Abstracts
BACKGROUND: The control of cardiovascular responses during resistance exercise (RE) is important for patient safety. OBJECTIVE: To investigate the influence of repetition maximum (RM) and rest interval between sets (RI) on heart rate (HR), systolic blood pressure (SBP) and rate-pressure product (RPP) during RE. METHODS: Twenty healthy subjects (26 ± 5 years of age) underwent RE protocols involving three sets of leg press (6 and 12 RM) and RI proportional to the contraction time (1:3 and 1:5). The HR was checked on a continuous basis by using a cardiotachometer and the SBP was checked at the end of the sets, via a protocol validated by the auscultatory method. RESULTS: The HR was influenced by the workload (p = 0.008) and sets (p < 0.001), but not by the RI (p = 0.087). The SBP suffered from the isolated effect of the number of sets (p < 0.001) and RI (p = 0.017), but not from the workload (p = 0.95). The RPP rose in direct proportion to the workload (p = 0.036) and sets (p < 0.001), but in inverse proportion to the RI (p = 0.006). In 6 RM protocols, the variation in the HR was higher for RI = 1:3 (Δ = 11.2 ± 1.1 bpm) than for RI = 1:5 (Δ = 4.5 ± 0.2 bpm; p = 0.002), but there was no difference for 12 RM (Δ 1:3 = 21.1 ± 2.2 bpm; Δ 1:5 = 18.9 ± 2.0 bpm, p = 0.83). The RI influenced the variation in SBP in all loads (6 RM - Δ 1:3 = 10.6 ± 0.9 mmHg, Δ 1:5 = 6.6 ± 0.7 mmHg; p = 0.02 and 12 RM - Δ 1:3 = 15.2 ± 1.1 mmHg, Δ 1:5 = 8.4 ± 0.7 mmHg; p = 0.04). The RPP rose in proportion to the workload (p = 0.036) and to the sets (p < 0.001), but in inverse proportion to the RI (p = 0.006). With RI = 1:3, there was difference in RPP for 6 RM (Δ = 2,892 ± 189 mmHg.bpm) and 12 RM (Δ = 4,587 ± 300 mmHg.bpm; p = 0.018), but not with RI = 1:5 (6 RM: Δ = 1,224 ± 141 mmHg.bpm, 12 RM: Δ = 2,332 ± 194 mmHg.bpm; p = 0.58). CONCLUSION: Regardless of the workload, an increased RI was associated with lower cardiovascular responses during RE, especially of SBP.
Exercise; resistance training; heart rate; blood pressure
FUNDAMENTO: O controle das respostas cardiovasculares durante exercício resistido (ER) é importante para a segurança do paciente. OBJETIVO: Investigar a influência do número de repetições máximas (RM) e dos intervalos de recuperação entre séries (IR) sobre a frequência cardíaca (FC), pressão arterial sistólica (PAS) e duplo produto (DP) durante ER. MÉTODOS: Vinte sujeitos saudáveis (26 ± 5 anos) realizaram protocolos de ER envolvendo três séries do leg press (6 e 12 RM) e IR proporcional ao tempo de contração (1:3 e 1:5). Aferiu-se a FC continuamente com cardiofrequencímetro e a PAS foi verificada ao final das séries, por meio de protocolo validado com método auscultatório. RESULTADOS: A FC sofreu influência da carga (p = 0,008) e das séries (p < 0,001), mas não do IR (p = 0,087). A PAS sofreu efeito isolado do número de séries (p < 0,001) e do IR (p = 0,017), mas não da carga (p = 0,95). O DP elevou-se em relação direta com a carga (p = 0,036) e com as séries (p < 0,001), mas inversamente ao IR (p = 0,006). Nos protocolos de 6 RM, a variação da FC foi maior para IR = 1:3 (Δ = 11,2 ± 1,1 bpm) do que para IR = 1:5 (Δ = 4,5 ± 0,2 bpm; p = 0,002), mas não houve diferença para 12 RM (Δ 1:3 = 21,1 ± 2,2 bpm; Δ 1:5 = 18,9 ± 2,0 bpm, p = 0,83). O IR influenciou a variação da PAS em todas as cargas (6 RM - Δ 1:3 = 10,6 ± 0,9 mmHg, Δ 1:5 = 6,6 ± 0,7 mmHg; p = 0,02 e 12 RM - Δ 1:3 = 15,2 ± 1,1 mmHg, Δ 1:5 = 8,4 ± 0,7 mmHg; p = 0,04). O DP elevou-se proporcionalmente à carga (p = 0,036) e para séries (p < 0,001), mas inversamente ao IR (p = 0,006). Com IR = 1:3, houve diferença de DP para 6 RM (Δ = 2.892 ± 189 mmHg.bpm) e 12 RM (Δ = 4.587 ± 300 mmHg.bpm; p = 0,018), mas não com IR = 1:5 (6 RM: Δ = 1.224 ± 141 mmHg.bpm, 12 RM: Δ = 2.332 ± 194 mmHg.bpm; p = 0,58). CONCLUSÃO: Independentemente da carga, um maior IR associou-se a menores respostas cardiovasculares durante ER, especialmente de PAS.
