
Application of artificial intelligence for the classification of the clinical outcome and therapy in patients with viral infections: The case of COVID-19
Abstract
BACKGROUND:
With the end of the coronavirus disease 2019 (COVID-19) pandemic, it becomes intriguing to observe the impact of innovative digital technologies on the diagnosis and management of diseases, in order to improve clinical outcomes for patients.
OBJECTIVE:
The research aims to enhance diagnostics, prediction, and personalized treatment for patients across three classes of clinical severity (mild, moderate, and severe). What sets this study apart is its innovative approach, wherein classification extends beyond mere disease presence, encompassing the classification of disease severity. This novel perspective lays the foundation for a crucial decision support system during patient triage.
METHODS:
An artificial neural network, as a deep learning technique, enabled the development of a complex model based on the analysis of data collected during the process of diagnosing and treating 1000 patients at the Tešanj General Hospital, Bosnia and Herzegovina.
RESULTS:
The final model achieved a classification accuracy of 82.4% on the validation data set, which testifies to the successful application of the artificial neural network in the classification of clinical outcomes and therapy in patients infected with viral infections.
CONCLUSION:
The results obtained show that expert systems are valuable tools for decision support in healthcare in communities with limited resources and increased demands. The research has the potential to improve patient care for future epidemics and pandemics.
1.Introduction
Originating in Wuhan, China, the severe acute respiratory syndrome caused by the SARS-CoV-2, a member of the coronavirus family, swiftly emerged as the novel coronavirus disease 2019 (COVID-19). Its rapid global transmission has profoundly impacted the daily lives of billions of individuals worldwide. The World Health Organization reported that COVID-19 primarily resulted in mild respiratory disease with little or no pneumonia, affecting approximately 80% of cases. Roughly 14% of cases resulted in severe disease with dyspnea or hypoxia, and around 5% of cases resulted in severe respiratory disease with various complications [1]. Pulmonary fibrosis, a severe and potentially permanent damage to the lungs, was a risk associated with SARS-CoV-2 infection, possibly resulting in deterioration of the patient’s condition, with the potential for serious acute respiratory distress syndrome (ARDS) and disseminated intravascular coagulation [2, 3, 4]. Based on the three disease stages and radiological criteria, the US National Institutes of Health (NIH) developed a categorization system with five clinical stages for COVID-19 [5, 6], as shown in Table 1.
The severity of the pandemic has resulted in substantial challenges within healthcare systems across various countries [7]. It was shown that late or delayed detection of COVID-19 resulted in severe complications that increased the duration of hospitalization, overburdened the healthcare system, and had higher probability to lead to fatalities. In May 2023, the World Health Organization (WHO) declared the COVID-19 pandemic over [8], and with this it became intriguing to observe the influence of innovative digital technologies on the diagnosis and management of diseases. Based on the experience gained through the COVID-19, the need for enhanced diagnostics, prediction, and personalized treatment for patients is emphasized. Special attention should be focused to the decision support systems during patient triage, especially during these epidemic/pandemic situations.
In the 21st century, access to the internet and novel technologies such as artificial intelligence (AI) represent a new stage and inevitable trend of medical development [9]. The rapid progress in high-performance computing (HPC) and high-performance data analytics (HPDA), in conjunction with AI (collectively known as HPC
Even though the emergence of the COVID-19 pandemic excelled the innovation and use of technologies to effectively respond to the crisis and mitigate the challenges arising from healthcare systems and financial burdens [13], there was a significant challenge in distinguishing the initial clinical progression of COVID-19 infection from other medical conditions [14, 15].
Table 1
| Stage | Description |
|---|---|
| Asymptomatic or pre- | Patients are diagnosed with SARS-CoV-2 but have no symptoms, and they can still spread the virus |
| symptomatic infection | |
| Mild disease | Patient experiences mild symptoms but has no breathing difficulties or noticeable radiological changes |
| Moderate disease | Patient’s blood oxygen saturation level, as detected by an oximeter, is equal to or greater than 94%, and there is evidence of clinical or radiological pneumonia |
| Severe disease | Patient’s blood oxygen saturation level is less than 94% |
| Critical illness | Patient experiences respiratory failure, septic shock, and/or failure of one or more organs |
Standard procedures upon admission typically involved conducting a chest x-ray and performing blood tests, including a complete and differential blood count, inflammatory markers, and blood gas analysis. In routine admission procedures, AI has been used to differentiate between different forms of pneumonia using the Expert Diagnostic System [16, 17, 18], such as for tracing epidemiological peaks, the prediction of its diffusion and the effects of restrictive measures, X-ray and CT image recognition [19, 20, 21, 22].
In recent years, there has been notable advancement in artificial intelligence, particularly in the development of predictive machine learning models for medical applications. Among these, deep learning stands out as a prominent technique within machine learning, characterized by intricate structures inspired by artificial neural networks (ANNs) [23]. Its capabilities hold the promise of substantially improving the efficiency of the current medical and healthcare systems amid the COVID-19 pandemic [24, 25].
