SUMMARY
Uterine inversion is an uncommon complication of the puerperium and it is an even rarer complication of the non-puerperal period. In this way, uterine inversions are classified into two groups, being of puerperal origin due to obstetric problems and non-puerperal origin due to gynecological problems. In general, a non-puerperal uterine inversion occurs as a possible complication of a sub mucosal leiomyoma, after an expansive process, a dilation of the cervix occurs and thus its protuberance over the vaginal canal.
KEYWORDS:
Uterine inversion; Uterine diseases; Leiomyoma
RESUMO
A inversão uterina é uma complicação incomum do puerpério e é uma complicação ainda mais rara do período não puerperal. Dessa forma, as inversões uterinas são classificadas em dois grupos, sendo as de origem puerperal decorrentes de problemas obstétricos e as inversões de origem não puerperal decorrentes de problemas ginecológicos. Em geral, a inversão uterina não puerperal decorre como uma possível complicação de um leiomioma submucoso — após o processo expansivo, ocorre a dilatação do colo uterino e, dessa forma, a sua protusão sobre o canal vaginal.
PALAVRAS-CHAVE:
Inversão uterina; Doenças uterinas; Leiomioma
INTRODUCTION
In general terms, uterine inversions are divided into two groups: those of puerperal origin and non-puerperal inversions11. Kouamé A, Koffi SV, Adjoby R, Diomandé FA, Effoh D, Oussou C, et al. Non-puerperal uterine inversion in a young woman: a case report. J West Afr Coll Surg. 2015;5(3):78-83.–33. Teimoori B, Esmailzadeh A. A large uterine leiomyoma leading to non-puerperal uterine inversion: a case report. Intern J Reprod Biomed (Yazd). 2017;15(1):55-6.. As a rule, most cases published to date report puerperal uterine inversion as more frequent and common22. Mihmanli V, Kilic F, Pul S, Kilinc A, Kilickaya A. Magnetic resonance imaging of non-puerperal complete uterine inversion. Iran Radiol. 2015;12(4):e9878.–44. Kirbas A, Daglar K, Kara O, Sucak A, Caglar T. Non-puerperal uterine inversion due to submucous myoma in a woman: a case report. J Exp Ther Oncol. 2016;11(3):221-3..
Non-puerperal uterine inversion is scarcely recorded in the literature and, among the reported cases, that caused by submucosal leiomyoma is the most frequently described condition and, generally, in black women11. Kouamé A, Koffi SV, Adjoby R, Diomandé FA, Effoh D, Oussou C, et al. Non-puerperal uterine inversion in a young woman: a case report. J West Afr Coll Surg. 2015;5(3):78-83.,44. Kirbas A, Daglar K, Kara O, Sucak A, Caglar T. Non-puerperal uterine inversion due to submucous myoma in a woman: a case report. J Exp Ther Oncol. 2016;11(3):221-3.–66. Kulkarni KK, Ajmera SK. A rare case of non-puerperal acute uterine inversion. J Obstet Gynaecol India. 2014;64(5):364-5..
Thus, the differential of the expelled myomas is associated with the capacity of the myoma to distend the endometrial cavity (by the increase in size and location), whereas this process triggers an inflammatory reaction on the uterine wall, leading to a contraction of response as an attempt to expel the tumor, justifying the nomenclature as expelled myoma77. Gonçalves ER, Bezerra LRPS, Karbage SAL, Rocha AP. Inversão uterina não puerperal em paciente jovem por mioma parido gigante: relato de caso e revisão de literatura. Rev Med UFC. 2016;56(2):58-62..
