
Abstract
Objective: This study aimed to assess the pharmacokinetics and tolerability of once-and twice-daily frovatriptan given for 6 days, a regimen that has previously been reported to reduce the incidence and severity of menstrual migraine when administered during the perimenstrual period.
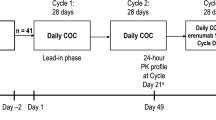
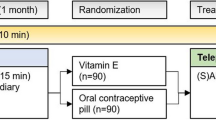
Methods: This was a double-blind, placebo-controlled, two-period crossover study carried out in healthy premenopausal female volunteers aged ≥18 years (equal number taking or not taking estrogen-containing contraceptives [ECCs]) who were admitted to a clinical pharmacology unit. Women alternately received frovatriptan once daily (day 1: 5mg; days 2–6: 2.5mg) and twice daily (day 1: 5mg [10mg total]; days 2–6: 2.5mg [5mg total]) in a randomized treatment sequence. Dosing was also random with respect to the menstrual cycle. Whole blood samples were obtained on days 1 and 6 (predose and at 0.5, 1, 2, 4, 6, 8, 12 [before evening dose], 13, 14, 16 and 18 hours post-dose) and on days 2–5 (samples were taken before the morning dose). A final sample was drawn at 24 hours after the last treatment on day 6. A fully validated liquid chromatography assay coupled to a tandem mass spectroscopy assay measured drug concentrations (simultaneous measurement of frovatriptan and its metabolites). Pharmacokinetic parameters were determined using a noncompartmental approach. Safety and tolerability were measured by monitoring adverse events, haematology and biochemistry, vital signs, ECG results and physical examination findings.
Results: Twenty-six healthy women participated in the study and 24 (12 ECC users and 12 ECC nonusers) completed the study. One ECC user during period 1 and one nonuser during period 2 withdrew before completion; both were taking frovatriptan once daily. Most women were White (n = 21), three were Black, and one each was Hispanic or Asian; mean ±SD age was 25.4 ±4.9 years; and mean ±SD weight was 61.9 ±6.5 kg. For both once-and twice-daily dosing, time to reach maximum blood concentration (Cmax) [tmax] was in the range of 2–4 hours. The loading dose enabled steady state (defined as constant trough blood concentration [Cmin]) to be reached by day 2 with both regimens. Geometric mean Cmax and area under the blood concentration-time curve from 0 to 12 hours (AUC12) were higher with twice-versus once-daily dosing (day 1: p <0.02; day 6: p <0.001 for both). Cmin was lower with once-(range 0.8–1.7ng/mL) versus twice-daily frovatriptan (range 1.7–3.6ng/mL). The ratio of Cmax: Cmin on days 1 and 6 was lower with twice-than with once-daily dosing, indicating less fluctuation in frovatriptan blood concentrations. ECC users had 26–68% higher Cmax and AUC from 0 to 24 hours values than nonusers on days 1 and 6 (p <0.02); the clinical relevance of this is not known. Both dosing regimens were well tolerated; one incident of vomiting and one of headache were rated as moderate, with all other adverse events being rated as mild.
Conclusion: Both frovatriptan regimens achieved steady-state therapeutic blood concentrations by day 2. Twice-daily dosing maintained more consistent drug concentrations than once-daily dosing and was well tolerated.







Similar content being viewed by others

References
Dzoljic E, Sipetic S, Vlajinac H, et al. Prevalence of menstrually related migraine and nonmigraine primary headache in female students of Belgrade University. Headache 2002 Mar; 42(3): 185–93
Granella F, Sances G, Allais G, et al. Characteristics of menstrual and nonmenstrual attacks in women with menstrually related migraine referred to headache centres. Cephalalgia 2004 Sep; 24(9): 707–16
Couturier EG, Bomhof MA, Neven AK, et al. Menstrual migraine in a representative Dutch population sample: prevalence, disability and treatment. Cephalalgia 2003 May; 23(4): 302–8
Diener HC, Ryan R, Sun W, et al. The 40-mg dose of eletriptan: comparative efficacy and tolerability versus sumatriptan 100mg. Eur J Neurol 2004 Feb; 11(2): 125–34
Nett R, Landy S, Shackelford S, et al. Pain-free efficacy after treatment with sumatriptan in the mild pain phase of menstrually associated migraine. Obstet Gynecol 2003 Oct; 102(4): 835–42
Allais G, Acuto G, Cabarrocas X, et al. Efficacy and tolerability of almotriptan versus zolmitriptan for the acute treatment of menstrual migraine. Neurol Sci 2006 May; 27Suppl. 2: S193–7
Silberstein SD, Elkind AH, Schreiber C, et al. A randomized trial of frovatriptan for the intermittent prevention of menstrual migraine. Neurology 2004 Jul 27; 63(2): 261–9
Mannix LK, Files JA. The use of triptans in the management of menstrual migraine. CNS Drugs 2005; 19(11): 951–72