The COVID-19 crisis in Bosnia and Herzegovina has been characterized by one of the highest mortality rates in Europe, and even worldwide [26]. The healthcare system was strained and faced difficulties in providing adequate care and support to the affected population. The shortage of medical personnel, equipment, and hospital beds posed significant challenges in managing the influx of COVID-19 cases. This has revealed structural weaknesses and deficiencies in the healthcare system, highlighting the necessity for improvement. The application of AI in the healthcare sector in Bosnia and Herzegovina will become increasingly important, considering that our society is aging and the country is facing a potential shortage of healthcare professionals due to increased migration of young, working-age individuals. As the global landscape advanced in the wake of the COVID-19 pandemics, the imperative to cultivate innovation and proactively equip ourselves against potential future pandemics remains resolute. Evidently, discerning the nuances of disease severity during the critical phase of patient triage exerted a profound influence on patient recuperation. Thus, the exigency for the decision support systems remains unabating. The ability to recognize earlier indicators of deterioration enables timely intervention, reduces the need for more intensive treatments and improves the outcome of treatment [27].
Motivated by a tremendous challenge in differentiating in COVID-19 disease stages in a patient especially, an early clinical course of the COVID-19 infection from other medical presentations especially between asymptomatic, mild and moderate disease stages collaboration between researchers, clinicians and pharmaceutical experts was established.
The aim of the research was to design a clinical decision-making system (eDSS) that can classify the severity of clinical conditions and identify the most appropriate treatment regimen for patients with infection of COVID-19. Our research goes beyond the conventional binary approach to encompass disease severity. This holds immense potential for improving patient care and optimizing resource allocation. By providing a comprehensive decision support system tailored for triage, we bridge the gap between disease classification and patient-centered care, ultimately enhancing the overall quality of healthcare delivery.
2.Methods
A connectivism approach was used in this research. The research was done in two parts, first concerning data collection and preprocessing and the second system development.
For the development of the artificial intelligence based clinical decision-making system, an interdisciplinary team used raw data collected at the General Hospital Tešanj from June 2020 to June 2021. Data collection was carried out according to prior established medical protocol in General Hospital Tešanj. The study was approved by the institutional board and written informed consent was obtained from each study participant or patient’s legal guardian before enrollment. Upon admission and based on epidemiological guidelines and protocols, patients were evaluated for COVID-19 using SARS-CoV-2 PCR or polymerase chain reaction in pharyngeal swabs and underwent radiological imaging. Within 48 hours, PCR results were collected that had no impact on admission treatment, considering the conclusions from the literature, which confirm that it often happens that patients have clear symptoms of COVID-19 at the time of data collection, even though their PCR tests are negative.
The standard of care was followed for the examination, diagnosis, and treatment of all patients who had been involved, including laboratory blood cell counts and clinical chemistry evaluations. The methodology for the AI system development included analysis of medical data in its original form, defining technical specifications of a system, training and validation and performance measurement.
2.1Dataset
Total of 1000 samples were made available for the development of AI based decision support system-eDSS that can classify between three classes of the severity of clinical conditions (mild, moderate and severe) of viral infection of COVID-19.
Among a total of 1000 samples, 99 were deemed incomplete and subsequently excluded. The detailed information about the dataset is shown in Table 2.
Table 2
Dataset overview
| Total | 901 | Age [Years] | Count | Age [Years] | Count |
| 15–30 | 43 | 50–60 | 154 | ||
| Male (M) | 508 (56.38%) | 30–40 | 44 | 60–70 | 272 |
| Female (F) | 393 (43.61%) | 40–50 | 94 | 70–80 | 225 |
| 80–90 | 69 | ||||
| Condition (Disease severity category) | Mild | 36% of the dataset | |||
| Moderate | 36% of the dataset | ||||
| Severe | 28% of the dataset | ||||
Every data sample consisted of the 3 group of parameters:
1. General patient information: age and gender.
2. Laboratory values from biological material (whole blood and serum) were measured as standard of care at the time of admission to the General Hospital Tešanj, including following parameters: erythrocyte sedimentation (SE), blood count-red blood cells (RBC), white blood cells (WBC), hemoglobin (Hb), mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), mean corpuscular Hb concentration (MCHC); clinical biochemical analysis: C-reactive protein (CRP), alanine aminotransferase (ALT), aspartate aminotransferase (AST), lactate dehydrogenase (LDH), lipase, creatine kinase (CK), international normalized ratio (INR), partial thromboplastin time (aPTT), D-dimer, Sodium (Na), potassium (K), Glucose, Creatitin, blood urea (Urea), Uric acid, total proteins, Albumins, Globulins. Analysis of specific inflammatory markers-Interleukin-6, Interleukin-1
3. Disease outcome information: According to WHO guidelines medical professionals at General Hospital Tešanj grouped patients in three categories according to the severity of the clinical picture.
