
Abstract
Objective: Numerous studies examining the relationship between human epidermal growth factor receptor 2 (HER-2) overexpression and survival in patients with colorectal cancer (CRC) have yielded controversial results. We therefore performed a meta-analysis more precisely to estimate its prognostic value. Methods: Published studies investigating the effect of HER-2 overexpression on CRC survival were identified; the hazard ratios (HRs) and their corresponding 95% confidence intervals (95% CIs) were pooled in terms of disease-specific or overall survival. Results: Eleven studies were included in the meta-analysis. The pooled data showed that HER-2 overexpression was negatively related to CRC survival (HR=1.10, 95% CI: 0.77–1.44). Subgroup analyses regarding test method and study quality also demonstrated little association between HER-2 overexpression and CRC survival (HR=0.89, 95% CI: 0.50–1.29; HR=0.90, 95% CI: 0.43–1.37, respectively). Conclusions: Regardless of several limitations, our study suggested that HER-2 overexpression probably had little impact on CRC survival.
Similar content being viewed by others


1 Introduction
Colorectal cancer (CRC) is the third most com-mon cancer worldwide with approximately 1.23 million new cases diagnosed globally in 2008, accounting for one in ten cancers (Ferlay et al., (2010)). Although surgical treatment combined with multimodality therapy has given rise to improvements in CRC survival, prognoses of some patients are still poor. Therefore, prognostic tools are commonly adopted for predicting the survival of CRC patients. Many factors have been identified to date, the most important of which is the TNM stage determined by depth of tumor invasion, involvement of lymph nodes, and distant metastasis. However, differences are commonly observed among patients with the same stage. Therefore, it is necessary to establish new predictors for CRC other than conventional factors.
Recently, a biologic marker named ‘human ep-idermal growth factor receptor 2 (HER-2)’, also known as c-erbB-2, neu, or p185, has emerged as a potential prognostic factor for CRC. In addition, HER-2 can be a therapeutic option with monoclonal antibodies such as trastuzumab. However, most CRCs which overexpress HER-2 show cytoplasmic staining and only approximately 5% have cell membrane staining, but unfortunately only this 5% are amenable to antibody therapy (Blok et al., (2013)). Therefore, the detection of HER-2 expression is of great importance not only for being a prognostic marker but also a therapeutic factor. The amplifica-tion of the HER-2 gene was first reported as a predictor of poor survival in breast cancer patients by Slamon et al. (1987). Since then, several studies have demonstrated that HER-2 is overex-pressed in 10%–34% of invasive breast cancer and related to a poor prognosis (Kaptain et al., (2001)). In gastric cancer, approximately 20% of pa-tients overexpress HER-2 (Gravalos and Jimeno, (2008)). However, the role of HER-2 overexpression in gastric cancer survival remains unclear, with some studies reporting HER-2 positivity to be a poor prognostic factor, while others report that HER-2 overexpression does not impact on the prognosis of gastric cancer (Pazo Cid and Antón, (2013)). CRCs also express HER-2 protein (Koeppen et al., (2001)); however, conflicting data were reported re-garding its prognostic value. Some studies reported that HER-2 overexpression was a poor predictor (Osako et al., (1998); Park et al., (2007); Baiocchi et al., (2009); Chen et al., (2010); Lu et al., (2012)), while others reported that it was negatively related to patient sur-vival (McKay et al., (2002); Rossi et al., (2002); Jesus et al., (2005); Kavanagh et al., (2009); Li et al., (2011)). Still others reported that HER-2 was a good predictor (Conradi et al., (2013)). Therefore, we performed a systematic meta-analysis of all available studies using rigorous methods aiming to quantitatively estimate the prognostic value of HER-2 overexpression in CRC.
2 Materials and methods
2.1 Search strategies
Two authors, Dr. Da-ren LIU and Dr. Long-yun YE, independently searched PubMed, Embase, and the Cochrane Central Registry of Con-trolled Trials from January 1990 to September 2013 to identify studies on the association between HER-2 expression and CRC survival. The language was li-mited to English and the search terms were as follows: ‘colorectal cancer’, ‘colon cancer’, or ‘rectal cancer’; ‘HER2’, ‘HER-2’, ‘neu’, ‘human epidermal growth factor receptor 2’, or ‘erbB2’; and, ‘prognosis’ or ‘survival’. Bibliographies of all relevant publications were scanned to identify relevant studies.
