


- © 2005 CMA Media Inc. or its licensors
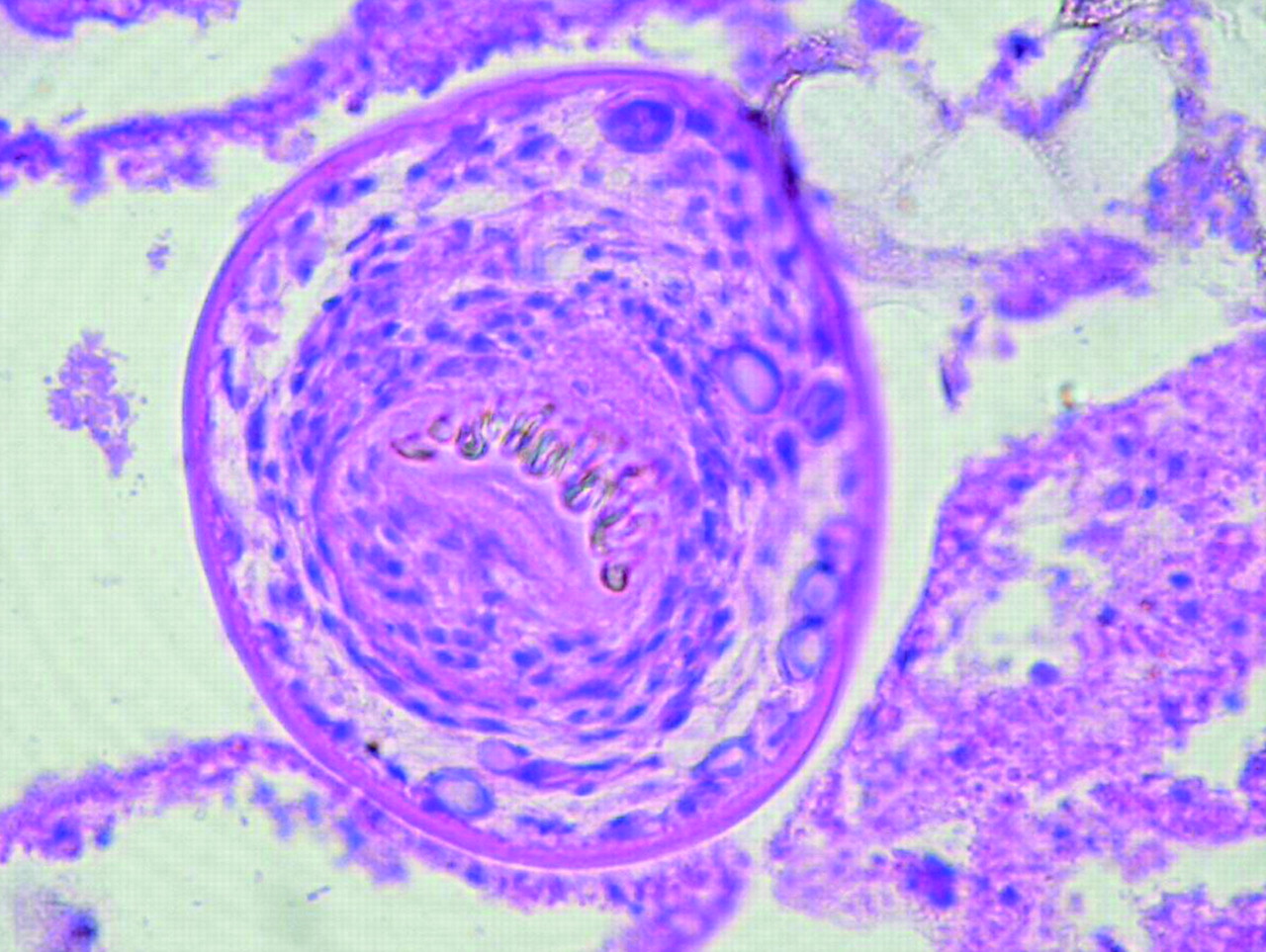
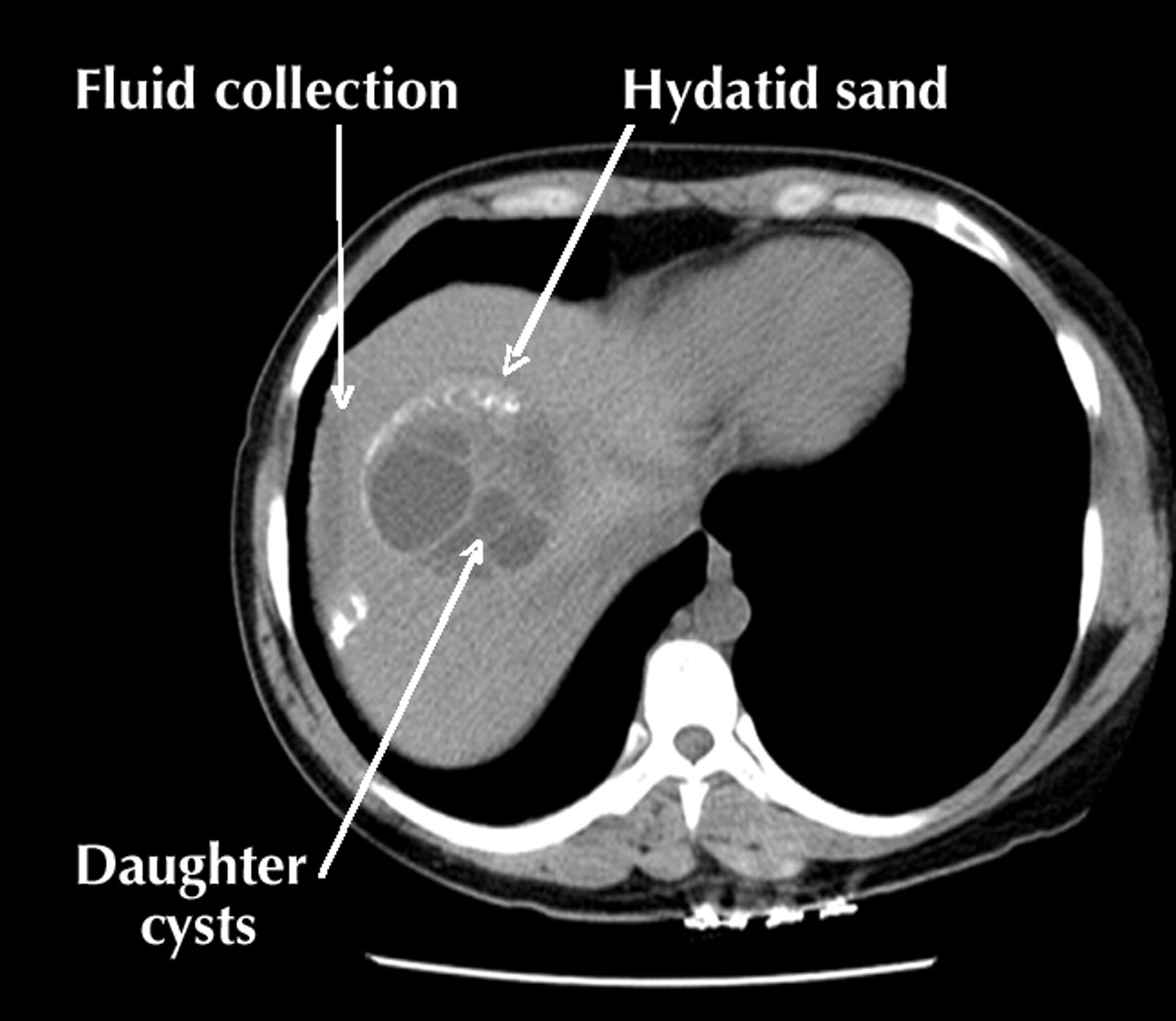
A 37-year-old woman presented to the emergency department with a 5-day history of increasing right upper quadrant pain, mild fever, chills and night sweats. She had had a hepatic hydatid cyst treated with “deworming drugs” in India 9 years previously. She was febrile (38.5°C) and had mild tenderness in the right upper quadrant of her abdomen, with no rebound, guarding, mass or hepatosplenomegaly. Routine blood tests yielded normal results. A CT of the abdomen and pelvis revealed a cystic lesion measuring 11.5 х 9.4 х 17 cm in the right lobe of the liver, with numerous small, hypodense “daughter” cysts, signs of hydatid sand and a region of free perihepatic fluid (Fig. 1). A possible rupture of the cyst or associated abscess was diagnosed and albendazole therapy given for 4 days to decrease the risk of secondary dissemination (hydatosis), after which the patient underwent surgical removal of the pericyst. Pathology confirmed the classic laminated cyst wall encircling many scolices with a double layer of hooklets, consistent with Echinococcus granulosus infection (Fig. 2). The patient was discharged on postoperative day 7 and prescribed three 28-day cycles of albendazole therapy. No recurrence was evident on CT imaging 9 months later.