Exercício; treinamento de resistência; frequência cardíaca; pressão arterial
FUNDAMENTO: El control de las respuestas cardiovasculares durante ejercicio de resistencia (ER) es importante para la seguridad del paciente. OBJETIVO: Investigar la influencia del número de repeticiones máximas (RM) y de los intervalos de recuperación entre series (IR) sobre la frecuencia cardíaca (FC), presión arterial sistólica (PAS) y doble producto (DP) durante ER. MÉTODOS: Veinte sujetos sanos (26 ± 5 años) realizaron protocolos de ER comprendiendo tres series del leg press (6 y 12 RM) y IR proporcional al tiempo de contracción (1:3 y 1:5). Se midió la FC continuamente con cardiofrecuencímetro y la PAS fue verificada al final de las series, por medio de protocolo validado con método auscultatorio. RESULTADOS: La FC sufrió influencia de la carga (p = 0,008) y de las series (p < 0,001), pero no del IR (p = 0,087). La PAS sufrió efecto aislado del número de series (p < 0,001) y del IR (p = 0,017), pero no de la carga (p = 0,95). El DP se elevó en relación directa con la carga (p = 0,036) y con las series (p < 0,001), pero inversamente al IR (p = 0,006). En los protocolos de 6 RM, la variación de la FC fue mayor para IR = 1:3 (Δ = 11,2 ± 1,1 lpm) que para IR = 1:5 (Δ = 4,5 ± 0,2 lpm; p = 0,002), pero no hubo diferencia para 12 RM (Δ 1:3 = 21,1 ± 2,2 lpm; Δ 1:5 = 18,9 ± 2,0 lpm, p = 0,83). El IR influenció la variación de la PAS en todas las cargas (6 RM - Δ 1:3 = 10,6 ± 0,9 mmHg, Δ 1:5 = 6,6 ± 0,7 mmHg; p = 0,02 y 12 RM - Δ 1:3 = 15,2 ± 1,1 mmHg, Δ 1:5 = 8,4 ± 0,7 mmHg; p = 0,04). El DP se elevó proporcionalmente a la carga (p = 0,036) y para series (p < 0,001), pero inversamente al IR (p = 0,006). Con IR = 1:3, hubo diferencia de DP para 6 RM (Δ = 2.892 ± 189 mmHg.lpm) y 12 RM (Δ = 4.587 ± 300 mmHg.lpm; p = 0,018), pero no con IR = 1:5 (6 RM: Δ = 1.224 ± 141 mmHg.lpm, 12 RM: Δ = 2.332 ± 194 mmHg.lpm; p = 0,58). CONCLUSIÓN: Independientemente de la carga, un mayor IR se asoció a menores respuestas cardiovasculares durante ER, especialmente de PAS.
Ejercicio; entrenamiento de resistencia; frecuencia cardíaca; presión arterial
ORIGINAL ARTICLE
IPrograma de Pós-Graduação em Ciências da Atividade Física - Universidade Salgado de Oliveira, Niterói, RJ - Brazil
IIInstituto de Educação Física e Desportos - Laboratório de Atividade Física e Promoção da Saúde - Universidade do Estado do Rio de Janeiro, Rio de Janeiro, RJ - Brazil
Mailing address
ABSTRACT
BACKGROUND: The control of cardiovascular responses during resistance exercise (RE) is important for patient safety.
OBJECTIVE: To investigate the influence of repetition maximum (RM) and rest interval between sets (RI) on heart rate (HR), systolic blood pressure (SBP) and rate-pressure product (RPP) during RE.
METHODS: Twenty healthy subjects (26 ± 5 years of age) underwent RE protocols involving three sets of leg press (6 and 12 RM) and RI proportional to the contraction time (1:3 and 1:5). The HR was checked on a continuous basis by using a cardiotachometer and the SBP was checked at the end of the sets, via a protocol validated by the auscultatory method.
RESULTS: The HR was influenced by the workload (p = 0.008) and sets (p < 0.001), but not by the RI (p = 0.087). The SBP suffered from the isolated effect of the number of sets (p < 0.001) and RI (p = 0.017), but not from the workload (p = 0.95). The RPP rose in direct proportion to the workload (p = 0.036) and sets (p < 0.001), but in inverse proportion to the RI (p = 0.006). In 6 RM protocols, the variation in the HR was higher for RI = 1:3 (Δ = 11.2 ± 1.1 bpm) than for RI = 1:5 (Δ = 4.5 ± 0.2 bpm; p = 0.002), but there was no difference for 12 RM (Δ 1:3 = 21.1 ± 2.2 bpm; Δ 1:5 = 18.9 ± 2.0 bpm, p = 0.83). The RI influenced the variation in SBP in all loads (6 RM - Δ 1:3 = 10.6 ± 0.9 mmHg, Δ 1:5 = 6.6 ± 0.7 mmHg; p = 0.02 and 12 RM - Δ 1:3 = 15.2 ± 1.1 mmHg, Δ 1:5 = 8.4 ± 0.7 mmHg; p = 0.04). The RPP rose in proportion to the workload (p = 0.036) and to the sets (p < 0.001), but in inverse proportion to the RI (p = 0.006). With RI = 1:3, there was difference in RPP for 6 RM (Δ = 2,892 ± 189 mmHg.bpm) and 12 RM (Δ = 4,587 ± 300 mmHg.bpm; p = 0.018), but not with RI = 1:5 (6 RM: Δ = 1,224 ± 141 mmHg.bpm, 12 RM: Δ = 2,332 ± 194 mmHg.bpm; p = 0.58).
CONCLUSION: Regardless of the workload, an increased RI was associated with lower cardiovascular responses during RE, especially of SBP.
Key words: Exercise; resistance training; heart rate: blood pressure.
Introduction
Resistance training causes significant increase in heart rate (HR) and blood pressure (BP)1,2. The adjustment of training variables can control these responses and change the cardiovascular overload during exercise2,3. Previous studies investigated the influence of several variables, such as speed of movement4, number of sets5, the intensity and number of repetitions2,6, the muscle mass involved2,7, the types of exercise1 or training status8.