As for the diagnosis of non-puerperal uterine inversion, it is taken from chronic signs (which mainly include irregular transvaginal bleeding, anemia and sensation of mass being externalized by the vaginal introitus) and from acute signs (which include pelvic pain and intense vaginal bleeding)11. Kouamé A, Koffi SV, Adjoby R, Diomandé FA, Effoh D, Oussou C, et al. Non-puerperal uterine inversion in a young woman: a case report. J West Afr Coll Surg. 2015;5(3):78-83.,33. Teimoori B, Esmailzadeh A. A large uterine leiomyoma leading to non-puerperal uterine inversion: a case report. Intern J Reprod Biomed (Yazd). 2017;15(1):55-6.,44. Kirbas A, Daglar K, Kara O, Sucak A, Caglar T. Non-puerperal uterine inversion due to submucous myoma in a woman: a case report. J Exp Ther Oncol. 2016;11(3):221-3.,88. Rathod S, Samal SK, Pallavee P, Ghose S. Non puerperal uterine inversion in a young female: a case report. J Clin Diagn Res. 2014;8(9):OD01-2.,99. Casanova J, Huang KG, Adlan AS, Artazcoz S. Uterine inversion caused by a submucous leiomyoma. J Gynecol Surg. 2014;29(6):294-6.. Some studies highlight the occurrence of ureterovaginal fistula and acute urinary retention, and, as a rule, urinary events are justified by several reports that describe extrinsic urethral compression as a closely associated factor11. Kouamé A, Koffi SV, Adjoby R, Diomandé FA, Effoh D, Oussou C, et al. Non-puerperal uterine inversion in a young woman: a case report. J West Afr Coll Surg. 2015;5(3):78-83.,44. Kirbas A, Daglar K, Kara O, Sucak A, Caglar T. Non-puerperal uterine inversion due to submucous myoma in a woman: a case report. J Exp Ther Oncol. 2016;11(3):221-3.,66. Kulkarni KK, Ajmera SK. A rare case of non-puerperal acute uterine inversion. J Obstet Gynaecol India. 2014;64(5):364-5.–99. Casanova J, Huang KG, Adlan AS, Artazcoz S. Uterine inversion caused by a submucous leiomyoma. J Gynecol Surg. 2014;29(6):294-6..
In time, it is still valid to mention that complaints of pelvic pain and transvaginal bleeding are characterized as the main manifestations recorded in the literature77. Gonçalves ER, Bezerra LRPS, Karbage SAL, Rocha AP. Inversão uterina não puerperal em paciente jovem por mioma parido gigante: relato de caso e revisão de literatura. Rev Med UFC. 2016;56(2):58-62.. Scientific considerations also describe that the rectal examination is a complementary diagnostic examination of great value in order to confirm the absence of the uterus in the pelvis and to rule out elemental diagnostic doubts in more severe uterine inversions77. Gonçalves ER, Bezerra LRPS, Karbage SAL, Rocha AP. Inversão uterina não puerperal em paciente jovem por mioma parido gigante: relato de caso e revisão de literatura. Rev Med UFC. 2016;56(2):58-62..
Complementary imaging tests, such as nuclear magnetic resonance and ultrasonography are mentioned in the literature as tools to support the diagnosis because they help with any doubts found in the physical examination, as well as support surgeons for the establishment of surgical planning and approach77. Gonçalves ER, Bezerra LRPS, Karbage SAL, Rocha AP. Inversão uterina não puerperal em paciente jovem por mioma parido gigante: relato de caso e revisão de literatura. Rev Med UFC. 2016;56(2):58-62..
The treatment to be instituted may vary according to the patient's current clinical situation and previous history66. Kulkarni KK, Ajmera SK. A rare case of non-puerperal acute uterine inversion. J Obstet Gynaecol India. 2014;64(5):364-5.,88. Rathod S, Samal SK, Pallavee P, Ghose S. Non puerperal uterine inversion in a young female: a case report. J Clin Diagn Res. 2014;8(9):OD01-2.,99. Casanova J, Huang KG, Adlan AS, Artazcoz S. Uterine inversion caused by a submucous leiomyoma. J Gynecol Surg. 2014;29(6):294-6.. Abdominal or vaginal hysterectomies are commonly recommended for women with established offspring44. Kirbas A, Daglar K, Kara O, Sucak A, Caglar T. Non-puerperal uterine inversion due to submucous myoma in a woman: a case report. J Exp Ther Oncol. 2016;11(3):221-3.–66. Kulkarni KK, Ajmera SK. A rare case of non-puerperal acute uterine inversion. J Obstet Gynaecol India. 2014;64(5):364-5.. The option of vaginal myomectomy may be indicated for cases in which the malignancy is ruled out; as for cases of uterine inversion in which the malignancy is installed, the literature supports radical abdominal hysterectomy11. Kouamé A, Koffi SV, Adjoby R, Diomandé FA, Effoh D, Oussou C, et al. Non-puerperal uterine inversion in a young woman: a case report. J West Afr Coll Surg. 2015;5(3):78-83.,22. Mihmanli V, Kilic F, Pul S, Kilinc A, Kilickaya A. Magnetic resonance imaging of non-puerperal complete uterine inversion. Iran Radiol. 2015;12(4):e9878.,66. Kulkarni KK, Ajmera SK. A rare case of non-puerperal acute uterine inversion. J Obstet Gynaecol India. 2014;64(5):364-5.,99. Casanova J, Huang KG, Adlan AS, Artazcoz S. Uterine inversion caused by a submucous leiomyoma. J Gynecol Surg. 2014;29(6):294-6..
