
Table of Contents
Background
In 2011, the Institute of Medicine completed a landmark report on the health of lesbian, gay, bisexual, and transgender (LGBT) persons in the US. This report documented that across numerous health-related domains, including health risk behaviors and both mental and physical health, sexual minorities were at a distinct disadvantage compared to their heterosexual peers (IOM, 2011). As a result of this report, more federal surveys began to include measures of sexual orientation. In 2012, the Utah Behavioral Risk Factor Surveillance Survey (BRFSS) began to include indicators of sexual orientation in its data collection. This paper presents the first snapshot of sexual orientation disparities across multiple indicators of health in Utah, including alcohol use behaviors, asthma and cardiovascular health, and mental health.
Sexual minority women are more likely to report a variety of negative health-related outcomes (IOM 2011). These disparities in health are largely attributed to increased exposure to “minority stress,” broadly defined as the increased exposure to victimization, discrimination, and stress due to the excess stigma associated with non-heterosexual identities and behavior (Meyer, 2003). As a result of these negative exposures, sexual minority women have been found to have higher levels of depression (Marshal et al., 2011), negative coping behaviors such as alcohol use and misuse (Hughes, 2011), and poorer physical health outcomes including increased risk for cardiovascular and respiratory diseases (Blosnich, Lee, Bossarte, & Silenzio, 2013).
Previous research suggests that sexual minority health can vary across contexts. In particular studies have examined the extent to which health can vary depending on the cultural climate within a state. For example, studies have linked changes in LGBT-specific policies, such as the passing of same-sex marriage bans or the legalization of same-sex relationships to changes in the health of sexual minority women (Hatzenbuehler, 2014). Generally, a politically conservative climate has been shown to have negative effects on the health and well-being of sexual minorities (Everett B, 2013).
To our knowledge, no research has examined the health of sexual minority women in the state of Utah. Sexual minorities in Utah may have a health disadvantage similar to what has been observed in national data. While same-sex marriage became permanently legal in 2014, other challenges that are related to a larger religious and politically conservative climate persist.
Data
Data came from the 2012-2015 Utah Behavioral Risk Factor Surveillance System
(BRFSS) data set. In 2012, the BRFSS began including data on sexual orientation identity in addition to a wide-ranging set of other health-related outcomes. We focused on several important domains of women’s health including general perceived health, physical limitations, asthma, diabetes, alcohol use, and depression. Previously, these health indicators have been linked to sexual orientation disparities in national data sets. Our sample was restricted to women who answered the sexual identity measure questions, as well as all of our health-indicator items. Our final sample size was 19343 women, 260 of whom identified themselves as gay or lesbian, 156 as bisexual, and 156 as “other.” Individuals who indicated “don’t know” or did not answer were excluded.
Health indicators were derived from survey items that asked respondents if they had ever been diagnosed with diabetes or pre-diabetes (yes=1, no=0), , or asthma (yes=1, no=0) by a medical provider. We also assessed whether or not respondents reported being “limited in any way in any activities because of physical, mental, or emotional problems“(yes=1, no=0). Self-rated health was measured using an item that asked participants,” Would you say that in general your health is:” with possible answers from “excellent” (1) to “poor” (5). We constructed a measure of alcohol use based on the question: “During the past 30 days, how many days per week or per month did you have at least one drink of any alcoholic beverage such as beer, wine, a malt beverage or liquor?” Based on the responses, we calculated how many of the past 30 days a respondent had consumed any alcohol. We also included a binge drinking indicator, which measured whether or not the respondent had consumed 5 or more alcoholic drinks on a single occasion during the past month.
Finally, we included two mental health indicators: 1) whether a health provider had ever told the respondents that they had a depressive disorder (including depression, major depression, dysthymia, or minor depression); and 2) a count of the days in the past month during which respondents experienced mental health problems, derived from the survey item: “Now thinking about your mental health, which includes stress, depression, and problems with emotions, for how many days during the past 30 days was your mental health not good?”
We compiled descriptive statistics and performed bivariate tests to examine differences by sexual identity in the prevalence of the assessed health conditions in the state of Utah. We compared means between non-sexual minority (heterosexual) and sexual minority women (bisexual, gay/lesbian, other). We also compared each sexual minority identity group to heterosexual women to capture variability within the sexual minority group. To assess whether differences were statistically significant we estimated F-tests that took our complex survey design into account. All statistics were weighted to produce population estimates and adjusted for year of the survey using the “svy” commands in Stata 14.