However, there is scarce information about the influence of the rest interval between sets and exercises. Only one study specifically investigated the influence of this variable on HR and BP values9, identifying greater pressure response in sessions with shorter intervals. Ratamess et al10 did not specifically measure the BP, but they did not find significant differences in HR responses to exercise done with different rest intervals. However, the gradual increase in pulse rate throughout the sets was more evident for shorter intervals.
It is worth highlighting that these studies9,10 applied fixed rest intervals. So, they did not consider the cumulative effect of muscle fatigue in the course of the sets. In practice, it is possible to notice that different exercises require different execution times, either due to their complexity or due to the required range of motion. We could argue, for example, that if the rest interval were proportional to the exercise execution time, there would be a smaller ratio of decrease in workload due to lower accumulated fatigue.
Rest strategies with fixed time may not allow full recovery in consecutive sets, and this may intensify the increase in BP and HR5,9,11. It may be more appropriate to establish the rest interval according to the exercise execution time (or time under tension), depending on the overload with one is working. Unfortunately, it was not possible to find studies that have confirmed this hypothesis, which would be especially important in the context of training programs for patients at risk of cardiovascular complications.
Thus, this study investigated the influence of two rest intervals established according to the time under tension, in multiple sets of resistance exercise, performed with different repetition maximums, by normotensive individuals, on acute responses of HR and systolic BP (SBP) and, consequently, of the rate-pressure product (RPP).
Methods
Sampling
Twenty volunteers (26 ± 5 years; 70.9 ± 8.1 kg, 173.9 ± 7.0 cm), with 6 to 12 months of experience in resistance training, participated in this study.
The following exclusion criteria were observed: a) use of drugs that could influence cardiovascular responses at rest or during exercise, b) musculoskeletal limitations that would cause the exercises to be contraindicated c) diagnosis of hypertension, heart disease or other cardiovascular problem that would cause the exercises to be contraindicated or which would influence the results.
The study was approved by the Institutional Ethics Committee and all participants signed an informed consent form, as recommended by the National Health Council (Resolution 196/96).
Determination of workloads - 6 and 12 repetition maximum (RM)
Four visits were required for conducting the tests that established the workloads associated with the execution of 6 RM and 12 RM on the leg press, as well as for checking the reliability of the results obtained. The horizontal leg press was chosen because it involves large groups of muscles and, therefore, it supposedly has greater impact on blood pressure values. Moreover, it is an exercise that is easy to do, which is often included in exercise routines prescribed for patients with cardiovascular disease.
Before the RM tests were conducted, the subjects performed a specific warm-up, which consisted in the execution of 12 repetitions with workload equivalent to 30% of the maximum workload predicted. Every day, the subjects could make up to 5 attempts to successfully complete the tests, with an interval of 5 min between each attempt.
The tests of 6 RM and 12 RM were conducted on different days, with an interval of at least 48 h in between. The subjects were verbally stimulated so as to keep the high level of stimulation during the exercises. The weights used were previously weighed on a precision scale. If it was not possible to determine the workload associated with 6 RM or 12 RM by the 5th attempt, a new date was scheduled, also after an interval of at least 48 h. The reproducibility of the RM tests was tested by the intraclass correlation coefficient (ICC), and it proved to be satisfactory (6 RM ICC = 0.89; p < 0.01 and 12 RM ICC = 0.85; p < 0.01).
Experimental protocol
Once the 6 RM and 12 RM workloads had been determined, the subjects underwent 4 random protocols of exercises, in an order defined in a counterbalanced way. Each session took place on a specific day, with a total of other 4 visits to the laboratory, with intervals of 48 hours in between. All subjects performed the following procedures: a) three "6 RM" sets with interval of 1:3; b) three "6 RM" sets with interval of 1:5; c) three "12 RM" sets with interval of 1:3; and d) three "12 RM" sets with interval of 1:5.
The subjects were instructed to observe the following recommendations before the exercise sessions: a) not to do any type of physical activity within 48 hours before the test; b) abstain from alcohol, caffeinated drinks or stimulants for 24 hours; c) make as little effort as possible during the trip to the laboratory.
Before performing the protocols, the subjects remained seated for 10 minutes, in a calm and quiet environment. Then, the HR and BP at rest were measured and the average HR of the last two 2 minutes was recorded, and the average of two measurements of BP made in the same period was also recorded. Then, the subjects performed a warm-up of 12 repetitions with 30% of the expected workload for the session. After the warm-up, the subjects rested for 5 minutes and started the exercise.
The cardiovascular variables were measured at rest and during the exercise, by using the same equipment, as described below:
a) Rest - the individuals remained seated for 10 minutes. The HR was measured continuously and the average of the last two minutes was recorded, by using heart rate monitor Polar S810 (Kempele, Finland). The SBP and diastolic blood pressure (DBP) were measured twice, between the 8th and 10th minutes, by the indirect auscultatory method, with the use of a mercury column manometer Heidji (São Paulo, Brazil). The standard of measurement followed the recommendations of the 5th Brazilian Guidelines on Hypertension12, with the measurements always made by the same observer, both at rest and during the exercise. The BP was measured in both arms and the largest measure was considered, in case of difference.