CASE DESCRIPTION
MPR, 55 years old, female, black, stay-at-home mom, GIIIPIIIA0 (two NB and one caesarean section), was admitted to the Gynecology outpatient care of Hospital Universitário Materno Infantil da UFMA (HUMI-UFMA) with complaints of lumbar pain, urinary incontinence for six months, with uterus externalized by the vaginal introitus, characterizing the diagnostic impression of uterine prolapse. The clinical state also included abdominal pain in the Right Iliac Fossa (RIF), irregular menstrual cycles with increased flow and average duration of three days.
At physical examination: blood pressure: 130x80 mmHg, heart rate: 82 bpm, respiratory rate: 18 bpm, regular general state, paleness 2+/4+, hydrated, acyanotic, anicteric, afebrile. Abdomen: hydro-aerial sounds present (RHA+), tympanic to percussion, absence of palpable masses or visceromegaly, superficial pain to palpation in RIF, negative decompression in the whole abdomen, Pfannenstiel incision scar visualized in the abdomen. On genital examination: total uterine prolapse, with visible genital bleeding; atrophic uterine body with mucosal dryness; uterine cervix undetermined, not being possible to determine its anatomical limits. Pap smear (06/16/2016 - negative for epithelial lesions).
Personal morbid antecedents: diabetes mellitus type II and systemic arterial hypertension; makes use of glyphage 500 mg and olmesartan + hydrochlorothiazide 40 mg + 12.5 mg. Laboratory exams (Complete Blood Count, Creatinine, Urea, Glycaemia and Urine Culture) and imaging (Pelvis CT) were requested, then she was admitted to the service for diagnostic investigation and treatment.
During hospitalization, the patient developed a good general condition, with some episodes of transvaginal bleeding and elimination of yellowish fetid odor secretion, with prolapse being hydrated with AGE on alternate days. Complete blood count presented: Hemoglobin (Hb) at 6.70 g/dL, Hematocrit (Ht) at 26%, Leukocytes at 8,600/uL without left shift, platelets 319,000/uL, Creatinine at 0.8mg/dL, Urea at 23mg/dL, Urine 1 normal and negative Urine Culture. As practice, three red blood cell concentrates were prescribed to control anemia, as well as Metronidazole EV of 8/8h for seven days for bacterial vaginosis.
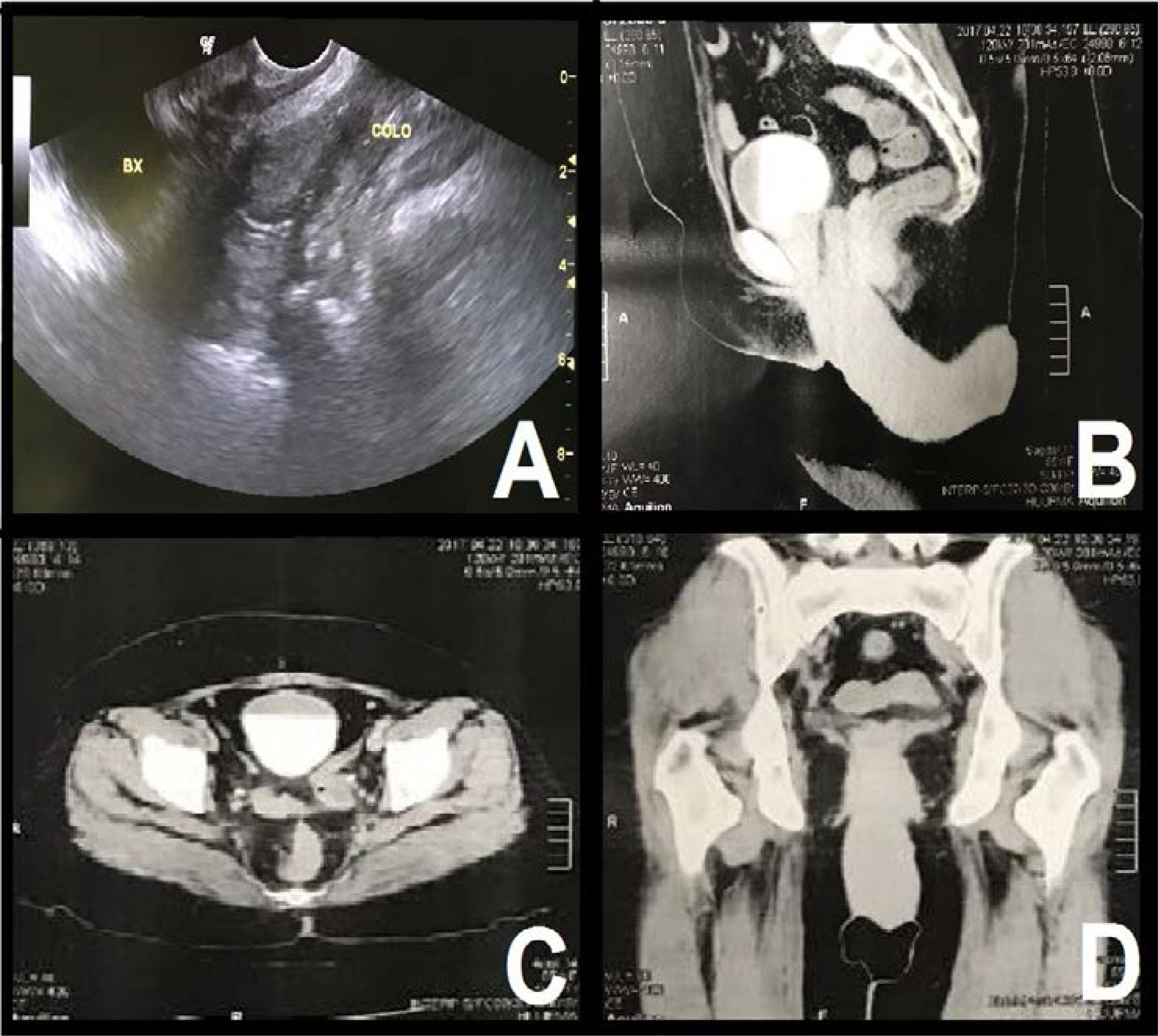
TVUS showed uterine prolapse with uterine myoma (Figure 1A).
Imaging exams. A: TVUS with uterine myoma in uterine prolapse - B: Pelvic CT sagittal cut - C: Pelvic CT axial cut - D: Pelvic CT coronal cut. Vieira, GTB. São Luís - MA, 2018.
Pelvis CT pelvis showed complete uterine prolapse; bladder with irregular contours and spaced walls, especially on its floor, with an apparent low bladder component; no filling failure ureters, with low insertion ureteral meatus; absence of free fluid or lymph node enlargement in the pelvis; absence of adnexal masses; bone structures without particularities and abdominal wall without abnormalities (Figures 1B, C, D).
