
Routine plain film of abdomen in asymptomatic patients with video capsule retention in small bowel-time to change practice?
 0
0Abstract
Aim: Small bowel capsule retention is rare, with a rate of approximately 2%, defined as visible retention on plain film of abdomen (PFA) after 14 days. Currently, PFA is performed if the capsule is not seen to reach the large bowel during recording. Alternatively, for upper gastrointestinal (UGI) capsule studies, the risk of retention is determined if the capsule fails to reach the small bowel during recording. Given the similar physical specifications of the capsules (Medtronic) used, we considered whether 14-day PFA is no longer required for small bowel capsules not observed in the large bowel.
Methods: The use of patency capsules in our lab allows careful selection of small bowel capsule studies to minimize the risk of retention. All PFAs performed over a five-year period were reviewed to determine if careful selection and use of patency negate the need for capsule retention PFA screening.
Results: In total, 688 small-bowel capsules were performed during the study period, and 3.6% had prior patency capsules. Thirty-one PFAs with a query of capsule retention were performed during the study period on 28 patients. This included 15 females, and the median age was 53.5 years. None of the films demonstrated capsule retention.
Conclusion: Our data suggest that 14-day PFA may no longer be required for small bowel capsules not seen to reach the large bowel. Advice regarding symptoms of capsule retention and precaution with magnetic resonance imaging, similar to current UGI capsule advice, may suffice. This may reduce the burden on radiology imaging slots and, in particular, eliminate unnecessary radiation exposure and repeat hospital attendance for patients.
Keywords
INTRODUCTION
Video capsule endoscopy (VCE), first introduced in 2000[1], has an increasingly important role in gastrointestinal investigation. Most commonly used to identify a cause for anemia, occult gastrointestinal bleed, or characterize and diagnose small bowel inflammatory bowel disease, capsule endoscopy technology has recently advanced to allow video inspection of the entire gastrointestinal tract. Procedures and patient preparation are tailored to the intestinal segment of interest, similar to standard endoscopy. Upper gastrointestinal tract, small bowel, and colon capsules all require specific fasting and preparation to achieve diagnostic mucosal views. Following the procedure, however, a more standard approach may be reasonable. The ingested capsule, regardless of recording segment, consists of similar components and size and must pass through the alimentary canal. Thus, post-procedure protocols should not differ in asymptomatic patients.
Capsule retention, defined as visible retention on plain film of abdomen (PFA) after 14 days, is the most concerning risk with VCE[2]. Overall retention risk is low, estimated at 1.2%-4.63%[3], and in the absence of symptoms of capsule retention, conservative management is often advocated. Retention risk may be reduced further by careful patient selection, use of patency capsules, and screening of referrals by an experienced capsule endoscopist. Currently, if a small bowel capsule is not seen to pass into the caecum during the recording window [Figure 1], a follow-up PFA is advised by current guidelines 14 days later to identify possible capsule retention[2,4,5]. With regard to upper gastrointestinal tract capsule endoscopy, the protocol and recording window does not allow sufficient time to observe the capsule passing into the caecum. A routine PFA in these cases is, for the most part, unnecessary and would significantly burden both radiology departments and patients with repeat hospital attendance. In addition, as capsule endoscopy services continue to expand, in part driven by the COVID-19 pandemic, a large increase in capsule procedures may be expected.
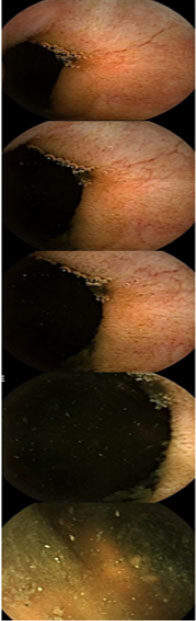
Figure 1. Representative images of small bowel video capsule passing from terminal ileum through the ileo-caecal valve and into the caecum.
To reduce the effect an increased capsule endoscopy service may have on radiology departments and to improve patient care and experience, we aimed to standardize the post-capsule procedural advice offered to asymptomatic patients. We considered whether current guideline advice[2] of a 14-day PFA in small bowel capsule cases not seen to reach caecum is no longer required in the absence of patient symptoms, similar to upper gastrointestinal tract VCE. To better inform patient safety, future risk of retention, and address whether PFA is required or a more generalized patient information booklet may suffice, a review of all small bowel VCE and PFAs performed within our unit over a five-year period was performed.