2.2 Inclusion and exclusion criteria
Studies meeting the following criteria were included: (1) the patients had surgical treatment and the disease was identified as CRC pathologically; (2) the endpoint was disease specific or overall survival; (3) the HER-2 expression was evaluated by immuno- histochemistry (IHC); and, (4) the hazard ratio (HR) and 95% confidence interval (CI) were reported or could be estimated from other data provided in the articles. Case reports, review articles, experimental studies, as well as studies that did not supply suffi-cient survival data were excluded. If a study matching the selection criteria had missing data, the authors were contacted in an attempt to obtain the missing information. For publications containing duplicated findings, the study containing the largest number of subjects was included.
2.3 Data extraction and quality assessment
Two authors, Ling-na HUANG and Sanjay JAISWAL, independently extracted information from eligible publications by means of a predefined form. Recorded data included the first author’s name, year of publication, country, mean patient age, number of patients, tumor stage, cut-off point, positive percentage, primary surgery and post-operative treatment, time of follow-up, other influential factors, and results of survival analysis. Quality of the enrolled studies was assessed individually by two authors, Xiao-wen LI and Dr. Hou-hong WANG, based on the Newcastle-Ottawa scale (Wells et al., 2010), which examines patient selection methods, comparability of study groups and assessment of outcomes. Studies obtaining 7–9 stars are considered to be of ‘high quality’, 5–6 stars as ‘moderate quality’, and 5 stars or below as ‘low quality’. Studies of low quality were excluded. Disagreements were resolved through discussion or consensus with a third reviewer, Dr. Li CHEN.
2.4 Statistical analysis
HR was used in this time-to-event analysis, which takes into consideration the number and timing of events. The overall survival value of each study was determined by the combination of HR and its corresponding 95% CI. All data were directly ob-tained or indirectly computed using the formula recommended by Tierney et al. (2007). The significance of the pooled HR was determined by Z test, and P≤0.05 was considered statistically significant.
The I2 was calculated to assess the impact of heterogeneity on results. Heterogeneity was considered significant when I2 was greater than 50%, then the random-effects model was used; otherwise, the fixed-effects model was used (Higgins et al., (2003)). Publication bias was investigated through a funnel plot by the Egger’s and Begg’s tests. Funnel plot asymmetry implied results were subject to publication bias, whereas symmetry implied a lack of bias. P≤0.1 was regarded as statistically significant of publication bias. The Kaplan-Meier curves were read by Engauge Digitizer (Version 2.11; http://sourceforge.net) and all statis-tical calculations were performed by Stata software (Version 11.0; StataCorp LP, College Station, Texas, USA), using two-sided P values.
3 Results
3.1 Literature search and characteristics of the included studies
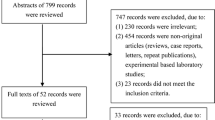
Fig. 1 depicts the flow of the literature search; 293 studies were initially identified, of which 11 were eligible for final analysis. As shown in Table 1, 1761 patients were included in the 11 studies. Five studies (770 patients, 43.7%) were from Asian countries while the other six (991 patients, 56.3%) were non-Asian. IHC was used to evaluate HER-2 expression levels for all studies with five studies additionally performing fluorescence in situ hybridization, silver in situ hybridization, western blotting, or quantitative polymerase chain reaction (qPCR). Five different cut-off values were used to determine HER-2 status, of which the HercepTest scoring system was the most frequently adopted (n=5). As for prognostic value, five studies identified HER-2 overexpression as an indicator of poor prognosis (Osako et al., (1998); Park et al., (2007); Baiocchi et al., (2009); Chen et al., (2010); Lu et al., (2012)), five studies revealed that HER-2 overexpression had no influence on CRC survival (McKay et al., (2002); Rossi et al., (2002); Jesus et al., (2005); Kavanagh et al., (2009); Li et al., (2011)), and one study reported HER-2 overexpression to be a good predictor (Conradi et al., (2013)) (Table 2).

