Epidemiological Profile and Risk Factors of Ovarian Cancer in Ibn Rochd University Hospital of Casablanca Morocco: About 131 Cases
A B S T R A C T
Introduction: Ovarian cancer is one of the leading causes of morbidity and mortality in women worldwide, generally characterized by a poor prognosis. Most cases are diagnosed at an advanced stage. The standardized incidence rate for the world population is 8.1/100,000 women per year, with an estimated 239,000 new cases and 152,000 deaths per year worldwide.
Methods: This study aims to evaluate the epidemiological characteristics and risk factors of ovarian cancer by studying the risk factors of this pathology on a sample of 131 cases followed at the Ibn Rochd University Hospital in Casablanca from 2010 to 2012 using SPSS version 16.0 software.
Results: The average age of the patients is 51.47±13 years, the significant risk factors observed are multiparity (64.3%), menopause (58%) as personal history and hypertension (77.78%) as medical history. The majority of the patients (60%) came from urban areas, (50.4%) had cystic looking tumors (34.4%) on the right side, cystadenocarcinoma (20.6%) was the most frequent histological type, (74.8%) metastases were noted, including (44.3%) peritoneal carcinosis.
Conclusion: We concluded that the epidemiological profile of ovarian cancer is close to national and Maghreb data. A better biological investigation as well as an adequate management would allow its early diagnosis and the reduction of its incidence.
Keywords
Ovarian cancer, incidence, risk factors
Introduction
Ovarian cancer is the deadliest gynaecological cancer [1]. It is the seventh most common cancer in women [2]. Its particularity lies in its silent nature, which is responsible for a delay in diagnosis and difficulty in treatment; however, only 20% of cases are detected at an early stage [3]. The high mortality rate among ovarian cancer patients is mainly due to late diagnosis in about 75% of patients [4]. Ovarian cancer is a serious disease because it is detected after it has reached the peritoneal surface and is more common in both economically more developed and less developed countries, with a five-year survival rate [5]. The standardized mortality rate for the world population is 4.6/100,000 women per year [6]. It is the fifth most common cancer in women in developed countries, with an average incidence of 1/10000 and an estimated 5000 new cases each year [7]. Globally, an estimated 239,000 new cases and 152,000 deaths from ovarian cancer occur each year [8].
In Morocco, ovarian cancer ranks fourth among female cancers, and in more than (35%) of cases it is only detected at stage IV of the disease; more than half of the cases occur between 45 and 64 years of age [9, 10]. The aim of this work is to evaluate the epidemiological profile of ovarian cancer in Casablanca and to identify the risk factors through a retrospective study including 131 ovarian cancer patients.
Methods
This is a descriptive retrospective study spread over a period of thirty-six months from January 2010 to December 31, 2012, conducted at the Oncology Center of the Ibn Rochd University Hospital in Casablanca.
Operating Sheet
This is a retrospective descriptive study spread over a period of thirty-six months from January 2010 to December 31, 2012, conducted at the Oncology Center of the Ibn Rochd University Hospital in Casablanca. All patients with histologically confirmed ovarian cancer hospitalized at the CHU Ibn Rochd de Casablanca were included. Any file with missing information on several sections of the operating sheet was excluded (clinical, radiological, among others). The data collection was carried out using an exploitation sheet of hospitalization records which were processed by a statistical study using the SPSS software. A univariate analysis was performed to reveal the characteristics of the study population. A bivariate analysis was conducted to identify risk factors. We used the Chi-2 test to analyse qualitative variables and the Student and Anova test (analysis of variance) for quantitative variables. The significance level was set at 5% (p < 0.05: significant test).
Results
I Ovarian Cancer Risk Factors
The risk factors for ovarian cancer with significant findings in our study were personal history (16%, p=0.0001 <0.05) and medical history (13.7%, P<0.0001 (=0.000012) <0.05), on the other hand the surgical history (12.2%, P<0.0001 (=0.00004)) and family history (13.7%, P<0.0001 (=0.000012)) do not show significant results.
i Personal History
Of the 131 patients included in this study, (16%) had a personal history, of which (58%) were postmenopausal, (11.5%) were taking contraceptives, (7.6%) had miscarriages, and (64.3%) were multiparous. Multiparity is the risk factor most frequently found in our patients (64.3%) of cases, followed by menopause (58%) of cases.
ii Medical History
In our series of studies, (13.7%) of the cases had a medical history. MTA is the most common risk factor found in our patients (77.78%) of the cases (Table 1).