After stabilization of the condition (Hb: 9.5 g/dL and Ht: 38%), with volume expansion of crystalloids and blood transfusion, she presented a favorable opinion from anesthesiology and cardiology, followed by a surgical procedure on the 16th Day.
Surgical report: Proposed surgery: Vaginal hysterectomy + bilateral anexectomy. Patient in lithotomy position, under spinal anesthesia, asepsis and antisepsis. Surgical findings: Uterine prolapse, with inverted uterus and uterine fundus externalizing under the expelled myoma (Figures 2A, B), there was no significant intraoperative blood loss without intercurrences during the surgical procedure, opening of the posterior wall of the uterus (Figure 2C) with visualization, section and bilateral ligature of the round and annexes ligaments (Figure 2D), lowering of the bladder, clamping, sectioning and ligature of the uterine arteries (Figure 3A), of the cardinal and uterus ligaments bilaterally (Figure 3B), removal of surgical piece (uterus and annexes) (Figure 3C), bilateral adnexectomy was performed with revision of hemostasis and closure of the vaginal vault (Figure 3D), the excisional material was referred for anatomopathological analysis. Bladder drainage: functioning and with clear diuresis. Rectal touch without alteration and cleansing of the perineum. The patient leaves the operating room in good condition.
A: Uterine prolapse with inverted uterus - B: Mobilization of the surgical piece - C: Opening of the posterior wall - D: Ligature of the round ligament and annex. Vieira, GTB. São Luís - MA, 2018.
A: Ligature of the uterine arteries - B: Ligature of the cardinal and uterosacral ligaments - C: Surgical piece (uterus and annexes) - D: Closure of the vaginal vault. Vieira, GTB. São Luís - MA, 2018.
On the 17th Day and 1st Post-op Day, she complained of moderate intensity pelvic pain, with prescription of tramadol 100 mg + 250 ml SF0, 9%, satisfactory diuresis and no transvaginal bleeding.
On the 18th Day and 2nd Post-op Day, she presented good general condition, without complaints, communicative, acyanotic, anicteric, afebrile.
She was discharged on the 19th Day and 3rd Post-op Day, with no complaints, with preserved physiological eliminations, good general condition, lucid, oriented in time and space, paleness +1/+4, hydrated, acyanotic, anicteric, afebrile, eupneic in ambient air, abdomen flaccid, rounded, painless to superficial and deep palpation, RHA+, without visceromegaly, lower limbs without edema, well perfused, without transvaginal bleeding. She received return orientations for outpatient consultation in 15 days with result of anatomopathological examination and US of pelvis for follow-up.