The data set used for the development of the expert system consisted of 901 samples with 43 monitored parameters. In order to further strengthen the selection process, the selection of parameters was carried out carefully taking into account their significant impact on the clinical picture of the patient, and according to the suggestions of experts from Tešanj General Hospital. As can be seen from Table 2, the set of data used to create the expert system had a balanced representation of all categories.
2.2Data processing
During the data preprocessing, feature selection was performed in order to determine the relevance of laboratory parameters for diagnosis of disease severity category. Data preprocessing is a crucial step that ensures that the input data is in a suitable form for further analysis and processing, leading to reliable and useful results in various fields of research and application. Pearson correlation coefficients were calculated in this step. Pearson’s correlation coefficient can help identify the features that are most related to the target variable. If the coefficient is close to 1, it means that there is a strong positive linear correlation between the feature and the target variable, while a coefficient close to
Some of the laboratory parameters did not show relevant correlation with the disease progression, even though this was expected for COVID-19 hallmark parameters such as D-dimer and CRP. Hence, advanced data preprocessing was performed using principal component analysis (PCA), an unsupervised machine learning algorithm commonly used to extract value from previously uncorrelated data and extracting the most important features.
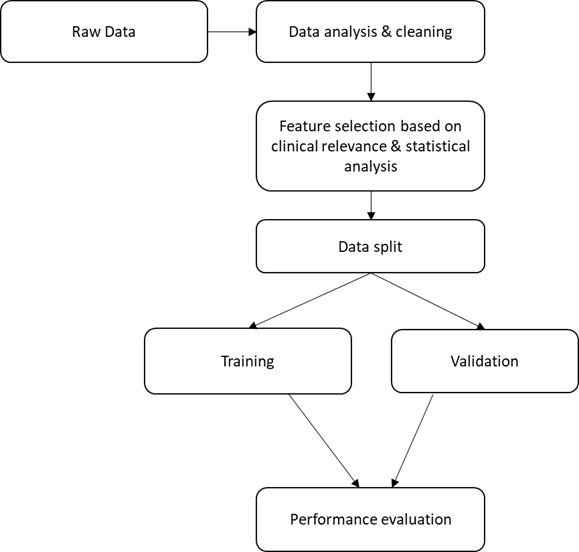
Prior to the development of the expert system, the data was divided into training and validation datasets (Fig. 1). Conventionally, an 80:20 ratio is used, however, due to the scarcity of the data, 90:10 division of the dataset for training and validation respectively was used [17]. This adaptation enabled better management of limited data resources and the achievement of adequate model evaluation and testing.
Figure 1.
A workflow of all major steps taken in this work. Initially raw data was cleaned i.e., to deal with missing data and analyse outliers. Statistical analysis was performed to evaluate possible heterogeneity characteristics and variable distribution between patient groups. Initial feature selection on the clean dataset was completed before data splitting. Finally, performance of the models on the data was evaluated using several metrics recommended by the literature.
2.3Development of an expert system based on artificial intelligence
The expert system was developed using the Python programming language and keras library. This research used a special type of neural network, known as an ANN, due to its ability to process complex medical data. The ANN developed in this research is a feed-forward network. The basic architecture of ANN consists of connected collections of neurons organized in three layers: input, hidden, and output. The input layer is the first layer in the developed neural network and represents the point at which data is introduced into the network. Each neuron in the input layer represents one characteristic (attribute) of the input data. The number of input neurons is 43. The input neurons send their values further to the hidden layer, where the data is processed and transformed. This is the key part of ANN where data processing and transformation takes place in order to learn the appropriate shapes and patterns. Finally, the neural network developed in this research has two hidden layers. The first hidden layer consists of 20 neurons and uses hyperbolic tangents (tanh) as activation function, while the second hidden layer has 50 neurons and uses the same activation function.
The number of neurons in the hidden layers was varied during the training process to achieve the optimal performance of the neural network, while the number of neurons in the output layer was kept at 3 due to the number of different classes (mild, moderate and severe) predicted by the model. The output layer represents the last layer in the ANN, which generates the final results based on data processing through the hidden layer. The values that the output neurons generate represent the predictions or results that the ANN gives for the input data set.
Figure 2.
System training phase
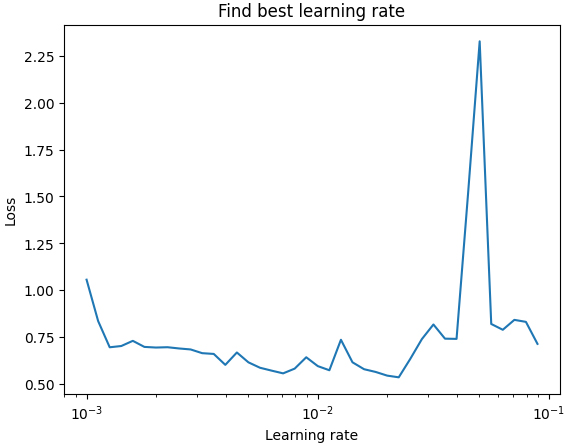
During development of ANN an optimizer was used. This is extremely important in ANNs because they play a key role in achieving the optimal weight parameters of the neural network during the training process. The optimizers were used to provide faster convergence to the global minimum of function loss, avoidance of local minima, improved performance and training. Optimizer used in this research was Adam optimizer (Adaptive Moment Estimation) was used as an algorithm for training the neural network (Fig. 2).