Table 1: Medical history among the 131 ovarian cancer patients in the Oncology Department of the Ibn Rochd University Hospital of Casablanca (2010-2012).
|
Medical history |
Number of cases |
Frequency (%) |
|
HTA |
14 |
77.78 |
|
Tuberculosis |
2 |
11.11 |
|
Valvulopathy |
2 |
11.11 |
|
Total |
18 |
100 |
iii Family History and Surgical History
In our study series (13.7%) of our patients' cases have a family history (Table 2), (12.2%) of cases have a surgical history (Table 3).
Table 2: Surgical history among the 131 ovarian cancer patients in the Oncology Department of the Ibn Rochd University Hospital of Casablanca (2010-2012).
|
Surgical history |
Number of cases |
(%) |
|
Ovarian cyst adnexectomy |
4 |
25 |
|
Fibroma |
3 |
18,75 |
|
Hysterectomy |
1 |
6,25 |
|
Colorectal |
1 |
6,25 |
|
Cyst |
1 |
6,25 |
|
Crack |
1 |
6,25 |
|
Cholecystectomy |
1 |
6,25 |
|
Left breast cyst |
1 |
6,25 |
|
Hand fracture |
1 |
6,25 |
|
Eye problem |
1 |
6,25 |
|
Bladder cyst |
1 |
6,25 |
|
Total |
16 |
100 |
Table 3: Family history among the 131 ovarian cancer patients in the Oncology Department of the Ibn Rochd University Hospital of Casablanca (2010-2012).
|
Family history |
Number of cases |
% |
|
Breast Neo |
8 |
44,44 |
|
Brain tumor |
2 |
11,12 |
|
Neo stomach |
2 |
11,12 |
|
Colonist Neo |
2 |
11,12 |
|
Liver metastasis |
1 |
5,55 |
|
Neo liver |
1 |
5,55 |
|
pulmonary TBK |
1 |
5,55 |
|
Neo lung |
1 |
5,55 |
|
Total |
18 |
100 |
II Epidemiological Profile Prevalence
Out of a total number of 8555 registered cancer cases, 131 cases of ovarian cancer have been recorded at the Oncology Centre of the Ibn Rochd University Hospital in Casablanca. The average number of ovarian cancers in our series per year is 43.66. According to our calculations, the prevalence of ovarian cancer at the CHU Ibn Rochd Casablanca from 2010 to 2012 is 2.7%.
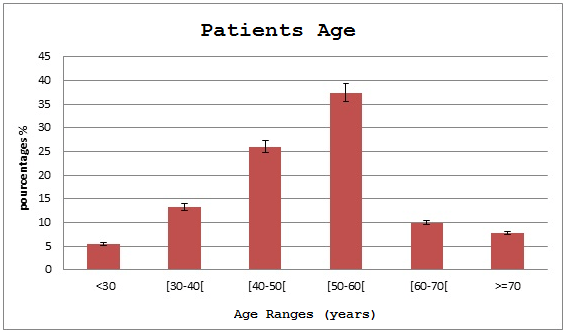
Figure 1: Age of selected patients from 131 ones with ovarian cancer at the Ibn Rochd University Hospital, Casablanca, Morocco, 2010-2012.
i The Age of the Patients
In our series, the average age of our patients is 51.47 years with extremes ranging from 19 to 91 years and an ecotype of 13,200. The peak in frequency (31.3%) is in the fifth decade (Figure 1). The age group most concerned is between 50 and 60 years old (31.3%), followed by 40 and 50 years old (26.7%). Patients at a young age (≤ 30 years old) were the least affected (3.8%).
ii Origin of Patients
According to the statistical data of our series, about half of our patients 78 cases or (60%) are from urban areas while 52 cases or (40%) are from rural areas.
iii Location of the Disease
Tumors are on the right side in (35.9%), bilateral in (34.4%) of cases and on the left side in (29.7%) of cases.
iv Distribution According to Anatomo-Pathological Aspect
According to macroscopic appearance, cystic looking tumors account for the majority of cases and according to microscopic appearance, malignant tumors predominate (Table 4). It should be noted that three patients did not have information on the macroscopic aspect. According to histological type, the most frequent tumors are cystadenocarcinoma (20.6%), mucinous cystadenocarcinoma (12.2%), serous cystadenocarcinoma (10.7%) and serous tumors (9.1%). The others were (6.9%) granulosa tumor, (5.3%) endometriosis, (4.6%) papillary and (3.1%) mucinous.
