


Abstract
Background: Internationally, Indigenous Peoples experience worse surgical outcomes than non-Indigenous patients, but equity of surgical care is less well studied in Canada. This study compares outcomes after appendectomy in First Nations and non–First Nations patients.
Methods: In this population-based study, we reviewed administrative data of patients who underwent appendectomy between Apr. 1, 2004, and Mar. 31, 2017, in Northern Alberta. Demographic variables and characteristics of surgical care for First Nations and non–First Nations patients were collected. We identified adverse outcomes by the presence of predefined administrative codes. We identified variables related to a complex postoperative course (at least 1 of wound dehiscence, surgical site infection, abscess, bowel obstruction, pneumonia, deep vein thrombosis, sepsis, emergency department visit, readmission or death within 30 d after appendectomy) through a logistic regression model, and those related to longer length of stay using a Cox proportional hazards model.
Results: A total of 28 453 patients met the selection criteria, of whom 1737 (6.1%) had First Nations status. Compared to non–First Nations patients, First Nations patients were younger, lived farther away from the hospital of their appendectomy, were in lower socioeconomic quintiles, and had higher rates of obesity and diabetes (all p < 0.001). After adjustment for age, sex, distance to hospital, socioeconomic deprivation and comorbidities, First Nations status remained independently associated with higher rates of adverse outcomes (odds ratio 1.548, 95% confidence interval [CI] 1.384–1.733) and longer lengths of stay (hazard ratio 0.877, 95% CI 0.832–0.924).
Conclusion: Although rurality, comorbidities and socioeconomic status contributed to worse outcomes after appendectomy for First Nations patients, First Nations status remained independently associated with worse surgical outcomes. Surgical care, an integral component of health care delivery, must be improved for First Nations patients in order to achieve equitable health care.
Disparities between First Nations patients and non–First Nations patients exist in multiple health measures.1–3 Internationally, Indigenous Peoples experience worse outcomes across several surgical disciplines than non-Indigenous patients,4–6 and there is similar evidence pointing to a disparity in access to surgical care for Indigenous Peoples in Canada.7,8 Despite these health inequalities, research on the health needs of Indigenous Peoples in Canada is insufficient.9 The authors of a recent systematic review reported higher rates of adverse events after surgery for Indigenous patients than for non-Indigenous patients in Canada; however, their study had limited data on surgical outcomes after emergent general surgery procedures and highlighted risks of bias in current literature.10 Surgical care is an essential component of delivery of health care services, and equity in this domain is therefore necessary in fulfilling the obligations mandated for health equity set out by the United Nations Declaration on the Rights of Indigenous Peoples.11
Owing to the relative paucity of research, studies examining disparity of surgical outcomes for First Nations patients are both timely and merited. Population-based data of health outcomes linked with socioeconomic factors can help to identify inequities,12 and, similarly, surgical outcomes may be used to assess equity in surgical care.13–15 Iglesias and colleagues16 investigated the quality of surgical care from different care providers in Canada by examining rates of complications after appendectomy. Our objective was to compare outcomes of appendectomy between First Nations and non–First Nations populations in Northern Alberta in order to describe the current state of equity in surgical care delivery. We hypothesized that First Nations patients systemically experience worse surgical care than non–First Nations patients, which would be reflected in worse outcomes after appendectomy.
Methods
Study population
Alberta Health Services (AHS) is the organization charged with delivering medical care across Alberta. We retrospectively reviewed secondary administrative health data for patients in Northern Alberta who had undergone appendectomy. We included all hospital admissions during which an appendectomy procedure was performed between Apr. 1, 2004, and Mar. 31, 2017, in the AHS North, Edmonton and Central zones, which represent an estimated population of 2 402 715 residents.17
Data sources
We linked 3 administrative data sets accessed through AHS: the Discharge Abstract Database (DAD), National Ambulatory Care Reporting System (NACRS) and Provincial Registry. These databases collect information pertaining to inpatient hospital admissions, emergency department (ED) visits and annual records of patient coverage under the Alberta Health Care Insurance Plan, respectively. Since April 2002, the DAD and NACRS have used the enhanced Canadian version of the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10-CA) and the Canadian Classification of Health Interventions (CCI) for diagnosis and procedure codes,18 which were abstracted retrospectively by trained nosologists. We obtained de-identified data from the AHS Enterprise Data Warehouse with support from the Alberta Strategy for Patient Oriented Research (SPOR) Support Unit data platform.
Study cohort
We identified patients who had undergone appendectomy by the presence of the CCI code for appendectomy (1.NV.89*), which has been validated with a high level of agreement (sensitivity 98%, specificity 86%) between administrative codes and medical records.19 For patients with more than 1 hospital admission for appendectomy during the study period, we retained only the first admission in our cohort.
All patients within AHS have unique health care numbers, which do not identify First Nations status, and health care providers are not informed of patients’ insurance coverage. However, payment of health care services differs in that patients with First Nations status (as defined under the federal Indian Act) are financed nationally, whereas most other patients receive care through payment from the province of Alberta. As a result, First Nations status was identifiable based on provincial health premium payment history within the Alberta Health Care Insurance Plan, and this method has been validated and successfully used to trace patients with First Nations status.8,20 We referred to all other patients as non–First Nations.