In the outpatient return, she was in good general condition, lucid, oriented in time and space, colored, hydrated, anicteric, afebrile, absence of transvaginal bleeding and secretions, anatomopathological report without criteria for malignancy, presenting in the uterine body: intramural leiomyomas and a larger submucosal, adenomyomas. In cervix: chronic cervicitis with erosion and ectocervical mucosa presenting irregular acanthosis and common parakeratosis of uterine prolapse. US: no change worthy of note.
Thus, the outcome of the clinical case continues discharged from gynecological surgery, with improvement of the patient's body perception and, consequently, quality of life, in aspects related mainly to sexual activity.
DISCUSSION
Uterine inversion is an uncommon complication of the puerperium and is an even rarer complication of the non-puerperal period11. Kouamé A, Koffi SV, Adjoby R, Diomandé FA, Effoh D, Oussou C, et al. Non-puerperal uterine inversion in a young woman: a case report. J West Afr Coll Surg. 2015;5(3):78-83.. Thus, uterine inversions are classified into two groups, being those of puerperal origin due to obstetric problems and inversions of non-puerperal origin due to gynecological problems22. Mihmanli V, Kilic F, Pul S, Kilinc A, Kilickaya A. Magnetic resonance imaging of non-puerperal complete uterine inversion. Iran Radiol. 2015;12(4):e9878.,33. Teimoori B, Esmailzadeh A. A large uterine leiomyoma leading to non-puerperal uterine inversion: a case report. Intern J Reprod Biomed (Yazd). 2017;15(1):55-6..
The uterine inversion of non-puerperal origin reported more frequently in the literature stands out for those caused by benign submucosal leiomyoma and prevalent in black women, often of African origin11. Kouamé A, Koffi SV, Adjoby R, Diomandé FA, Effoh D, Oussou C, et al. Non-puerperal uterine inversion in a young woman: a case report. J West Afr Coll Surg. 2015;5(3):78-83.–55. Song YJ, Yang J, Yun HS, Lee SK, Kim HG, Lee DH, et al. Non-puerperal uterine inversion presented with hypovolemic shock. J Menopausal Med. 2016;22(3):184-7..
Non-puerperal uterine inversion occurs less frequently in postmenopausal women and its pathophysiology is associated with the traction effect of lesions in benign masses22. Mihmanli V, Kilic F, Pul S, Kilinc A, Kilickaya A. Magnetic resonance imaging of non-puerperal complete uterine inversion. Iran Radiol. 2015;12(4):e9878.,66. Kulkarni KK, Ajmera SK. A rare case of non-puerperal acute uterine inversion. J Obstet Gynaecol India. 2014;64(5):364-5..
In young women of reproductive age, non-puerperal uterine inversion is frequently associated with leiomyosarcoma, rhabdomyosarcoma, malignant mixed müllerian tumor and endometrial polyp11. Kouamé A, Koffi SV, Adjoby R, Diomandé FA, Effoh D, Oussou C, et al. Non-puerperal uterine inversion in a young woman: a case report. J West Afr Coll Surg. 2015;5(3):78-83.,88. Rathod S, Samal SK, Pallavee P, Ghose S. Non puerperal uterine inversion in a young female: a case report. J Clin Diagn Res. 2014;8(9):OD01-2..
Leiomyomas are considered the most common gynecological disorders found in the gynecological specialty; however, non-puerperal uterine inversion by leiomyoma is classified as an extremely rare pathology11. Kouamé A, Koffi SV, Adjoby R, Diomandé FA, Effoh D, Oussou C, et al. Non-puerperal uterine inversion in a young woman: a case report. J West Afr Coll Surg. 2015;5(3):78-83..
The literature indicates that there is a great relationship of approximately 90% of non-puerperal uterine inversion with tumors, of which approximately 70% were leiomyomas and 20% malignant tumors, which justifies anatomopathological research in all situations88. Rathod S, Samal SK, Pallavee P, Ghose S. Non puerperal uterine inversion in a young female: a case report. J Clin Diagn Res. 2014;8(9):OD01-2..