Major characteristics of the studies included in meta-analysis

Method characteristics and effects of HER-2 overexpression on CRC survival

Identification process for eligible studies
3.2 Results of meta-analysis
Meta-analysis of the 11 studies using the random- effects model showed that HER-2 overex-pression was negatively related to the overall survival of CRC (HR=1.10, 95% CI: 0.77–1.44), and hetero-geneity between the included studies was significant (I2=69.8%). Subgroup analyses were performed after stratifying the data by ethnicity and cut-off value. In the Asian subgroup, the associ-ation between HER-2 overexpression and CRC sur-vival was weak; the pooled HR was 1.51 and the lower 95% CI was close to 1 (95% CI: 1.04–1.97). In the non-Asian subgroup, however, the pooled HR was 0.84 (95% CI: 0.44– 1.23), suggesting that HER-2 overexpression was negatively related to CRC sur-vival (Fig. 2). To reduce technology bias, we further performed a subgroup analysis of the five studies based on the same Hercep- Test criteria scoring sys-tem. The results gave a pooled HR=0.89 (95% CI: 0.50–1.29) (Fig. 3), suggesting that HER-2 status determined by the HercepTest scoring system was a negative predictor. Meanwhile, subgroup analysis of high-quality studies also produced similar results (HR=0.90, 95% CI: 0.43–1.37) (Fig. 4).

Meta-analysis with random- effects model for the association between HER-2 overexpression and CRC survival and subgroup analysis of the Asian and non-Asian

Meta-analysis with random-effects model for the association between HER-2 overexpression determined by the HercepTest criteria and CRC survival

Meta-analysis of studies of high quality with random-effects model for the association between HER-2 overexpression and CRC survival
3.3 Publication bias
Egger’s test and Begg’s funnel plot were used for detecting publication bias. Little funnel plot asymmetry was found among the included studies, with P≥0.1 for both Egger’s and Begg’s tests (0.566 and 0.371, respectively), suggesting that the publication bias was statistically insignificant (Fig. 5).

Funnel plot for publication bias of all studies included in this meta-analysis
Begg’s funnel plot with pseudo 95% confidence limits
4 Discussion
The HER-2 oncogene is located on chromosome 17q21 and encodes a 185-kDa trans-membrane protein that exhibits tyrosine kinase activity (Akiyama et al., (1986)). The HER-2 protein belongs to the epidermal growth factor receptor (EGFR) family, and dimerization of HER-2 with an activated EGFR molecule activates the downstream signaling pathway (Jorissen et al., (2003)). The possible effects of HER-2 for tumors include controlling cell proliferation and migration (Wolf-Yadlin et al., (2006)).
Regardless of the potential roles of HER-2 on tumorigenesis, the present meta-analysis suggested that HER-2 overexpression probably has little impact on CRC survival. The overall pooled HR was 1.10, with the 95% CI ranging from 0.77 to 1.44. In the non-Asian subgroup, as well as in the HercepTest criteria scoring system adopted subgroup and the high quality subgroup, the pooled HRs and their corres-ponding 95% CIs also showed a negative relationship between HER-2 overexpression and CRC survival. All these results suggested that elevated HER-2 ex-pression probably has little prognostic value for CRC patients. Nevertheless, in the Asian subgroup the pooled HR showed a modest effect of HER-2 over-expression on CRC survival (HR=1.51, 95% CI: 1.04–1.97). This difference between the Asian and non-Asian subgroups may be caused by ethnic differences. However, the more likely reason may be the various scoring systems used, considering that four different criteria were reported in the five studies of the Asian subgroup. In addition, it is worth noting that Conradi et al. (2013) showed that HER-2 overexpression was a good predictive factor. They reported that patients with HER-2 positivity showed a trend towards a better disease-free survival and a benefit in cancer-specific survival, and the 5-year survival rate was 96.0% (HER-2 positive) versus 80.0% (HER-2 negative). This enhances our confidence in the results that unlike breast cancer, HER-2 overexpression probably has little influence on CRC survival.