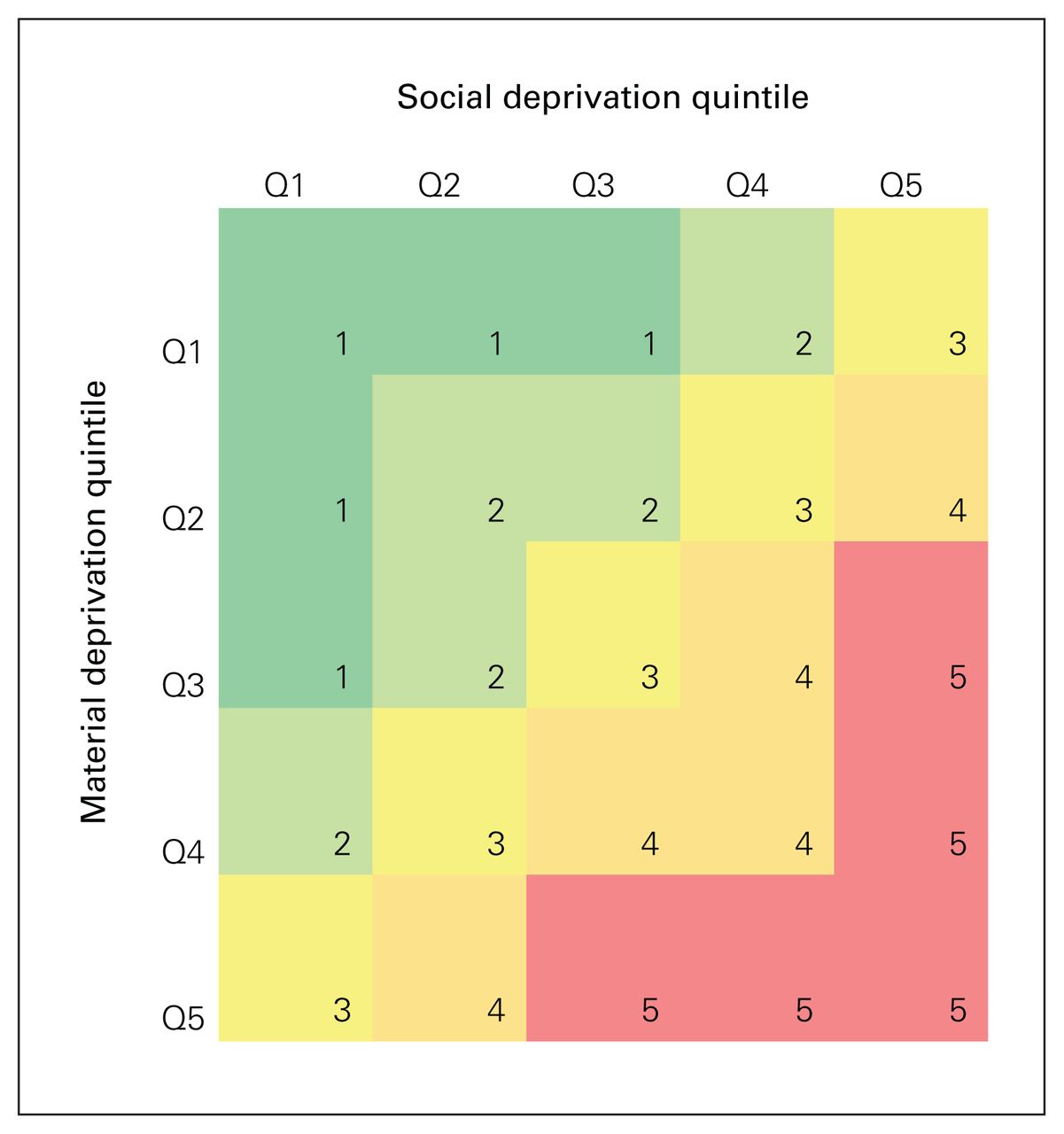
We also linked this data set by postal code to the Material and Social Deprivation Index21 to provide an estimate of material and social deprivation by quintile. We derived combined socioeconomic deprivation from these data (Figure 1), as is commonly done by other researchers.21
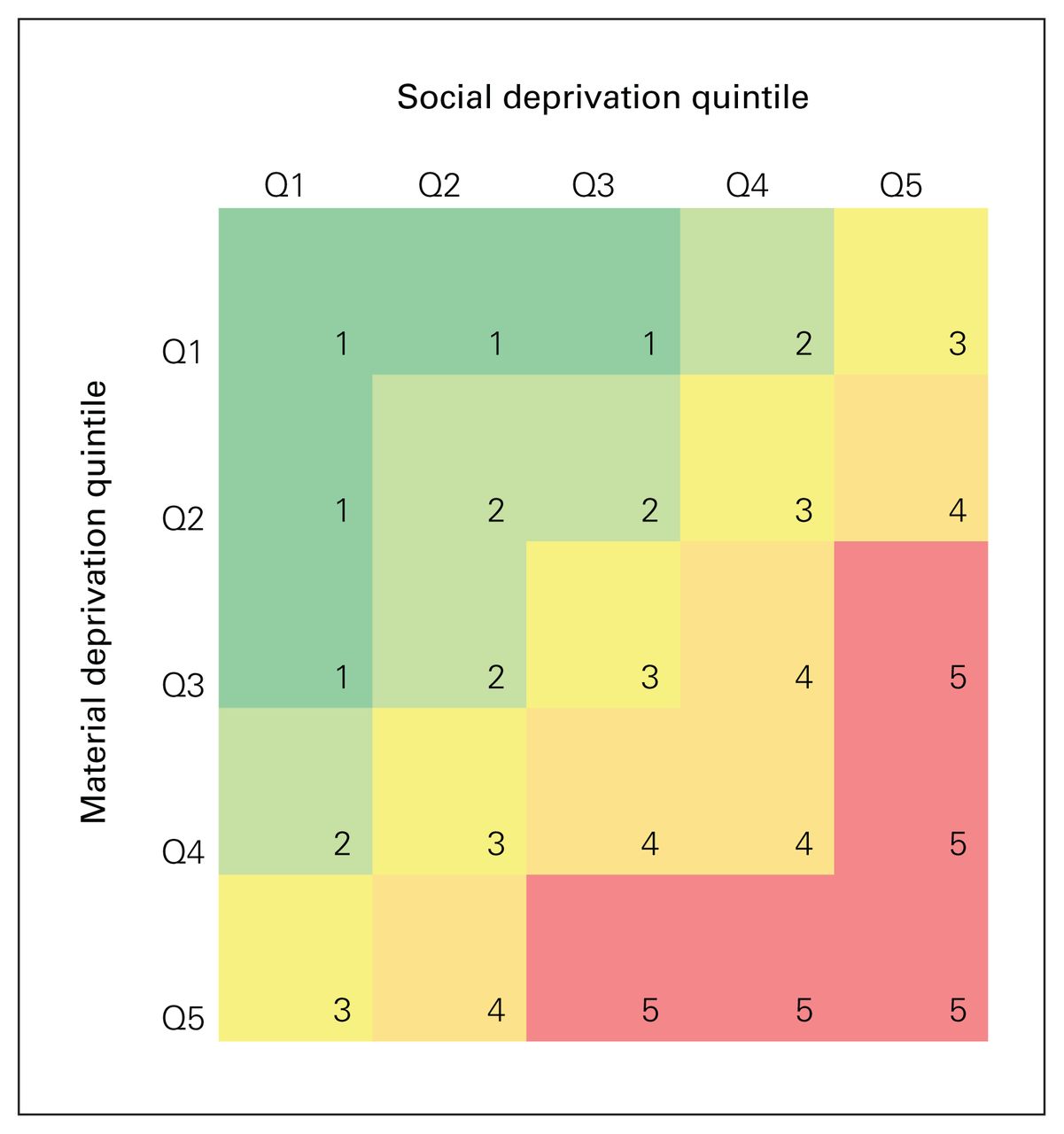
Grouping of material and social deprivation quintiles (Q).20
Variables
Patient characteristics
Defined patient demographic characteristics included age, sex, distance to hospital (derived with the use of postal codes), socioeconomic deprivation, and comorbid conditions of obesity, diabetes22 and hypertension.22–24 We defined comorbid conditions using the presence of relevant ICD-10-CA codes recorded during the index hospital admission or in any DAD or NACRS record within 2 years before surgery.
Surgical management
The variables pertaining to the surgical management included urgent versus elective surgery, laparoscopic versus open surgery, perforated appendicitis, pre- and postsurgery transfers, time to surgery, intensive care unit (ICU) admission, length of stay and complex postoperative course. Perforated appendicitis was described with the ICD-10-CA code for acute appendicitis with generalized peritonitis (K35.2). From the presence of generalized peritonitis, we inferred perforated appendicitis, and the absence of this code denoted nonperforated appendicitis. Presurgery and postsurgery transfers indicated whether the patient was transferred from another institution before surgery or transferred elsewhere after surgery, respectively. Time to surgery signified the amount of time between hospital admission and appendectomy.
Outcomes
The primary outcome of this study was complex postoperative course after appendectomy. We determined the list of included adverse outcomes a priori based on the experience of 2 general surgeons (K.F. and D.C.W.). We defined a complex postoperative course as a deviation from the ideal postoperative outcome, which included at least 1 of the following conditions within 30 days after appendectomy: wound dehiscence, surgical site infection (SSI),25 abscess, bowel obstruction, pneumonia,26 deep vein thrombosis,27 sepsis,28 ED visit, readmission or death.