Table 3
Categorical variables count across classes
| MILD | MODERATE | SEVERE | |||||||
|---|---|---|---|---|---|---|---|---|---|
| MEAN | Standard deviation | MEDIAN | MEAN | Standard deviation | MEDIAN | MEAN | Standard deviation | MEDIAN | |
| LE WBC | 1.051 | 0.311 | 1.000 | 1.092 | 0.409 | 1.000 | 1.089 | 0.353 | 1.000 |
| Limf% | 17.378 | 10.621 | 1.000 | 16.122 | 12.553 | 16.000 | 13.123 | 7.204 | 16.700 |
| Mid% | 6.723 | 2.767 | 13.000 | 6.694 | 2.624 | 6.700 | 5.646 | 2.686 | 6.800 |
| Gran% | 70.685 | 12.745 | 5.500 | 73.904 | 10.546 | 77.600 | 78.716 | 7.865 | 75.450 |
| HGB | 134.829 | 18.017 | 80.600 | 130.864 | 15.819 | 134.000 | 130.210 | 19.736 | 138.500 |
| ER RBC | 4.535 | 40.112 | 134.000 | 4.283 | 0.478 | 4.330 | 4.227 | 0.616 | 4.460 |
| HCT | 38.502 | 5.136 | 4.310 | 37.614 | 4.544 | 38.200 | 37.201 | 5.501 | 38.900 |
| MCV | 87.567 | 4.738 | 38.000 | 87.939 | 5.817 | 88.500 | 88.130 | 6.552 | 87.600 |
| TR PLT | 194.331 | 91.276 | 88.800 | 187.257 | 86.099 | 190.000 | 166.688 | 83.798 | 194.000 |
| SE | 47.064 | 38.991 | 166.000 | 64.669 | 37.130 | 70.000 | 62.250 | 37.616 | 60.000 |
| INR | 1.100 | 0.843 | 65.000 | 1.133 | 0.348 | 1.090 | 1.138 | 1.074 | 1.040 |
| APTT | 27.936 | 6.959 | 1.080 | 27.510 | 4.594 | 28.000 | 27.967 | 4.941 | 28.000 |
| D DIMER | 884.249 | 1381.966 | 28.000 | 1221.242 | 1781.446 | 1136.070 | 1409.614 | 1854.959 | 817.460 |
| GLUCOSE | 7.191 | 3.648 | 1294.190 | 8.017 | 4.731 | 7.100 | 8.726 | 5.642 | 6.700 |
| UREA | 6.636 | 3.590 | 8.100 | 7.857 | 4.920 | 7.400 | 8.420 | 5.729 | 6.450 |
| CREATININE | 89.179 | 45.498 | 7.800 | 94.770 | 40.523 | 89.000 | 107.333 | 53.248 | 87.000 |
| AC URICUM | 251.277 | 114.885 | 99.000 | 286.174 | 162.491 | 286.000 | 312.780 | 168.492 | 257.500 |
| AST | 33.122 | 54.463 | 307.000 | 35.280 | 44.404 | 36.000 | 50.082 | 121.183 | 31.500 |
| ALT | 33.467 | 58.374 | 49.000 | 33.117 | 49.864 | 32.000 | 64.800 | 87.703 | 30.000 |
| LDH | 1.507 | 0.593 | 40.000 | 1.778 | 0.636 | 2.000 | 2.027 | 0.630 | 2.000 |
| CK | 1.287 | 0.707 | 2.000 | 1.334 | 0.723 | 1.000 | 1.482 | 0.774 | 1.000 |
| POTASSIUM | 4.215 | 0.556 | 1.000 | 4.269 | 0.638 | 4.300 | 4.251 | 0.687 | 4.300 |
| SODIUM | 139.003 | 11.070 | 4.300 | 138.734 | 10.956 | 141.000 | 136.733 | 11.815 | 142.000 |
| TOTAL PROTEIN | 69.829 | 6.999 | 140.000 | 68.732 | 6.496 | 68.700 | 66.689 | 8.500 | 70.700 |
| ALBUMINES | 43.282 | 4.704 | 67.600 | 41.051 | 3.974 | 41.400 | 40.066 | 5.646 | 44.100 |
| CRP | 1.598 | 0.754 | 41.500 | 2.005 | 0.785 | 2.000 | 2.230 | 0.706 | 2.000 |
| pH | 19.555 | 2586.165 | 2.000 | 33.234 | 3071.006 | 7.404 | 21.541 | 2696.271 | 7.381 |
| pCO2 | 32.502 | 24.603 | 7.388 | 30.543 | 7.002 | 30.700 | 30.103 | 6.996 | 32.850 |
| pO2 | 2.527 | 0.494 | 30.900 | 2.509 | 0.497 | 3.000 | 2.597 | 0.479 | 3.000 |
| ctHb | 150.961 | 21.106 | 3.000 | 147.748 | 18.661 | 151.000 | 145.792 | 24.314 | 154.500 |
| sO2 | 89.309 | 6.728 | 152.000 | 88.041 | 6.683 | 89.800 | 82.988 | 9.965 | 91.500 |
| FO2Hb | 87.321 | 6.566 | 86.500 | 86.055 | 7.270 | 88.200 | 81.194 | 9.834 | 89.550 |
| FCOHb | 0.938 | 0.664 | 84.600 | 0.829 | 0.385 | 0.800 | 0.951 | 0.345 | 0.800 |
| FHHb | 8.812 | 8.427 | 0.900 | 9.854 | 6.119 | 10.000 | 13.734 | 38.082 | 8.300 |
| FMetHb | 1.266 | 0.191 | 13.200 | 1.236 | 0.242 | 1.200 | 1.245 | 0.237 | 1.300 |
