
Abstract
▴ Dutasteride, a potent inhibitor of type 1 and 2 5α-reductase, reduced dihydrotestosterone levels by >90% in 85% of patients following 1 years’ administration of oral dutasteride 0.5 mg/day.
▴ A combined analysis of three placebo-controlled clinical studies conducted in patients with benign prostatic hyperplasia (BPH) found sustained improvements in American Urological Association-Symptom Index scores and urinary flow rate and a 57% decrease in the risk of acute urinary retention throughout the 2-year treatment period (all p < 0.001 vs placebo).
▴ Total prostate and transition zone volume were also reduced (both p < 0.001), as was the risk of BPH-related surgery (by 48%).
▴ A nonblind extension study found that dutasteride maintains efficacy for up to 4 years. Dutasteride monotherapy maintained symptom relief following combination treatment with dutasteride and tamsulosin in all patients but those with severe symptoms.
▴ Dutasteride was generally well tolerated. Impotence, reduced libido, gynaecomastia and ejaculation disorder occurred significantly more often in dutasteride than placebo recipients, but incidence was generally low. With the exception of gynaecomastia, incidence consistently decreased over time.
Similar content being viewed by others


Benign prostatic hyperplasia (BPH) is characterised by nonmalignant enlargement of the prostate gland, which exerts pressure on the prostatic urethra and obstructs urinary flow.[1] It is the most prevalent urological disorder in men, and is likely to remain a frequently occurring disorder as a result of the aging population and the tendency for the incidence of BPH to increase with age.[2] For example, the incidence of prostatic enlargement at autopsy increases from ≊25% in 50-year-old men to >80% in men aged 80 years (reviewed by Gisleskog et al.[3]). Similarly, longitudinal studies conducted in the US found that ≊60% of men aged ≥60 years and ≊80% of men aged ≥80 years had a diagnosis of BPH (reviewed in Drugs & Aging[4]).


The development of BPH is thought to be dependent on the androgen dihydrotestosterone (DHT).[1,3] DHT is converted from testosterone by the enzyme 5α-reductase of which there are two forms. Type 1 5α-reductase is found primarily in the skin and liver, but has also been found in prostatic tissue in BPH.[5] Type 2 5α-reductase is found in the prostate.[1,3]
Current medical treatments for BPH include the use of α-adrenoceptor antagonists and 5α-reductase inhibitors to relieve symptoms and improve urinary flow.[2] α-Adrenoceptor antagonists act directly on prostatic smooth muscle to decrease muscle tone.[6] 5α-Reductase inhibitors decrease the size of the prostate.[7]
It has been proposed that lowering DHT levels further, via the inhibition of both types 1 and 2 5α-reductase, may enhance the reduction of BPH symptoms.[3] Dutasteride (Avodart®Footnote 1) is a potent inhibitor of both isoforms of 5α-reductase. Although dutasteride is currently being investigated in the treatment of prostate cancer,[8] this review focuses on the pharmacodynamics, pharmacokinetics, clinical efficacy and tolerability of orally administered dutasteride in patients with BPH.
1. Pharmacodynamic Profile
The effects of dutasteride on 5α-reductase inhibitory activity have been investigated in vitro,[3,9,10] while studies of the effects of dutasteride on DHT, testosterone, luteinising hormone and prostate-specific antigen (PSA) levels have generally been assessed in volunteers[11] or patients with BPH.[12–15] The effects of dutasteride on spermatogenesis,[16] lipid profile and bone metabolism[17] have also been investigated in volunteers.
5α-Reductase Inhibitory Activity
-
Dutasteride, 4-azasteroid, is a selective and potent inhibitor of types 1 and 2 5α-reductase.[3,9,10] In vitro, dutasteride has an inhibition constant (Ki) of 6 nmol/L for type 1 5α-reductase and 7 nmol/L for type 2 5α-reductase.[9] Compared with finasteride, which has a Ki of 360 nmol/L, dutasteride is 45 times more potent at inhibiting type 1 5α-reductase, with a more rapid onset of action (≊5 times).[9,10,18] For type 2 5α-reductase inhibition, dutasteride is calculated to be 2.5-fold more potent than finasteride.[18]
Effects on Levels of DHT and Other Hormones
The effect of dutasteride on serum hormone levels has been investigated in three randomised, placebo-controlled, dose-ranging studies conducted in male volunteers[11] or patients with BPH.[12–14] The study conducted in volunteers (n = 48) was single-blind and volunteers received a single dose of dutasteride (0.01–40mg), finasteride 5mg or placebo.[11] The double-blind studies, conducted in patients with a prostate volume ≥30mL or an International Prostate Symptom Score (IPSS) ≥8, were of 4 (n = 53)[12] or 24 (n = 399)[14] weeks’ duration.