In general, the etiology of uterine inversion is not clearly defined. The most plausible explanations are justified by a thin uterine wall, disordered growth of the tumor mass, size of the mass, its location, fixation of the mass in the uterine wall by only a single pedicle, dilation of the uterine cervix due to distension of the uterine cavity and dehiscence of tumor mass11. Kouamé A, Koffi SV, Adjoby R, Diomandé FA, Effoh D, Oussou C, et al. Non-puerperal uterine inversion in a young woman: a case report. J West Afr Coll Surg. 2015;5(3):78-83.,55. Song YJ, Yang J, Yun HS, Lee SK, Kim HG, Lee DH, et al. Non-puerperal uterine inversion presented with hypovolemic shock. J Menopausal Med. 2016;22(3):184-7.,88. Rathod S, Samal SK, Pallavee P, Ghose S. Non puerperal uterine inversion in a young female: a case report. J Clin Diagn Res. 2014;8(9):OD01-2.,99. Casanova J, Huang KG, Adlan AS, Artazcoz S. Uterine inversion caused by a submucous leiomyoma. J Gynecol Surg. 2014;29(6):294-6..
In general, non-puerperal uterine inversion occurs as a possible complication of a submucosal leiomyoma: after the expansion process, dilation of the uterine cervix occurs and, thus, its protrusion on the vaginal canal11. Kouamé A, Koffi SV, Adjoby R, Diomandé FA, Effoh D, Oussou C, et al. Non-puerperal uterine inversion in a young woman: a case report. J West Afr Coll Surg. 2015;5(3):78-83.,33. Teimoori B, Esmailzadeh A. A large uterine leiomyoma leading to non-puerperal uterine inversion: a case report. Intern J Reprod Biomed (Yazd). 2017;15(1):55-6.–55. Song YJ, Yang J, Yun HS, Lee SK, Kim HG, Lee DH, et al. Non-puerperal uterine inversion presented with hypovolemic shock. J Menopausal Med. 2016;22(3):184-7.,99. Casanova J, Huang KG, Adlan AS, Artazcoz S. Uterine inversion caused by a submucous leiomyoma. J Gynecol Surg. 2014;29(6):294-6..
Its diagnosis can be very complex. Thus, as a rule, the patient may present several clinical aspects, which are fundamental for the clinical diagnosis of non-puerperal uterine inversion11. Kouamé A, Koffi SV, Adjoby R, Diomandé FA, Effoh D, Oussou C, et al. Non-puerperal uterine inversion in a young woman: a case report. J West Afr Coll Surg. 2015;5(3):78-83.,22. Mihmanli V, Kilic F, Pul S, Kilinc A, Kilickaya A. Magnetic resonance imaging of non-puerperal complete uterine inversion. Iran Radiol. 2015;12(4):e9878.,66. Kulkarni KK, Ajmera SK. A rare case of non-puerperal acute uterine inversion. J Obstet Gynaecol India. 2014;64(5):364-5.. In this way, the diagnosis is organized into signs and symptoms of chronic and acute order55. Song YJ, Yang J, Yun HS, Lee SK, Kim HG, Lee DH, et al. Non-puerperal uterine inversion presented with hypovolemic shock. J Menopausal Med. 2016;22(3):184-7..
The chronic signs that stand out are intense/irregular vaginal bleeding, iron deficiency (anemia) and sensory perception of a bulky mass coming down the vagina11. Kouamé A, Koffi SV, Adjoby R, Diomandé FA, Effoh D, Oussou C, et al. Non-puerperal uterine inversion in a young woman: a case report. J West Afr Coll Surg. 2015;5(3):78-83.,55. Song YJ, Yang J, Yun HS, Lee SK, Kim HG, Lee DH, et al. Non-puerperal uterine inversion presented with hypovolemic shock. J Menopausal Med. 2016;22(3):184-7.,88. Rathod S, Samal SK, Pallavee P, Ghose S. Non puerperal uterine inversion in a young female: a case report. J Clin Diagn Res. 2014;8(9):OD01-2..
The acute signs that stand out are an intense pain in the pelvic floor and intense vaginal bleeding55. Song YJ, Yang J, Yun HS, Lee SK, Kim HG, Lee DH, et al. Non-puerperal uterine inversion presented with hypovolemic shock. J Menopausal Med. 2016;22(3):184-7.. Routinely, some literature also highlights intermittent acute urinary retention, presentation of ureterovaginal fistula and vaginal secretion55. Song YJ, Yang J, Yun HS, Lee SK, Kim HG, Lee DH, et al. Non-puerperal uterine inversion presented with hypovolemic shock. J Menopausal Med. 2016;22(3):184-7.,99. Casanova J, Huang KG, Adlan AS, Artazcoz S. Uterine inversion caused by a submucous leiomyoma. J Gynecol Surg. 2014;29(6):294-6..
