
Clinical evaluation of the effectiveness of a new orthotic device for the non-operative treatment of scoliosis
Abstract
BACKGROUND:
Bracing is one of the oldest non-operative treatments for patients with scoliosis. However, a wide variety of braces is used, and some show no effect, while others show conflicting results.
OBJECTIVE:
We aimed to evaluate the effectiveness of a new orthotic device for the treatment of adult scoliosis.
METHODS:
Twenty adult patients who were diagnosed with scoliosis and qualified for the study were selected and all participants were treated for 12 hours/day for 12 weeks using a new orthotic device. Various efficacy assessments (Cobb’s angle, spine length, pelvic angle, shoulder angle, thoracic angle, lumbar angle, pelvic sacral angle) were performed before and after the 12-week treatment. The values at each time point were compared.
RESULTS:
There were significant treatment effects in a time-dependent manner on every efficacy assessment (
CONCLUSION:
In this clinical study, it was demonstrated that a new brace that is more comfortable for the wearer reduced scoliosis and may be a useful option for non-operative treatment of scoliosis.
1.Introduction
Normal human movement begins with maintaining proper posture. The human body may appear to be standing in a static state with no movement; however, in fact, the body itself is being finely controlled continuously to counteract gravity and to maintain the center of mass stable on the base of support. Therefore, imbalances create biomechanical compensation during postural activities [1]. In particular, pelvic obliquity that appears in the frontal plane due to imbalance may cause scoliosis by exerting asymmetrical pressure on the pelvis [2].
Generally, the spine is considered a uniquely unstable system that maintains posture with muscle-ligament structure, while providing movement at the same time [3, 4, 5, 6, 7]. Repetitive weight shift to one side of the pelvis or hip pressure being concentrated on one side [8] may lead to permanent deformities, including scoliosis and kyphosis [9]. Progression of scoliosis takes place during the development of young humans, and as a progressive disease that can have a major impact on function, scoliosis has a high incidence rate during this period and causes high socioeconomic costs owing to disease progression [10, 11, 12].
Treatment modalities for scoliosis include physiotherapy, use of orthopedic devices (braces), and surgery. Nevertheless, there remains debate as to the efficacy of these modalities [13]. With respect to physiotherapy [14, 15, 16, 17, 18, 19, 20], studies reported that there were no evidence-based results because of lack of reports of application of physiotherapy only that made observations until maturation of the musculoskeletal system [16, 19]. Other studies compared physiotherapy and bracing, but reported that it is difficult to identify which modality was more effective for scoliosis due to lack of scientific evidence [17, 20].
Surgical methods used include spinal fusion surgery [21, 22, 23, 24, 25, 26] and use of interspinous spacers [8]. However, spinal fusion surgery is not an effective treatment modality because of the health issues that it may cause [21, 22, 23, 24], including rib cysts and spinal herniation within 1 year after surgery [21, 22]. Some studies also reported that surgery is questionable as a treatment modality for scoliosis because of recurrence of long-term complications [21, 25, 26].
With respect to bracing, various braces, including the Cheneau brace and the Boston brace, are used regardless of growth stage [27, 28, 29, 30, 31, 32, 33]. A recent review reported that the treatment modality with the application of a brace is an evidence-based modality and it was found to be effective even in follow-up observations after completed growth of the musculoskeletal system [13]. Nevertheless, because a wide variety of braces being used, some show no effect whatsoever, while others show conflicting results [27, 28, 29, 30, 31, 32, 33, 34]. Braces made of soft material that were developed to overcome the disadvantages of braces made of hard material have been reported to not provide sufficient compliance, contrary to the claims of the manufacturers [35]. Bracing is one of the oldest non-operative treatment modalities; nevertheless, it continues to have problems while new methods of bracing are being introduced.
Currently, braces that have been used as non-operative treatment modalities have consisted mostly of devices that limited movement by wrapping the entire upper body where scoliosis is present with a hard material. Recent braces, by contrast, use a method of correction that allows flexibility by separating the upper parts (towards the shoulders) and lower parts (towards the pelvis) of scoliosis. Accordingly, the present study applied the newly introduced brace on adult patients with scoliosis as a non-operative treatment modality to identify its preliminary clinical effect.