Data regarding changes in serum DHT and testosterone levels have also been taken from a combined analysis of three large (n = 4325), randomised, double-blind, placebo-controlled, multicentre, studies each of 2 years’ duration in patients with BPH (the ARIA trials; see section 3 for further study design details).[15]
-
Dutasteride produced dose-related reductions in mean DHT levels in volunteers[11] and in patients receiving dutasteride once daily for 4[12] or 24[14] weeks. Reductions tended to plateau at doses >0.5mg (the recommended dose). DHT levels were significantly reduced from baseline by 72–95% following single-dose administration of dutasteride 1–40mg in volunteers (all p ≤ 0.001 vs placebo)[11] and by 52.9–98.4% after repeat administrations of dutasteride 0.05–5 mg/day for 24 weeks in patients (all p < 0.001 vs placebo).[14]
-
Reductions in DHT levels are rapid and sustained.[19,20] DHT levels decreased by a median 91% at 1 month in the ARIA trials.[20] This reduction persisted (93–94%) throughout the 24 months of treatment and was maintained at 4 years.[19]
-
Dutasteride reduced DHT levels in the majority of patients.[15,20] A combined analysis of the ARIA trials found that a ≥90% reduction in serum DHT levels was achieved in 58% of dutasteride recipients at 1 month, in 85% at 12 months[15] and in 81% of recipients at 2 years.[20]
-
Dutasteride at doses ≥0.5 mg/day is superior to finasteride 5 mg/day in reducing mean levels of DHT.[12,14] Reductions in DHT levels were greater with dutasteride ≥0.5 mg/day than with finasteride 5 mg/day in the 4-week study (≥90% vs 76%; p < 0.05)[12] and in the 24-week trial (≥94.7% vs 70.8%; p < 0.001).[14]
-
Dutasteride increased serum testosterone levels,[15] an effect observed within the first month of treatment.[20] In the combined analysis of the ARIA trials, serum testosterone increased from baseline by a mean 24.5% with dutasteride (p < 0.001 vs baseline) and 5.4% with placebo at 24 weeks.[15] Analysis of a subset of the total ARIA trials population found that dutasteride-induced increases in testosterone that occurred following 1 month of treatment remained relatively constant throughout the remaining treatment period.[20] When stated, increases in testosterone generally stayed within the normal range and were not regarded as clinically significant.[13,14]
-
Dutasteride- and finasteride-induced increases in testosterone were broadly similar.[13,14] Mean testosterone levels in the 24-week study increased from baseline by 5.6–21.2% in patients receiving dutasteride 0.01–5.0mg compared with a 13.6% increase in finasteride recipients and a 4.2% increase in patients receiving placebo. Significant increases compared with placebo were observed for dutasteride at the 0.5 mg/day dosage (21.2%; p < 0.05).[14]
-
Luteinising hormone and androstenedione also increased with dutasteride administration, but these increases were not regarded as clinically significant.[13,14,20] In the 24-week study, mean increases in luteinising hormone of 0.3 and 0.2 mIU/mL in patients receiving dutasteride 0.5 mg/day and finasteride 5 mg/day did not differ significantly from the mean decrease observed with placebo (0.9 mIU/mL).[14] In the ARIA trial, median increases in luteinising hormone remained relatively stable over the treatment period.[20] Androstenedione levels were mildly increased from baseline (by 20%) in the 4-week study.[13]
Effects on PSA Levels
-
PSA levels decreased following dutasteride treatment.[15,21] An individual analysis of one of the ARIA trials (n = 674) found that mean baseline measures of total and free PSA in dutasteride recipients were 4.4 and 0.9 ng/mL and that these values were reduced by a mean 45.7% and 55.5% following 12 months of treatment.[21] In contrast, total PSA levels increased a mean 8.4% from 4.1 ng/mL at baseline and free PSA increased a mean 14.0% from 0.9 ng/mL at baseline with placebo. The ratio of free-to-total PSA showed a similar trend, reducing by a mean 6.7% in dutasteride recipients and increasing by a mean 6.7% in placebo recipients.[21] The combined analysis of the ARIA trials found significant between-group differences in serum PSA levels (p < 0.001) at 24 months and that, compared with baseline, mean serum PSA levels decreased by 52.4% with dutasteride treatment and increased by 15.8% with placebo treatment (both p < 0.001 vs baseline).[15]
Effects on Spermatogenesis
-
Dutasteride and its associated reductions in DHT had no clinically significant effect on spermatogenesis in a randomised, double-blind study in volunteers (n = 99).[16] Compared with that of placebo recipients, semen volume was significantly (p value not stated) decreased by 19–24% at 24–52 weeks for dutasteride 0.5 mg/day and for finasteride 5 mg/day recipients at 24–48 weeks. Sperm motility was also reduced by 7–15% in both treatment groups at treatment weeks 24–28 and 48–52 and at weeks 20–24 of follow-up. Reductions from baseline in sperm count were observed in both treatment groups. None of these changes met the criteria for clinical significance, with the exception of a 40% reduction in finasteride recipients at 24–48 weeks which resolved at weeks 48–52 of treatment.[16]
Effects on Bone Metabolism and Lipid Profile
-
Dutasteride 0.5 mg/day for 1 year had no clinically significant effect on bone density, bone metabolism or lipid profile in volunteers.[17] All treatment groups, including placebo, demonstrated an upward trend in mean cholesterol and low density lipoprotein during the study. At week 8 of the 24-week follow-up, mean serum total cholesterol levels were higher in dutasteride- than finasteride-recipients (p = 0.038). By week 24 of follow-up, all lipid levels were similar to baseline, except for increased triglyceride levels in the placebo and dutasteride groups, but these were not considered clinically significant.[17]
