


Abstract
Background: The training of orthopedic residents in adequate pedicle screw placement is very important. We sought to investigate orthopedic residents’ perspectives on the use of computer-assisted surgery (CAS) in a training trial.
Methods: Orthopedic residents were randomly assigned to independently place a screw using the free-hand technique and the CAS technique on 1 of 3 cadavers (Cobb angles 5º, 15º and 67º) at randomly selected thoracolumbar vertebral levels. All residents were blinded to their colleagues’ pedicle screw placements and were asked to complete a short questionnaire at the end of the session to evaluate their experience with CAS. We obtained CT images for each cadaver to assess pedicle screw placement accuracy and classified placement as A) screw completely in pedicle, B) screw < 2 mm outside pedicle, C) screw 2–4 mm outside pedicle, or D) screw > 4 mm outside pedicle.
Results: Twenty-four orthopedic residents participated in this trial study. In total, 65% preferred using the free-hand technique in an educational setting even though most (60%) said that CAS is safer. The main reason for free-hand technique preference was the difficult technical aspects encountered with CAS. In addition, accuracy of pedicle screw placement in this trial showed that 5 screws were classified as A or B (safe zone) and 19 as grade C or D (unsafe zone) using the free-hand technique compared with 15 and 9, respectively, using CAS (p = 0.008).
Conclusion: Orthopedic residents perceived CAS as safe and demonstrated improved accuracy in pedicle screw placement in a single setting. However, the residents preferred the free-hand technique in an educational stetting owing to the difficult technical aspects of CAS.
Pedicle screws were first used in the United States by Harrington and colleagues1,2 to reduce complicated cases of spondylolithesis. Today, pedicle screw fixations are used for the treatment of many ailments affecting the spine, including vertebral fractures, degenerative disc disease, spine tumours, spondylolisthesis and scoliosis. Pedicle screws used in spine constructs improve the overall spine stability while restoring vertebral height and alignment. In order to maximize biomechanical stability and safety,3 screws are placed directly within the pedicle of vertebrae. Owing to the proximity of the spinal canal and feeding vessels, pedicle screw misplacement can potentially harm vascular and neural structures.4,5 Other possible complications associated with screw misplacement include instability and nonunion.6–8
Pedicle screw placement accuracy differs across spinal regions (e.g., thoracic v. lumbar) and may be increasingly challenging in patients with spine deformity. Studies using conventional surgical techniques have reported pedicle screw misplacement varying between 5% and 41% for the lumbar spine and up to 55% in the thoracic spine.9–12 As a result, novel image-guided and navigation surgical techniques have been developed to increase the placement accuracy and the safety of pedicle screw insertion. A recent systematic review reported that the rate of pedicle screw placement fully contained in the pedicle (without perforation) using a free-hand technique ranged between 69% and 94% compared with the help of fluoroscopy (28%–85%), computed tomography (CT) navigation (89%–100%) and fluoroscopy-based navigation (81%–92%).4 Therefore, it appears that navigation techniques may improve pedicle screw accuracy compared with free-hand techniques and fluoroscopy. Orthopedic spine surgeons are typically introduced to different navigation techniques throughout their careers. However, as pedicle screw placement accuracy is critical in spine surgery, it may be relevant to introduce these techniques at the residency level. Therefore, the purpose of this study was to evaluate residents’ perceptions of computer-assisted surgery (CAS) and to assess the effectiveness of CAS as a tool for the training of pedicle screw placement among a group of orthopedic residents in an educational trial.
Methods
Sample
We recruited the residents (postgraduate years [PGY] 1–4) from the McGill University orthopedic surgery program, Montreal, Que., for this research project. The trial study was conducted during a protected teaching day in which all orthopedic residents were expected to be present. The PGY5 residents had an alternative teaching session organized and did not attend the event. Other residents who were on approved leave or who were on post-call days were exempt from the session. We obtained informed consent from all residents who agreed to take part in this study.