In summary, the main symptoms highlighted in non-puerperal uterine inversion are anemia due to irregular vaginal bleeding, vaginal (foul-smelling) secretion, abdominal or pelvic floor pain, mass in the vagina and urinary retention due to obstruction of the urethra11. Kouamé A, Koffi SV, Adjoby R, Diomandé FA, Effoh D, Oussou C, et al. Non-puerperal uterine inversion in a young woman: a case report. J West Afr Coll Surg. 2015;5(3):78-83.,99. Casanova J, Huang KG, Adlan AS, Artazcoz S. Uterine inversion caused by a submucous leiomyoma. J Gynecol Surg. 2014;29(6):294-6..
The literature describes a classification for the treatment of uterine inversion in which the option is according to the stage of the inversion22. Mihmanli V, Kilic F, Pul S, Kilinc A, Kilickaya A. Magnetic resonance imaging of non-puerperal complete uterine inversion. Iran Radiol. 2015;12(4):e9878.. In stage 1, the inversion of the uterus is said to be incomplete and is restricted to the intra-uterus with the fundus occupying the cavity22. Mihmanli V, Kilic F, Pul S, Kilinc A, Kilickaya A. Magnetic resonance imaging of non-puerperal complete uterine inversion. Iran Radiol. 2015;12(4):e9878.. In stage 2, the complete inversion of the fundus of the uterus through the fibromuscular colon is observed22. Mihmanli V, Kilic F, Pul S, Kilinc A, Kilickaya A. Magnetic resonance imaging of non-puerperal complete uterine inversion. Iran Radiol. 2015;12(4):e9878.. Stage 3 refers to total inversion with the fundus located in the vaginal vulva22. Mihmanli V, Kilic F, Pul S, Kilinc A, Kilickaya A. Magnetic resonance imaging of non-puerperal complete uterine inversion. Iran Radiol. 2015;12(4):e9878.. Finally, stage 4 is characterized by the involvement of the vagina in the inversion22. Mihmanli V, Kilic F, Pul S, Kilinc A, Kilickaya A. Magnetic resonance imaging of non-puerperal complete uterine inversion. Iran Radiol. 2015;12(4):e9878..
The delay in the treatment of uterine inversion can be very compromising, besides leading to constriction (strangulation) ring formation, cervical edema and tissue necrosis. In several studies, vaginal myomectomy followed by vaginal hysterectomy were instituted as definitive treatment, being the gold standard for those women who are perimenopausal, menopausal or postmenopausal44. Kirbas A, Daglar K, Kara O, Sucak A, Caglar T. Non-puerperal uterine inversion due to submucous myoma in a woman: a case report. J Exp Ther Oncol. 2016;11(3):221-3.–66. Kulkarni KK, Ajmera SK. A rare case of non-puerperal acute uterine inversion. J Obstet Gynaecol India. 2014;64(5):364-5.,88. Rathod S, Samal SK, Pallavee P, Ghose S. Non puerperal uterine inversion in a young female: a case report. J Clin Diagn Res. 2014;8(9):OD01-2..
However, depending on the situation, certain surgical approaches may be defined for the treatment of non-puerperal uterine inversion88. Rathod S, Samal SK, Pallavee P, Ghose S. Non puerperal uterine inversion in a young female: a case report. J Clin Diagn Res. 2014;8(9):OD01-2.. Thus, we can classify the approaches in two, with the abdominals using the Huntington and Haultain techniques, and the vaginal ones including the techniques of Kustner and Spinelle66. Kulkarni KK, Ajmera SK. A rare case of non-puerperal acute uterine inversion. J Obstet Gynaecol India. 2014;64(5):364-5.,88. Rathod S, Samal SK, Pallavee P, Ghose S. Non puerperal uterine inversion in a young female: a case report. J Clin Diagn Res. 2014;8(9):OD01-2.,99. Casanova J, Huang KG, Adlan AS, Artazcoz S. Uterine inversion caused by a submucous leiomyoma. J Gynecol Surg. 2014;29(6):294-6..
The literature suggests that patients who present in stage 1 of the inversion are those in which the repositioning of the uterus should often be evaluated and performed if feasible; however, for patients who present inversion in stages 2, 3 and 4, hysterectomy would be the best indication22. Mihmanli V, Kilic F, Pul S, Kilinc A, Kilickaya A. Magnetic resonance imaging of non-puerperal complete uterine inversion. Iran Radiol. 2015;12(4):e9878..