2. Pharmacokinetic Profile
The pharmacokinetic profile of dutasteride has been investigated in two randomised, single-blind (n =48)[3,10,11,22] or double-blind (n = 399),[14] placebo-controlled, dose-ranging trials (see section 1 for study details). Pharmacokinetic information has also been taken from prescribing information.[23,24] The pharmacokinetic profile has been described using noncompartmental methods[11] and using a two-compartmental model with linear and nonlinear elimination pathways operating in parallel.[3,22]
Absorption and Distribution
-
Dutasteride is quickly absorbed and demonstrates dose proportionality in mean maximum plasma concentrations (Cmax) following oral administration.[10,23] Bioavailability is 60% (range 40–94%) following oral administration.[23,24] After administration of dutasteride 0.1–40mg, the dutasteride absorption lag time (tlag) was 0.32 hours, according to the two-compartmental model.[3,22] Single doses of dutasteride 0.1–40mg resulted in Cmax values of 0.6–166 ng/mL.[10] Cmax may be reduced by 10–15% with concurrent food administration, but this is not clinically significant.[23,24] Following a single administration of dutasteride at the recommended dose of 0.5mg, the time to maximum serum concentrations is 1–3 hours.[23,24]
-
Dutasteride steady-state plasma concentrations also demonstrate dose proportionality and are reached after ≊3–6 months.[14] Mean steady-state dutasteride serum concentrations were ≊40 ng/mL following 24 weeks of receiving 0.5 mg/day of dutasteride.[14] With daily administration, dutasteride serum concentrations reach 65% of steady-state after 1 month and ≊90% after 3 months.[23]
-
Dutasteride is highly (>99.5%) protein plasma bound, mainly to plasma albumin (99%) and α1 acid glycoprotein (96.6%).[23,24]
-
The drug has a large volume of distribution and is extensively distributed into central and peripheral compartments, including semen.[22–24] Using standard noncompartmental methods, the steady-state volume of distribution is 300–500L.[11,14] According to the two-compartmental model, volumes of distribution of dutasteride in the central and peripheral compartments were 173L and 338L.[3,22] The mean semen dutasteride concentration was 3.4 ng/mL (range 0.4–14 ng/mL) following 12 months of dutasteride 0.5 mg/day. On average, 11.5% of the serum dutasteride concentration was found in the semen after 12 months.[24]
Metabolism and Elimination
-
Dutasteride is extensively metabolised and excreted primarily in the faeces.[23,24] In vitro, dutasteride is metabolised by cytochrome P450 (CYP) 3A4.[24] At steady state, a mean 5.4% (range 1.0–15.4%) of the 0.5 mg/day dose was excreted in the faeces as unchanged dutasteride. A further 7–39% was excreted in the faeces as either one of three monohydrated metabolites or as a dihydroxylated metabolite. Six minor metabolites each accounted for <5% of the excreted dose. Less than 0.1% of the dose is detected in the urine as unchanged dutasteride and ≊55% of the dose is unaccounted for.[23,24]
-
The elimination of dutasteride is dose-dependent and is best described by a linear and nonlinear pathway operating in parallel.[3,22,23] At high dutasteride plasma concentrations (daily doses >1mg), the linear pathway is the main route of elimination, resulting in a clearance of 0.58 L/h. At low dutasteride concentrations (<3 ng/mL), dutasteride is eliminated rapidly using both linear and nonlinear pathways.[3,22,23] In patients receiving dutasteride 0.01–5.0 mg/day for 24 weeks, dutasteride elimination was nonlinear and had a clearance rate of 0.83–1.54 L/h.[14] During repeat administration of dutasteride 0.5 mg/day, the linear elimination pathway dominates and the elimination half-life (t1/2) is 3–5 weeks.[23]
Special Populations
-
No dosage adjustment is necessary in the elderly or in patients with renal impairment.[23,24] In a single-dose study, age had no significant clinical effects on the pharmacokinetic profile of dutasteride 0.5mg except for prolonging t1/2 in volunteers >50 years. Mean t1/2 was ≈170 hours in volunteers aged 20–49 years, ≈260 hours in those aged 50–69 years and ≈300 hours in those aged ≥70 years.[24] Because dutasteride is extensively metabolised before being eliminated and only a small proportion of the dose is eliminated via renal clearance, it is expected that hepatic impairment, but not renal impairment, will result in greater exposure to dutasteride (see section 5).[23,24]
Drug Interactions
-
Dutasteride pharmacokinetics are not significantly affected by concomitant exposure to α1-adrenoceptor antagonists (e.g tamsulosin and terazosin) digoxin or warfarin; however, serum concentrations may increase in the presence of CYP 3A4 inhibitors such as ritonavir, ketoconazole, verapamil, diltiazem, cimetidine and ciprofloxacin.[23–25] In vitro, there is no displacement from plasma protein binding sites following concomitant administration of dutasteride and either warfarin, diazepam or phenytoin.[24] In volunteers, a single 5mg dose of dutasteride followed 1 hour later by 12g of cholestyramine had no affect on the relative bioavailability of dutasteride.[26]
3. Therapeutic Trials
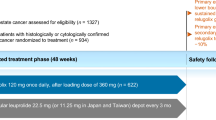
Data regarding the therapeutic efficacy of dutasteride in treating BPH have been primarily obtained from three large (n = 4325), randomised, double-blind, placebo-controlled, multicentre studies each of 2 years’ duration.[15,27–33] Two of the studies were conducted in the United States (ARIA 3001 and ARIA 3002) and the third (ARIA 3003) was conducted in 19 countries.[15] Combined data from the three trials have been presented in abstracts[27,28,31] or have been fully published.[15,33]