Study settings
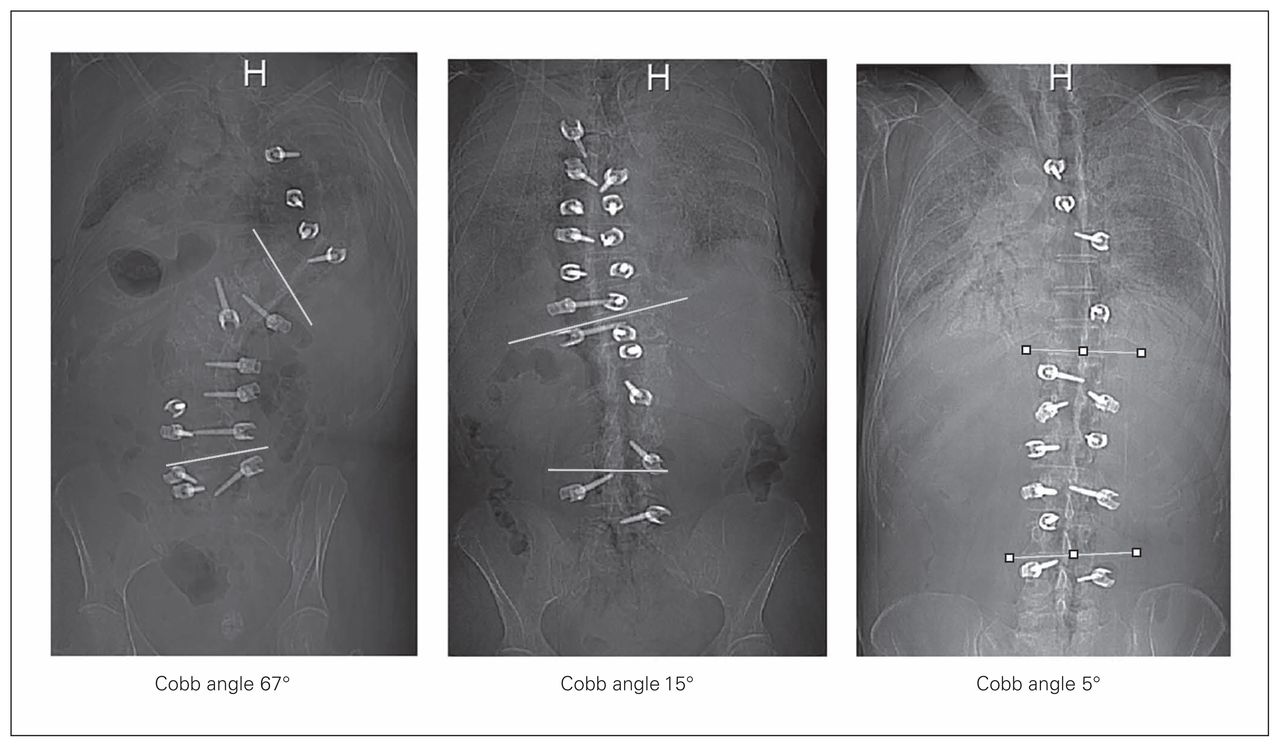
The study was conducted at the Arnold and Blema Steinberg Medical Simulation Centre, McGill University. In order to simulate different levels of difficulty for pedicle screw placement, 3 cadavers with varying degrees of scoliosis (Cobb angles 5°, 15° and 67°) were selected for the purpose of this training session (Fig. 1). Each cadaver was designated to a respective station and dissected by a trained orthopedic spine surgeon (M.W.) to allow for clear identification of anatomic surface landmarks. Each training station, cadaver and vertebral levels were clearly labelled (Fig. 2). Standard pedicle screw placement instrumentation as well as a fully functional Stryker Fluoro Navigation 2D CAS system (Stryker Navigation System, Stryker Leibinger) was provided at each station. All images for CAS were acquired before the start of the study using a GE 9800 C-arm machine. The CAS system accuracy was verified before the start of the educational trial by taking anteroposterior (AP) and lateral radiographs of the spine and verifying the accuracy of the depicted virtual reality tool on the navigation image in relation to the real time position of the tool (spinous processes were used as easy reference points). In addition, the reference tracker was repositioned to ensure that instrumentation at a maximum of 2 levels above or below the reference was used. Radiographs were verified to ensure accuracy for different instrumented levels each time the tracker was repositioned as detailed above.