2.Materials and methods
2.1The principle of a new orthotic brace
When the pelvis becomes twisted, it generally shows three types of directionalities (elevation/ deviation/rotation). Three-dimensional (3D) stabilization of the pelvis using an orthopedic brace is designed to achieve spinal stabilization, and having a positive effect on balancing the center of gravity during gait and movement. When the two ilium bones in the pelvis become twisted, space is created between the sacroiliac joint, the pubic symphysis, and the left and right hip joints, for which convergence and 3D-stabilization must be promoted together. The typical correction method is based on the principle of force in one or two directions being countered by force in opposite direction, meaning the three-point pressure principle of applying force that pushes in the direction opposite to incurvation (curved spine) (Fig. 1(L)). The principle of correction mechanism of ALL LINE
Figure 1.
(L) Three point pressure method; (R) Counter compensation method: Two forces F

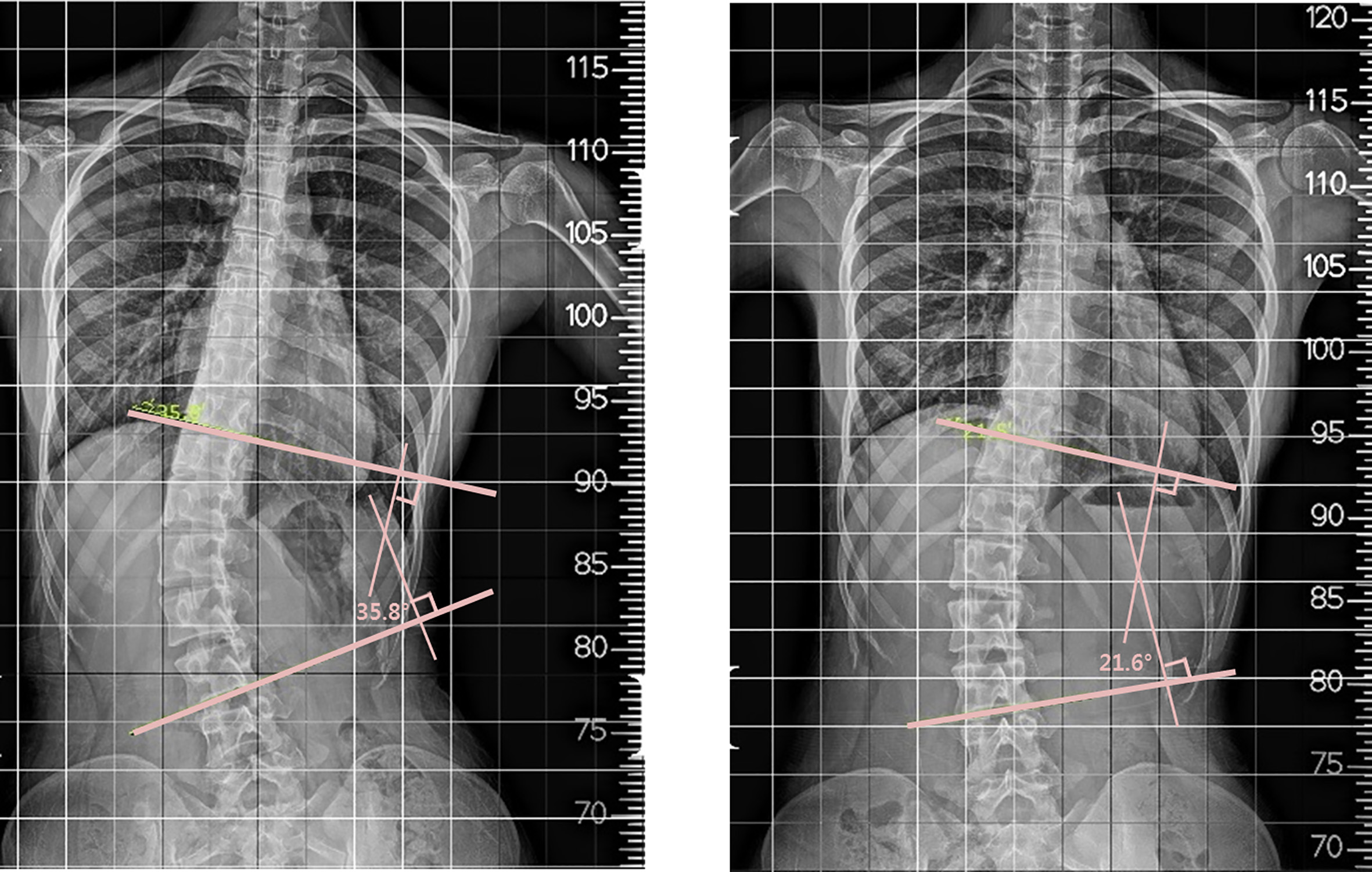
Figure 2.