Data from randomised studies have also been used to compare the efficacy of dutasteride in patients with varying prostate volumes and these results have been published in abstracts.[29,30] Long-term, nonblind, extension studies have been conducted in patients from the ARIA trials who opted to begin receiving or continue to receive dutasteride. Two of the 3 trials (ARIA 3001 and ARIA 3002) are complete and results for ARIA 3002 are available via an abstract and conference proceedings.[34] Pooled results for both trials are available via media release[35] and company newsletter (data on file[19]; results from pooled analysis are discussed in preference to results from the ARIA 3002 study). In the ARIA 3001 and 3002 extension studies, 778 patients previously assigned to placebo and 792 patients previously assigned to dutasteride received dutasteride 0.5 mg/day for two years. Finally, the Symptom Management After Reducing Therapy (SMART) study was a double-blind, multicentre study involving 327 patients that investigated the efficacy of both dutasteride in combination with tamsulosin, an α1-adrenoceptor antagonist and dutasteride monotherapy post tamsulosin withdrawal; results are available as an abstract[36] and a conference report.[37]
In all randomised trials, patients had a prostate volume of ≥30cm3 and a score ≥12 on the American Urological Association-Symptom Index (AUA-SI)[15] or IPSS.[36] In the ARIA trials, patients had a clinical diagnosis of BPH, were aged ≥50 years, and had a urine flow rate (Qmax) of ≤15 mL/sec and a serum PSA level between 1.5 and 10.0 ng/mL.[15] In the ARIA trials, exclusion criteria were a history of prostate cancer, prostate surgery, or acute urinary retention within 3 months of screening. Patients receiving an α-adrenoceptor antagonist within the last 4 weeks or a 5α-reductase inhibitor were also excluded.[15]
In all controlled trials, patients underwent a 1-month, single-blind, placebo run-in period prior to randomisation.[15,36] In the ARIA trials, patients were randomised to receive either dutasteride 0.5 mg/day (n = 2167) or placebo (n = 2158). In the SMART trial, patients received dutasteride 0.5 mg/day in combination with tamsulosin 0.4 mg/day for 36 weeks or dutasteride 0.5 mg/day in combination with tamsulosin 0.4 mg/day for 24 weeks followed by dutasteride 0.5 mg/day and placebo for a further 12 weeks.[36] In all of the studies, dutasteride was administered once daily.[15,34,36]
In the combined analysis of the ARIA trials, efficacy analyses were carried out for the intention-to-treat population. In the fully published study, results using last observation carried forward data and data from study completers were similar, but only data from study completers were reported.[15] Primary endpoints in the ARIA trials were changes in the AUA-SI score from baseline and the incidence of acute urinary retention (defined as urination requiring catheterization). Secondary endpoints included changes in total prostate volume, transition zone volume (both measured by transrectal ultrasonography), Qmax and the incidence of surgical intervention (specific procedures not stated), in addition to a number of pharmacodynamic-related endpoints (section 1). Changes in quality of life (measured on the BPH Impact Index) have also been reported.[27,29,30,33] Endpoints in the extension study included symptom improvement rated on the AUA-SI and change in Qmax.[34]
The efficacy population was not reported in the SMART trial[36] and was not clearly stated in the extension study.[34] In the SMART trial, the primary endpoint was the number of patients with either no change or improvements in urinary symptoms as a result of continuation or discontinuation of tamsulosin from week 24, and was measured by subjective assessment at week 30.[37]
Monotherapy
-
Dutasteride and placebo significantly improved AUA-SI scores (a primary endpoint) and Qmax from baseline; however, dutasteride was superior to placebo (all p < 0.001).[15,27] At 24 months, mean AUA-SI scores were 12.2 in dutasteride and 14.7 in placebo recipients, corresponding to mean reductions of 4.5 and 2.3 points.[15] Mean Qmax was 12.5 and 11.2 mL/sec in the dutasteride and placebo groups, corresponding to mean increases of 2.2 and 0.6 mL/sec.[15]
-
Dutasteride improved AUA-SI scores and increased Qmax regardless of baseline total prostatic or transitional zone volume.[29,30] Stratification of patients based on prostate and transitional zone volume revealed improvements in both measures in all groups, except for AUA-SI scores in patients with a transitional zone volume <10cm3 (no p values given). Furthermore, improvements in Qmax tended to increase in proportion to enlarging total prostatic volume.[29]
-
Dutasteride significantly reduced total prostate volume and transition zone volume, unlike placebo (figure 1).[15,27] At study completion, mean total prostate volume had decreased by 14.6cm3 (25.7%) from baseline to 41.2 cm3 in dutasteride recipients (p < 0.001 vs baseline), but had increased by 0.8cm3 (1.7%) to 54.1cm3 in placebo recipients (p < 0.04 vs baseline).[15]
-
The difference between dutasteride and placebo was apparent from 1 month for Qmax (p < 0.01), total prostate volume and transition zone volume (both p < 0.001) and from 6 months in the combined analysis for AUA-SI scores (p < 0.001).[15] In one of the ARIA trials, a significant difference in AUA-SI scores was demonstrated after 3 months (p = 0.016 vs placebo).[27] For all measures this difference persisted throughout the 24-months of treatment.[15]
-
Dutasteride reduced the incidence of acute urinary retention (a primary endpoint) and BPH-related surgery.[15,27,28,30] Compared with placebo, dutasteride reduced the rate of urinary retention (1.8% vs 4.2% [39 vs 90 episodes]) and the rate of BPH-related surgical interventions (2.2% vs 4.1% [47 vs 89 episodes)] in patients with BPH.[15] The relative risk for acute urinary retention was 0.43 (95% CI 0.29–0.62), and that for BPH-related surgery was 0.52 (95% CI 0.37–0.74), translating to risk reductions with dutasteride treatment of 57% and 48% relative to placebo (both p < 0.001).[15,27,28] Kaplan-Meier estimates revealed that the differences between dutasteride and placebo for acute urinary retention and BPH-related surgery increased over time.[15]