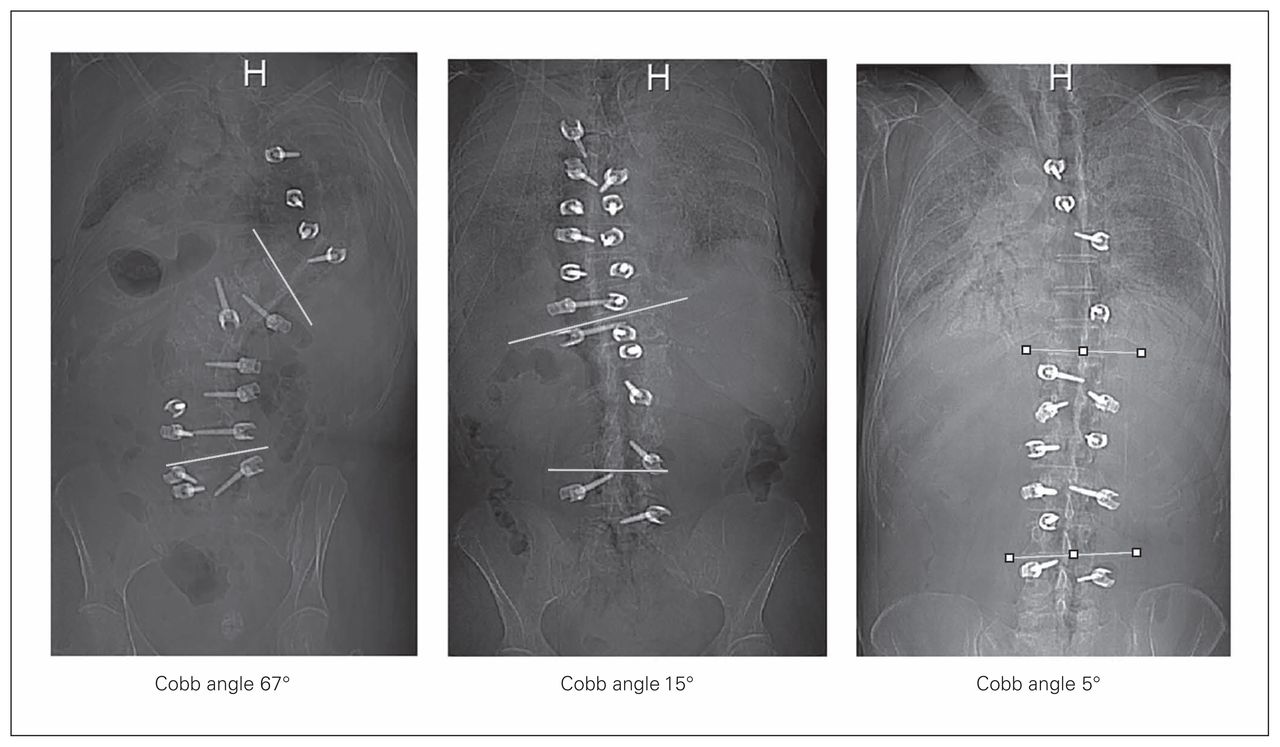
Cobb angle measurements for each cadaver.

Cadaver station setup.
A trained orthopedic spine surgeon (M.W.) familiar with both standard instrumentation and CAS was present at each station to answer questions regarding instrumentation. Prior to the beginning of the training session, all residents received a brief lecture (30 min) on CAS and freehand techniques for the placement of pedicle screws. Each resident was then randomly assigned to place 1 screw using the free-hand technique and 1 screw using the CAS technique on 1 of the cadavers at randomly selected vertebral levels (only thoracolumbar levels were used). The supervisor at each station informed the resident what level to instrument, and all of the residents sequentially placed their 2 screws independently, with no assistance. Only polyaxial screws were used. To minimize visual cues, the head position of the polyaxial screws were altered between residents, thus all residents were blinded to their colleagues’ placement orientation.
At the end of the session all residents completed a short questionnaire regarding their experiences and preferences during the training session, including their preferred technique for educational purposes. The questionnaire also asked which technique they thought was safer and whether they would use navigation in future practice. A later survey was sent to all participants to determine why a technique was their preferred choice, thus giving a global impression of surgical residents’ perceptions of CAS and spine surgery. This survey was sent after pedicle screw results were seen for both free-hand and CAS techniques.