Table 4: Distribution of ovarian cancer tumors according to anatomical aspect (out of 131 cases collated at the Oncology Department of the Ibn Rochd Casablanca UHC 2010-2012).
|
Appearance of tumor |
The nature of the tumor |
Percentage (%) |
|
Macroscopic aspect |
Cystic Tumors |
50,4 |
|
Solid tumors |
30,5 |
|
|
Mixed Neoplasms |
16,8 |
|
|
Malignant tumors |
65,6 |
|
|
Microscopic appearance |
Borderline Neoplasms |
29,0 |
|
Benign Neoplasms |
5,4 |
v Evolution of the Pathology
Most patients in our series are being followed up and this represents (73.2%) of the cases. (26%) of the patients have recovered and only one case of death (0.8%) was noted. In our study, 74.8% of cases of metastases were noted in different locations including (44.3%) peritoneal carcinoma, (18.6%) pelvic extension, (18.4%) invasion of fallopian tubes, (5.3%) extra pelvic extension, (3.8%) invasion of pelvic lymph nodes, (3.1%) invasion of uterus and other locations of (6.5%).
Discussion
Ovarian cancer is one of the most common pelvic cancers in women [3]. It is not a very frequent cancer, unlike breast or cervical cancer, but it is a cancer characterized by extreme severity due to its diagnosis, which most often occurs at an advanced stage of the disease [11]. In our series of studies, the prevalence in Casablanca is 2.7%. The estimated incidence of ovarian cancer in Morocco was similar to that observed in Algeria (1.7 versus 1.5 per 100,000 women/year respectively) and slightly lower than that estimated in Tunisia (2.1 per 100,000 women/year) [12]. On the other hand, it was very low compared to that estimated in other developed countries (Europe) where the incidence was 13 per 100,000 [13]. In our series of studies, multiparity (64.3%), menopause (58.21%) and hypertension (77.78%) are the risk factors most frequently found in our patients. These factors have often been presented as risk factors favouring the occurrence of ovarian cancer in several studies [14, 15]. For other authors, it is rather advanced age, nulliparity, endometriosis, family history of breast cancer and prolonged use of hormone replacement therapy during menopause that constitute a risk factor [14].
In our series of studies, the mean age of ovarian cancer patients is 51.47 years with a median age of 52 years, confirming the data in the literature which reports a mean age of 49 and 48 years. 3 years which is relatively close to our results, as well as (31.3%) are over 50 years of age, which corresponds to the age of early menopause where the risk of developing ovarian cancer is increased, and only 13% of the population studied are under 40 years of age, so it is essentially a tumor of the postmenopausal woman [3, 11, 16]. Early diagnosis is difficult due to the lack of specific symptomatology and poor anatomical accessibility of the ovaries [14]. The age group most affected is between 50-60 years of age, which could explain the percentage of 58% of postmenopausal patients for other authors, it is rather the age group between 65-69 years of age that has been most affected [14]. We have found that the overall trend in incidence is favoured with age and therefore this factor should be taken into consideration if a screening program is to be initiated.
In Morocco, the frequency of this cancer is (4.7%) of all female cancers [11]. On a global scale, there is a lack of uniformity between the frequencies found in Africa (3.7%) and those found in sub-Saharan countries (11.5%), with a high incidence in developed countries (8 per 100,000) [11, 16, 17]. Although the estimated incidence and mortality of ovarian cancer appear to be higher in Morocco than in other countries of comparable socio-economic level, the estimated figures remain very low in comparison with those of developed countries. This should not lead to minimizing the scale of the problem in our country.