-
Dutasteride reduced prostatic volume and decreased the risk of acute urinary retention and BPH-related surgery in patients with a slightly enlarged prostate (prostate volume of 30–40cm3 or ≥40cm3).[30] Compared with placebo, dutasteride reduced prostate volume by 26.1% and 26.9% in patients with a baseline prostate volume of 30–40cm3 and ≥40cm3 over the 2-year treatment period (both p < 0.001). Similarly, compared with placebo, the risk of acute urinary retention was reduced by 85% and 55% and BPH-related surgical interventions by 35% and 52% in dutasteride-treated patients with a prostate volume of 30–40cm3 or ≥40cm3.[30]
-
Dutasteride improved quality of life regardless of baseline prostate or transition zone volume.[27,29,30,33] Overall, the mean reduction from baseline in BPH Impact Index score at 6 months was 0.63 and 0.41 for dutasteride and placebo recipients (p = 0.003). Improvements were maintained throughout the study period, with mean reductions at endpoint of 1.0 and 0.26 for dutasteride and placebo recipients (p < 0.001).[27,33] Stratification of BPH Impact Index scores by prostatic and transitional zone volume revealed mean reductions in BPH Impact Index scores for all groups, except in patients with a transition zone volume <10cm3, where a small increase was observed.[29] Likewise, another analysis found significant improvements from placebo in BPH Impact Index in patients with a baseline prostatic volume of 30–40cm3 or ≥40cm3 who received dutasteride (both p < 0.001).[30]

Efficacy of dutasteride in men with benign prostatic hyperplasia (BPH). Mean changes from baseline in total prostatic volume (TPV) and transitional zone volume (TZV) in patients with BPH treated with dutasteride 0.5 mg/day (n = 2167) or placebo (2158) for 24 months.[15] Results from three randomised, double-blind, multicentre studies were reported as combined data. * p < 0.04 vs baseline; ** p < 0.001 vs baseline.
Extension Study
-
Dutasteride provides continued symptom improvement for up to 4 years, according to pooled analysis.[19,35] Mean improvement from baseline in AUA-SI score at month 48 was 5.3 in patients who received placebo for 2 years followed by dutasteride for 2 years and 6.1 in those who received dutasteride for 4 years.[19] Similarly, improvements from baseline occurred in Qmax (26.1% and 35.6%), total prostate volume (20.7% and 26.2%) and transition zone volume (14.2% and 20.0%) in these groups of patients.[19]
Combined with an α1-Adrenoceptor Antagonist
-
Dutasteride in combination with tamsulosin rapidly improved urinary symptoms for 24 weeks, an outcome that was maintained with dutasteride monotherapy in patients with moderate BPH symptoms.[36,37] After 4 weeks’ therapy, 66% of patients reported subjective improvements in their urinary symptoms. By week 30, 77% of 149 patients receiving dutasteride monotherapy and 91% of 154 patients who continued to receive dutasteride in combination with tamsulosin reported that they felt that urinary symptoms were unchanged or had improved compared with week 24 (95% CI –0.18, –0.04). Furthermore, improvements in symptoms were maintained in 93% and 96% of patients receiving dutasteride monotherapy and dutasteride combination therapy.[36,37]
-
Patients with more severe symptoms received greater benefit from an extended dutasteride plus tamsulosin combination therapy period.[37] Of the patients with a baseline IPSS ≥20, 42% who received dutasteride monotherapy after 24 weeks reported worse symptoms at week 30 compared with 14% of patients continuing to receive combination treatment.[37]
4. Tolerability
The tolerability of dutasteride has been investigated in combination with efficacy in the three ARIA trials,[15] the SMART trial[36,38] and the nonblind ARIA extension studies[34,35] (section 3). The tolerability data from the three ARIA trials have been presented in combined analyses.[15,31,32] Events were generally sexually related; however, other adverse events were also reported. Tolerability data have also been reported in a dose-ranging study[14] (section 3), a 1-year study comparing dutasteride 0.5 mg/day (n = 813) and finasteride 5 mg/day (n = 817) in patients with BPH[38] and in a pharmacokinetic study comparison of tamsulosin and terazosin administered with or without dutasteride.[25]
General Tolerability
-
Dutasteride and placebo were similarly well tolerated.[14,15,31] Overall, in the ARIA trials, similar proportions of dutasteride or placebo recipients experienced any adverse event (77% vs 75%) or a drug-related adverse event (19% vs 14%).[15] In each treatment group 9% of patients withdrew because of adverse events, and drug-related withdrawals occurred in 4% and 3% of dutasteride and placebo recipients. Severe adverse events occurred in 330 of 2167 dutasteride recipients (15%) and 301 of 2158 placebo recipients (14%).[31]
-
Dutasteride continued to be well tolerated in the 2-year extension studies.[34] The incidences of adverse events, drug-related or severe adverse events, and drug-related treatment withdrawals were similar to those observed in the placebo-controlled trials.[34]
-
Ear-nose-throat infections, malaise, fatigue, headaches, musculoskeletal pain and dizziness were the most frequent general adverse events.[14,15] In the 24-week phase II study, there were no significant differences in the occurrence of these adverse events between patients receiving dutasteride 0.01–5.0 mg/day, finasteride 5.0 mg/day or placebo.[14] Likewise, in the ARIA trials, ear-nose-throat infections, musculoskeletal pain and upper respiratory infections were the most frequently reported adverse events.[15]