Currently, IHC is a method commonly used to evaluate HER-2 status at the protein level. It is eco-nomical, widely available, easy to operate, and re-quires little time and equipment. In all the included studies, IHC was used to evaluate the HER-2 expression level. However, a wide range of HER-2 positive rates was reported among the 11 studies, ranging from 8.3% to 81.9%. The following issues may be responsible for the wide difference. First, there is no unified and widely accepted scoring system to evaluate the HER-2 expression of CRC. In the present study, the most frequently used scoring system is the Hercep-Test criteria widely used for breast cancer. However, whether it is suitable for CRC still needs further investigations, considering the significantly different biological origins of the two cancers. Moreover, IHC is a semi-quantitative method that may be easily influenced by the subjective perceptions of the pathologist. Finally, the various primary antibodies used, the different sizes of samples, and the varied experimental designs all may lead to inconsistency. Given all these reasons, it is probably not surprising that significant differences are observed in terms of HER-2 positivity, and as a result, these differences highlight the need for a scientific, unified detection system for HER-2 expression in CRC.
Several limitations should be mentioned about this meta-analysis. On literature searching, we tried our best to identify all relevant studies and retrieve additional unpublished information, but missing some data was unavoidable. In some studies, the HRs and their corresponding 95% CIs were indirectly calculated from other survival data or extracted from the survival curves, which may bias our results. Fur-thermore, as is well known, the survival of CRC is influenced by a synergy of many confounding factors such as age, differentiation degree, TNM stage, and post-operative treatment. Generally, if we perform subgroup analysis by as many confounding factors as possible including TNM stage, post-operative treatment, cut-off value, ethnicity, and study quality, a more accurate HR and a comparatively clearer relationship between HER-2 overexpression and CRC survival can be illustrated. However, not all studies considered these variables and in some studies many of the primary data were unavailable. Therefore, we could only perform subgroup analysis by ethnicity, cut-off value, and study quality, which may lead to an overestimate of the power of HER-2 overexpression on CRC prognosis. Moreover, publication bias is a major concern in all forms of meta-analysis, since the positive studies are more likely to be published and the pooled HR may be exaggerated by the omission of unpublished studies. Finally, as we restricted our analysis to studies written in English, language bias cannot be ignored. All these limitations may decrease the reliability of our analysis; thus, our results must be interpreted with caution. In future, more rigorous studies of large sample sizes, using standardized testing methods, unified scoring system, and complete analysis of results are needed to verify the prognostic value of HER-2 overexpression on CRC.
Trastuzumab is a recombinant humanized monoclonal antibody directed against the extracellular domain of the HER-2 protein (Tokunaga et al., (2006)). It is now clear that HER-2 positive breast cancer patients can benefit from trastuzumab therapy (Seidman et al., (2008)). In gastric cancer patients expressing high HER-2 protein, the combination of standard chemotherapy with trastuzumab was also reported to improve survival (Bang et al., (2010); Sawaki et al., (2012)). Trastuzumab was found to inhibit colony formation of colon cancer cells in vitro (Mann et al., (2001)). In a case reported by Sorscher (2011), a marked radio-graphic response to trastuzumab was observed in a HER-2 positive CRC patient. However, large-scale clinical trials on trastuzumab therapy for CRC are still lacking, and the benefits of neoadjuvant trastuzumab treatment for CRC patients remain unknown. Thus, a randomized controlled trial to address this potentially beneficial therapeutic option is warranted, especially for HER-2-positive CRC patients.
5 Conclusions
In summary, this meta-analysis suggests that HER-2 overexpression probably has little impact on CRC survival. Nevertheless, differences in selection and scoring, and publication and language biases must be taken into consideration when dealing with the results. Our study needs further confirmations by large-scale, well-designed, and rigorously-conducted studies in order to determine the relationship between HER-2 overexpression and CRC survival.
Compliance with ethics guidelines
Chao LI, Da-ren LIU, Long-yun YE, Ling-na HUANG, Sanjay JAISWAL, Xiao-wen LI, Hou-hong WANG, and Li CHEN declare that they have no conflict of interest.
