

- Departments of Neurosurgery, Zagazig University, Zagazig, Egypt,
- Departments of Neurosurgery, AlMokatam Insurance Hospital, Cairo, Egypt.
Correspondence Address:
Mahmoud M. Taha
Departments of Neurosurgery, AlMokatam Insurance Hospital, Cairo, Egypt.
DOI:10.25259/SNI-266-2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Amr AlBakry, Mahmoud M. Taha, Hassan A. Al Menshawy. Cranial migration of lumboperitoneal shunt: A case report and review of literature. 28-Jun-2019;10:124
How to cite this URL: Amr AlBakry, Mahmoud M. Taha, Hassan A. Al Menshawy. Cranial migration of lumboperitoneal shunt: A case report and review of literature. 28-Jun-2019;10:124. Available from: http://surgicalneurologyint.com/surgicalint-articles/9436/
Date of Submission
21-Apr-2019
Date of Acceptance
01-Jun-2019
Date of Web Publication
28-Jun-2019
Abstract
Background: Lumboperitoneal shunt is an easy and effective way of managing benign intracranial hypertension (BIH) and other causes of increased intracranial pressure. Yet, it is associated with a relative high failure rate. Proximal migration of the shunt is rare and only few cases have been reported.
Case Description: Here, we present a case of a 16-year-old female, diagnosed with BIH, who had a proximal shunt migration 4 months after surgery and was managed conservatively, along with the review of literature.
Conclusion:
Keywords: Cranial, Lumboperitoneal shunt, Migration, Proximal
INTRODUCTION
Lumboperitoneal shunt is an established treatment for the management of idiopathic intracranial hypertension.[
CASE REPORT
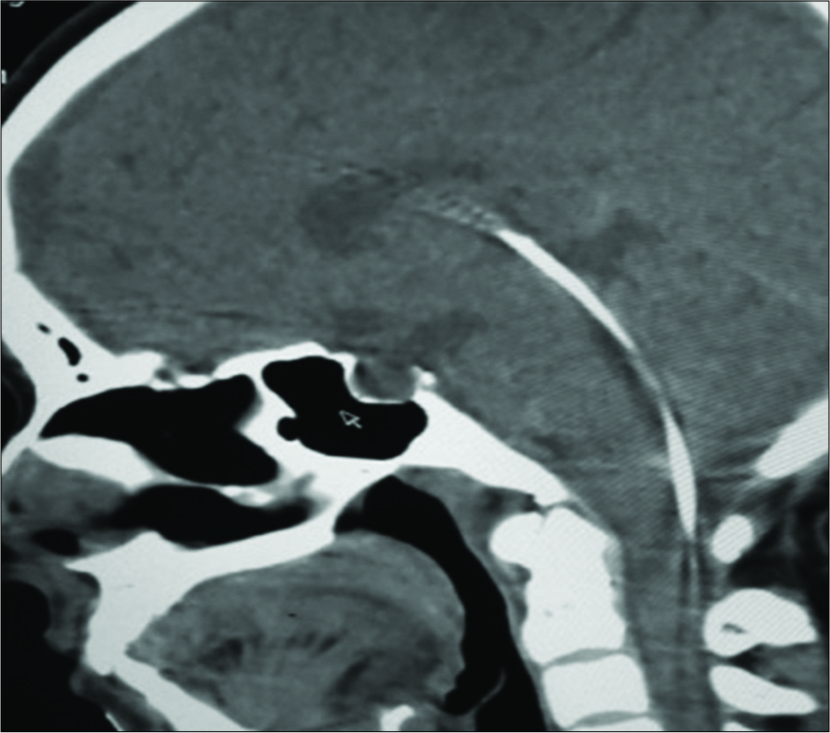
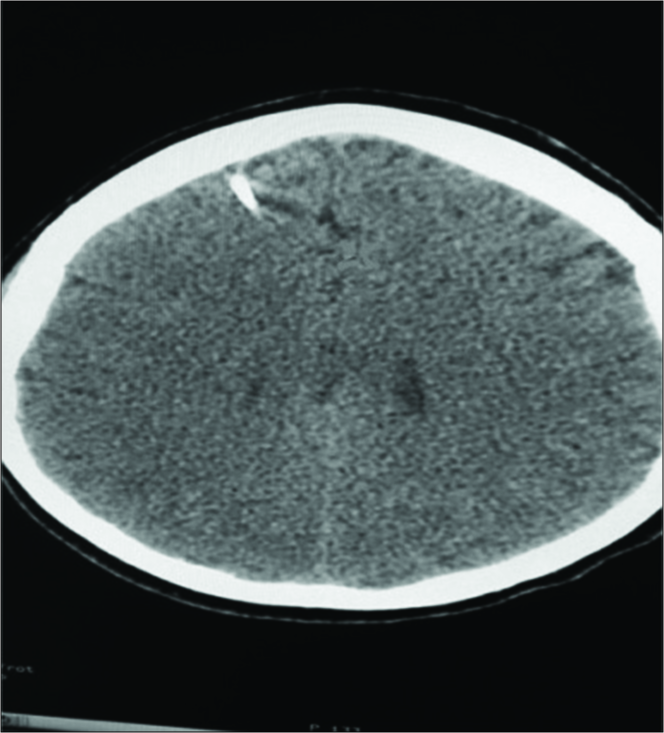
A 16-year-old right-handed female complaining of headache and diminution of vision sought for ophthalmologic consultation and was found to have the 2nd degree papilledema, was then referred to our department. Full analysis of the complaint and full neurological examination were done. Computed tomography (CT) brain was free. A provisional diagnosis of pseudotumor cerebri was made. Spinal manometry revealed an elevated cerebrospinal fluid (CSF) pressure. A course of conservative measures (diuretics, steroids, and lumbar puncture) was decided, with no significant improvement. We decided to go for surgical management and a lumboperitoneal shunt was inserted. All patient’s