, children, methodology, observational tasks, questionnaires, self-report
Citation: Papaioannou MA, Micheli N, Power TG, Fisher JO and Hughes SO (2022) Associations Between Independent Assessments of Child Appetite Self-Regulation: A Narrative Review. Front. Nutr. 8:810912. doi: 10.3389/fnut.2021.810912
Received: 08 November 2021; Accepted: 22 December 2021;
Published: 27 January 2022.
Edited by:
Alan Russell, Flinders University, AustraliaReviewed by:
Ashley Nicole Gearhardt, University of Michigan, United StatesAnne Claire Grammer, Washington University School of Medicine in St. Louis, United States
Copyright © 2022 Papaioannou, Micheli, Power, Fisher and Hughes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sheryl O. Hughes, shughes@bcm.edu