The secondary outcome of interest was length of stay. We measured this from the index hospital admission until the final discharge, and included any subsequent hospital admission within 24 hours after the index hospital admission (i.e., during the same episode of care).
Statistical analysis
We reported values as mean and standard deviation (SD) for normally distributed continuous data, or median and interquartile range (IQR) for nonnormally distributed continuous data, and compared them between First Nations and non–First Nations patients using the Student t test and Mann–Whitney test, respectively. We presented categorical variables as number and proportion and compared them using the Pearson χ2 test.
We included patient characteristics in univariable and multivariable regression models to identify any variables associated with complex postoperative course and length of stay. For complex postoperative course, we completed a logistic regression and calculated odd ratios (ORs). We analyzed length of stay using a Cox proportional hazards model in which the time to event was defined as time from admission to final discharge. Using this model, we performed a regression using length of stay as the dependent variable and identified variables independently associated with length of stay and their respective hazard ratios (HRs); variables with a lower HR were associated with a longer length of stay. We illustrated length of stay by First Nations status using a Kaplan–Meier curve.
We conducted all data management and statistical analyses in Microsoft Excel and SPSS version 24 (IBM Corp). Statistical tests were considered significant at p < 0.05.
Ethics approval
This study was conducted under the approval of the Health Research Ethics Board of the University of Alberta (Pro00087547). The Alberta First Nations Information Governance Centre was consulted during study conception and supported the use of First Nations data for the purposes of this study. The analyses and narrative within this manuscript were reviewed with the centre before submission.