symptoms improved postoperative, and papilledema improved in postoperative follow-up. Four months later, the patient started to complain of sudden severe back pain with recurrence of the headache, and the patient had a different complain of “something hitting the head from inside” in the patient’s own words. The patient went to an orthopedic surgeon to seek for the cause of the low back pain, and she ordered a pelvis and lumbar X-ray. The lumbar X-ray showed straightening of lumbar lordosis and a diagnosis of muscular low back pain was made and the patient was treated accordingly with improvement of her back pain. Accidentally, she found the proximal end of the shunt migrating upward and the patient was referred again to us. We ordered a full spine CT scan and a CT brain and we found the shunt migrating proximally up to the frontal horn of the right ventricle [


DISCUSSION
Lumboperitoneal shunt is a simple and effective procedure for the treatment of pseudotumor cerebri. Lumboperitoneal shunt accounts for 40% of the CSF shunting procedures. Possible complications of the shunt are obstruction, overdrainage, mechanical failure, catheter migration, catheter fracture, abdominal complications, lumbospinal complications, infections, or other less commonly reported complications.[
Possible mechanisms for proximal shunt migration are inappropriate fixation and increased intra-abdominal pressure and alterations in the CSF pressure in synchronization with the respiratory pressure.[
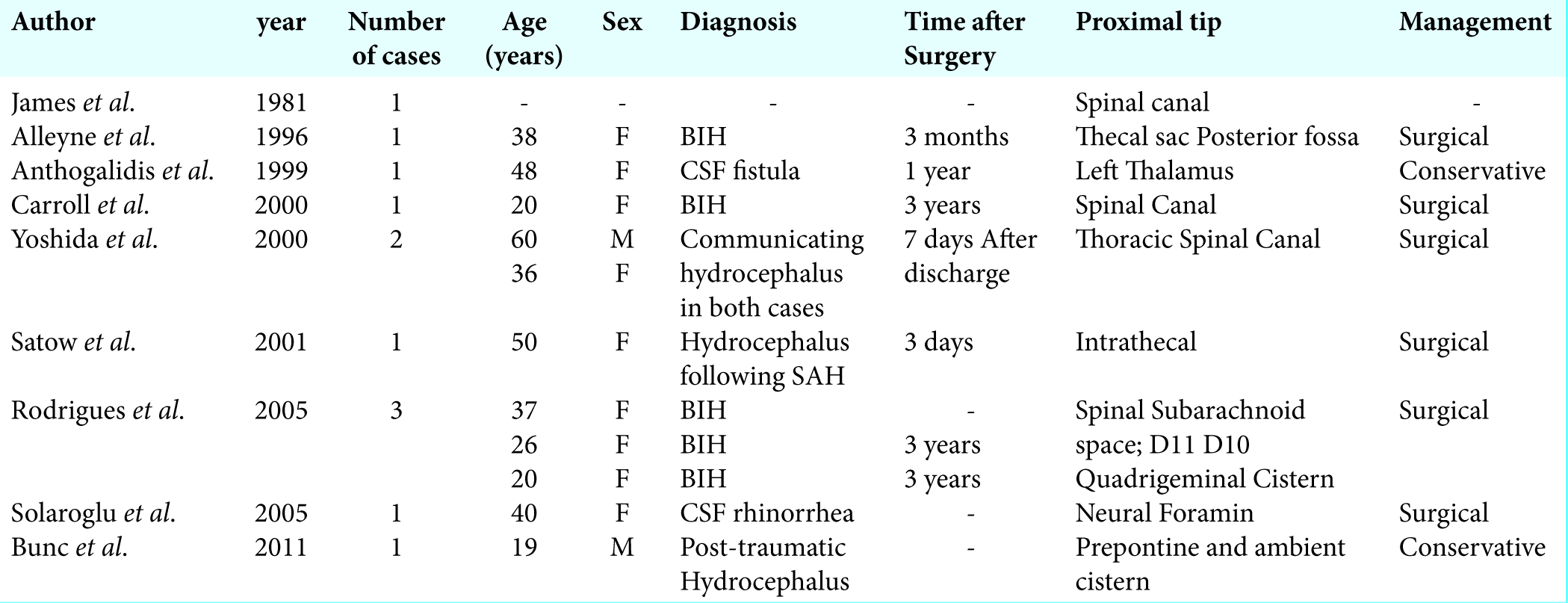
Yoshida et al. reported two cases of communicating hydrocephalus where the shunt migrated into the thoracic theca, the shunt was pulled back to place and a reservoir chamber was added to fix it in place and patients remained symptom free.[
In the case reported by Bunc et al., they had an LP shunt placed for the management of posttraumatic hydrocephalus with neck infection, which interfered with implantation of a VP shunt. The patient’s symptoms started to improve followed by deterioration, radiological investigation showed the shunt to migrate to the ambient and prepontine cistern, removing the shunt from its new site was risky, especially that it was not causing any symptoms and the decision was to leave it in place and insert a VP shunt.[