Before (L) and after (R) treatment. X-ray images of a patient wearing the new brace.
2.2Evaluation of effectiveness of a new brace
Anteroposterior (AP) and lateral view radiographs of the thoracolumbar spine in the standing posture were obtained from patients aged 19–40 years. Patients who were diagnosed with scoliosis with a Cobb’s angle of 10
2.3Measurement methods
2.3.1Measurement of changes in Cobb’s angle
Cobb’s angle is a diagnostic measure of scoliosis. After locating T2, where spinal curvature begins, and T8, where the lowest structural curve is found, T5 representing the apex at the midline of T2–T8 is defined. After drawing a line along the top of the vertebral body (T3) with a large slope above T5 and a line along the bottom of the vertebral body (T7) with a large slope below T5, lines perpendicular to the top and bottom lines are drawn and the angle formed where the two lines intersect represents Cobb’s angle [37]. This is the most reliable and accurate method for measuring spinal curvature. In the present study, patients with Cobb’s angle
2.3.2Measurement of other changes
Other bodily changes were measured as described below.
Change in height
The difference of the length from the bottom of the feet to the top of the head when a person stands upright before and after the brace.
Spine length
Spine length is from the top of the seventh cervical vertebra to the bottom of the fifth lumbar vertebra.
Pelvic angle
In the pelvic area, the angles were measured relative to the apex of left and right iliac crest.
Shoulder angle
In the shoulder area, angle of the location of the left and right acromioclavicular joints.
Deviation of scoliotic spine from the midline
Definition of endpoint: measure deviation of scoliotic apex relative to the midline passing through the first sacral vertebra.
2.4Data analysis
Spine length, pelvic angle, shoulder angle, and deviation of scoliotic spine from the midline measured before and 12 weeks after wearing the brace were compared. Data satisfying normality were analyzed using paired
3.Results
Normality test for comparison of spine length, pelvic angle, shoulder angle, and deviation of scoliotic spine from the midline measured before and 12 weeks after wearing the brace showed that shoulder angle, deviation of scoliotic spine from the midline (thoracic angle), and deviation of scoliotic spine from the midline (lumbar angle) satisfied normality; therefore, they were analyzed using paired
A total of 20 adults were enrolled in the present study; however, due to drop-out of two participants, the study was ultimately conducted with 18 participants (17 females and 1 male). The mean age of the participants was 24.33 years, ranging between 19 and 34 years (Table 1).
Table 1
Patients’ demographic information
| Mean | |
|---|---|
| Age (years) | 24.33 |
| Height (cm) | 163.13 |
Table 2
Treatment results of the group with the brace
| Before wearing the brace | 12 weeks after wearing the brace | Before – After | ||
| Mean | Mean | Mean | ||
| Cobb’s angle | 29.34 | 23.99 | 5.35 | 0.000 |
| Spine length | 41.41 | 42.21 | 0.000 | |
| Pelvic angle | 2.32 | 1.04 | 1.28 | 0.001 |
| Shoulder angle | 2.27 | 1.19 | 1.08 | 0.010 |
| Thoracic angle | 4.22 | 3.46 | 0.75 | 0.001 |
| Lumbar angle | 4.36 | 3.80 | 0.56 | 0.002 |
| Pelvic sacral angle | 0.53 | 0.36 | 0.17 | 0.002 |
As shown in Table 2, the mean Cobb’s angle changed from 29.34
4.Discussion
We conducted a clinical trial which applied a newly introduced method of bracing for adult patients diagnosed with scoliosis. Applying the brace showed improvement in all parameters: Cobb’s angle, spine length, pelvic angle, shoulder angle, and thoracic, lumbar, and pelvic sacral angles from the midline.
Currently, various braces (Cheneau, Boston, Spine Cor, Milwaukee, and CAD/CAM) are used, regardless of whether the patient is an adolescent or adult [27, 28, 29, 30, 31, 32, 33, 34]. However, some braces are disliked by adolescent patients because of their outer appearance; for this reason, some people falsely participated in previous studies, claiming to have worn the brace when they actually did not [36]. As mentioned before, people feel uncomfortable about wearing braces in spite of the improvement of design and material compliance [27, 28, 29, 30, 31, 32, 33, 34, 35]. Therefore, despite its long history, there remains the need to develop braces that have few problems with appearance for use in long-term treatment, stability for therapeutic effect, assuring flexibility needed for movement during daily life, and being highly effective even when worn for a short time.
