


A 64-year-old woman with a history of colon and cervical cancer presented with a six-month history of episodes of small, raised papules on her face. Her family history included cervical cancer (her sister) and gastric cancer (her father).
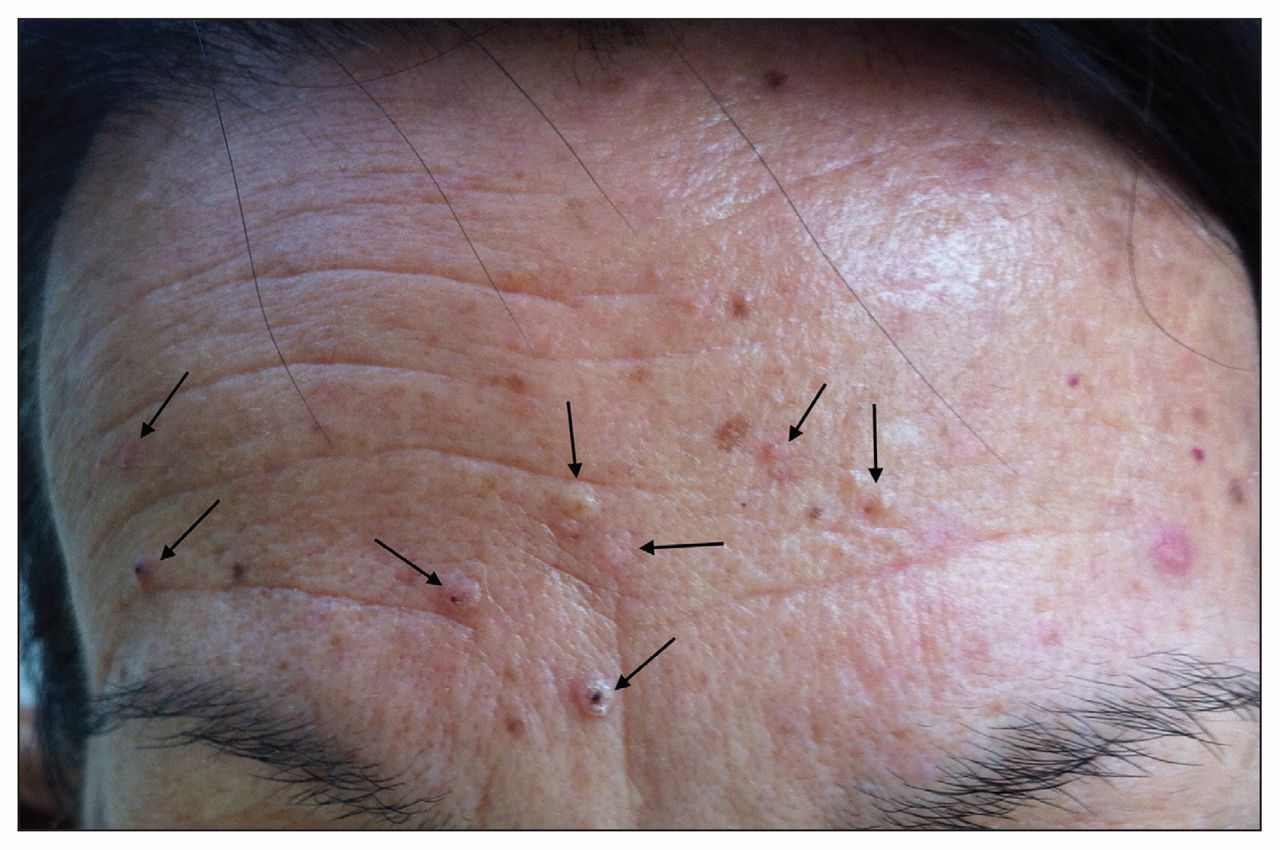
The patient had multiple skin-coloured to yellow–pink papules (Figure 1) on her face. A biopsy sample from the skin on her forehead confirmed a diagnosis of sebaceous adenoma, a benign, multilobular tumour with sebaceous differentiation. Sebaceous adenomas can be differentiated histologically from large sebaceous glands by a comparatively lower degree of cellular maturation.1 Based on the pathology findings, history and genetic testing, we diagnosed Muir–Torre syndrome.

Multiple skin-coloured to yellow–pink papules (arrows) on the face of a 64-year-old woman with a history of colon and cervical cancer. A skin biopsy confirmed a diagnosis of sebaceous adenoma resulting from Muir–Torre syndrome, which was confirmed with genetic testing.
Muir–Torre syndrome is an autosomal dominant cancer syndrome expressed clinically as cutaneous tumours (sebaceous neoplasms or multiple keratoacanthomas) and visceral malignant disease.1,2 It is related to Lynch syndrome (also known as hereditary nonpolyposis colorectal cancer), which accounts for 3%–5% of all colorectal cancers.3 Both Muir–Torre and Lynch syndromes are linked to germline mutations in the DNA mismatch repair genes MLH1, MLH3, MSH2 and MSH6.2,3 Sebaceous neoplasms occur in 9% of patients with Lynch syndrome.2 In patients with Muir–Torre syndrome, sebaceous neoplasms appear as pink-to-yellowish papules or nodules,1 which may precede visceral malignant disease in 22%–60% of patients.2
In our patient’s case, the results of the skin biopsy were the clue to the hereditary cancer syndrome, prompting genetic testing and cancer surveillance for her and her family. The patient had an MSH2 mutation, which is present in 90% of patients with Muir–Torre syndrome.3 Oral Fordyce granules appear at a higher rate among high-risk families than in the general population, and may be a useful clinical screening tool (Appendix 1, available www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.150171/-/DC1).4
Sebaceous neoplasms should prompt clinicians to consider Muir–Torre syndrome: biopsy and cancer screening should be considered in the setting of multiple, especially eruptive, facial papules and a patient or family history of cancer. Sebaceous hyperplasias alone are not an indication for screening.1 Management should emphasize surveillance for visceral malignant disease, including hemoccult testing, colonoscopy and pelvic examination with Papanicolaou testing, and endometrial biopsy or transvaginal ultrasound.2 Retinoids given orally have been used to treat sebaceous neoplasms.5
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