| Hctc | 46.494 | 6.650 | 1.300 | 45.326 | 5.615 | 46.300 | 44.741 | 7.301 | 47.350 |
| ctO2c | 18.539 | 2.776 | 46.700 | 18.017 | 3.245 | 18.600 | 16.602 | 3.467 | 18.900 |
| p50c | 23.918 | 6.128 | 17.400 | 23.835 | 2.217 | 23.980 | 24.771 | 2.666 | 23.490 |
| cBase(Ecf)c | 3.208 | 24.400 | 4.181 | 3.735 | |||||
| cHCO3(P.st)c | 20.653 | 14.614 | 20.116 | 3.001 | 20.700 | 19.593 | 2.735 | 20.400 | |
| cHCO3(P)c | 18.724 | 3.025 | 20.000 | 18.733 | 3.345 | 18.800 | 17.754 | 3.143 | 19.100 |
| ABEc | 3.148 | 18.300 | 3.948 | 3.524 | |||||
Activation functions of the hidden layers were tangent hyperbolic functions while the output layer had softmax activation function. The Softmax function is used in multiclass classification and its output is probabilities that range from 0 to 1, with a total sum of 1, thus obtaining the probability distribution that determines whether an object belongs to a certain class, enabling the identification of the exact class to which the object belongs.
3.Results
The data set consisted of 901 samples, with 36% of patients having mild symptoms, 36% with a moderate condition, and 28% of patients with a severe condition of COVID-19 infection. Table 3 shows the mean, median, standard deviation and range of continuous variables.
The results of the research show that the developed Clinical Decision-making system (eDSS) for classification of the severity of the COVID-19 infection achieves a high accuracy of 92.1% during training. After performing the subsequent validation, the overall accuracy of the system is 82.4%, which still represents an extremely satisfactory level of precision.
Table 4
eDDS system performance evaluation
| ANN output/real output | Mild | Moderate | Severe |
|---|---|---|---|
| Total number of samples 91 | 32 | 32 | 27 |
| Mild | 28 | 3 | 1 |
| Severe | 4 | 25 | 3 |
| Critical | 3 | 2 | 22 |
Analysis of the confusion matrix reveals details of the system’s performance for each severity category, shown in Table 4. The prediction rate for the category of mild symptoms is 87.5%, indicating a high ability of the system to recognize patients with a milder form of infection. On the other hand, the prediction rate for the moderate symptoms category is 78.1%, which is lower compared to other categories. This is understandable, given that there is an overlap between the moderate and mild/severe categories, making it difficult to distinguish precisely between them. Despite this, the system still showed a decent ability to identify patients with moderate symptoms. A prediction rate of 81.48% was achieved for the category of patients with severe infection. This suggests that the system is very successful in identifying patients with severe symptoms and enables timely and adequate treatment for these sensitive cases.
4.Discussion
This research proposes an easily interpreted decision-support system based on artificial intelligence for classifying the degree of severity of viral infection: COVID-19 use case based entirely on parameters collected during patient admission and standard medical protocol. The research was done taking into account more than 40 parameters processed in laboratory testing. The results showed that by using these parameters the model correctly classifies more than 80% of patients to respective classes of disease severity.