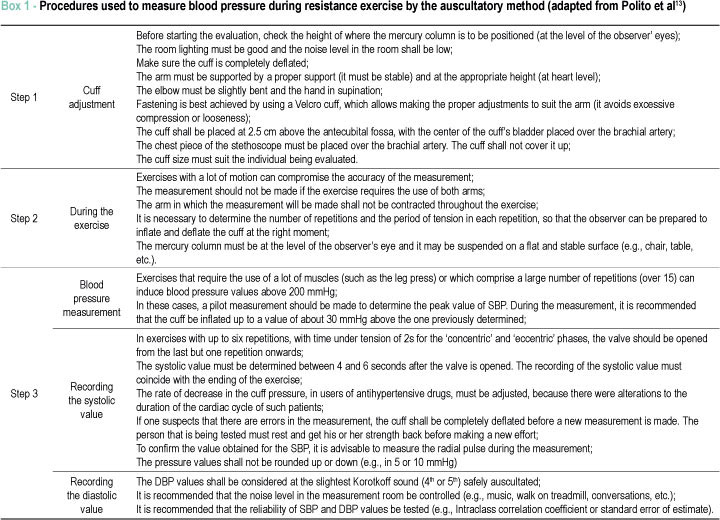
b) Exercise - The HR was measured on a continuous basis, and the highest value presented at the end of the sets was recorded. For measuring the BP, the recommendations previously validated for measurement during resistance exercises13,14 were observed, as detailed in Box 1.
In general, the valve opened before the end of the set, in order to record the systolic value between the last but one repetition and last repetition. A pilot measurement was made to determine the SBP peak value, so as to increase the pressure of the cuff to an approximate value of 30 mmHg higher, before the opening of the valve. The cuff was deflated at a rate of approximately 6 mmHg/s. The subjects were instructed not to curl their arms and to keep the left arm, used for the measurement, in supination, with elbows slightly flexed and supported on proper support. The measurements were made by the same trained observer, who was unaware of the purposes of this study.
To determine the reliability of the BP measurement at rest, two measurements of BP were made, 10 minutes apart from each other, in 20 subjects (ICC = 0.93 for intra-observer SBP; ICC = 0.86 for inter-observer SBP). The reliability of the measurement during exercise was tested in two sessions, 48 hours apart from each other, in the same 20 subjects (ICC = 0.84 and p = 0.03 for intra-observer SBP; ICC = 0.82 and p = 0.022 for inter-observer SBP).
In a previous study of validation14, there was evidence of a high correlation between the measurements made by auscultation and PPG, both at rest and in different repetition maximums for exercise of the lower limbs (p <0.05) (rest: r = 0.89; 6 RM: r = 0.85; 15 RM: r = 0.88). Moreover, the percentage of match in the classification into tertiles of the measurements in all situations was always above 60%, reaching 75% for SBP during the exercise. The non-parametric association between the methods, considering the levels of classification by tertiles at rest, 6 RM and 12 RM, also produced high correlation coefficients of Gamma and Kruskall (γ = 0.77 - 0.97, p < 0.05).
Determination of the rest intervals between sets
The duration of rest intervals between sets took into account the duration of the sets. The execution of the exercise was timed and the result was multiplied by three or 5, for determining an interval that would be in accordance, respectively, with the ratios of 1:3 or 1:5, between the execution time and rest time. To determine the execution time of the set, a progressive digital timer was used. The timer was started when the feet support platform moved and the timer was stopped when the platform touched its base at the end of the set.
The timer allowed restarting the measurement in a simple way, by using the same button used to interrupt such timer, thereby allowing the definition of precise intervals. To make it easier to view the rest period (1:3 or 1:5) and to minimize the chance of error in the interval calculation, a previously prepared conversion table was used.
Statistical analyses
The Shapiro-Wilk test was used to verify the normality of the data and the Levene's test was used to confirm the equality of variances. The stability of SBP and HR values measured at rest, in each one of the sessions, was tested by means of a one-way ANOVA. The isolated and combined influence of factors observed (RM, sets and intervals) on RPP, HR and SBP was tested by means of a three-way ANOVA, followed by Fisher's post-hoc test, with the adoption of p < 0.05 as a significance threshold. Software Statistica 6.0 (Statsoft, Tulsa, USA) was used on all calculations.
Results
There was no significant difference between the values of HR and SBP at rest measured in each one of the exercise sessions (F = 2.02; p = 0.78). Therefore, for analysis purposes, we adopted the lowest values obtained for these variables during the rest periods prior to exercise. The HR and SBP values during the sets proved to be always significantly higher than measurements taken at rest (F = 1.41 to 2.56; p = 0.027 to p = 0.039).
It is also important to highlight that the double of repetitions maximum (6 RM and 12 RM) was not related to the same proportion of variation in the absolute work load (weight in kg). The ratio between the loads of 6 and 12 RM was only 12% or, in absolute terms, 7.5 ± 0.8 kg.
The impact of the manipulated variables was different on HR and SBP. Thus, HR was significantly influenced by the isolated effect of the number of repetitions maximum (F = 7.33; p = 0.008) and the number of sets (F = 77.65; p < 0.001), but not by the rest interval (F = 3.00; p = 0.087). However, the combined effect of the sets with the intervals proved to be significant (F = 4.87; p = 0.02). As for the SBP, the isolated and statistically stronger effect resided in the number of sets (F = 63.33; p < 0.001), followed by the rest interval (F = 5.97; p = 0.017). The variable intensity had no significant independent effect (F = 0.042; p = 0.95).