It is worth mentioning that in those patients in whom there is a desire to gestate or who are nulliparous, one must, whenever possible, opt for the abdominal approach and preservation of the uterus; otherwise, vaginal myomectomy followed by routine vaginal hysterectomy should be recommended11. Kouamé A, Koffi SV, Adjoby R, Diomandé FA, Effoh D, Oussou C, et al. Non-puerperal uterine inversion in a young woman: a case report. J West Afr Coll Surg. 2015;5(3):78-83.,22. Mihmanli V, Kilic F, Pul S, Kilinc A, Kilickaya A. Magnetic resonance imaging of non-puerperal complete uterine inversion. Iran Radiol. 2015;12(4):e9878.,44. Kirbas A, Daglar K, Kara O, Sucak A, Caglar T. Non-puerperal uterine inversion due to submucous myoma in a woman: a case report. J Exp Ther Oncol. 2016;11(3):221-3.,55. Song YJ, Yang J, Yun HS, Lee SK, Kim HG, Lee DH, et al. Non-puerperal uterine inversion presented with hypovolemic shock. J Menopausal Med. 2016;22(3):184-7.,88. Rathod S, Samal SK, Pallavee P, Ghose S. Non puerperal uterine inversion in a young female: a case report. J Clin Diagn Res. 2014;8(9):OD01-2..
CONCLUSIONS
The case reports a non-puerperal uterine inversion with myomatosis, which is a rare condition and, if not properly treated, it can evolve with major complications such as infection, anemia and hypovolemic shock.
As already mentioned, in the cases reported to date, the diagnosis was concrete regarding the visual inspection of externalized mass in the vaginal introitus, however, it is highlighted that the anatomopathological diagnosis is essential for patient follow-up.
CT, although it is not the gold standard diagnostic test for pelvic masses, may substitute the MRI, when conditions do not allow its use.
Finally, the therapeutic effect achieved with the use of the vaginal hysterectomy and bilateral anexectomy surgical intervention, in view of the improvements of the symptoms related to non-puerperal uterine inversion with myomatosis, is mainly regarding symptoms of urinary incontinence, increased sexual satisfaction and better perception of the image body.
-
Study carried out: Department of Gynecology, Health Sciences Sector of the Hospital Universitário da Universidade Federal do Maranhão, HU-UFMA.
ACKNOWLEDGEMENT
To Hospital Universitário da Universidade Federal do Maranhão/HU-UFMA.
Ethical aspects: We emphasize total exemption from direct or indirect financial interest with the publication of this article. We maintain that it did not require extra-institutional funds. The authors declare that there is no conflict of interest of the parties involved. CAAE: 82980218.0.0000.5086 and Consubstantiated Opinion of CEP: 2.525.672 (Approval 03/05/2018).
REFERENCES
-
1Kouamé A, Koffi SV, Adjoby R, Diomandé FA, Effoh D, Oussou C, et al. Non-puerperal uterine inversion in a young woman: a case report. J West Afr Coll Surg. 2015;5(3):78-83.
-
2Mihmanli V, Kilic F, Pul S, Kilinc A, Kilickaya A. Magnetic resonance imaging of non-puerperal complete uterine inversion. Iran Radiol. 2015;12(4):e9878.
-
3Teimoori B, Esmailzadeh A. A large uterine leiomyoma leading to non-puerperal uterine inversion: a case report. Intern J Reprod Biomed (Yazd). 2017;15(1):55-6.
-
4Kirbas A, Daglar K, Kara O, Sucak A, Caglar T. Non-puerperal uterine inversion due to submucous myoma in a woman: a case report. J Exp Ther Oncol. 2016;11(3):221-3.
-
5Song YJ, Yang J, Yun HS, Lee SK, Kim HG, Lee DH, et al. Non-puerperal uterine inversion presented with hypovolemic shock. J Menopausal Med. 2016;22(3):184-7.
-
6Kulkarni KK, Ajmera SK. A rare case of non-puerperal acute uterine inversion. J Obstet Gynaecol India. 2014;64(5):364-5.
-
7Gonçalves ER, Bezerra LRPS, Karbage SAL, Rocha AP. Inversão uterina não puerperal em paciente jovem por mioma parido gigante: relato de caso e revisão de literatura. Rev Med UFC. 2016;56(2):58-62.
-
8Rathod S, Samal SK, Pallavee P, Ghose S. Non puerperal uterine inversion in a young female: a case report. J Clin Diagn Res. 2014;8(9):OD01-2.
-
9Casanova J, Huang KG, Adlan AS, Artazcoz S. Uterine inversion caused by a submucous leiomyoma. J Gynecol Surg. 2014;29(6):294-6.
Publication Dates
-
Publication in this collection
Feb 2019
History
-
Received
24 May 2018 -
Accepted
20 June 2018