Moschiano F, Allais G, Grazzi L, et al. Naratriptan in the short-term prophylaxis of pure menstrual migraine. Neurol Sci 2005; 26Suppl. 2: S162–6
Newman L, Mannix LK, Landy S, et al. Naratriptan as short-term prophylaxis of menstrually associated migraine: a randomized, double-blind, placebo-controlled study. Headache 2001 Mar; 41(3): 248–56
Newman LC, Lipton RB, Lay CL, et al. A pilot study of oral sumatriptan as intermittent prophylaxis of menstruation-related migraine. Neurology 1998; 51(1): 307–9
Buchan P, Keywood C, Wade A, et al. Clinical pharmacokinetics of frovatriptan. Headache 2002 Apr; 42Suppl. 2: S54–62
Rapoport A, Ryan R, Goldstein J, et al. Dose range-finding studies with frovatriptan in the acute treatment of migraine. Headache 2002 Apr; 42Suppl. 2: S74–83
Wade A, Warrington S, Whale H, et al. Pharmacokinetics and tolerability in healthy subjects of 6-day frovatriptan dosing regimen used for the short-term prevention of menstrual migraine. Headache 2006; 46(5): 844
MacGregor EA, Frith A, Ellis J, et al. Incidence of migraine relative to menstrual cycle phases of rising and falling estrogen. Neurology 2006 Dec 26; 67(12): 2154–8
Lee AJ, Cai MX, Thomas PE, et al. Characterization of the oxidative metabolites of 17beta-estradiol and estrone formed by 15 selectively expressed human cytochrome p450 isoforms. Endocrinology 2003 Aug; 144(8): 3382–98
Frova® tablets. Frovatriptan succinate. Chadds Ford (PA): Endo Pharmaceuticals Inc., 2007
Koch G. The use of nonparametric methods in the statistical analysis of the two-period change-over design. Biometrics 1972; 28: 277–84
Hodges Jr JL, Lehmann EL. Estimates of location based on rank tests. Ann Math Stat 1963; 34: 598–611
Granfors MT, Backman JT, Laitila J, et al. Oral contraceptives containing ethinyl estradiol and gestodene markedly increase plasma concentrations and effects of tizanidine by inhibiting cytochrome P450 1A2. Clin Pharmacol Ther 2005 Oct; 78(4): 400–11
Campbell J, MacGregor A, Pawsey S, et al. Short-term frovatriptan for prevention of menstrual migraine: safety and efficacy over 12–15 months. Cephalalgia 2007; 27(6): 753
Brandes JL, MacGregor A, Silberstein S, et al. Prevention of difficult-to-treat menstrual migraine using a 6-day regimen of frovatriptan: a second double-blind, randomized, placebo-controlled trial. Headache 2007; 47(5): 789–90
Shelepova T, Nafziger AN, Victory J, et al. Effect of a triphasic oral contraceptive on drug-metabolizing enzyme activity as measured by the validated Cooper-stown 5+1 cocktail. J Clin Pharmacol 2005 Dec; 45(12): 1413–21
Zomig®, Zomig-ZMT® tablets and orally disintegrating tablets: zolmitriptan. Wilmington (DE): AstraZeneca, 2005
Amerge® tablets: naratriptan hydrochloride. Research Triangle Park (NC): GlaxoSmithKline, 2006
Geraud G, Spierings EL, Keywood C. Tolerability and safety of frovatriptan with short-and long-term use for treatment of migraine and in comparison with sumatriptan. Headache 2002 Apr; 42Suppl. 2: S93–9
Lipton RB, Stewart WF, Diamond S, et al. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache 2001 Jul–Aug; 41(7): 646–57
Leonardi M, Steiner TJ, Scher AT, et al. The global burden of migraine: measuring disability in headache disorders with WHO’s Classification of Functioning, Disability and Health (ICF). J Headache Pain 2005 Dec; 6(6): 429–40
Steiner TJ, Scher AI, Stewart WF, et al. The prevalence and disability burden of adult migraine in England and their relationships to age, gender and ethnicity. Cephalalgia2003 Sep; 23(7): 519–27s
Acknowledgements
This paper was previously presented at the 48th Annual Scientific Meeting of the American Headache Society, 22–25 June 2006, Los Angeles, CA, USA.
This research was supported by Vernalis Development Ltd, Winnersh, UK, and Endo Pharmaceuticals Inc., Chadds Ford, PA, USA. The sponsor or their agents were responsible for study design, management of the study, and collection and analysis of the data. The authors were responsible for the interpretation of the data and the preparation, review and approval of the final manuscript. The authors would like to thank Kristine W. Schuler, MS, of Complete Healthcare Communications, Inc., for her assistance in the preparation of the manuscript. All authors are employees of the sponsor or were hired by the sponsor to conduct certain study procedures.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wade, A., Pawsey, S., Whale, H. et al. Pharmacokinetics of Two 6-Day Frovatriptan Dosing Regimens Used for the Short-Term Prevention of Menstrual Migraine. Clin. Drug Investig. 29, 325–337 (2009). https://doi.org/10.2165/00044011-200929050-00005
Published:
Issue Date:
DOI: https://doi.org/10.2165/00044011-200929050-00005