This article does not contain any studies with human or animal subjects performed by any of the authors.
References
Akiyama, T., Sudo, C., Ogawara, H., et al., 1986. The product of the human c-erbB-2 gene: a 185-kilodalton glycoprotein with tyrosine kinase activity. Science, 232(4758): 1644–1646. [doi:10.1126/science.3012781]
Baiocchi, G., Lopes, A., Coudry, R.A., et al., 2009. ErbB family immunohistochemical expression in colorectal cancer patients with higher risk of recurrence after radical surgery. Int. J. Colorectal Dis., 24(9):1059–1068. [doi:10. 1007/s00384-009-0702-6]
Bang, Y.J., van Cutsem, E., Feyereislova, A., et al., 2010. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet, 376(9742):687–697. [doi:10.1016/S0140-6736(10)61121-X]
Blok, E.J., Kuppen, P.J.K., van Leeuwen, J.E.M., et al., 2013. Cytoplasmic overexpression of HER2: a key factor in colorectal cancer. Clin. Med. Insights Oncol., 7:41–51. [doi:10.4137/CMO.S10811]
Chen, J., Li, Q., Wang, C., et al., 2010. Prognostic significance of c-erbB-2 and vascular endothelial growth factor in colorectal liver metastases. Ann. Surg. Oncol., 17(6): 1555–1563. [doi:10.1245/s10434-009-0897-3]
Conradi, L.C., Styczen, H., Sprenger, T., et al., 2013. Frequency of HER-2 positivity in rectal cancer and prognosis. Am. J. Surg. Pathol., 37(4):522–531. [doi:10. 1097/PAS.0b013e318272ff4d]
Ferlay, J., Shin, H.R., Bray, F., et al., 2010. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int. J. Cancer, 127(12):2893–2917. [doi:10.1002/ijc. 25516]
Gravalos, C., Jimeno, A., 2008. HER2 in gastric cancer: a new prognostic factor and a novel therapeutic target. Ann. Oncol., 19(9):1523–1529. [doi:10.1093/annonc/mdn169]
Higgins, J.P., Thompson, S.G., Deeks, J.J., et al., 2003. Measuring inconsistency in meta-analyses. BMJ, 327(7414):557–560. [doi:10.1136/bmj.327.7414.557]
Jesus, E.C., Matos, D., Artigiani, R., et al., 2005. Assessment of staging, prognosis and mortality of colorectal cancer by tumor markers: receptor erbB-2 and cadherins. Acta Cirurg. Bras., 20(6):422–427. [doi:10.1590/S0102-86502 005000600005]
Jorissen, R.N., Walker, F., Pouliot, N., et al., 2003. Epidermal growth factor receptor: mechanisms of activation and signalling. Exp. Cell Res., 284(1):31–53. [doi:10.1016/ S0014-4827(02)00098-8]
Kaptain, S., Tan, L.K., Chen, B., 2001. Her-2/neu and breast cancer. Diagn. Mol. Pathol., 10(3):139–152.