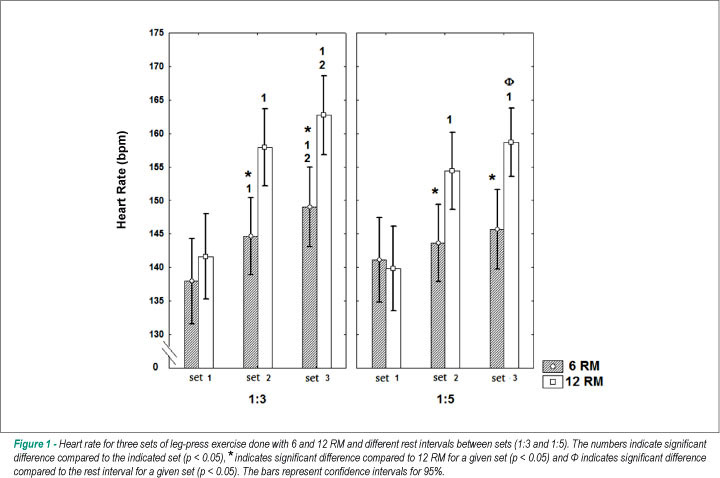
Figures 1 and 2 present the results of the post-hoc tests for HR and SBP. It was found that the influence of the number of sets systematically consisted in an increase in cardiovascular responses. On the other hand, the rest interval had the opposite influence and it even offset the cumulative effect of the sets in some cases, particularly with respect to SBP.
We also compared the absolute variations in each situation, considering the peak values recorded between the first and third sets. With regard to HR, for 6 RM protocols, the variation in the sets with an interval of 1:3 was significantly higher than that the one observed in 1:5 (Δ = 11.2 ± 1.1 bpm versus Δ = 4.5 ± 0.2 bpm, respectively) (F = 9.98; p = 0.002). As to the 12 RM workload, there was no significant difference in the variation in HR in sets with an interval of 1:3 compared to the variation observed in the 1:5 interval (Δ = 21.1 ± 2.2 bpm versus Δ = 18.9 ± 2.0 bpm, respectively) (F = 0.58; p = 0.83). The variations in SBP between the 1st and 3rd sets were influenced by the rest interval, regardless of the load. In protocols with 6 RM, the variations for the intervals of 1:3 and 1:5 were, respectively, 10.6 ± 0.9 mmHg and 6.6 ± 0.7 mmHg (F = 6.67; p = 0.02). For protocols of 12 RM, the variation with the interval of 1:3 was of 15.2 ± 1.1 mmHg, and the variation with the interval of 1:5 was of 8.4 ± 0.7 mmHg (F = 5.12; p = 0.04).
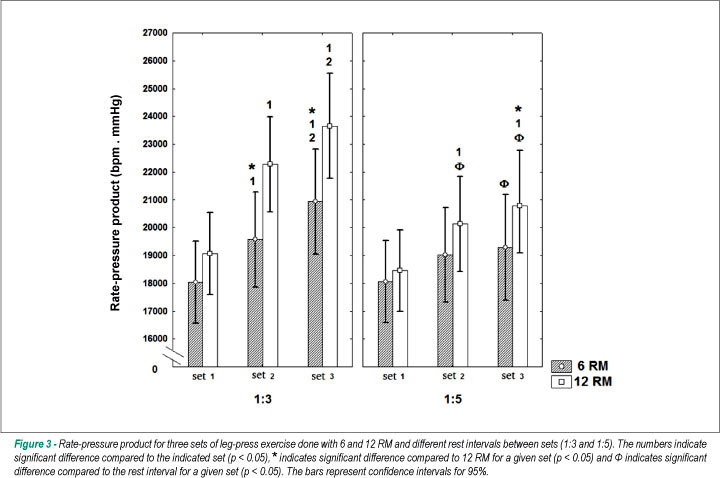
The results for SBP proved to be more sensitive to manipulation of the three training variables, considered separately or in combination. This reflected on the behavior of the RPP, in direct proportion to the number of repetitions maximum (F = 4.57, p = 0.036) and number of sets (F = 141.38, p <0.001), and in inverse proportion to the interval between sets (F = 5.38, p = 0.006).
Figure 3 shows the results for the post hoc tests referring to the standard deviation.
The variation between the first and third sets performed with an interval of 1:3 was of 2,892 ± 189 mmHg.bpm for 6 RM and 4,587 ± 300 mmHg.bpm for 12 RM (F = 4.17; p = 0.018). When we applied a longer interval (1:5), the variation in RPP for the 6 RM load was 1,224 ± 141 mmHg.bpm, while for 12 RM we obtained a delta of 2,332 ± 194 mmHg.bpm (F = 0.56; p = 0.58).
Discussion
This study compared the responses of HR, SBP and RPP during consecutive sets of resistance exercise, performed with different numbers of repetitions maximum and rest intervals, considering that these rest intervals were based on the total execution time of each set.
Both HR and SBP increased significantly in the course of the sets, regardless of the intensity and rest interval. However, the cardiovascular responses associated with the horizontal leg press were minimized by manipulating the rest time: when the proportion was higher compared to the time under tension, the HR value and especially the SBP value were lower. The longer rest interval was also associated with lower rise in HR and SBP during the sets, in the two pre-determined intensities. Thus, the exercise done with longer rest interval caused less cardiovascular stress for both intensities tested.
Interestingly, the average peak SBP value in the last sets of the study conducted by Gotshall et al5, measured by photoplethysmography, was 293 ± 21 mmHg, which is well above the value recorded in the last set of this study (181 ± 16 mmHg for the 12 RM protocol with progressive interval in the 1:3 ratio). This difference can be attributed to the time under tension in each set (one minute in the study conducted by Gotshall et al5versus 24 seconds in this study), but also, and perhaps mainly, to the BP measurement. As we known, even though the auscultatory method is suitable for comparing different resistance-exercise protocols, when such method is used on an inactive limb, it may underestimate absolute pressure values14,15. In other words, the auscultatory method is extremely useful in practical situations and it has proved valid and reproducible to indicate differences in BP responses to resistance exercise. Thus, this method is a useful strategy to develop training sessions with lower cardiovascular overload. Moreover, the auscultatory method should not be used to accurately establish blood pressure values during resistance exercise.