Results
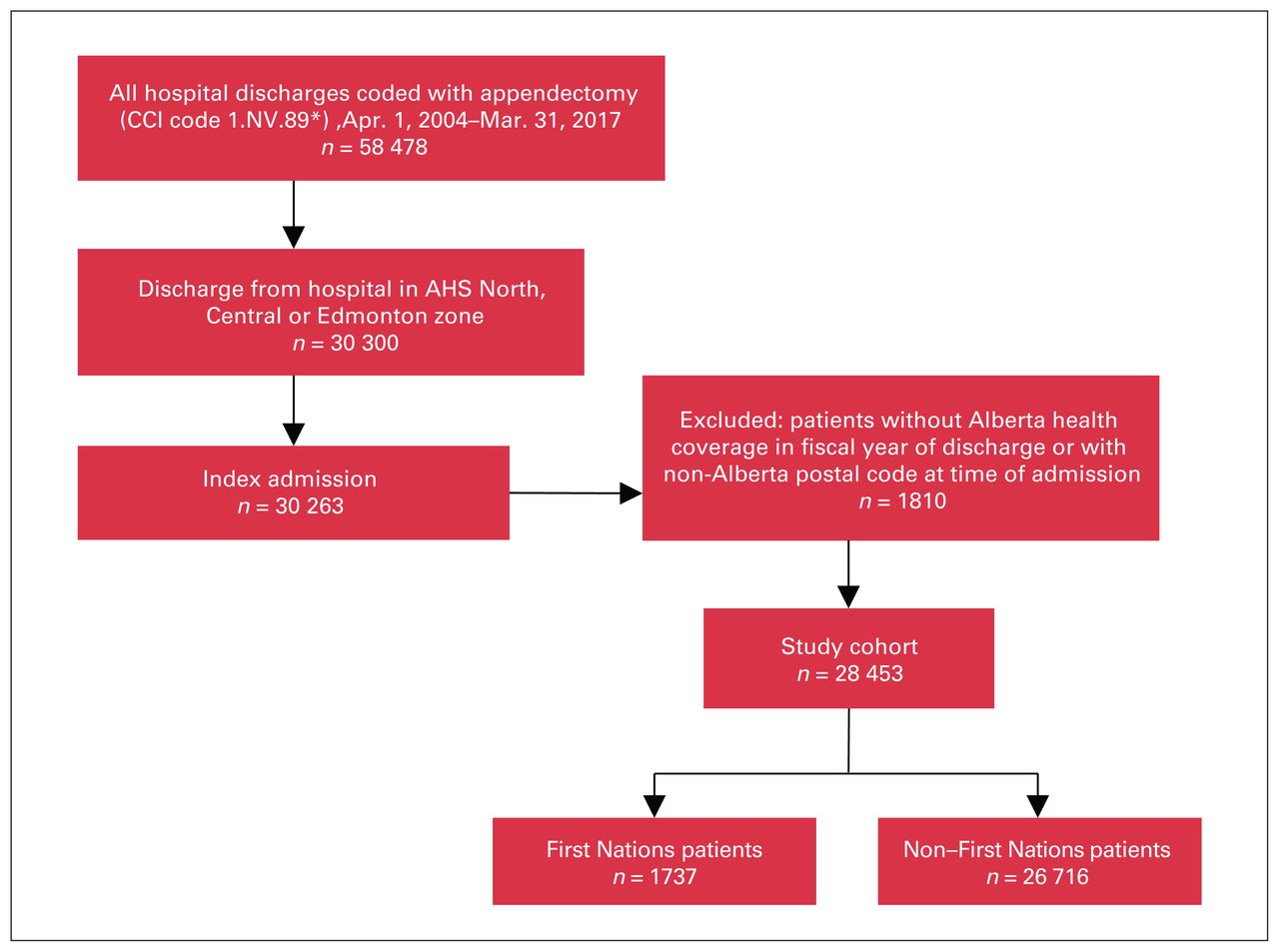
Across the 13-year study period, 28 453 patients met the selection criteria, of whom 1737 (6.1%) had First Nations status (Figure 2). There were 15 008 males (52.7%) and 13 445 females (47.2%) with a mean age of 32.1 (SD 18.1) years (Table 1). The study population lived a median of 15 (IQR 5–51) km from the hospital where they received their surgery. There were greater proportions of patients with higher levels of socioeconomic deprivation: 12.9% in quintile 1 (least deprived), 17.3% in quintile 2, 18.7% in quintile 3, 20.1% in quintile 4 and 25.9% in quintile 5 (most deprived); information on socioeconomic deprivation was missing for 1445 patients (5.1%). The rates of obesity, diabetes and hypertension were 4.5%, 6.5% and 11.9%, respectively.