In Alleyne et al., a 38-year-old female had a lumboperitoneal shunt inserted for BIH; 2 months later, the shunt migrated proximally into the thecal sac with recurrence of symptoms, surgical intervention was done, and the shunt was pulled back to place with improvement of the symptoms; 3 months later, symptoms recurred and the shunt was found to migrate into the posterior fossa and surgical removal was difficult and the plan was to leave it in place and insert a VP shunt.[
Carroll and Jakubowski reported that a shunt placed for BIH which migrated entirely into the spinal canal and was removed through a laminectomy.[
Rodrigues et al. reported three cases of LP shunt migration; a 37-year-old female had an LP shunt which migrated into the thecal sac to opposite D11 following a road traffic accident and was removed through a laminectomy and a new shunt was inserted and fixed tightly to rectus abdominus and lumbar fascia; a 26-year-old female had an LP shunt placed for BIH, 3 years later, the shunt migrated to opposite D10 after normal vaginal delivery and was retrieved and a new one was put, a 20-year-old female had an LP shunt for the management of BIH, and after an attack of acute bronchitis and severe cough, the shunt migrated into the 4th ventricle and was left in place and a new one was applied.[
The case reported by Solaroglu et al. was a 40-year-old female with CSF rhinorrhea following surgical removal of a clival tumor. Postoperatively, the proximal end of the shunt was found inside the foramina with severe radicular pain, the patient was taken to theater and the shunt was pulled back.[
Anthogalidis et al. reported a 48-year-old female with CSF fistula, who had the shunt slipped after 1 year into the left thalamus. The shunt was a one-piece valveless shunt. Removing the shunt was associated with a high risk of injury, so decision was to leave it in place and insert a new VP shunt.[
The case by Satow et al. was a 50-year-old female who had hydrocephalus following SAH. An LP shunt was inserted and 3 days later, no improvement in symptoms or CT imaging was noticed. The shunt migrated intrathecally and the peritoneal end slipped out of the peritoneal cavity. Shunt revision was done and repositioned with proper fixation. They conveyed the shunt migration to the movement of the spine which acts like a driving force pushing the shunt from its place.[