According to previous studies, there were no major differences of brace effect between wearing a brace part-time (12–16 hours) versus full time (23 hours) [6, 9]. Kahanowitz reported that similar results were found when the pre-brace Cobb’s angle was
The limitations of the present study include the fact that the orthopedic brace was worn for a short period of only 12 weeks (3 months), which is shorter than observational periods in previous studies. Moreover, the study did not observe return of symptoms during the period when the orthopedic brace was no longer worn. The study also did not identify the efficacy and safety of the brace in patients with scoliosis who were in the growing stage. Nonetheless, this preliminary study could provide clinical evidence that wearing an appropriate orthopedic brace, even for a short period, sufficiently relieved scoliosis in adult patients with moderate scoliosis. Expanded clinical trials will be performed to address these limitations are needed in the future.
Acknowledgments
This research was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute, funded by the Ministry of Health and Welfare, Republic of Korea (grant no. HI15C1529).
Conflict of interest
None to report.
References
[1] | Neumann D. Kinesiology of the musculoskeletal system: Foundations for rehabilitation. st louis, MO: Mosby (2010) . |
[2] | Drummond D, Breed AL, Nerechina R. Relationship of spine deformity and pelvic obliquity on sitting pressure distributions and decubitus ulceration. J Pediartr Orthop. (1985) ; 5: (4): 396-402. |
[3] | Klein JA, Hukins DWL. Functional differentiation in the spinal column. Eng Med. (1983) ; 12: : 3-18. |
[4] | Panjabi MM. The stabilising system of the spine. 1: Function, dysfunction, adaptation and enhancement. J Spinal Disord. (1992) ; 5: : 383-9. |
[5] | Roaf R. Vertebral growth and its mechanical control. J Bone Joint Surg [Br]. (1960) ; 42: : 40-59. |
[6] | White AA, Panjabi MM, Thomas CL. Clinical biomechanics of kyphotic deformities. Clin Orthop. (1977) ; 128: : 8-17. |
[7] | White AA, Panjabi MM. Clinical biomechanics of the spine, 2 |
[8] | Drummond D, Guadagni J, Keene JS, Breed A, Narechania R. Interspinous process segmental spinal instrumentation and posterior spinal fusion for idiopathic scoliosis. J Paediat Orthop. (1984) ; 4: : 405-408. |
[9] | Rosalind H, Patsy A, David P. Wheelchair users and postural seating: A clinical approach. London, Churchill Livingstone, (1998) ; 7-9. |
[10] | Kotwicki T, Durmała J, Czaprowski D, Głowacki M, Kołban M, Snela S, Sliwiński Z, Kowalski IM. Conservative management of idiopathic scoliosis-guidelines based on SOSORT 2006 Consensus. Ortop Traumatol Rehabil. (2009) Sep-Oct; 11: (5): 379-95. |
[11] | Weinstein SL. Natural history. Spine. (1999) ; 24: : 2592-2600. |
[12] | Weiss HR, Negrini S, Rigo M, Kotwicki T, Hawes MC, Grivas TB, Maruyama T, Landauer F. Indications for conservative management of scoliosis. Scoliosis. (2005) ; 1: : 5. |
[13] | Weiss HR. Intervention studies on scoliosis – Review of the reviews. Pol Ann Med. (2012) ; (19): 72-83. |
[14] | den Boer WA, Anderson PG, Limbee kJ, Kooijman MA. Treatment of idiopathic scoliosis with side-shift therapy: An initial comparison with a brace treatment historical cohort. Eur Spine J. (1999) ; 8: (5): 406-410. |
[15] | Ferraro C, Masiero S, Venturin A. Effect of exercise therapy on mild idiopathic scoliosis. Eur Medicophys. (1998) ; 34: : 25-31. |
[16] | Fusco C, Zaina F, Atanasio S, Romano M, Negrini A, Negrini S. Physical exercises in the treatment of adolescent idiopathic scoliosis: An updated systematic review. Physiother Theory Pract. (2011) ; 27: (1): 80-114. |
[17] | Negrini S, Atanasio S, Negrini F, Zaina F, Marchini G. The Sforzesco brace can replace cast in the correction of adoles-cent idiopathic scoliosis: a controlled prospective cohort study. Scoliosis. (2008) ; 31: (3): 15. |