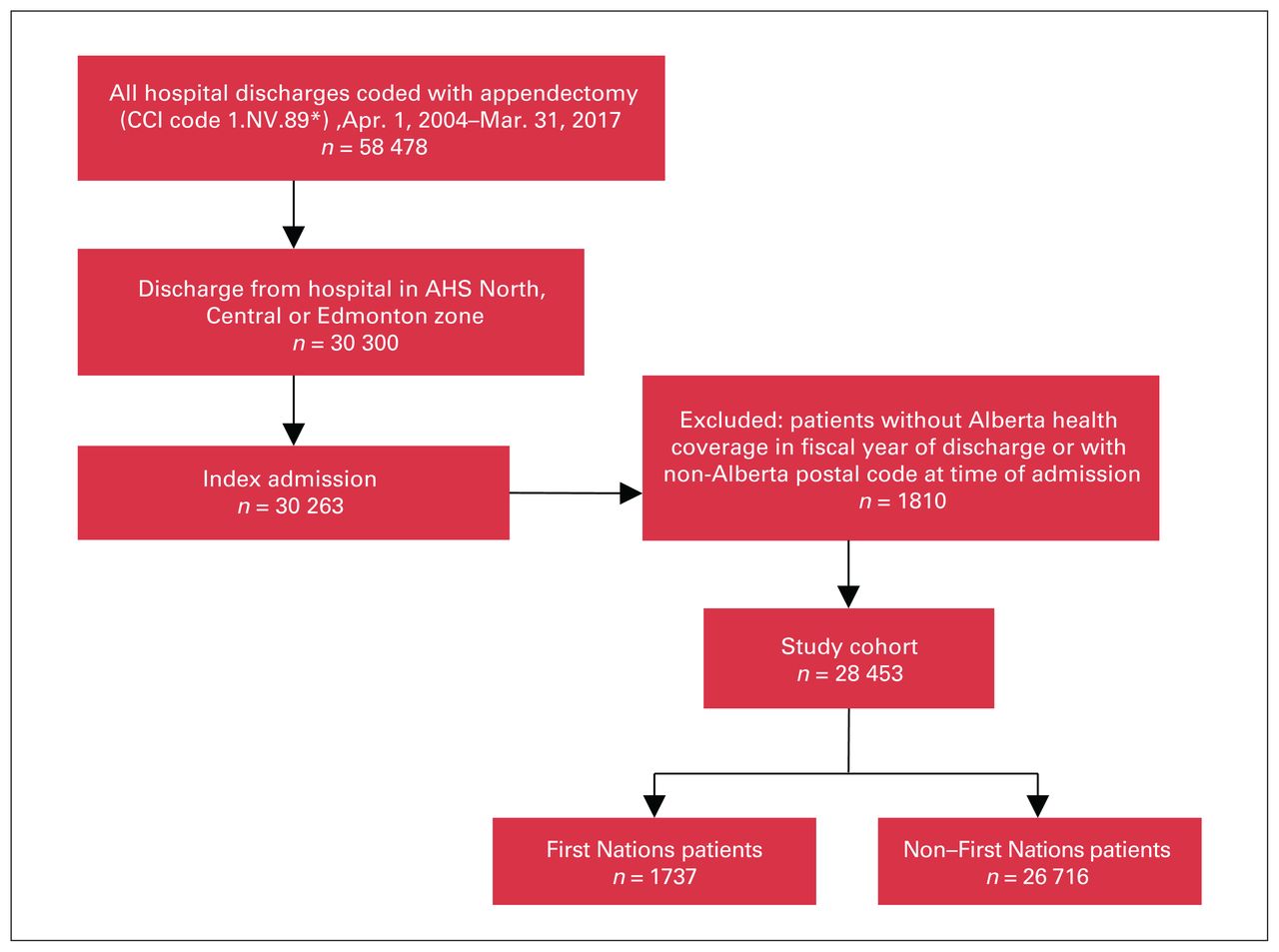
Flow chart showing patient selection. AHS = Alberta Health Services, CCI = Canadian Classification of Health Interventions.
Population characteristics
Patient characteristics by First Nations status
First Nations patients were younger than non–First Nations patients (25.8 [SD 16.2] yr v. 32.5 [SD 18.1] yr, p < 0.001) and lived farther away from the hospital where they underwent appendectomy (60 [IQR 9–184] km v. 14 [IQR 5–43] km, p < 0.001) (Table 1).
There was a significant difference between the 2 groups in socioeconomic status, with a greater proportion of First Nations patients in the more deprived groups (p < 0.001). First Nations patients also had higher rates of obesity (7.2% v. 4.3%, p < 0.001) and diabetes (9.7% v. 6.3%, p < 0.001) than non–First Nations patients.
Surgical management
A higher proportion of First Nations patients than non–First Nations patients were treated with open surgery (45.7% v. 38.7%, p < 0.001) (Table 2). First Nations patients were more likely to have been transferred from another institution before surgery (44.9% v. 24.7%, p < 0.001) and to another location after their surgery (3.4% v. 1.4%, p < 0.001). In addition, First Nations patients presented more often with perforated appendicitis (2.4% v. 1.7%, p = 0.04) and required a longer hospital stay (2 [IQR 1–4] d v. 2 [IQR 1–3] d, p < 0.001).
Characteristics of surgical care
The proportion of elective procedures, median time to surgery from admission and rates of ICU admission were similar for the 2 groups.
First Nations patients were more likely to have had a complex postoperative course (35.1% v. 24.0%, p < 0.001): rates of wound dehiscence, SSI, sepsis, ED visits and readmission were significantly higher for that patient group than for non–First Nations patients. Rates of abscess, bowel obstruction, pneumonia, deep vein thrombosis, severe sepsis and death were similar for the 2 groups.
Complex postoperative course
In logistic regression analysis, after adjustment for other variables, all variables assessed were significantly associated with a complex postoperative course (Table 3). Older age (OR 1.038, 95% CI 1.020–1.057), female sex (OR 1.121, 95% CI 1.060–1.186) and living farther from the hospital (OR 1.014, 95% CI 1.011–1.016) were associated with poor outcomes after appendectomy. The OR for having a complex postoperative course also increased with increasing socioeconomic deprivation (quintile 5 [most deprived] OR 1.437, 95% CI 1.304–1.584). Obesity (OR 1.469, 95% CI 1.293–1.668), diabetes (OR 1.197, 95% CI 1.068–1.342) and hypertension (OR 1.484, 95% CI 1.351–1.631) were all significantly associated with a complex postoperative course.
Complex postoperative course — logistic regression analysis
After adjustment for the influence of other variables, First Nations status remained significantly associated with worse outcomes after appendectomy (OR 1.548, 95% CI 1.384–1.733).