Computed tomography and grading
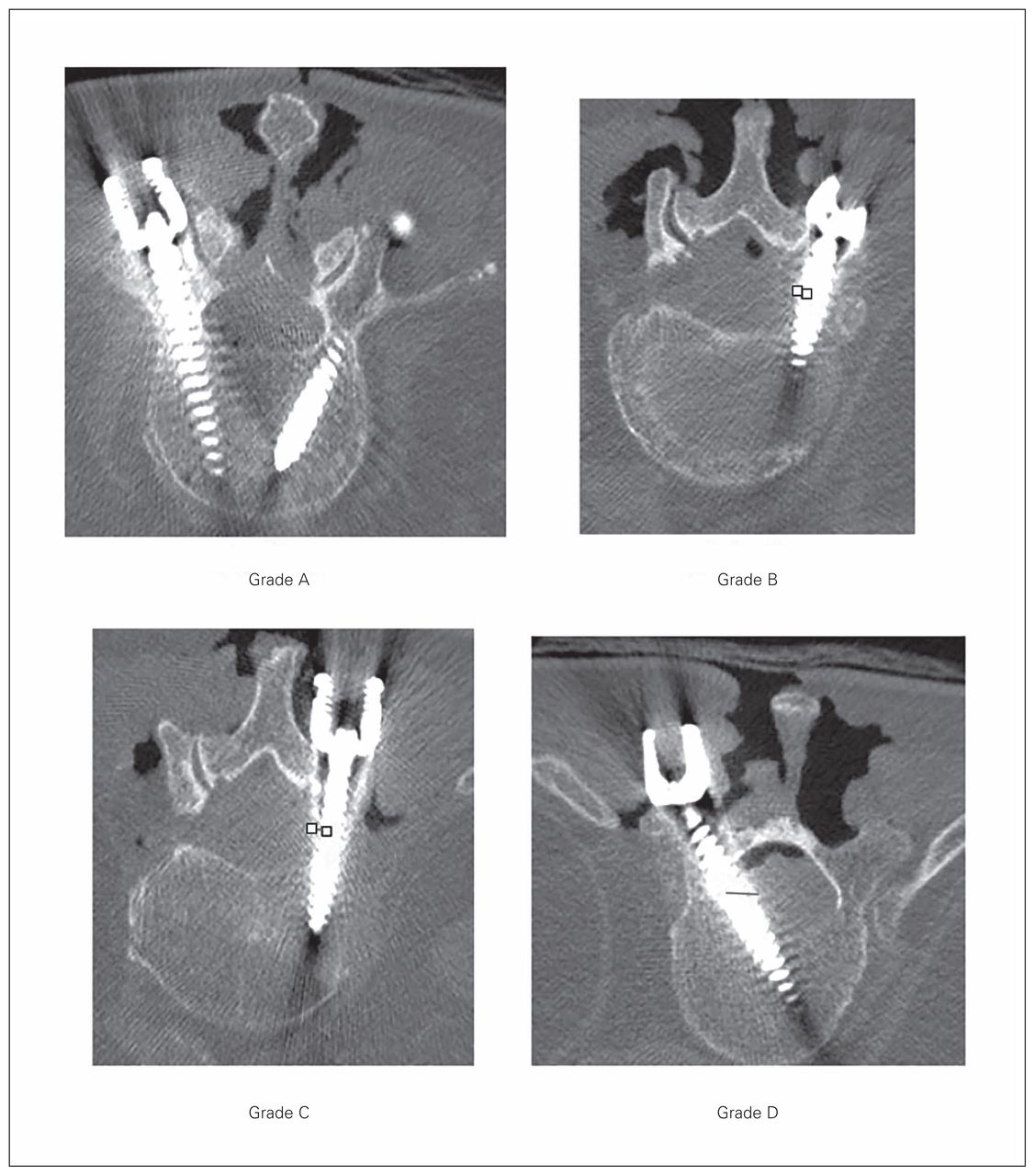
We obtained CT images for each cadaver to assess pedicle screw placement accuracy. Sagittal, coronal and axial cuts were acquired for all instrumented levels using 2.5 mm slices. Based on the CT images, pedicle screw accuracy was classified as follows: A) screw completely in pedicle, B) screw < 2 mm outside of pedicle, C) screw 2–4 mm outside of pedicle, or D) screw > 4 mm outside of pedicle. All screws were scored by the same rater, who verified all 3 planes (sagittal, coronal, axial) to determine the grade. A grade D score was also given to any screw that was dislodged before imaging, as poor placement was assumed to have resulted in screw instability. In accordance with the literature,13–15 grade A and B screws were deemed to be within the “safe zone,” whereas grade C and D screws were deemed to be in the “unsafe zone.”