-
Dutasteride had no significant effect on laboratory measurements.[14] In one phase II study, haematology, blood chemistry, liver function, renal function and lipid profile demonstrated normal variation over the 24-week treatment and 16-week follow-up period. The proportion of patients with any laboratory abnormality was broadly similar across the dutasteride 0.01–0.05 mg/day, finasteride 5 mg/day and placebo treatment groups. Similarly, there were no significant changes detected in blood pressure, pulse, ECG and cardiac rhythm for any of the treatment groups.[14]
Sexually Related Adverse Events
-
Sexually related adverse events, though uncommon, occurred significantly more frequently in dutasteride than placebo recipients.[15] For the entire study period of the ARIA trials, significant differences favoured placebo (all p < 0.001) for impotence (7.3% vs 4.0% of patients), decreased libido (4.2% vs 2.1%), gynaecomastia (2.3% vs 0.7%) and ejaculation disorder (2.2% vs 0.8%). These sexual events were more common with dutasteride than placebo after 1 year (all p < 0.01), but not after 2 years, when only gynaecomastia was more frequent (1.3% vs 0.3%; p < 0.001).[15]
-
The incidence of impotence, decreased libido and ejaculation disorder tended to decrease with continued dutasteride treatment.[32] As demonstrated in figure 2, the incidence of these events reduced most markedly during the first 6–12 months of dutasteride treatment.[32]
-
The incidence of gynaecomastia tended to show small increases with continual treatment with dutasteride in the ARIA studies,[32] but decreased during the nonblind phase of treatment.[35] As figure 2 indicates, the incidence of gynaecomastia increased during the first 18 months of dutasteride treatment but decreased in the final 6 treatment months. The incidence of gynaecomastia in placebo recipients was relatively stable.[32] In the extension study, the incidence of gynaecomastia decreased from 1.9% during the first year of nonblind treatment to 1% during the second year.[35]
-
Consistent with the ARIA trials, the incidence of other sexually related adverse events in the extension study decreased over the 2-year treatment period.[35] Compared with the first year of nonblind treatment, the incidence of impotence (1.6% vs 0.4%), decreased libido (0.5% vs 0%) and ejaculation disorders (0.3% vs 0.1%) decreased in the second year of nonblind dutasteride therapy.[35]
-
The incidence of sexually related adverse events did not significantly differ between dutasteride or finasteride recipients in the 1-year fixed-dose trial.[38] The only adverse events classified as drug-related by the investigator and which occurred with an incidence of >2% were impotence in 7% of dutasteride and 8% of finasteride recipients and decreased libido (5% and 6%). Ejaculation disorder and gynaecosmastia occurred in 1% of patients in each treatment group.[38]

The incidence of various sexually related adverse events in patients with benign prostatic hyperplasia treated with either (a) dutasteride or (b) placebo.[32] Data were taken from a combined analysis of three multicentre, randomised, double-blind studies in which patients were randomised to receive dutasteride 0.5 mg/day or placebo for 2 years.
Combined with an α1-Adrenoceptor Antagonist
-
Dutasteride was well tolerated when administered in combination with tamsulosin.[36] In the SMART trial (see section 3 for further details), coadministration of dutasteride and tamsulosin for 36 weeks was as well tolerated as coadministration of these drugs for 24 weeks followed by dutasteride plus placebo for 12 weeks. In each treatment regimen, 4% of patients withdrew from the study because of an adverse event.[36] There were no significant differences in the incidence of sexually related adverse events.[38]
-
Another study found a reduced incidence of adverse events when dutasteride was coadministered with tamsulosin or terazosin compared with tamsulosin or terazosin monotherapy (see section 2.1 for further details).[25] The incidence of adverse events, including headache, dizziness, musculoskeletal pain, orthostasis, nausea and emesis, was 18% and 35% when dutasteride was coadministered with tamsulosin or terazosin and 29% and 67% when the latter drugs were administered as monotherapy.[25]
5. Dosage and Administration
Dutasteride is available as a soft capsule containing a 0.5mg dose and should be administered orally, once daily.[23] Capsules should be swallowed whole and can be taken with or without food.[23] No dose adjustment is necessary in the elderly, or in patients with renal impairment. Dutasteride should be administered with caution to patients with mild-to-moderate hepatic impairment and is contraindicated in patients with severe hepatic impairment, and in patients with hypersensitivity to dutasteride or other 5α-reductase inhibitors.[23] Dutasteride is also contraindicated in women, children and adolescents, who must avoid skin contact with the drug. Should contact be made with a leaking capsule, the affected area should be immediately washed because dutasteride is absorbed through the skin.[24]
6. Dutasteride: Current Status
Dutasteride has been approved in several countries for the treatment of moderate-to-severe symptoms of BPH and the reduction in risk of acute urinary retention and surgery in patients with moderate-to-severe BPH.[39–42] Dutasteride 0.5 mg/day reduces DHT levels by >90% in 85% of patients whilst simultaneously improving AUA-SI score and Qmax and reducing the incidence of acute urinary retention and associated surgical interventions in large placebo-controlled trials. Furthermore, dutasteride has been shown to reduce total prostate and transition zone volume and improve quality of life. Dutasteride is well tolerated and is associated with a low incidence of drug-induced, including sexually related, adverse events.