Concerning the origin of the patients, about half of the 78 cases or (59.5%) are from urban areas while 52 cases or (39.7%) are from rural areas. Given that the CHU drains essentially the region of Greater Casablanca, it is logical that most of our patients are from urban areas, and the Oncology Center of the CHU is a specialized structure which explains the high percentage of patients from rural areas. The predominant histological type is adenocarcinoma, which is consistent with the literature [11]. More than 70% of cases are found at advanced stages (III or IV) [3]. Epithelial tumors are the most common [18]. Metastases represent (12.32%) of ovarian tumors, 80% of which are of digestive origin [12]. It has been found that more than 70% of cases are found in advanced stages of metastasis (44.3% of cases have metastasis at the peritoneal level), which is consistent with the data in the literature [5]. The majority of tumors occurring in patients under 30 years of age (12 cases) were metastatic in 50% of cases and germ cell tumors in 33% of cases [19]. This finding could be partly explained by a different distribution of histological forms, some of which occur at a younger age and more frequently.
Conclusion
Ovarian cancer is relatively frequent but given the poor prognosis and high mortality rate, it is becoming a worrying public health reality in Morocco. Frequently found risk factors are multiparity, menopause as a personal history and high blood pressure as a medical history. The histological profile is that of an epithelial cystadenocarcinoma type tumor with a cystic appearance on the right side. Better biological investigation would allow its early diagnosis and reduction of its incidence.
Conflicts of Interest
None.
What's Known About This Subject?
i. The literature has already presented the epidemiological situation in developed countries.
ii. Daily hospital practice in various departments in Morocco seems to report lower ovarian cancer figures than in neighbouring countries.
What's New in This Study
This study is an original study since it reports, via a statistical study using the SPSS software, the various risk factors for ovarian cancer in the study population (multiparity, menopause, age, hypertension) as well as evaluating the epidemiological profile related to this pathology.
Author Contributions
MB: Manuscript writing, processing and statistical analysis. MB: Collection of data from medical records. SS and AB: Manuscript validation. TA and NA: Supervision, correction and validation of the manuscript. All authors contributed to the conduct of this work. All authors also report having read and approved the final version of the manuscript.
Acknowledgements
We would like to thank the Oncology Centre of the Ibn Rochd University Hospital of Casablanca, for its collaboration in the collection of clinical data and all those who participated in this study.
Article Info
Article Type
Research ArticlePublication history
Received: Wed 27, May 2020Accepted: Mon 15, Jun 2020
Published: Tue 30, Jun 2020
Copyright
© 2023 Benfateh Meriem. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.COR.2020.06.16
Figures & Tables
Table 1: Medical history among the 131 ovarian cancer patients in the Oncology Department of the Ibn Rochd University Hospital of Casablanca (2010-2012).
|
Medical history |
Number of cases |
Frequency (%) |
|
HTA |
14 |
77.78 |
|
Tuberculosis |
2 |
11.11 |
|
Valvulopathy |
2 |
11.11 |
|
Total |
18 |
100 |
Table 2: Surgical history among the 131 ovarian cancer patients in the Oncology Department of the Ibn Rochd University Hospital of Casablanca (2010-2012).
|
Surgical history |
Number of cases |
(%) |
|
Ovarian cyst adnexectomy |
4 |
25 |
|
Fibroma |
3 |
18,75 |
|
Hysterectomy |
1 |
6,25 |
|
Colorectal |
1 |
6,25 |
|
Cyst |
1 |
6,25 |
|
Crack |
1 |
6,25 |
|
Cholecystectomy |
1 |
6,25 |
|
Left breast cyst |
1 |
6,25 |
|
Hand fracture |
1 |
6,25 |
|
Eye problem |
1 |
6,25 |
|
Bladder cyst |
1 |
6,25 |
|
Total |
16 |
100 |
Table 3: Family history among the 131 ovarian cancer patients in the Oncology Department of the Ibn Rochd University Hospital of Casablanca (2010-2012).
|
Family history |
Number of cases |
% |
|
Breast Neo |
8 |
44,44 |
|
Brain tumor |
2 |
11,12 |
|
Neo stomach |
2 |
11,12 |
|
Colonist Neo |
2 |
11,12 |
|
Liver metastasis |
1 |
5,55 |
|
Neo liver |
1 |
5,55 |
|
pulmonary TBK |
1 |
5,55 |
|
Neo lung |
1 |
5,55 |
|
Total |
18 |
100 |
Table 4: Distribution of ovarian cancer tumors according to anatomical aspect (out of 131 cases collated at the Oncology Department of the Ibn Rochd Casablanca UHC 2010-2012).