METHODS
In an Irish single-center tertiary referral unit for VCE, all cases of small bowel VCE requiring PFA performed over a five-year period were reviewed. This included PFAs evaluating possible capsule retention 14 days post VCE as well as those undergoing luminal patency capsule testing. Cases where a cause for capsule retention was identified on the capsule recording and those with symptoms suggestive of obstruction were evaluated separately, as they did not undergo 14-day follow-up PFA but rather definitive management based on VCE findings. Approval for this study was granted by the Cork university-affiliated hospital’s clinical ethics review board.
All referrals for capsule endoscopy to our unit are screened by an experienced capsule endoscopist and laboratory scientist to ensure accurate indication, patient suitability, and safety. All patients with suspected inflammatory bowel disease have prior magnetic resonance enterography performed as standard care, for example, and those with increased risk for stricturing luminal disease undergo luminal patency capsule testing prior to VCE. Appropriate patients then proceed to video capsule endoscopy.
Clear instructions for bowel preparation are sent to patients prior to attending for capsule ingestion. The day prior to the capsule study, patients consume clear liquids only in addition to the bowel preparation regime and fully fast for 12 h prior to the study. On the day of the study, the patient’s history is revisited to ensure accuracy and compliance with pre-procedure protocol is confirmed. All procedures are carried out following current health service executive guidelines on hand hygiene and the use of personal protective equipment. The device recording equipment is then fitted to the patient. The capsule, once inspected to ensure its integrity and paired with a recording device, is then swallowed with water containing Simethicone to aid small bowel mucosal views. Following confirmation that the capsule has entered the stomach, the patient remains fasting for a further 2 h, after which water may be consumed, followed by solid food from 4 h. Post-procedure, the capsule data are reviewed and cases where the capsule has not reached the caecum by the end of the recording window are flagged for follow-up 14-day PFA to evaluate capsule retention[2,4,5].
The current practice for upper gastrointestinal tract capsules where the capsule is unlikely to be seen to reach the caecum given the shorter recording time and protocol variation is to advise patients to attend the hospital if they experience any abdominal symptoms suggestive of capsule retention or obstruction. Additionally, a PFA is advised prior to a future MRI to ensure the capsule has passed.
RESULTS
During the five-year study period, 688 small bowel VCE were performed. Of these, 3.6% (25/688) underwent prior patency capsule testing. All patients who required patency capsules during this study period were deemed suitable to proceed with capsule endoscopy. Cases where there was clear video evidence of capsule hold-up or significant small bowel pathology on the video recording were excluded from primary analysis.
Twenty-eight cases were identified where the capsule was not seen to reach the large bowel within the recording window. Of these, 15 cases were female and the median age was 53.5 years (range 23-85 years). In total, 31 PFAs were performed to investigate possible capsule retention, none of which demonstrated definitive evidence of capsule retention [Figure 2]. Two patients underwent a second PFA as the first did not demonstrate clear capsule progression, although both patients remained asymptomatic. The capsule was demonstrated in the large bowel or was excreted on repeat PFA. A third patient had a repeat PFA due to a metal artifact in the abdomen, which was deemed unrelated to the capsule which had been excreted. In only one case where the video capsule could not be confirmed to reach the caecum did a patient report abdominal pain post VCE. Subsequent PFA demonstrated the capsule had been excreted.
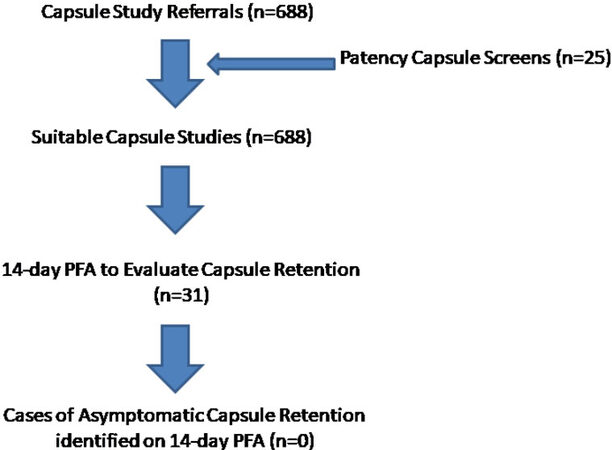
Figure 2. The number of cases of video capsule endoscopy performed during the study period and the number of cases of retention identified on 14-day plain film abdomen (PFA) follow-up.