Studies that examine in detail the influence of rest intervals between sets and exercises on the behavior of BP and HR are relatively scarce. It was not possible to find studies that investigated the matter by adopting an approach similar to the one taken in this study.
Polito et al9 had young normotensive individuals do 4 sets of 8 RM, separated by fixed intervals of one and two minutes, and they also found higher values of blood pressure for the sequence with the shortest interval. The most pronounced cardiovascular responses at short rest intervals can be associated with lower systemic recovery from the stress generated by the exercise. The accumulation of metabolites, with consequent nerve stimulation via mechanical and chemical receptors, may potentiate these responses16.
In this sense, Ratamess et al10 observed the effects of different fixed rest intervals (30s, one, two, three and five minutes) on cardiovascular and metabolic responses throughout the course of 5 sets in two training intensities (5 RM and 10 RM), in the bench press exercise. No difference was found between the rest intervals, considering the peak values of HR in both training intensities. However, there was significant increase in HR as the sets were performed (p < 0.05), mainly for shorter rest intervals. The production of lactate was also higher for shorter rest intervals, which is suggestive of the relationship between accumulated fatigue due to insufficient rest and cardiovascular responses.
Our results indicated that the workload can also independently influence the responses of HR and SBP. By comparison with the protocol with a workload of 12 RM, the sets done with 6 RM had less impact on the cardiovascular responses for similar rest intervals. There may be a relationship between the time under tension (6 RM = 17 ± 3 s versus 12 RM = 29 ± 5 s) and such results. This possibility confirms the results reported by Lamotte et al17, who analyzed the effect of the execution of leg extension exercise in a leg extension machine, with workloads equivalent to 40% and 70% of an RM (4 sets with one-minute interval between sets), on the responses of HR and BP in patients with heart disease. The sets involving the intensity of 40% lasted 34s on average (for 17 repetitions) against 20s of the set done with 70% of the maximum workload (for 10 repetitions). There was a significant difference for the peak values of SBP, with higher cardiac overload for the protocol of lower intensity (p < 0.01). There was a cumulative effect of the sets on blood pressure (p < 0.01), which was attributed by the authors to the short rest interval applied.
In the present study, there was also a cumulative effect of the sets on HR and SBP responses, with greater increase from the second set onwards, especially for a shorter effort-rest interval. Similarly, Gotshall et al5 had three young and healthy individuals do three sets of 10 RM in the bilateral leg press (fixed rest interval of three minutes; speed of three seconds in the concentric and eccentric phases). At the end of each set, the values of SBP and DBP always proved to be significantly higher than the ones observed in the previous sets. Other studies have demonstrated that there is influence of the number of sets on cardiovascular responses2,17.
Two factors may be in the origin of the results referring to the cumulative effect of consecutive sets on cardiovascular responses. The first one would result from the fatigue accumulated due to the shorter rest time18. The second one takes into account the time under tension: the dynamic resistance exercise causes occlusion of blood vessels and it may, depending on its intensity and duration, lead to a compensatory baroreflex response, which is more common in exercises done until fatigue19,20.
The hemodynamic responses to muscular work in resistance exercises can also be linked to increased sympathetic activity and decreased parasympathetic activity, due to the greater activation of central command and muscle and joint mechanoreceptors16. The central mechanism involves the transmission of impulses from the motor cortex to the cardiovascular control center. On the other hand, the peripheral mechanism consists of a reflex pathway with multiple control bases21. The increased peripheral vascular resistance, caused by partial occlusion of blood flow, contributes to an imbalance between supply and demand of O2 in tissue. In fact, starting from 15% of the maximum voluntary contraction, it is possible to notice progressive obstruction of muscle blood flow22. As a result, the removal of metabolites (lactate, hydrogen, phosphate, adenosine, potassium etc) is hindered, by the stimulation of chemoreceptors to increase sympathetic nervous activity16.
Finally, the increase in blood pressure could also be influenced by the number of motor units requested. In this case, muscle and joint mechanoreceptors, sensitive to the increase in voluntary strength (recruitment of motor units) and the load on the joints, inform the cardiovascular control center about the need to modify the cardiovascular responses to regulate the flow23.
The increased peripheral vascular resistance associated with arterial occlusion during exercise is another factor to be considered. The leg press exercise, besides involving several major muscle groups, is also done in a posture that can hinder the perfusion of blood into active muscles, since the course of the main arteries that irrigate such muscles is changed by the hip flexion24. This problem is even greater during the transition from the concentric phase to the eccentric phase. In this context, the activation of baroreceptors and chemoreceptors may lead to a compensatory blood pressure response, so as to reach a satisfactory cardiac output during exercise.
Therefore, the cardiovascular responses to resistance exercise may be associated with the central adaptation resulting from the greater peripheral resistance. The increased need for perfusion is likely to be directly related to the inotropic capacity of the heart, since changes in HR tend to be slower than changes in SBP25. By the way, this pressure overload associated with resistance exercise can be beneficial from the standpoint of prophylaxis, especially for patients with chronic cardiovascular disease and users of anti-hypertensive medication26. Some studies have reported that coronary patients, under pharmacological treatment, can do resistance exercise of moderate intensity and the results of this practice include the improvement in global left ventricular function, especially of the ejection fraction26,27.
