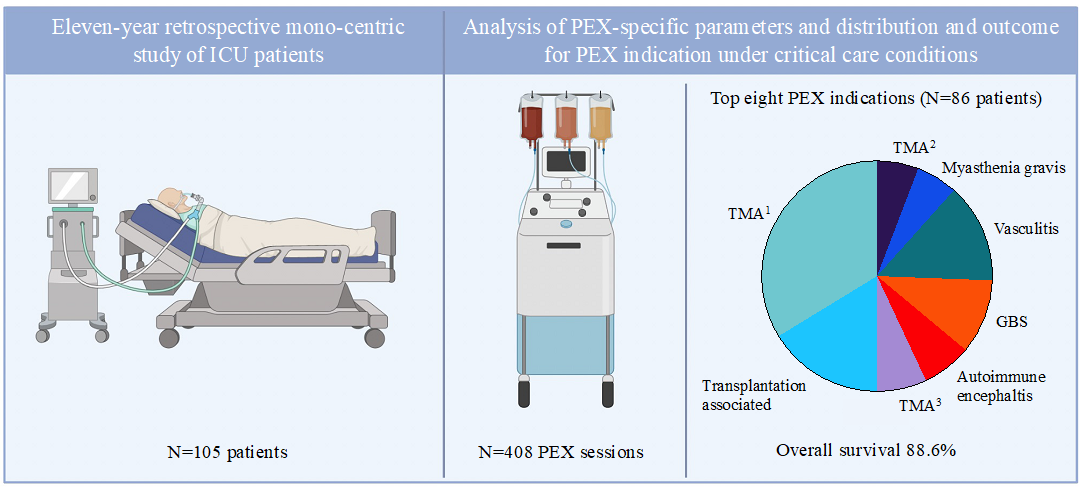
Our retrospective study spanning 11 years and a sizeable number of patients (n = 105) treated with TPE in the ICU setting demonstrated that TPE is overall save and beneficial, with ICU survival reaching 88.6% across all indications, reaffirming the role of TPE in the treatment of ICU patients. Indication for TPE according to ASFA was grade I in 59% of cases, demonstrating the overall robustness of decision making but also encouraging further investigations towards rigorous standards. The spectrum of indications for TPE in the critically ill in our cohort was to a large degree comparable to common indications in non-ICU cohorts published previously (2–4, 13), including TMA (TTP), catastrophic antiphospholipid syndrome, Guillain-Barré Syndrome or acute liver failure. Other explorative indications such as sepsis (14), PANDAS (pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections) (15) or drug overdoses / poisoning (16) were not present in our cohort.
While ASFA guidelines are comprehensive, currently listing 89 diseases or 179 indications supported by various levels of evidence (I-III), uncertainties remain. For example, TMAs were the most common indication for TPE in our study (n = 40, 38.1%), which represent a heterogeneous group of disorders characterized by similar clinical laboratory findings, but markedly different underlying pathophysiology (17). The striking success of TPE as upfront emergency therapy in TTP, reducing morbidity and mortality from 90% in untreated patients to below 20% led to application in other forms of TMA, often before confirmation of ADAMTS13 status (18, 19). In our cohort 11 (10.5%) patients received TPE for TMAs other than TTP and subsequent analysis normal ADAMTS13 activity or lack of inhibitor in nine (82%). The underlying pathology for these entities may not be circulatory factors purgeable via TPE, and could be associated with endothelial cell related factors or enterotoxins, thus potentially limiting benefit or causing harm in these conditions (17, 20). A retrospective evaluation of TPE used during the EHEC-HUS pandemic in 2011 revealed lack of efficiency of plasma exchange in enterotoxin-mediated HUS in adults (21). On the other hand, current tests do not detect all ADAMTS13 deficiencies in patients presenting with TTP (22) and lack of specific criteria complicate decision making. Further studies are warranted, also regarding management of refractory TMA cases (e.g., TPE regimens; combination with caplacizumab) (23, 24), ideally in randomized trials. A growing number of explorative indications for TPE further underline the potential and at the same time the necessity for standardization. Some examples include infections for example utilized in a) pediatric patients with H1N1 influenza A related respiratory failure and hemodynamic compromise (25), b) COVID-19 coagulopathy (26, 27), c) septic shock (28) or d) enhanced removal of inflammatory cytokines by combining conventional TPE with specific adsorbers, has been applied in enveloped viral disease (e.g., Ebola) (29).
In terms of procedural aspects, strong evidence for recommendations regarding the ideal treatment initiation and duration time-points, amount of the exchange volume, anticoagulation, type and composition of the substitute solution or vascular access are lacking and often locally defined in standard operating procedures within individual institutions. For example, the choice of replacement fluid, though important, partially lacks solid standards. The predominant use of FFP in our study can be partially explained by the high percentage of TMAs (TTP) compared to other studies (30) where FFP is the obligatory replacement solution to increase ADAMTS13 activity. A contrary example is the use of FFP in patients with GBS, which showed no benefit but an association with greater risks of citrate and transfusion reactions (31, 30). In our study one third (n = 3) of GBS patients received FFP and one patient experienced atrial fibrillation during TPE with FFP, which was resolved with cardioversion. Still, the adverse advent rate for TPE in GBS vs. comparable to the overall complication rate (was 11% vs. 9.5%). Previously reported TPE-associated complication rates vary significantly, ranging from 1–2% up to 39%) (9, 30, 32). Anaphylactic reactions were the primary complications as reported by others in conjunction with plasma use (9, 32). Only a single bleeding event was found which compares favorably with previous reports of up to 8.7% (9). Hypotension as a complication of TPE was not recorded in any patient, despite being the most common complications according to literature and correlating with a low hematocrit as present in most of our patients (9). Patients in our study received on average 3.9 ± 3.3 TPE sessions, similar to other studies in the ICU setting (9, 11). Unlike the report from Lemaire et al. we did not see a higher amount of TPE procedures required in patients with TMAs compared to other indications (9). On the contrary, several other indications (Guillain-Barré Syndrome (5.8 ± 3.5), autoimmune encephalitis (5.5 ± 2.6) and Goodpasture Syndrome (7.7 ± 6)) resulted in more TPE sessions than all TMAs (3.5 ± 3.7). The median length of ICU stay (8 ± 14.4 days) was similar to previously results, but has also been reported with a median of 20.2 ± 25 days (9, 11, 12). Since cost and patient outcome are correlated with length of ICU stay (33) this difference is of importance and warrants further investigation of underlying factors.
A strength of our study is the substantial amount of critically ill patients from a large tertiary care center in Switzerland with a total of 408 analyzed TPE sessions. Another strength is the detailed analysis of patient characteristics and laboratory findings as well as procedural aspects of TPE.
Limitations of our study include its retrospective character and non-uniform documentation over the study period. Bias might occur through inconsistent reporting of minor complications. SOFA scores have only been recorded systematically in Switzerland after 2013 and 41 patients had no SOFA score available, which hindered a thorough assessment of the severity of illness. Finally, our analysis did not allow us to reliably distinguish solid indications for ICU treatment vs. other factors leading to TPE in the ICU.
In conclusion, we provide a comprehensive analysis of TPE indications in patients requiring ICU treatment according to our in-house clinical practice at the University Hospital of Zurich. Overall, specific disease remission and ICU survival with almost 90% was excellent. We believe that our study is representative and could serve as a point of reference for other similar hospitals and might encourage similar research to form a basis for comparative analysis. Such shared experiences may be translated into reliable treatment standards and ultimately improved patient outcomes.
{kind=link}