Of the cases that underwent follow-up PFA to assess for capsule retention, ten VCE studies were indicated to evaluate small bowel inflammatory bowel disease (IBD), seven for investigation of iron deficiency anemia, one for polyp surveillance in Peutz-Jeghers syndrome, and one to further investigate abnormal terminal ileum thickening on cross-sectional imaging. The remaining nine cases were referred from external services and access to indication was unavailable. None of these video capsule cases identified findings consistent with an obstructing lesion, stricture, or other concerning features that would potentially result in capsule retention.
DISCUSSION
Our data show no cases of unexpected capsule retention identified over a five-year period, with 688 small bowel video capsule endoscopies performed. In addition, our patency capsule rate was 3.6%, used in addition to cross-sectional imaging to help determine the risk of capsule retention.
Our data compare favorably with previous studies where capsule retention rates are estimated to be
In the majority of cases of suspected capsule retention, particularly in the absence of obstructive symptoms, conservative treatment options are often appropriate[7]. The use of corticosteroids or immunomodulators may result in spontaneous capsule excretion, particularly in cases of IBD[3,8]. In a previous large retrospective study of 2300 patients, including 196 with small bowel Crohn’s disease, capsule retention was seen in five cases[8,9]. In three of these cases, the capsule passed spontaneously after steroid therapy, with two patients undergoing surgery for capsule retrieval[8,9]. Furthermore, a 10-year retrospective study identified capsule retention in 1% (25/2401) of cases, most commonly in cases of Crohn’s disease and occult gastrointestinal bleeding[10]. Previous gastrointestinal surgery was also found to correlate with the risk of retention, with an odds ratio of 7.64 (95%CI: 3.45-16.93, P < 0.001)[10]. Five of these cases required emergency endoscopic or surgical removal. Notably, this study reports that symptoms had resolved for all cases of capsule retention after follow-up or intervention, suggesting the presence of symptomatic capsule retention. Surgical intervention is rarely required; endoscopic retrieval, such as device-assisted enteroscopy, may be considered, but a conservative, observant approach is often sufficient in the absence of symptoms[3,7].
We suggest that careful history taking and referral screening helps identify and reduce the risk of capsule retention in patients undergoing VCE. In addition, the appropriate use of cross-sectional imaging and patency capsule testing further reduces the risk of both symptomatic and asymptomatic capsule retention[8,11]. Our study is limited, however, as a retrospective review and access to some external referral data were unavailable. As mentioned above, cases with clear evidence of luminal pathology on video recording and capsule hold-up were not included in the analysis and underwent specific intervention and management. In the future, information booklets for patients with advice to seek urgent medical attention should they develop abdominal symptoms post-VCE, as well as recommendations regarding future potential MRI, may suffice in asymptomatic cases without clear evidence of capsule excretion. In cases of confirmed Crohn’s disease, perhaps a more cautious approach is wise until further data are available.
In conclusion, a PFA is often requested following small bowel video capsule endoscopy to rule out capsule retention. This is particularly so in cases where the capsule is not seen to reach the caecum within the recording window. We question the value of PFA in asymptomatic patients where the capsule is not seen to pass the ileocaecal valve. In total, 28 cases were identified from a 688 cohort of capsule studies where PFA was required to exclude capsule retention. No cases of unexpected capsule retention over a five-year period were identified. No intervention was required in any case. Our data suggest that 14-day PFA may no longer be required for small bowel capsules not seen to reach the large bowel in asymptomatic cases. Careful screening of referrals and use of patency capsule and cross-sectional imaging may further reduce the risk of capsule retention. In the future, larger prospective studies should be considered to further evaluate these findings and address new guideline implementation.
DECLARATIONS
Authors’ contributionsStudy design, data collection, interpretation, and drafting of the manuscript: O’Grady J, Bennett S, Kaar A, Nolan L, O’Neill J, Quinlivan L, Buckley M
Availability of data and materialsNot applicable.