|
Appearance of tumor |
The nature of the tumor |
Percentage (%) |
|
Macroscopic aspect |
Cystic Tumors |
50,4 |
|
Solid tumors |
30,5 |
|
|
Mixed Neoplasms |
16,8 |
|
|
Malignant tumors |
65,6 |
|
|
Microscopic appearance |
Borderline Neoplasms |
29,0 |
|
Benign Neoplasms |
5,4 |
References
- Doubeni CA, Doubeni AR, Myers AE (2016) Diagnosis and management of ovarian cancer. Am Fam Physician 93: 937-944. [Crossref]
- Abuidris DO, Weng HY, Elhaj AM, Eltayeb EA, Elsanousi M et al. (2016) Incidence and survival rates of ovarian cancer in low-income women in Sudan. Mol Clin Oncol 5: 823-828. [Crossref]
- Raherinantenaina F, Rakotomena SD, Emile Hasiniatsy NR, Rakototiana FA, Rafaramino F et al. (2015) A retrospective study of ovarian cancer with a median follow of 42 months. Pan Afr Med J 20: 211. [Crossref]
- Clarke Pearson DL (2009) Clinical practice screening for ovarian cancer. N Engl J Med 361: 170-177. [Crossref]
- Kurman J, Shih I (2010) The origin and pathogenesis of epithelial ovarian cancer. Am J Surg Pathol 34: 433-443. [Crossref]
- Dinh P, Harnett P, Piccart Gebhart MJ, Awada A (2008) New therapies for ovarian cancer: cytotoxics and molecularly targeted agents. Critical Rev Oncol Hematol 67: 103-112. [Crossref]
- Guppy AE, Nathan PD, Rustin GJS (2005) Epithelial Ovarian Cancer: A Review of Current Management. Clin Oncol (R Coll Radiol) 17: 399-411. [Crossref]
- Reid BM, Permuth JB, Sellers TA (2017) Epidemiology of ovarian cancer: a review. Cancer Biol Med 14: 9-32. [Crossref]
- Cancer Registry of the Greater Casablanca Region (RCRC) 2012.
- Rabat Cancer Registry 2005.
- Benhessou M, Anicet Boumba LM, Benchkrroun MN, Bouhya S, Ennaji M et al. (2016) Epithelial ovarian cancer in Morocco: epidemiology analysis on a series of 182 cases at the Ibn Rochd University Hospital of Casablanca Morocco. Int J Innov Sci Res 20: 153-162.
- Ferlay J, Soerjomataram I, Dikshit R, Eser S (2015) International Agency for Research on Cancer (IARC). globocan 2002. Cancer Incidence Mortality Prevalence Worldwide 136: 359-386.
- Li k, Hüsing A, Fortner RT, Tjønneland A, Hansen L et al. (2015) An epidemiologic risk prediction model for ovarian cancer in Europe: the EPIC study. Br J Cancer 112: 1257-1265. [Crossref]
- Pfeiffer RM, Park Y, Kreimer AR, Lacey JV Jr, Pee D (2013) Risk Prediction for Breast, Endometrial, and Ovarian Cancer in White Women Aged 50 Y or Older: Derivation and Validation From Population-Based Cohort Studies. PLoS Med 10: e1001492. [Crossref]
- Jozwicki W, Windorbska W, Brozyna AA, Jochymski C, Basta P et al. (2011) The analysis of receptor-binding cancer antigen expressed on siso cells (rcas1) immunoreactivity within the microenvironment of the ovarian cancer lesion relative to the applied therapeutic strategy 345: 405-414. [Crossref]
- Sando Z, Fouogue JT, Fouelifack FY, Fouedjio JH, Mboudou ET et al. (2014) Profile of breast and gynecological cancers in Yaoundé Cameroon. Pan Afr Med J 17: 28. [Crossref]
- Reid BM, Permuth JB, Sellers TA (2017) Epidemiology of ovarian cancer: a review. Cancer Biol Med 14: 9-32. [Crossref]
- Desai A, Xu J, Aysola K, Qin Y, Okoli C et al. (2014) Epithelial ovarian cancer: An overview. World J Transl Med 3: 1-8. [Crossref]
- Cancer Registry CHU HASSAN II of Fez, 2012.