Statistical analysis
We used Fisher exact tests to assess the difference in screw placement accuracy between the free-hand technique and CAS method and to evaluate the difference according to the level of residency, the cadaver’s Cobb angles (5º, 15º and 67º) and the instrumented spine region (thoracic v. lumbar). We considered results to be significant at p < 0.05. Descriptive statistics where used to present the survey questionnaire results among residents.
Results
A total of 24 residents participated in the study: 3 PGY1, 7 PGY2, 8 PGY3 and 6 PGY4. No residents declined to be a part of the study, thus the rate of participation was 100%.
A total of 48 pedicle screws were inserted by the residents: 24 using the free-hand technique and 24 using CAS. Seventeen of the 24 residents (70%) completed the assessment survey (Table 1). Of these residents, 65% reported that CAS improved their pedicle screw placement accuracy, 60% found CAS to be a helpful educational tool, and 60% believed that CAS was a safer technique than free-hand placement. However, 65% of the residents indicated that they still preferred using the free-hand technique in an educational surgical simulation setting. A second survey was then sent to determine why residents preferred a technique over another after viewing the screw placement results. All residents who preferred CAS as an educational tool responded that visual queue during the trial session helped them to better understand the pedicle screw insertion technique. The residents who preferred the free-hand technique in an educational setting responded with varying reasons: 1 resident (9%) stated that the cost of CAS does not justify its use in an educational setting, another resident (9%) stated that limited experience with CAS does not justify its use, and all the remaining residents (82%) said that the technical aspects of CAS hinder its use in an educational setting.
Results of pedicle screw placement accuracy by resident level and technique*
Although not the primary objective of this pilot study the accuracy of placed screws were verified using CT scans after the training session. Five screws were placed in the safe zone (Grade A or B) and 19 screws were placed in the unsafe zone (Grade C or D; 4 of the screws were dislodged and classified as a grade D) using the free-hand technique, whereas 15 screws were placed in the safe zone and 9 in the unsafe zone using CAS (Table 2 and Fig. 3).
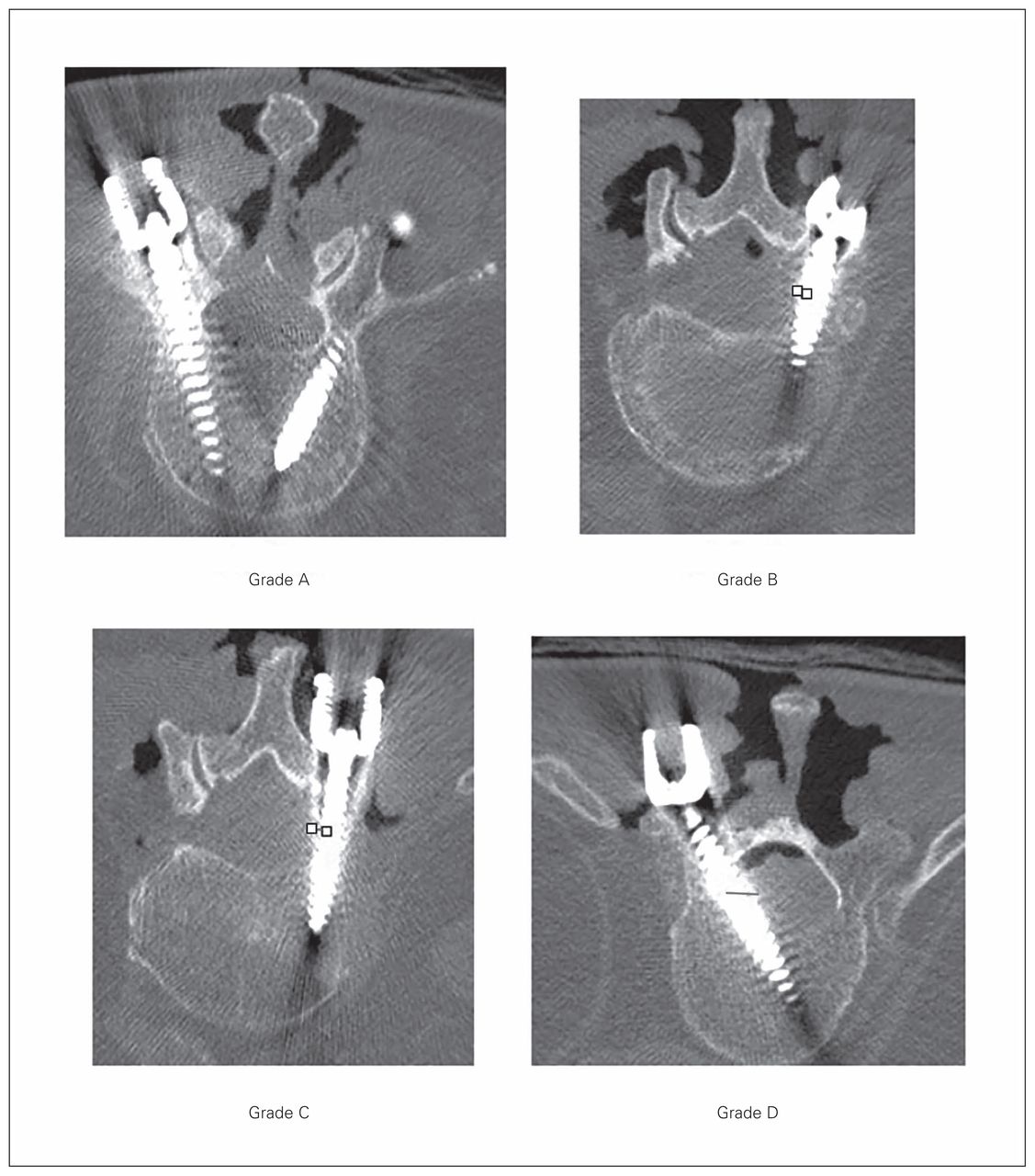
Computed tomography scan example of screw placement accuracy for each grade.
Screw placement accuracy based on residency level and technique*