Length of stay
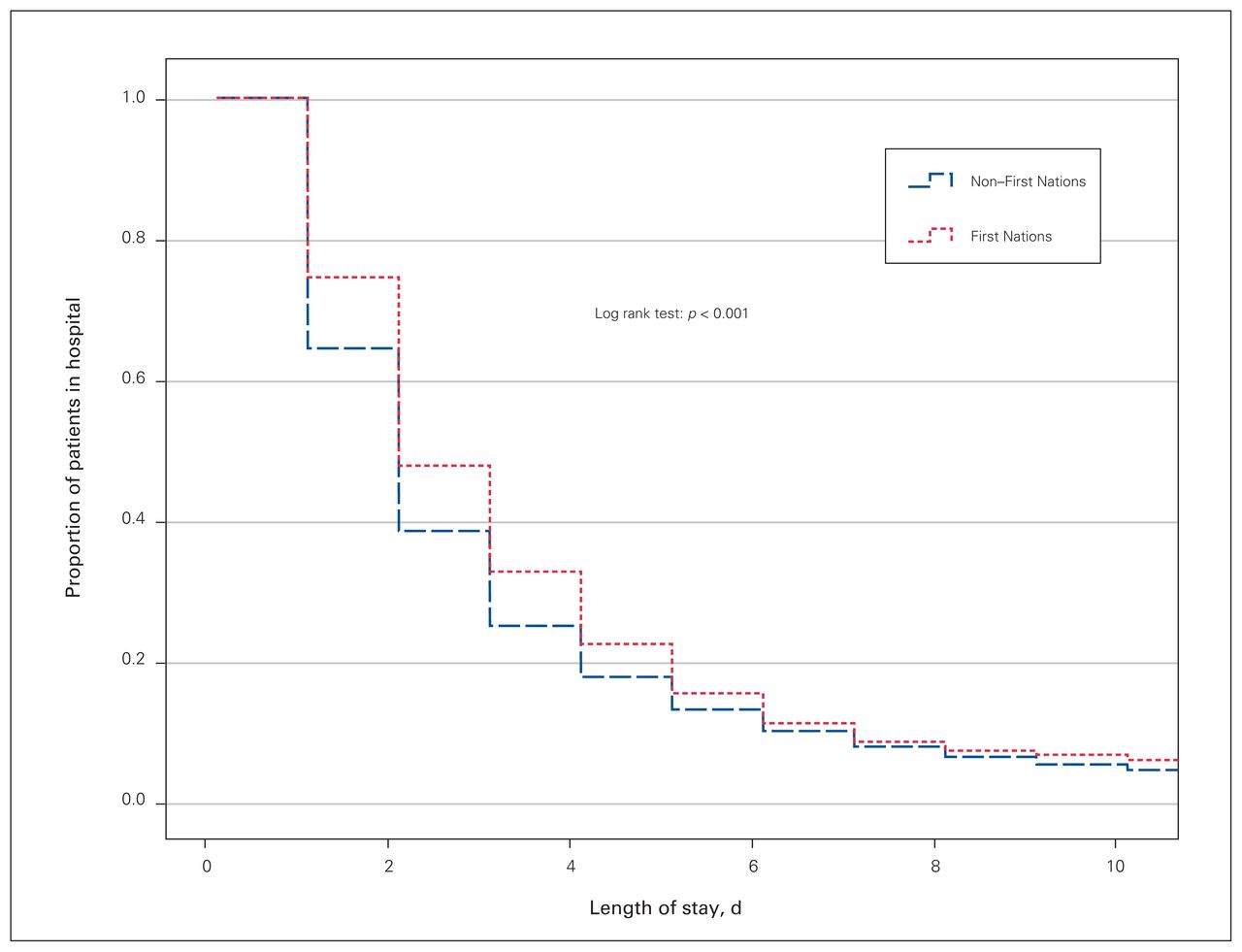
We identified a difference in length of stay between First Nations patients and non–First Nations patients (p < 0.001) (Figure 3). In the multivariable regression model, age (HR 0.962, 95% CI 0.955–0.968), distance to hospital (HR 0.994, 95% CI 0.993–0.995), First Nations status (HR 0.877, 95% CI 0.832–0.924), obesity (HR 0.868, 95% CI 0.817–0.921), diabetes (HR 0.870, 95% CI 0.826–0.917) and hypertension (HR 0.762, 95% CI 0.729–0.795) were associated with a longer length of stay (Table 4). Sex was not a significant factor in this model. The relation between socioeconomic deprivation and length of stay varied inconsistently, and, relative to quintile 1, only quintile 2 was associated with a shorter length of stay (HR 1.046, 95% CI 1.002–1.091).