[18] | Negrini S, Atanasio S, Zaina F, Romano M, Parzini S, Negrini A. End-growth results of bracing and exercises for adolescent idiopathic scoliosis. Prospective worst-case analysis. Stud Health TechnolIn Form. (2008) ; 135: : 395-408. |
[19] | Negrini S, Fusco C, Minozzi S, Atanasio S, Zaina F, Romano M. Exercises reduce the progression rate of adolescent idiopathic scoliosis: Results of a comprehensive systematic review of the literature. Disabil Rehabil. (2008) ; 30: (10): 772-785. |
[20] | Negrini S, Zaina F, Romano M, Negrini A, Parzini S. Specific exercises reduce brace prescription in adolescent idiopathic scoliosis: A prospective controlled cohort study with worst-case analysis. J Rehabil Med. (2008) ; 40: (6): 451-455. |
[21] | Hawes MC. Impact of spine surgery on sign sand symptoms of spinal deformity. Pediatr Rehabil. (2006) ; 9: (4): 318-339. |
[22] | Hawes MC, O’Brien JP. Acentury of spine surgery: What can patients expect? Disabil Rehabil. (2008) ; 30: (10): 808-817. |
[23] | Weiss H-R. Adolescent idiopathic scoliosis – case report of a patient with clinical deterioration after surgery. Patient Saf Surg. (2007) ; 1: : 7. |
[24] | Weiss H-R, Goodall D. The treatment of adolescent idiopathic scoliosis (AIS) according to present evidence. Asystematic review. Eur J Phys Rehabil Med. (2008) ; 44: (2): 177-193. |
[25] | Asher MA, Burton DC. Adolescent idiopathic scoliosis: Natural history and long term treatment effects. Scoliosis. (2006) ; 1: (1): 2. |
[26] | Weiss H-R, Goodall D. Rate of complications in scoliosis surgery – a systematic review of the Pub Med literature. Scoliosis. (2008) ; 5: (3): 9. |
[27] | Hasler CC, Wietlisbach S, Buchler P. Objective compliance of adolescent girls with idiopathic scoliosis in a dynamic Spine-Cor brace. J Child Orthop. (2010) ; 4: (3): 211-218. |
[28] | Danielsson AJ, Hasserius R, Ohlin A, Nachemson AL. A prospective study of brace treatment versus observation alone in adolescent idiopathic scoliosis: A follow-up mean of 16 years after maturity. Spine. (2007) ; 32: (20): 2198-2207. |
[29] | Hasler CC, Wietlisbach S, Büchler P. Objective compliance of adolescent girls with idiopathic scoliosis in a dynamic Spine-Cor brace. J Child Orthop. (2010) ; 4: (3): 211-218. |
[30] | Nachemson AL, Peterson LE. Effectiveness of treatment with a brace in girls who have adolescent idiopathics coliosis. A prospective, controlled study based on data from the Brace Study of the Scoliosis Research Society. J Bone Joint Surg (Am). (1995) ; 77: (6): 815-822. |
[31] | Rigo M. Radiological and cosmetic improvement 2 years after brace weaning – a case report. Pediatr Rehabil. (2003) ; 6: (3–4): 195-199. |
[32] | Weiss H-R, Weiss G. Brace treatment during pubertal growth spurt in girls with idiopathic scoliosis (IS) – a prospective trial comparing two different concepts. Pediatr Rehabil. (2005) ; 8: (3): 199-206. |
[33] | Wong MS, Cheng JC, Lam TP, Ng BK, Sin SW, Lee-Shum SL, et al. The effect of rigid versus flexible spinal orthosis on the clinical efficacy and acceptance of the patients with adolescent Idiopathic scoliosis. Spine. (2008) ; 33: (12): 1360-1365. |
[34] | Castro FP Jr. Adolescent idiopathic scoliosis, bracing, and the Hueter – Volkmann principle. Spine J. (2003) ; 3: (3): 180-185. |
[35] | Coillard C, Vachon V, Circo AB, Beauséjour M, Rivard CH. Effectiveness of the Spine Cor brace based on the new standardized criteria proposed by the scoliosis research society for adolescent idiopathic scoliosis. J Pediatr Orthop. (2007) ; 27: (4): 375-379. |
[36] | Houghton GR, McInerney A, Tew T. Monitoring true brace compliance. Orthop Trans. (1987) ; 11: : 105. |
[37] | Brooks WJ, Krupinski EA, Hawes MC. Reversal of childhood idiopathic scoliosis in an adult, without surgery: A case report and literature review. Scoliosis. (2009) ; 15: : 4-27. |