The importance and crucial function of AI-driven intelligent systems have significantly expanded over the past year due to the COVID-19 global health emergency. Recognizing the importance of AI in the healthcare sector, researchers from Bosnia and Herzegovina have embarked on a multidisciplinary project to leverage the data collected during routine medical practices at a general hospital. This project aimed to harness the potential of AI by developing the electronic Disease Severity Scoring (eDDS) system. The development of the eDDS system has yielded promising results, demonstrating the potential to achieve high accuracy in disease severity prediction. However, one notable challenge arose during the classification of the moderate class due to sample overlap. This highlights the complexity of accurately differentiating between moderate and other disease severity levels, but the developed eDSS enables rapid and accurate classification of patients according to symptom severity, which can help healthcare professionals make informed decisions about treatment and care. The high accuracy of the system indicates potential application in clinical practice, facilitating the work of healthcare teams and improving patient outcomes.
Numerous prior research endeavors primarily concentrated on detecting SARS-CoV2 infection in patients by utilizing chest CT scans, X-ray examinations, symptoms, or blood tests. In contrast, only limited investigations were conducted to forecast the potential severity of COVID-19. The majority of the parameters utilized in constructing the eDDS system were discovered to align with findings previously documented in literature. Age, a well-known predictor, is recognized as a significant risk factor for clinical severity [28]. CRP, an early indicator of inflammation, has also been identified as an early predictor of COVID-19 severity [29, 30]. Similarly, AST, a marker for liver damage, has been reported as an important predictor in forecasting severity [31].
Extensive review studies recently showcase the usage of AI for diagnosis or treatment of COVID-19 [24, 25, 27]. These studies deliver futuristic perspectives concerning forthcoming endemic and pandemic situations. By consolidating the advancements made during the COVID-19 era, where AI played a direct role, a framework to anticipate and address future outbreaks within the COVID-19 category can be established. COVID-19 has significantly accelerated the utilization of artificial intelligence (AI) in the healthcare industry, serving various purposes. Numerous AI-based solutions have been developed for COVID-19 prediction and classification. However, despite the progress, these solutions are still in the research phase, as not all regulatory challenges have been fully addressed for their widespread adoption.
In response to the pandemic, researchers have rushed to develop models that utilize AI, particularly machine learning, to assist clinicians as well as public health authorities in the challenging tasks of detecting, spreading, tracking, diagnosing, screening, monitoring and contact tracing of virus infections, complementing conventional approaches with state-of-the-art tools [32].
Machine learning algorithms have garnered considerable attention in the field of lung disease research [33]. By analyzing large volumes of data, such as patient records and genetic information, machine learning algorithms can identify patterns and correlations, and make accurate predictions has the potential to transform diagnosis, treatment, and drug development in the field of respiratory medicine.
Despite these satisfactory results, it is important to note that further validation and testing of the system on different datasets is needed to ensure its wider applicability and reliability. In addition, it is possible to consider the possibility of improving the system by adding new features and changing the architecture of the neural network to achieve even better performance.
Finally, this study highlights the power of artificial intelligence in medical applications, especially in the context of epidemics and pandemics. Systems such as the developed eDSS can be key tools in the fight against viral infections, providing important information to healthcare professionals and contributing to improved care and patient outcomes worldwide.
5.Conclusion
In this study, we presented the development and analysis of a decision support system (eDDS) designed for the classification of COVID-19 clinical severity into three distinct categories: mild, moderate, and severe. For the development of the system, a dataset from General Hospital Tešanj consisting of 1000 samples was used. For the development of the eDDS an ANN was used. The developed eDSS achieved accuracy of 92.1% during training and 82.4% accuracy during validation. The analysis of the system performance delineated the system’s performance across severity categories, with notably high recognition rates for patients with mild and severe symptoms, underscoring the system’s efficacy in facilitating precise and timely interventions for sensitive cases. The observed variation in prediction rates across different severity categories can be attributed to the inherent complexities of distinguishing between overlapping symptom profiles. Mild symptoms often exhibit distinct characteristics that the system can readily identify, leading to the higher prediction rate of 87.5%. Conversely, the moderate symptoms category presents challenges due to the shared features with both mild and severe cases, resulting in a comparatively lower prediction rate of 78.1%. Despite these complexities, the system still demonstrates a commendable ability to recognize patients with moderate symptoms. Notably, the system’s remarkable success in identifying patients with severe symptoms, attaining a prediction rate of 81.48%, underscores its proficiency in aiding prompt and appropriate treatment for critical cases.
However, we acknowledge the complexities associated with distinguishing overlapping symptom profiles, leading to varying prediction rates across severity categories. While our system demonstrated commendable proficiency in recognizing moderate symptoms (82.4%) and identifying severe cases (81.48%), the challenges presented by the moderate symptom category necessitate further exploration and refinement. Continuous model optimization, collaboration with clinical experts, and the implementation of a feedback loop contribute to its adaptive nature in response to evolving clinical scenarios. Emphasizing human-AI collaboration and maintaining an ethical framework for patient data usage will be pivotal in harnessing the full potential of AI while preserving the expertise of medical professionals. In conclusion, our research has unveiled a promising pathway for the integration of AI-based decision support systems into clinical practice especially in the low-middle income countries. The synergy between technological innovation and medical expertise holds the key to addressing the challenges posed by viral infections like COVID-19. With sustained collaboration and a forward-looking perspective, AI has the potential to revolutionize medical practice and contribute significantly to the management of infectious diseases.