The level of residency was not associated with screw placement accuracy (Table 3). Although no difference in screw placement accuracy was observed in cadavers with mild to moderate spine deformity (Cobb angles of 5º and 15º), a greater number of screws were placed in the unsafe zone using the free-hand technique than CAS (p = 0.030, Table 4) when severe spine deformity was present (Cobb angle of 67º). However, it is worth noting that the majority of the deformity in the cadaver with greatest Cobb angle was in the thoracic region, and no statistical difference between the free-hand and CAS techniques was noted for thoracic screws (Table 5). We observed a difference in screw placement accuracy with regards to the spine region instrumented. In the lumbar spine, only 1 screw was placed in the safe zone and 6 screws were placed in the unsafe zone using the free-hand technique, whereas 9 screws were placed in the safe zone and 1 screw in the unsafe zone using CAS (p = 0.004; Table 5).
Screw placement accuracy based on spine deformity and technique*
Screws placement accuracy based on spine region (thoracic v. lumbar) and technique*
Self-reported survey results
Discussion
This study aimed to investigate the perception of CAS as an educational tool for the training of orthopedic surgery residents and to verify its effect on pedicle screw placement accuracy among residents in a single educational trial.
The usefulness of CAS as a training tool was confirmed by the residents’ feedback, as the majority reported that CAS allowed for safer screw placement and was a useful tool to learn the standard free-hand technique. However, when residents were asked about their preferred technique in an educational setting, the majority (65%) responded that they preferred the free-hand technique. Among those who preferred the free-hand technique, the majority (82%) stated that the technical complexity of CAS was the main reason for their preference. The residents identified the added visual queue during pedicle screw insertion as an advantage of CAS, but the complex technical aspects seemed to have a negative effect on residents’ perception of this technique.
Interestingly, our findings suggest that CAS helped residents achieve a better screw placement accuracy than the standard free-hand technique, regardless of their level of training or experience. We found that CAS seemed to provide additional guidance for more complex cases, as we observed better screw placement accuracy in the cadaver with severe scoliosis (Cobb angle 67°). Overall, a greater number of screws were placed in the safe zone when residents used the CAS technique. However, this finding was significant only for lumbar screws, and it is important to stress that the study was limited to only 1 trial.