Notes
Use of tradenames is for product identification purposes only and does not imply endorsement.
References
Frye S. Inhibitors of 5alpha-reductase. Curr Pharm Des 1996; 2: 59–84
Tammela T. Benign prostatic hyperplasia: practical treatment guidelines. Drugs Aging 1997; 10(5): 349–66
Gisleskog PO, Hermann D, Hammarlund-Udenaes M, et al. A model for the turnover of dihydrotestosterone in the presence of the irreversible 5alpha-reductase inhibitors GII98745 and finasteride. Clin Pharmacol Ther 1998; 64: 636–47
Eri LM, Tveter KJ. Treatment of benign prostatic hyperplasia: a pharmacoeconomic perspective. Drugs Aging 1997; 10(2): 107–18
Shirakawa T, Okada H, Fujisawa M, et al. Messenger RNA levels and enzyme activities of 5 alpha-reductase type 1 and 2 in the human benign prostatic hyperplasia tissues [abstract no. 461]. 32nd Annual Meeting of the International Continence Society; 2002 27–30 August; Heidelberg, Germany
Cooper KL, McKiernan JM, Kaplan SA. alpha-adrenoceptor antagonists in the treatment of benign prostatic hyperplasia. Drugs 1999; 57(1): 9–17
Wilde MI, Goa KL. Finasteride: an update of its use in the management of symptomatic benign prostatic hyperplasia. Drugs 1999; 57(4): 557–81
GlaxoSmithKline. GlaxoSmithKline steps up efforts to recruit patients for clinical trial of dutasteride for prostate cancer [online]. Available from URL: http://www.gsk.com [Accessed 2003 Jul 2]
Tian G, Mook RA, Moss ML, et al. Mechanism of time-dependent inhibition of 5alpha-reductases by -4-azasteroids: toward perfection of rates of time-dependent inhibition by using ligand-binding energies. Biochemistry (Mosc) 1995; 34: 13453–9
Frye SV, Bramson HN, Hermann DJ, et al. Discovery and development of GG745, a potent inhibitor of both isozymes of 5 alpha-reductase. In: Borchardt RT, et al, editor. Integration of Pharmaceutical Discovery and Development: Case Studies. New York: Plenum Press, 1998; 11: 393–422
Bramson HN, Hermann D, Batchelor KW, et al. Unique preclinical characteristics of GG745, a potent dual inhibitor of 5AR. J Pharmacol Exp Ther 1997; 282: 1496–502
Hermann DJ, Wilson TH, Morrill BB. A 28-day evaluation of GI198745 (GG745), a potent dual 5-alpha reductase inhibitor, in BPH patients [abstract no. 1227]. J Urol 1997; 157 (4 Suppl.): 315
Clark RV, Gabriel H, Hermann DJ, et al. Hormonal effects of GI198745, a novel 5 alpha reductase inhibitor [abstract no. P3-380]. 81st Annual Meeting of the Endocrine Society; 1999 12–15 June; San Diego, 520
Clark RV, Hermann DJ, Gabriel H, et al. Almost complete suppression of dihydrotestosterone in men with benign prostatic hyperplasia by GI198745, a novel, dual 5alpha reductase inhibitor. North Carolina: GlaxoSmithKline (data on file)
Roehrborn CG, Boyle P, Nickel JC, et al. Efficacy and safety of a dual inhibitor of 5-alpha-reductase types 1 and 2 (dutasteride) in men with benign prostatic hyperplasia. ARIA 3001, ARIA 3002 and ARIA 3003 study investigators. Urology 2002 Sep; 60: 434–41
Clark RV, Huffman CS, Haberer LJ, et al. Marked suppression of dihydrotestosterone by dutasteride has no adverse effect on spermatogenesis in healthy men [abstract no. P2-673]. 84th Annual Meeting of the Endocrine Society; 2002 June 19–22; San Francisco, 478
Clark RV, Matsumoto AM. Bone density, bone metabolism markers and lipid profiles in healthy men are unaffected by the novel dual 5A-reductase inhibitor dutasteride [abstract no. 1796]. J Urol 2003; 169 Suppl.: 479. Plus poster presented at the 98th Annual Meeting of the American Urological Association; 2003 April 26 to May 1; Chicago
Critchley P, Brin S, Komas B, et al. Dutasteride: investigators brochure (US). GlaxoSmithKline, 2002
GlaxoSmithKline. Safety and efficacy of Avodart for the treatment of benign prostatic hyperplasia: open-label results from the 4-year trial. GlaxoSmithKline, 2003; (data on file)
Roehrborn CG, Andriole G, Nickel C, et al. Effect of the dual 5alpha-reductase inhibitor dutasteride on endocrine parameters [abstract no. 1049]. J Urol 2002 Apr; 167 (Suppl.): 266–7
Andriole G, Roehrborn CG, Nickel C, et al. Effect of the dual 5alpha-reductase inhibitor, dutasteride, on serum total PSA, free PSA and the ratio of F/T PSA [abstract no. 844]. J Urol 2002 Apr; 167 Suppl.: 209–10