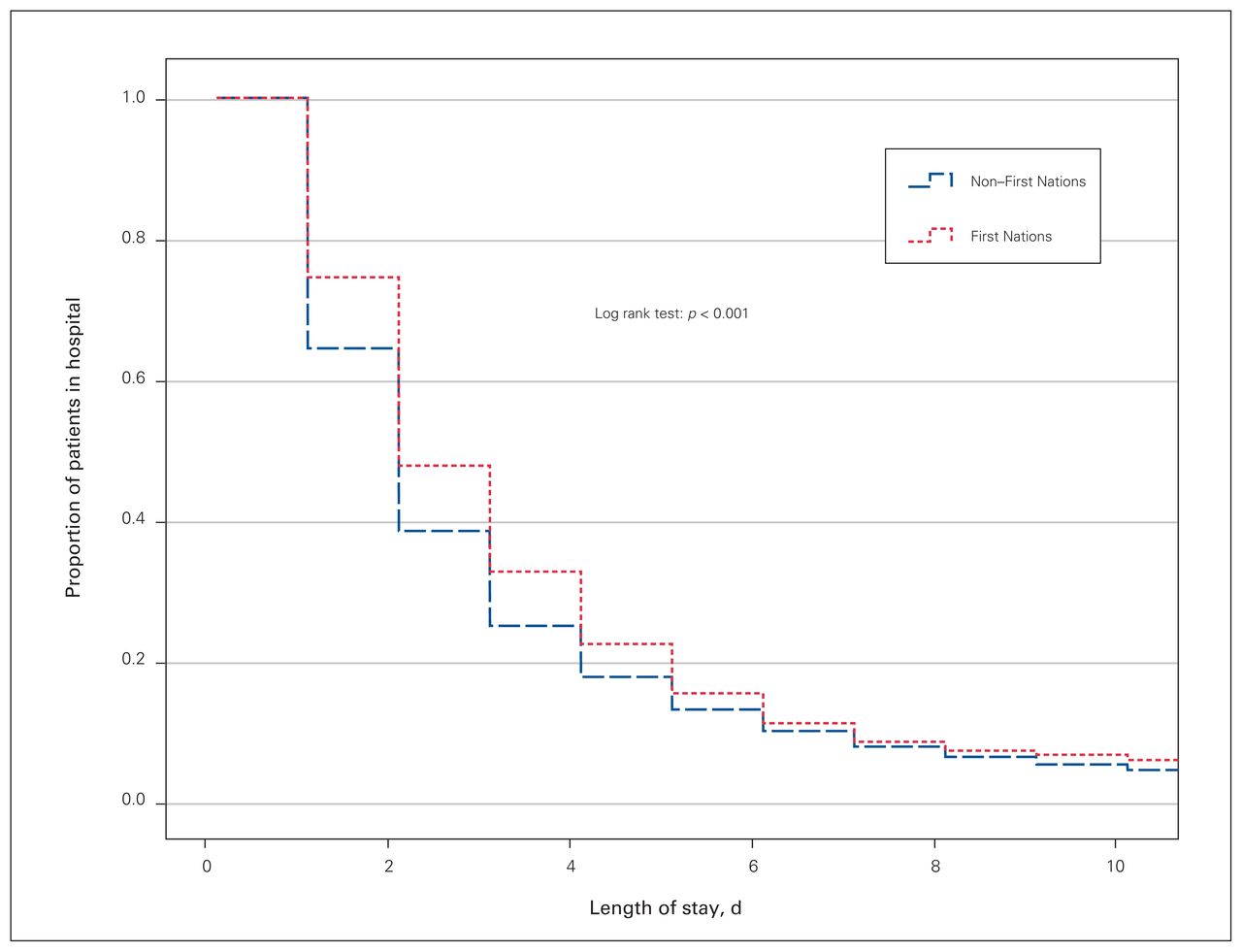
Kaplan–Meier curve of length of stay by First Nations status. Length of stay, d
Length of stay — Cox proportional hazards model*
Discussion
We found that 35.1% of First Nations patients experienced a complex postoperative course, compared to 24.0% of non–First Nations patients, and the former were consistently affected more frequently by individual adverse outcomes, which varied significantly between the 2 groups. Similar differences between First Nations and non–First Nations patients in rates of 30-day mortality, severe sepsis and ICU admission suggest that major complications may not disproportionately affect First Nations patients; however, we did not expect frequent occurrence of severe complications associated with appendectomy. Variables independently associated with a complex postoperative course included First Nations status, distance to hospital, socioeconomic deprivation and comorbidities, and First Nations status was related to all the other variables with the exception of hypertension. This suggests that the higher rates of poor outcomes experienced by First Nations patients may be partially mediated by other factors.
First Nations patients were more likely to be in socioeconomically deprived quintiles than non–First Nations patients. Previous authors have described poor health outcomes associated with lower socioeconomic status as due to complex mechanisms that frequently promote health-damaging behaviours, greater adverse risk factor profiles and a higher degree of pre-existing comorbidity.29–32 In our study, First Nations patients were more likely than non–First Nations patients to have accompanying obesity and diabetes. This finding suggests generally poorer health in this population, which is corroborated by other provincial data,33 and increases the likelihood of needing greater postoperative care. For example, both obesity and diabetes indicate additional surgical requirements and are frequently linked to increased postoperative morbidity and mortality.34,35 First Nations patients also experienced longer hospital stays. Length of stay is commonly used to assess quality of care provided, with a longer stay implicating a more difficult treatment course and poorer outcomes.36 Our findings may indicate that poorer surgical care was provided to First Nations patients, or that the surgery was more difficult and the patient required additional postoperative monitoring.
In addition to poorer initial health, First Nations patients were more likely than non–First Nations patients to live in rural locations and to require greater travel distances to receive treatment for acute appendicitis. In keeping with previous studies,37,38 distance travelled was found to be positively associated with adverse outcomes. First Nations patients were more likely to have transferred facilities during their surgical care, which implies the absence of physicians who could provide basic surgical procedures locally within their communities. Furthermore, a greater proportion of First Nations patients showed perforated appendicitis. Although in-hospital delays have not been found to be associated with the risk of perforated appendicitis,39,40 perforation can occur if appendicitis is not treated promptly enough.41,42 We suspect that the combination of delayed treatment and comorbidities may have exacerbated appendicitis and resulted in the greater frequency of complex postoperative course among First Nations patients in our study. Together, these findings suggest a delay in care and support that surgical care is not as readily accessible for First Nations populations as for non–First Nations populations.