The use of technology, such as robotics, simulations and CAS, for the training of residents is not new.16,17 In fact Haluck and colleagues16 have shown that the use of virtual reality or CAS for the training of residents can have many advantages. Computer simulation is very well documented and has been used successfully in the military and in the aviation field. Its use and interest as an educational tool in the medical field is rapidly growing;16–20 some universities even have dedicated departments for the virtual training of future medical practitioners. Accordingly, the number of orthopedic surgeons using navigation techniques is also increasing. Although CAS has been found to improve surgery outcomes in patients undergoing total knee21–23 or hip24 replacements and to facilitate pedicle screw placement,4,6–8 we are not aware of any study that evaluated the perception and effectiveness of CAS for the training of future orthopedic surgeons.
We believe that learning how to place a safer screw early in training will allow residents to acquire the right technical abilities in a faster time frame. That is, learning the free-hand technique with anatomic landmark is reinforced during training only if real-time feedback of the screw trajectory can be verified by the resident. Instead of just basing their trajectory on anatomic landmarks, CAS allowed residents to see the screw trajectory in real time on the screen and make appropriate adjustments in order to achieve proper screw placement. This real-time feedback may explain why pedicle screw placement accuracy was improved when the residents used CAS as opposed to the free-hand technique in this trial study. Nevertheless, the CAS technique in itself needs to be mastered and taught. Our trial involved an open exposure of the thoracolumbar spine, allowing residents to get both imaging and anatomic feedback during pedicle screw insertion. This can partly explain the improved accuracy of CAS. However, the technical challenges of using CAS were highlighted in the residents’ responses to the survey and should be weighed against its proposed benefit.
It is worth noting that the navigation system used in this study was a 2D fluoroscopy-based system, which may no longer be the norm in spine navigation. Other systems exist and include robotics and 3D navigation systems based on CT scans and even MRI. Moreover, some systems use advanced technology and allow for 3D image guidance. Although the literature has shown that CAS helps improve pedicle screw placement accuracy,25 different navigation systems27 may perform better than others with regards to pedicle screw placement accuracy.26,27 For instance, CAS systems based on CT scan seem to produce better results than 2D fluoroscopy-based systems. Our results suggest that a CAS system based on 2D fluoroscopy was well perceived by residents as a safe technique, but was limited owing to technical challenges. The results also demonstrated improved pedicle screw accuracy for residents using CAS in a single setting.
Limitations
Other navigation systems can prove to be just as beneficial as the 2D fluoroscopy-based system that we used and may increase accuracy even further. In addition, a major limitation of our study was that each resident placed only 2 screws owing to limited access to cadavers. Although the overall performance of residents was noted, this was only a single education simulation, and further studies with larger samples are required to confirm our findings in a more statistically significant manner (i.e., improve β and α error, which were lacking in our study). The technical challenges of CAS may also have been exaggerated since the residents at our institution are not exposed to CAS in a clinical setting; that is, most residents were using CAS for the first time in this trial study.
To the best of our knowledge, this is the first study to investigate residents’ perceptions of CAS and verify the accuracy of the standard free-hand technique compared with CAS for pedicle screw placement in a single trial among orthopedic surgery residents. Our results showed that residents perceived CAS as safe, but also difficult because of the technical challenges associated with its use. In addition, the accuracy of resident pedicle screw placement seemed to improve with CAS. However, our study was limited by a small sample size; although a group of 24 orthopedic residents from a single program is relatively large, we were limited by the number of cadavers available. Consequently, we had to limit the number of screws placed by each resident to only 2. This limitation affects the precision of our results and the statistical power in this preliminary study. Larger studies are warranted to determine whether the results obtained in our trial are reproducible. Studies examining the free-hand technique before and after CAS training can also give a better idea of the effect of CAS in an educational setting.
Conclusion
This pilot study investigated orthopedic surgery residents’ perceptions of CAS and showed that CAS was perceived as safe, but technically challenging. Therefore, CAS may need to be more user friendly and less technically challenging in order to improve residents’ perceptions of its use. In future work, a prospective study using the same cohort of residents would be helpful to assess the validity over time and to better evaluate the use of CAS in the training of orthopedic surgery residents.
Footnotes
Competing interests: None declared.
Contributors: A. Aoude, P. Jarzem, J. Ouellet and M. Weber designed the study. A. Aoude, H. Alhamzah and M. Fortin acquired and analyzed the data, which P. Jarzem, J. Ouellet and M. Weber also analyzed. All authors wrote and reviewed the article and approved the final version for publication.
- Accepted June 20, 2016.
References

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.