Hydatid disease due to infection with the larval stage of the E. granulosus tapeworm is endemic to Eurasia, Africa, Australia and South America. However, with changing patterns of migration and immigration, cases are being seen in urban centres of the developed world. Upon eating feces- contaminated grass, sheep or other hoofed mammals ingest the tapeworm eggs, which hatch in the small intestine and travel in the blood stream to other organs, where hydatid disease develops. Carnivores subsequently eat flesh containing a hydatid cyst, after which eggs are released into the bowel and excreted into the feces. Humans become intermediate, nonpropagating hosts by ingesting contaminated vegetables or water.
Hydatid cysts most often affect the liver (68.8%–75.2% of cases) but also affect the lungs (17.2%–22.4%) and, less commonly, muscle, bone, brain and spleen.1 Cysts usually grow slowly over many months, and infected people often remain asymptomatic for life. However, up to 5% of infected people die, usually because of secondary infection, rupture of the cyst into adjacent structures, rupture causing anaphylaxis or intraperitoneal dissemination of the disease, and biliary complications such as obstruction or cholangitis.1 Abdominal pain, a palpable mass, fever, fatigue, weight loss, jaundice and nausea are common presenting signs. On CT scans, a hydatid cyst appears as a well-defined hypoattenuating lesion with a distinguishable wall; coarse wall calcifications occur in 50% of cases and daughter cysts in 75%.2 Serologic testing is more specific, but less sensitive, than most imaging modalities.
The goal of treatment is to prevent secondary complications of the disease. Surgical removal of the cyst is the treatment of choice;3 however, small, “daughter” cysts may be left behind. In cases of inoperable disease, cyclic therapy with a benzimidazole compound for 3–6 months has been found to cure disease in 10%–30% of cases, to slow progression in 50%–70% and to yield no change in 20%– 30%.1
In this issue

{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