CONCLUSION
Although it is associated with a high complication rate, lumboperitoneal shunt is very effective in the management of many disorders. All measures to avoid these complications are a must. One of the most common complications is shunt migration. Although many mechanisms explaining shunt migration have been hypothesized, yet the mainstay for preventing shunt migration remains proper fixation of the shunt.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Alleyne CH, Shutter LA, Colohan AR. Cranial migration of a lumboperitoneal shunt catheter. South Med J. 1996. 89: 634-6
2. Anthogalidis EI, Sure U, Hellwig D, Bertalanffy H. Intracranial dislocation of a lumbo-peritoneal shunt-catheter: Case report and review of the literature. Clin Neurol Neurosurg. 1999. 101: 203-6
3. Bunc G, Vorsic M, Ravnik J, Velnar T. Proximal migration of a lumboperitoneal shunt into the prepontine and ambiens cisterns. Clin Neurol Neurosurg. 2011. 113: 75-7
4. Carroll TA, Jakubowski J. Intrathecal migration of a lumboperitoneal shunt. Br J Neurosurg. 2000. 14: 496-7
5. El-Saadany WF, Farhoud A, Zidan I. Lumboperitoneal shunt for idiopathic intracranial hypertension: Patients’ selection and outcome. Neurosurg Rev. 2012. 35: 239-43
6. James HE, Tibbs PA. Diverse clinical applications of percutaneous lumboperitoneal shunts. Neurosurgery. 1981. 8: 39-42
7. Jusué-Torres I, Hoffberger JB, Rigamonti D, Di Rocco C, Turgut M, Jallo G, Martínez-Lage JF.editors. Complications specific to lumboperitoneal shunt. Complications of CSF Shunting in Hydrocephalus: Prevention, Identification, and Management. United States: Cham Springer International Publishing; 2015. p. 203-11
8. Rodrigues D, Nannapaneni R, Behari S, Prasad M, Herwadkar A, Gerber CJ. Proximal migration of a lumboperitoneal unishunt system. J Clin Neurosci. 2005. 12: 838-41
9. Satow T, Motoyama Y, Yamazoe N, Isaka F, Higuchi K, Nabeshima S. Migration of a lumboperitoneal shunt catheter into the spinal canal case report. Neurol Med Chir (Tokyo). 2001. 41: 97-9
10. Solaroglu I, Okutan O, Beskonakli E. Foraminal migration of a lumboperitoneal shunt catheter tip. J Clin Neurosci. 2005. 12: 956-8
11. Yoshida S, Masunaga S, Hayase M, Oda Y. Migration of the shunt tube after lumboperitoneal shunt two case reports. Neurol Med Chir (Tokyo). 2000. 40: 594-6