As for the rise in HR, the time under tension seems to exert important influence. Hunter et al28 compared the metabolic responses and heart rate responses to 10 exercises done at two speeds of contraction, a 'traditional' speed (2 sets of 8 repetitions with 65% of one RM, speed of execution of one second for the concentric phase and eccentric phase, one minute of rest) and a 'super slow' speed (2 sets of 8 repetitions with 25% of one RM, execution speed of 10s for the concentric phase and 5s for the eccentric phase, with the same interval and number of exercises). It was found that the 'traditional' protocol led to a significantly higher increase in HR compared to the 'super slow' protocol (143 ± 8 bpm against 113 ± 12 bpm).
Kleiner et al4 studied the acute cardiovascular response in isokinetic exercises in 6 subjects that did knee extension exercises at three execution speeds (50, 100 and 200°/s) until fatigue (70% of peak torque). There were no significant differences in HR, SBP, DBP and RPP values. However, at programmed speeds, the HR values varied between 163.3 ± 28.4 bpm (50º/s) and 183.5 ± 16.8 bpm (200º/s). In contrast, the SBP values were higher for a lower angular speed (SBP = 348.2 ± 18.1 mmHg for 50º/s versus SBP = 335.5 ± 27.4 mmHg for 200º/s), with influence on RPP (50º/s = 56,861 ± 514 mmHg.bpm; 100º/s = 58,875 ± 479 mmHg.bpm; 200º/s = 61,564 ± 460 mmHg.bpm). The authors explain that their results are justified by the characteristic of the sessions, with the number of repeats varying among 30 (50º/s), 80 (100º/s) and 140 (200º/s).
As the protocols at higher speed offer less resistance, and, as a significantly greater amount of repetitions was produced, the execution of the exercise would have gotten close to what is found in continuous dynamic exercises of long duration, with greater impact on the HR. On the other hand, the increase in SBP for lower speeds would be related to the greater production of force, compared to the higher angular speeds.
In general, it is not prudent to extrapolate results of isokinetic exercises to dynamic isotonic exercises. However, it is important to note that the effect of 'time under tension' on HR is confirmed by the results of Kleiner et al4, and it is also clear that SBP values are sensitive to the tension produced, with strong influence on the RPP.
Another example is found in the study conducted by Kawano et al29, who had young and middle-aged normotensive patients do a set of leg press exercises at three levels of intensity (40%, 60% and 80% of one RM). There was no difference in the HR values at the levels of intensity tested, in any of the groups. However, the peak pressure values of young subjects was higher than the values of middle-aged subjects, for all intensities, and significantly higher only for the intensity of 80% of one RM (young subjects = 190 mmHg versus middle-aged subjects = 150 mmHg, p < 0.05). The variation in SBP compared to rest (Δ) was significant for all intensities, and it was greater among young subjects, perhaps because their values at rest were generally lower (40% RM: young subjects = 34 mmHg versus middle-aged subjects = 18 mmHg; 60% RM: young subjects = 54 mmHg versus middle-aged subjects = 31 mmHg; 80% RM: young subjects = 73 mmHg versus middle-aged subjects = 42 mmHg; p < 0.05).
One may infer from these results that the single measurement of HR may not be sufficient to properly assess the cardiovascular overload produced by the resistance exercise. Therefore, we encourage the measurement of BP during the development of resistance training programs, especially for subjects in whom it is desirable to keep these responses under control (patients in cardiac rehabilitation, for example). That is why the protocol for measuring blood pressure during resistance exercise by the auscultation method, proposed by Polito and Farinatti13 and subsequently validated14, appears to be a viable and accessible option to most training centers.
In conclusion, multiple sets of resistance exercises for lower limbs cause significant and cumulative increase in cardiovascular responses, especially of BP, with an impact on the RPP. The level of cardiovascular stress associated with exercise did not depend only on the workload defined in terms of maximum repetitions, but also on the other training variables, especially the number of sets. On the other hand, longer rest intervals between sets contributed significantly to the reduction in RPP, BP and HR responses, while the workload and volume of training remained unchanged. The ratio between stimulation time and rest time, by itself, caused significant changes in cardiovascular responses, regardless of the maximum number of repetitions performed. Thus, the planning of rest intervals during the preparation of resistance training sessions appears to be a clinically important aspect for improving safety in such practice, especially in populations that are at a higher cardiovascular risk.
Further studies should be conducted to compare the hemodynamic responses associated with different strategies for the effort-rest ratio (fixed intervals, progressive intervals, division of sets, alternation of segments, etc). Such investigations are important to establish the most effective method to minimize the cardiovascular overload associated with multiple sets of resistance exercises, while the workload at training sessions is kept high.
Acknowledgments
This study was partially funded by CNPq (proceedings number 305729/2006-3) and by FAPERJ (proceedings E26/102.916/2008).
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
This study was partially funded by CNPq and by FAPERJ.
Study Association
This study is not associated with any post-graduation program.
References
- 1. Benn SJ, McCartney N, McKelvie RS. Circulatory responses to weight lifting, walking, and stair climbing in older males. J Am Geriatr Soc. 2003; 44 (2): 121-5.
- 2. MacDougall JD, Tuxen D, Sale DG, Moroz JR, Sutton JR. Arterial blood pressure response to heavy resistance exercise. J Appl Physiol. 1985; 58 (3): 785-90.
- 3. Polito MD, Simão R, Lira V, Nóbrega ACL, Farinatti PT. Série fracionada da extensão de perna proporciona maiores respostas cardiovasculares que séries contínuas. Arq Bras Cardiol. 2008; 90 (6): 382-7.
- 4. Kleiner DM, Blessing DL, Mitchell JW, Davis WR. A description of the acute cardiovascular responses to isokinetic resistance at three different speeds. J Strength Cond Res. 1999; 13 (4): 360-6.