Acknowledgments
This research study was supported by the Ministry of Science, Higher Education and Youth of Canton Sarajevo. Project title: [eDSS] – Classification of degree of clinical picture and prediction of therapy in patients with viral infections: COVID-19 case, 2021.
Conflict of interest
The authors declare that they have no conflict of interest.
References
[1] | Available online: COVID-19: Clinical features – UpToDate. |
[2] | Mercaldo F, Belfiore MP, Reginelli A, et al. Coronavirus COVID-19 detection by means of explainable deep learning. Sci Rep. (2023) ; 13: : 462. doi: 10.1038/s41598-023-27697-y. |
[3] | Thanh Le T, Andreadakis Z, Kumar A, et al. The COVID-19 vaccine development landscape. Nat Rev Drug Discov. (2020) ; 19: (5): 305-306. doi: 10.1038/d41573-020-00073-5. |
[4] | Şeyma Y, Cemil Ç, Saim Y. Artificial Intelligence-Based Prediction of COVID-19 Severity on the Results of Protein Profiling. Computer Methods and Programs in Biomedicine. (2021) ; 202: : 105996, ISSN 0169-2607. doi: 10.1016/j.cmpb.2021.105996. |
[5] | CDC COVID-19 Response Team. Severe Outcomes Among Patients with Coronavirus Disease 2019 (COVID-19) – United States, February 12–March 16, 2020. MMWR Morb Mortal Wkly Rep. (2020) ; 69: (12): 343-346. Published 2020 Mar 27. doi: 10.15585/mmwr.mm6912e2. |
[6] | Wang Y, Wang Y, Chen Y, Qin Q. Unique epidemiological and clinical features of the emerging 2019 novel coronavirus pneumonia (COVID-19) implicate special control measures. J Med Virol. (2020) ; 92: (6): 568-576. doi: 10.1002/jmv.25748. |
[7] | Khanna VV, Chadaga K, Sampathila N, et al. Diagnosing COVID-19 using artificial intelligence: A comprehensive review. Netw Model Anal Health Inform Bioinforma. (2022) ; 11: : 25. doi: 10.1007/s13721-022-00367-1. |
[8] | |
[9] | Zhou S, Jin Q, Jiang X, et al. Application of remote fetal heart rate monitoring via internet in late pregnancy during the COVID-19 pandemic [published online ahead of print, 2023 Apr 27]. Technol Health Care. (2023) ; 10.3233/THC-220700. doi: 10.3233/THC-220700. |
[10] | Lewandowski N, Koller B. Transforming medical sciences with high-performance computing, high-performance data analytics and AI [published online ahead of print, 2023 Jun 13]. Technol Health Care. (2023) ; 10.3233/THC-237000. doi: 10.3233/THC-237000. |
[11] | Majeed A, Lee S. Applications of Machine Learning and High-Performance Computing in the Era of COVID-19. Appl. Syst. Innov. (2021) ; 4: : 40. doi: 10.3390/asi4030040. |
[12] | Mbunge E, Akinnuwesi B, Fashoto SG, Metfula AS, Mashwama P. A critical review of emerging technologies for tackling COVID-19 pandemic. Hum Behav Emerg Technol. (2021) ; 3: (1): 25-39. doi: 10.1002/hbe2.237. |
[13] | Comito C, Pizzuti C. Artificial intelligence for forecasting and diagnosing COVID-19 pandemic: A focused review. Artif Intell Med. (2022) ; 128: : 102286. doi: 10.1016/j.artmed.2022.102286. |
[14] | Xu M, Ouyang L, Han L, et al. Accurately Differentiating Between Patients With COVID-19, Patients With Other Viral Infections, and Healthy Individuals: Multimodal Late Fusion Learning Approach. J Med Internet Res. (2021) ; 23: (1): e25535. doi: 10.2196/25535. |
[15] | Cohen PA, Hall LE, John JN, Rapoport AB. The Early Natural History of SARS-CoV-2 Infection: Clinical Observations From an Urban, Ambulatory COVID-19 Clinic. Mayo Clin Proc. (2020) ; 95: (6): 1124-1126. doi: 10.1016/j.mayocp.2020.04.010. |
[16] | Stokes, Katy, Castaldo, Rossana, Franzese, Monica, Salvatore, Marco, Fico, Giuseppe, Pokvic, Lejla Gurbeta, Badnjevic, Almir and Pecchia, Leandro. A machine learning model for supporting symptom-based referral and diagnosis of bronchitis and pneumonia in limited resource settings. Biocybernetics and Biomedical Engineering. (2021) ; 41: (4): 1288-1302. doi: 10.1016/j.bbe.2021.09.002 ISSN 0208-5216. |