Results
Table 1 summarizes our results, which showed that sexual minority women were at a health disadvantage for many but not all of the outcomes we evaluated. Looking at our physical/general health outcomes, we observed no differences by sexual orientation for having “any” health limitation, or for having diabetes or pre-diabetes. However, we did see that sexual minority women report a higher prevalence of asthma (17%) compared to heterosexual women (12%). This difference was most pronounced between heterosexual and lesbian women: 20% of lesbians reported being diagnosed with asthma compared to 12% of heterosexual women. Turning to self-rated health, on average, sexual minority women reported higher scores indicating perceptions of their health that were worse than perceptions reported by hetero-sexual women. These disparities were largest when we compared women who identified their sexuality as “other” to heterosexual women.
Turning to alcohol use, the results showed that sexual minority women reported more days of drinking and a higher prevalence of binge drinking than their heterosexual peers. Table 1, Panel B illustrates that the disparity was largest between lesbian and heterosexual women: 68% of lesbians compared to 35% of heterosexual women reported binge drinking.
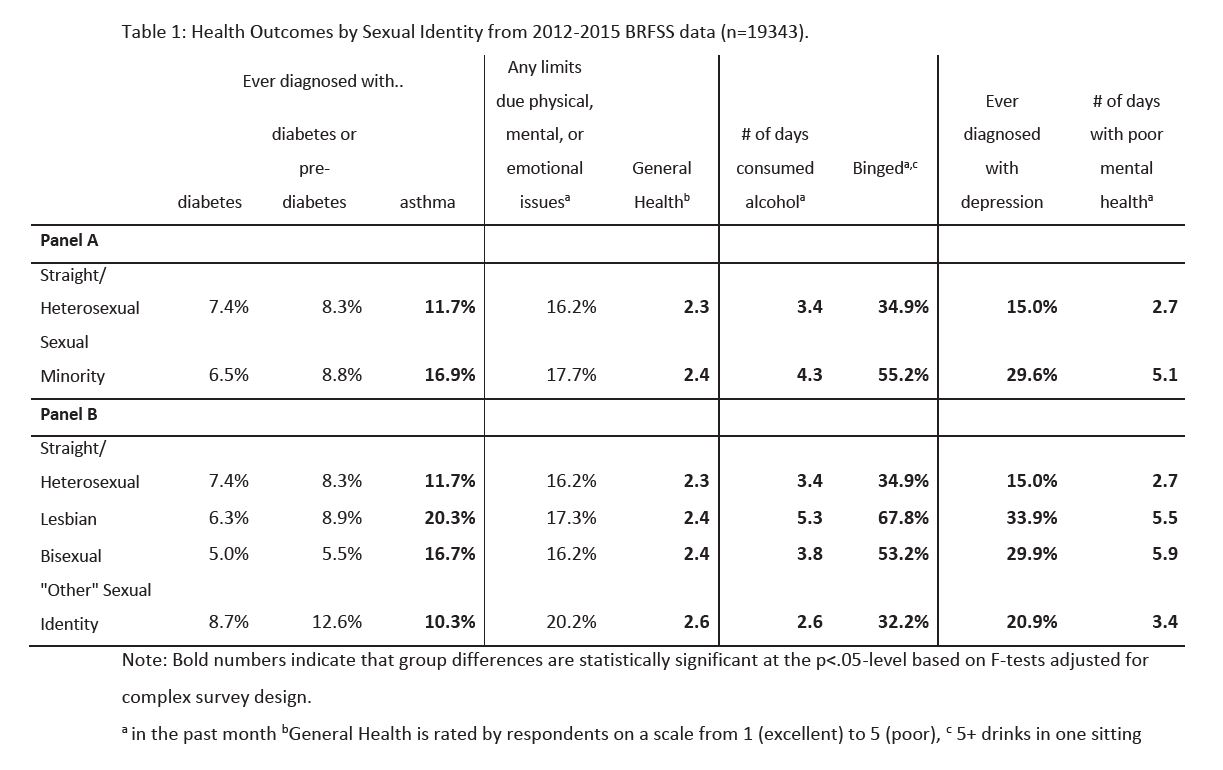
Looking at mental health outcomes, sexual minority women reported a higher prevalence of depression (30%) and almost double the number of days they were limited by poor mental health (m=5.1), compared to heterosexuals (15%, m=2.7). Rates of depression and number of days limited by mental health were similar between bisexual and lesbian women. Mental health disparities were even larger among sexual minority women ages 18-24, 50% of whom reported depression compared to 14% of heterosexual women in the same age group.