We also found greater ED use within 30 days of appendectomy for First Nations patients. An Australian study showed that Indigenous patients were more likely than non-Indigenous patients to be admitted for emergency rather than elective surgery, and the author suggested a “cultural bias against surgical procedures.”43 It is possible that a delay in seeking surgical care may have resulted in greater disease severity until urgent care was needed. Ongoing mistrust of the health care system as a result of negative personal and intergenerational experiences of discrimination and judgment within health care systems are well-described barriers to access to care.44 Furthermore, First Nations populations lack access to established primary and specialist care, which interferes with necessary postoperative follow-up care and worsens health outcomes after surgery.45,46 Given the greater distance between where they live and the location of their appendectomy, it would be more challenging for First Nations patients to follow up with their surgeons. The lower physician density in remote areas and the greater socioeconomic deprivation in First Nations communities necessitate increased reliance on ED as a primary health service.47 Combined with mistrust of the health care system,48 these systemic barriers may explain the higher ED use by First Nations patients observed in the present study.
To reduce geographic barriers to equitable surgical care, additional surgical training of primary care physicians may increase access and improve surgical outcomes. Introducing Family Physicians with Enhanced Surgical Skills (FPESS) in communities with greater need has been discussed for decades.49 Although FPESS practise throughout Alberta, increasing their prevalence may improve equity in surgical care, and curriculum redesign is underway in academic centres to better offer FPESS training (D.C.W., unpublished observations, 2016; Dr. Mark Prins, Director of Rural and Regional Health, Faculty of Medicine & Dentistry, University of Alberta, 2016). These programs must be supported by academic departments of surgery so that appropriate skills are taught and FPESS may develop collaborative relationships with their training institutions.
Even after adjustment for other variables, First Nations status remained highly associated with the risk of a complex postoperative course. These results describe an intrinsic disadvantage within our health care system for First Nations patients seeking surgical care, and illustrate systemic discrimination against First Nations patients, through overt or unconscious bias, that acts independently of geographic concerns, comorbidities and socioeconomic status. First Nations communities have ontologic nuances specific to their understanding of health and wellness,50 and, without acknowledging Indigenous systems of health and wellness that have prospered for thousands of years before European influence, the lack of reconciliation will continue to erode trust in the Canadian health care system and perpetuate cycles of health inequity.48 The experiences of First Nations patients in accessing surgical services need to be urgently explored for actionable changes toward equity in surgical care, and researchers must incorporate First Nations perspectives in the analysis and interpretation of their data to ensure that scientific conclusions resonate with the lived experiences of First Nations patients.51
Limitations
Our study has limitations that affect the interpretation of our results. Our adverse conditions included ED visits within 30 days of appendectomy, which contributed significantly to our high rates of complex postoperative course. There may be a relation between ED use shortly after appendectomy and a poor outcome of the procedure, but this was not verifiable within our data set. Excluding ED visits would reduce the rates of adverse outcomes for both First Nations and non–First Nations patients, but the difference between groups would remain statistically significant. We interpreted First Nations patients’ increased length of stay as additional evidence of worse outcomes after surgery, although this may have been mediated by difficulties with disposition, given rural status and transportation challenges.
Our First Nations group contained only patients with registered First Nations status. Self-identification may have identified more First Nations patients, but this information was not available within our data set, and the inclusion of non-status First Nations patients as non–First Nations may have minimized the differences between the study groups. We also stress that our findings do not apply to Métis and Inuit Peoples, who account for 44.2% and 1.0%, respectively, of the Indigenous population in Alberta.52 Although Indigenous Peoples share elements of history and world views, First Nations Peoples exist in a distinct legal, cultural and social structure from Métis and Inuit Peoples.53 For example, Ospina and colleagues47 found that rates of ED visits were higher for First Nations and Inuit groups but lower for a Métis group compared to a non-Indigenous cohort. Although our findings may offer insight into the surgical care provided to Inuit and Métis patients, further research must be done to describe these distinct populations.
As with all studies of secondary administrative data, there were challenges in the availability of pertinent variables. With a more robust database, additional data such as smoking status may have better informed initial patient health status, and complications after appendectomy may have been better captured with the inclusion of provision of blood transfusions, enterotomy or repeat operative management. We also need to consider the possibility of poor coding. As a result, the rates of adverse outcomes were likely not representative of the true incidence and prevalence. For example, the overall proportion of SSI was 3.2%, lower than the rate of 6.2% in a previous study that used clinical records.54 The ICD-10-CA also lacks codes for the characterization of complicated appendicitis. Therefore, our identification of perforated appendicitis relied on the coding for general peritonitis and provided only an inference on the proportion of complex cases. However, we identified validation studies when available, and, for our purposes of identifying differences between groups, we assumed that any imprecision in coding was at least consistent between First Nations and non–First Nations patients.
Conclusion
We found longer lengths of stay and higher rates of complex postoperative course after appendectomy among First Nations patients in Alberta, with First Nations status being highly associated with adverse outcomes independent of rurality, comorbidities and socioeconomic status. These findings indicate that the ongoing health disparity for First Nations people extends to surgical care, provide strong evidence that racial discrimination contributes to differences in surgical outcomes and highlight the acute need to promote equitable surgical care for this population. The needs voiced by First Nations communities will be a critical first step in identifying appropriate approaches to do so.
Acknowledgement
The authors acknowledge Dr. Abdullah Saleh from the Office of Global Surgery, University of Alberta, for his advice and expertise during initial study development.
Footnotes
Competing interests: A. Lafontaine is past president of the Canadian Medical Association, for which he receives a stipend. No other competing interests were declared.
Contributors: D. Williams supervised the study. R. Hsiao, D. Williams E. Youngson and A. Lafontaine designed the study. E. Youngson acquired the data, which R. Hsiao and K. Fathimani analyzed. R. Hsiao wrote the article, which all authors reviewed. All authors approved the final version to be published.
- Accepted September 11, 2023.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.