Gisleskog PO, Hermann D, Hammarlund-Udenaes M, et al. The pharmacokinetic modelling of GI198745 (dutasteride), a compound with parallel linear and nonlinear elimination. Br J Clin Pharmacol 1999; 47: 53–8
GlaxoSmithKline UK. Avodart [online]. Available from URL: http://emc.vhn.net [Accessed 2003 Jun 10]
GlaxoSmithKline. Avodart: Prescribing information. North Carolina: GlaxoSmithKline, 2002
Clark RV, Haberer LJ, Horton JR, et al. No evidence of drug interactions between G1198745, a novel dual 5 alpha reductase inhibitor, and alpha 1 adrenergic antagonists. J Urol 2000 Apr; 163 Suppl.: 219–20
Clark RV, Hermann DJ, Gabriel H, et al. Effective suppression of dihydrotestosterone by GI198745, a novel, dual 5 alpha reductase inhibitor [abstract no. 1037]. J Urol 1999; 161(4): 268
Boyle P, Roehrborn C, Andriole G, et al. The impact of dutasteride, a novel 5-alpha reductase inhibitor, on the hallmarks of BPH progression and outcomes [abstract no. 418]. Eur Urol 2002; 41(Suppl. 1): 107. Plus poster presented at the 17th Congress of the European Association of Urology; 2002 Feb 23–26; Birmingham
Boyle PP, Siami P, Wachs BH, et al. Effect of dutasteride on the risk of acute urinary retention and the need for surgical treatment. J Urol 2002 Apr; 167 Suppl.: 372
Roehrborn C, Ramsdell J, Siami P, et al. Prostrate volume at baseline predicts the margin of therapeutic response with the 5-alpha-reductase inhibitor, dutasteride [abstract no. 1483]. J Urol 2002 Apr; 167 Suppl.: 373
Boyle P, Roehrborn C, Marks L, et al. Early use of dutasteride arrests prostate growth, improves clinical parameters and prevents complications in men with benign prostatic hyperplasia [abstract no. 1789]. J Urol 2003; 169 (4 Suppl.): 477
Roehrborn CG, Andriole G, Nickel C, et al. Effect of dutasteride, a novel dual 5-alpha-reductase inhibitor, on BPH related signs and symptoms [abstract no. 1043]. J Urol 2002 Apr; 167 (4 Suppl.): 265
Carson C, Harkaway R, Marks L, et al. Effect of maximal dihydrotestosterone suppression with dutasteride on sexual function and gynecomastia [abstract no. 1790]. J Urol 2003; 169 (4 Suppl.): 478. Plus poster presented at the 98th Annual Meeting of the American Urological Association; 2003 April 26 to May 1; Chicago
O’Leary MP, Roehrborn C, Andriole G, et al. Improvements in benign prostatic hyperplasia-specific quality of life with dutasteride, the novel dual 5alpha-reductase inhibitor. BJU Int. 2003; 92(3): 262–6
Roehrborn CG, Boyle P, Nicket JC, et al. Dutasteride provides sustained and continued improvement in BPH-related symptoms over 4 years [abstract no. 1292]. J Urol 2003; 169 (4 Suppl.): 333. Plus oral presentation at the 98th Annual Meeting of the American Urological Association; 2003 April 26 to May 1; Chicago
GlaxoSmithKline. New data evaluating four years of treatment with Avodart (dutasteride) support long-term efficacy and tolerability in men with BPH [online]. Available from URL: http://www.gsk.com [Accessed 2003 Apr 2]
Barkin J, Guimaraes M, Do Castelo V, et al. Dutasteride provides sustained symptom relief following short term combination treatment with tamsulosin [abstract no. 1481]. J Urol 2002 Apr; 167 Suppl.: 372
Poole RM. Dutasteride: rapid benefit in patients with BPH. Inpharma 2002 Mar 30; 1331: 9–10
Andriole GL, Kirby R. Safety and tolerability of the dual 5alpha-reductase inhibitor dutasteride in the treatment of benign prostatic hyperplasia. Eur Urol 2003; 44(1): 82–8
GlaxoSmithKline. GlaxoSmithKline announces global launch of new treatment for benign prostatic hyperplasia [online]. Available from URL: http://www.gsk.com [Accessed 2003 Mar 20]
EU market news. Inpharma 2002 Aug 10; 1350: 18
GlaxoSmithKline. GlaxoSmithKline Receives European Approval for Avodart for Benign Prostatic Hyperplasia [online]. Available from URL: http://www.gsk.com [Accessed 2003 Sep 5]
GlaxoSmithKline. FDA Approves Avodart, the First Dual-Acting 5 Alpha-Reductase Inhibitor for Benign Prostatic Hyperplasia (BPH) [online]. Available from URL: http://www.gsk.com [Accessed 2003 Sep 5]
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Evans, H.C., Goa, K.L. Dutasteride. Drugs Aging 20, 905–916 (2003). https://doi.org/10.2165/00002512-200320120-00005
Published:
Issue Date:
DOI: https://doi.org/10.2165/00002512-200320120-00005