Discussion
Our results are in line with other research that has found sexual minority women to report poorer health outcomes and engage in increased risk behaviors compared to heterosexual women. While we did not examine all seven domains of health, our results show disadvantages in both emotional and physical health for sexual minority women. Due to data limitations, we were unable to demonstrate disadvantages in other health domains.
However, the mental health disparities we observed are particularly striking given the high rates of suicide in Utah, especially among youth (https://ibis.health.utah.gov/indicator/complete_profile/SuicDth.html). It is possible that this increase in suicide rates may be due to the marginalization of sexual minority individuals within Utah’s dominant religion, coupled with the policies, which often are perceived as discriminatory, and which are related to sexual minority status in the dominant religion in Utah. Religious leaders of both Utah’s dominant religion and other religious groups have begun efforts to deal with this marginalization and policies; some of these efforts have been more successful than others.
We also saw higher rates of alcohol use among sexual minority women, particularly lesbian-identified women. This difference may reflect engagement in negative coping behaviors related to stressors and depression. It may also reflect that this group of women may be less connected to religious institutions in Utah that prohibit drinking; thus, disparities between the groups may be easier to detect. Regardless, the high rates of binge drinking among lesbian women in Utah (68%) suggest a need to reduce engagement in this and other health risk behaviors.
More encouraging, our results showed no differences in physical limitations or diabetes. However, we did find that sexual minority women are more likely to report having been diagnosed with asthma. This finding is in line with other work that has found disparities in asthma among persons in same-sex relationships compared to those in opposite-sex relationships.
Recommendations
We recommend policies and practices that remove stigma, as well as an increase of mental health and support services for sexual minority women to minimize the impact of health issues on domains of health. This has the potential to curb binge drinking in sexual minority populations. Future analyses will show whether changes in policies
(for example, the recent legalization of same sex marriage) will be reflected in diminishing health disparities over time.
References
- Blosnich, J. R., Lee, J. G. L., Bossarte, R., & Silenzio, V. M. B. (2013). Asthma Disparities and Within-Group Differences in a National, Probability Sample of Same-Sex Partnered Adults. American Journal of Public Health, 103(9), e83–e87.
- Everett B, Sexual Orientation Identity Change and Depressive Symptoms: A Longitudinal Analysis. J Health Soc Behav. 2015 March ; 56(1): 37–58. doi:10.1177/0022146514568349
- Hatzenbuehler, M. L. (2014). Structural Stigma and the Health of Lesbian, Gay, and Bisexual Populations. Current Directions in Psychological Science, 23(2), 127–132.
- Hughes, T. (2011). Alcohol-Related Problems Among Sexual Minority Women. Alcoholism Treatment Quarterly, 29(4), 403–435.
- Institute of Medicine (IOM) Committee on Lesbian, Gay, Bisexual, and Transgender Health Issues and Research Gaps and Opportunities. (2011). The Health of Lesbian, Gay, Bisexual, and Transgender People: Building a Foundation for Better Understanding. Washington (DC): National Academies Press (US). Retrieved from http://www.ncbi.nlm.nih.gov/books/NBK64806/
- Marshal, M. P., Dietz, L. J., Friedman, M. S., Stall, R., Smith, H. A., McGinley, J., Thoma, B.C., Murray, P.J., D’Augelli, R., Brent, D. A. (2011). Suicidality and Depression Disparities Between Sexual Minority and Heterosexual Youth: A Meta-Analytic Review. Journal of Adolescent Health, 49(2), 115–123.
- Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychological Bulletin, 129(5), 674-697.
Citation
Geist C & Everett B. (2019). Sexual Minority Women’s Health in Utah. Utah Women’s Health Review. doi: 10.26054/0KC8V40BZQ.