Financial support and sponsorshipNone.
Conflicts of interestAll authors declared that there are no conflicts of interest.
Ethical approval and consent to participateApproval for this study was granted by the Cork university affiliated hospitals clinical ethics review board (reference number: ECM 4 (p) 11/5/2021).
Consent for publicationNot applicable.
Copyright© The Author(s) 2022.
REFERENCES
2. Rondonotti E, Spada C, Adler S, et al. Small-bowel capsule endoscopy and device-assisted enteroscopy for diagnosis and treatment of small-bowel disorders: European society of gastrointestinal endoscopy (ESGE) technical review. Endoscopy 2018;50:423-46.
3. Zammit S, Sidhu R. Capsule endoscopy-recent developments and future directions. Expert Rev Gastroenterol Hepatol 2021;15:127-37.
4. Rondonotti E. Capsule retention: prevention, diagnosis and management. Ann Transl Med 2017;5:198.
5. Sachdev MS, Leighton JA, Fleischer DE, et al. A prospective study of the utility of abdominal radiographs after capsule endoscopy for the diagnosis of capsule retention. Gastrointest Endosc 2007;66:894-900.
6. Al-Bawardy B, Locke G, Huprich JE, et al. Retained capsule endoscopy in a large tertiary care academic practice and radiologic predictors of retention. Inflamm Bowel Dis 2015;21:2158-64.
7. Fernández-Urién I, Carretero C, González B, et al. Incidence, clinical outcomes, and therapeutic approaches of capsule endoscopy-related adverse events in a large study population. Rev Esp Enferm Dig 2015;107:745-52.
8. Pennazio M, Spada C, Eliakim R, et al. Small-bowel capsule endoscopy and device-assisted enteroscopy for diagnosis and treatment of small-bowel disorders: European society of gastrointestinal endoscopy (ESGE) clinical guideline. Endoscopy 2015;47:352-76.
9. Viazis N, Zacharakis G, Saprikis E, et al. A single center experience of 2300 consecutive patients undergoing capsule endoscopy: indications and diagnostic yield. Endoscopy 2011;43:A129.
10. Nemeth A, Wurm Johansson G, Nielsen J, Thorlacius H, Toth E. Capsule retention related to small bowel capsule endoscopy: a large European single-center 10-year clinical experience. United European Gastroenterol J 2017;5:677-86.
Cite This Article
Export citation file: BibTeX | RIS
OAE Style
O’Grady J, Bennett S, Kaar A, Nolan L, O’Neill J, Quinlivan L, Buckley M. Routine plain film of abdomen in asymptomatic patients with video capsule retention in small bowel-time to change practice?. Mini-invasive Surg 2022;6:34. http://dx.doi.org/10.20517/2574-1225.2022.22
AMA Style
O’Grady J, Bennett S, Kaar A, Nolan L, O’Neill J, Quinlivan L, Buckley M. Routine plain film of abdomen in asymptomatic patients with video capsule retention in small bowel-time to change practice?. Mini-invasive Surgery. 2022; 6: 34. http://dx.doi.org/10.20517/2574-1225.2022.22
Chicago/Turabian Style
O’Grady, John, Siofra Bennett, Aidan Kaar, Lorraine Nolan, Julie O’Neill, Lucy Quinlivan, Martin Buckley. 2022. "Routine plain film of abdomen in asymptomatic patients with video capsule retention in small bowel-time to change practice?" Mini-invasive Surgery. 6: 34. http://dx.doi.org/10.20517/2574-1225.2022.22
ACS Style
O’Grady, J.; Bennett S.; Kaar A.; Nolan L.; O’Neill J.; Quinlivan L.; Buckley M. Routine plain film of abdomen in asymptomatic patients with video capsule retention in small bowel-time to change practice?. Mini-invasive. Surg. 2022, 6, 34. http://dx.doi.org/10.20517/2574-1225.2022.22
About This Article
Special Issue
Copyright

Data & Comments
Data
0

 Cite This Article 9 clicks
Cite This Article 9 clicks

 Like This Article 0
likes
Like This Article 0
likes






Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.