- 5. Gotshall R, Gootman J, Byrnes W, Fleck S, Valovich T. Noninvasive characterization of the blood pressure response to the double-leg press exercise. JEPonline. 1999; 2 (4): 1-6.
- 6. Haslam DRS, McCartney N, McKelvie RS, MacDougall JD. Direct measurements of arterial blood pressure during formal weightlifting in cardiac patients. J Cardiopulm Rehabil. 1988; 8 (6): 213-25.
- 7. Overend T, Versteegh T, Thompson E, Birmingham T, Vandervoort A. Cardiovascular stress associated with concentric and eccentric isokinetic exercise in young and older adults. J Gerontol A Biol Sci Med Sci. 2000; 55 (4): 177-82.
- 8. Sale DG, Moroz DE, McKelvie RS, MacDougall JD, McCartney N. Effect of training on the blood pressure response to weight lifting. Can J Appl Physiol. 1994; 19 (1): 60-74.
- 9. Polito MD, Simão R, Nóbrega ACL, Farinatti PTV. Pressão arterial, frequência cardíaca e duplo-produto em séries sucessivas do exercício de força com diferentes intervalos de recuperação. Rev Port Ciênc Desp. 2004; 4 (3): 7-15.
- 10. Ratamess NA, Falvo MJ, Mangine GT, Hoffman JR, Faigenbaum AD, Kang J. The effect of rest interval length on metabolic responses to the bench press exercise. Eur J Appl Physiol. 2007; 100 (1): 1-17.
- 11. Willardson JM, Burkett LN. A comparison of 3 different rest intervals on the exercise volume completed during a workout. J Strength Cond Res. 2005; 19 (1): 23-6.
- 12. Sociedade Brasileira de Cardiologia. V Diretrizes brasileiras de hipertensão arterial. Arq Bras Cardiol. 2007; 89 (3): e24-79.
- 13. Polito MD, Farinatti PTV. Considerações sobre a medida da pressão arterial em exercícios contra-resistência. Rev Bras Med Esporte. 2003; 9 (1): 1-9.
- 14. Polito MD, Lira VA, Nóbrega ACL, Farinatti PTV. Blood pressure assessment during resistance exercise: comparison between auscultation and Finapres. Blood Press Monit. 2007; 12 (2): 81-6.
- 15. Wiecek E, McCartney N, McKelvie R. Comparison of direct and indirect measures of systemic arterial pressure during weightlifting in coronary artery disease. Am J Cardiol. 1990; 66 (15): 1065-9.
- 16. Rowell LB, O'Leary DS. Reflex control of the circulation during exercise: chemoreflexes and mechanoreflexes. J Appl Physiol. 1990; 69 (2): 407-18.
- 17. Lamotte M, Niset G, Van de Borne P. The effect of different intensity modalities of resistance training on beat-to-beat blood pressure in cardiac patients. Eur J Cardiovasc Prev Rehabil. 2005; 12 (1): 12-7.
- 18. Willardson JM. A Brief review: factors affecting the length of the rest interval between resistance exercise sets. J Strength Cond Res. 2006; 20 (4): 978-84.
- 19. Negrão CE, Rondon MUPB. Exercício físico, hipertensão e controle barorreflexo da pressão arterial. Rev Bras Hipertens. 2001; 8 (1): 89-95.
- 20. MacDougall JD, McKelvie RS, Moroz DE, Sale DG, McCartney N, Buick F. Factors affecting blood pressure during heavy weight lifting and static contractions. J Appl Physiol. 1992; 73 (4): 1590-7.
- 21. Carrington CA, Ubolsakka C, White MJ. Interaction between muscle metaboreflex and mechanoreflex modulation of arterial baroreflex sensitivity in exercise. J Appl Physiol. 2003; 95 (1): 43-8.
- 22. Edwards RH, Wiles CM. Energy exchange in human skeletal muscle during isometric contraction. Circ Res. 1981; 48 (6 Pt 2): I11-7.
- 23. Prabhakar NR, Peng YJ. Peripheral chemoreceptors in health and disease. J Appl Physiol. 2004; 96 (1): 359-66.
- 24. Lewis SF, Snell PG, Taylor WF, Hamra M, Graham RM, Pettinger WA, et al. Role of muscle mass and mode of contraction in circulatory responses to exercise. J Appl Physiol. 1985; 58 (1): 146-51.
- 25. McCartney N. Acute responses to resistance training and safety. Med Sci Sports Exerc. 1999; 31 (1): 31-7.
- 26. Marchionni N, Fattirolli F, Fumagalli S, Oldridge N, Del Lungo F, Morosi L, et al. Improved exercise tolerance and quality of life with cardiac rehabilitation of older patients after myocardial infarction: results of a randomized, controlled trial. Circulation. 2003; 107 (17): 2201-6.
- 27. Sociedade Brasileira de Cardiologia. I Diretriz de reabilitação cardíaca. Arq Bras Cardiol. 2005; 84 (5): 431-40.
- 28. Hunter GR, Seelhorst D, Snyder S. Comparison of metabolic and heart rate responses to super slow contra traditional resistance training. J Strength Cond Res. 2003; 17 (1): 76-81.
- 29. Kawano H, Nakagawa H, Onodera S, Higuchi M, Miyachi M. Attenuated increases in blood pressure by dynamic resistance exercise in middle-aged men. Hypertens Res. 2008; 31 (5): 1045-53.
Cardiovascular responses to resistance exercise are affected by workload and intervals between sets
Publication Dates
-
Publication in this collection
03 Sept 2010 -
Date of issue
Oct 2010
History
-
Reviewed
17 Mar 2010 -
Received
01 Aug 2009 -
Accepted
11 May 2010