Kavanagh, D.O., Chambers, G., O’Grady, L., et al., 2009. Is overexpression of HER-2 a predictor of prognosis in colorectal cancer? BMC Cancer, 9:1. [doi:10.1186/1471-2407-9-1]
Koeppen, H.K.W., Wright, B.D., Burt, A.D., et al., 2001. Overexpression of HER2/neu in solid tumours: an immunohistochemical survey. Histopathology, 38(2): 96–104. [doi:10.1046/j.1365-2559.2001.01084.x]
Li, Q., Wang, D., Li, J., et al., 2011. Clinicopathological and prognostic significance of HER-2/neu and VEGF expression in colon carcinomas. BMC Cancer, 11:277. [doi:10.1186/1471-2407-11-277]
Lu, Y., Jingyan, G., Baorong, S., et al., 2012. Expression of EGFR, Her2 predict lymph node metastasis (LNM)- associated metastasis in colorectal cancer. Cancer Biomark., 11(5):219–226. [doi:10.3233/CBM-2012- 00282]
Mann, M., Sheng, H., Shao, J., et al., 2001. Targeting cyclooxygenase 2 and HER-2/neu pathways inhibits colorectal carcinoma growth. Gastroenterology, 120(7): 1713–1719. [doi:10.1053/gast.2001.24844]
McKay, J.A., Loane, J.F., Ross, V.G., et al., 2002. c-erbB-2 is not a major factor in the development of colorectal cancer. Br. J. Cancer, 86(4):568–573. [doi:10.1038/sj.bjc.6600 127]
Osako, T., Miyahara, M., Uchino, S., et al., 1998. Immunohistochemical study of c-erbB-2 protein in colorectal cancer and the correlation with patient survival. Oncology, 55(6):548–555. [doi:10.1159/000011911]
Park, D.I., Kang, M.S., Oh, S.J., et al., 2007. Her-2/neu overexpression is an independent prognostic factor in colorectal cancer. Int. J. Colorectal Dis., 22(5):491–497. [doi:10.1007/s00384-006-0192-8]
Pazo Cid, R.A., Antón, A., 2013. Advanced HER2-positive gastric cancer: current and future targeted therapies. Crit. Rev. Oncol. Hematol., 85(3):350–362. [doi:10.1016/j. critrevonc.2012.08.008]
Rossi, H.A., Liu, Q., Banner, B., et al., 2002. The prognostic value of invariant chain (II) and Her-2/neu expression in curatively resected colorectal cancer. Cancer J., 8(3): 268–275.
Sawaki, A., Ohashi, Y., Omuro, Y., et al., 2012. Efficacy of trastuzumab in Japanese patients with HER2-positive advanced gastric or gastroesophageal junction cancer: a subgroup analysis of the trastuzumab for gastric cancer (ToGA) study. Gastric Cancer, 15(3):313–322. [doi:10. 1007/s10120-011-0118-1]
Seidman, A.D., Berry, D., Cirrincione, C., et al., 2008. Randomized phase III trial of weekly compared with every-3-weeks paclitaxel for metastatic breast cancer, with trastuzumab for all HER-2 overexpressors and random assignment to trastuzumab or not in HER-2 non-overexpressors: final results of cancer and Leukemia Group B Protocol 9840. J. Clin. Oncol., 26(10): 1642–1649. [doi:10.1200/JCO.2007.11.6699]
Slamon, D.J., Clark, G.M., Wong, S.G., et al., 1987. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science, 235(4785):177–182. [doi:10.1126/science.3798106]
Sorscher, S.M., 2011. Marked response to single agent trastuzumab in a patient with metastatic HER-2 gene amplified rectal cancer. Cancer Invest., 29(7):456–459. [doi:10.3109/07357907.2011.590569]
Tierney, J.F., Stewart, L.A., Ghersi, D., et al., 2007. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials, 8(1):16. [doi:10.1186/1745-6215-8-16]
Tokunaga, E., Oki, E., Nishida, K., et al., 2006. Trastuzumab and breast cancer: developments and current status. Int. J. Clin. Oncol., 11(3):199–208. [doi:10.1007/s10147-006-0575-4] auWells, G.A, Shea, B., O’Connell, D., et al., 2010. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Available from http://www.ohri.ca/programs/clinical_epidemiology/ oxford.asp [Accessed on Sept. 2013].
Wolf-Yadlin, A., Kumar, N., Zhang, Y., et al., 2006. Effects of HER2 overexpression on cell signaling networks governing proliferation and migration. Mol. Syst. Biol., 2(1):54. [doi:10.1038/msb4100094]
Author information
Authors and Affiliations
Corresponding author
Additional information
Project supported by the National Natural Science Foundation of China (Nos. 81101837 and 81071959) and the Research Fund for the Doctoral Program of Higher Education of China (No. 20110101120129)
Rights and permissions
About this article

Cite this article
Li, C., Liu, Dr., Ye, Ly. et al. HER-2 overexpression and survival in colorectal cancer: a meta-analysis. J. Zhejiang Univ. Sci. B 15, 582–589 (2014). https://doi.org/10.1631/jzus.B1300258
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1631/jzus.B1300258