[17] | Badnjevic A, Gurbeta L, Custovic E. An expert diagnostic system to automatically identify asthma and chronic obstructive pulmonary disease in clinical settings. Scientific Reports. (2018) ; 8: (1): 11645. doi: 10.1038/s41598-018-30116-2. |
[18] | Šeho L, Šutković H, Tabak V, Tahirović S, Smajović A, Bečić E, Deumić A, Spahić Bećirović L, Gurbeta Pokvić L, Badnjević A. Using artificial intelligence in diagnostics of meningitis. IFAC-PapersOnLine. (2022) ; 55: (4): 56-61. doi: 10.1016/j.ifacol.2022.06.009. |
[19] | Vinod DN, Prabaharan SRS. COVID-19-The Role of Artificial Intelligence, Machine Learning, and Deep Learning: A Newfangled. Arch Computat Methods Eng. (2023) ; 30: : 2667-2682. doi: 10.1007/s11831-023-09882-4. |
[20] | Piccialli F, di Cola V, Giampaolo F, et al. The Role of Artificial Intelligence in Fighting the COVID-19 Pandemic. Inf Syst Front. (2021) ; 23: : 1467-1497. doi: 10.1007/s10796-021-10131-x. |
[21] | Laguarta J, Hueto F, Subirana B. COVID-19 Artificial Intelligence Diagnosis Using Only Cough Recordings. In IEEE Open Journal of Engineering in Medicine and Biology. Vol. 1, (2020) , pp. 275-281. doi: 10.1109/OJEMB.2020.3026928. |
[22] | Vaishya R, Javaid M, Khan IH, Haleem A. Artificial Intelligence (AI) applications for COVID-19 pandemic. Diabetes & Metabolic Syndrome. (2020) ; 14: (4): 337-339. doi: 10.1016/j.dsx.2020.04.012. |
[23] | Abdulaal A, Patel A, Charani E, Denny S, Mughal N, Moore L. Prognostic Modeling of COVID-19 Using Artificial Intelligence in the United Kingdom: Model development and validation. J Med Internet Res. (2020) Aug 25; 22: (8): e20259. doi: 10.2196/20259. PMID: 32735549; PMCID: PMC7451108. |
[24] | Wang L, Zhang Y, Wang D, Tong X, Liu T, Zhang S, Huang J, Zhang L, Chen L, Fan H, Clarke M. Artificial Intelligence for COVID-19: A Systematic Review. Front Med (Lausanne). (2021) Sep 30; 8: : 704256. doi: 10.3389/fmed.2021.704256. PMID: 34660623; PMCID: PMC8514781. |
[25] | Khan M, Mehran MT, Haq ZU, et al. Applications of artificial intelligence in COVID-19 pandemic: A comprehensive review. Expert Syst Appl. (2021) ; 185: : 115695. doi: 10.1016/j.eswa.2021.115695. |
[26] | Available online: COVID – Coronavirus Statistics – Worldometer (worldometers.info). |
[27] | Hasan MM, Islam MU, Sadeq MJ, Fung W-K, Uddin J. Review on the Evaluation and Development of Artificial Intelligence for COVID-19 Containment. Sensors. (2023) ; 23: (1): 527. doi: 10.3390/s23010527. |
[28] | Gallo Marin B, Aghagoli G, Lavine K, et al. Predictors of COVID-19 severity: A literature review. Rev Med Virol. (2021) ; 31: (1): 1-10. doi: 10.1002/rmv.2146. |
[29] | Ahnach M, Zbiri S, Nejjari S, Ousti F, Elkettani C. C-reactive protein as an early predictor of COVID-19 severity. J Med Biochem. (2020) ; 39: (4): 500-507. doi: 10.5937/jomb0-27554. |
[30] | Chen W, Zheng KI, Liu S, Yan Z, Xu C, Qiao Z. Plasma CRP level is positively associated with the severity of COVID-19. Ann Clin Microbiol Antimicrob. (2020) ; 19: (1): 18. doi: 10.1186/s12941-020-00362-2. |
[31] | Bennett TD, Moffitt RA, Hajagos JG, et al. Clinical Characterization and Prediction of Clinical Severity of SARS-CoV-2 Infection Among US Adults Using Data From the US National COVID Cohort Collaborative. JAMA Netw Open. (2021) ; 4: (7): e2116901. doi: 10.1001/jamanetworkopen.2021.16901. |
[32] | Comito C, Pizzuti C. Artificial intelligence for forecasting and diagnosing COVID-19 pandemic: A focused review. Artif Intell Med. (2022) ; 128: : 102286. doi: 10.1016/j.artmed.2022.102286. |
[33] | Bećirović LS, Deumić A, Pokvić LG, Badnjevic A. Aritificial Inteligence Challenges in COPD management: a review. 2021 IEEE 21st International Conference on Bioinformatics and Bioengineering (BIBE), Kragujevac, Serbia. (2021) , pp. 1-7. doi: 10.1109/BIBE52308.2021.9635374. |

