


Abstract
Background: An increasing need for laser lead extraction has grown in parallel with the increase of implantation of pacing and defibrillating devices. We reviewed the initial experience of a regional laser-assisted lead extraction program serving Atlantic Canada.
Methods: We retrospectively reviewed the cases of all consecutive patients who underwent laser lead extraction at the Maritime Heart Centre in Halifax, NS, between 2006 and 2015. We conducted univariate and Kaplan–Meier survivorship analyses.
Results: During the 9-year study period, 108 consecutive patients underwent laser lead extractions (218 leads extracted). The most common indication for extraction was infection (84.3%). Most patients were older than 60 years (73.1%) and had leads chronically implanted; the explanted leads were an average of 7.5 ± 6.8 years old. Procedural and clinical success (resolution of preoperative symptoms) rates and mortality were 96.8%, 97.2%, and 0.9%, respectively. Sternotomy procedures were performed in 3 instances: once for vascular repair due to perforation and twice to ensure that all infected lead material was removed. No minor complications required surgical intervention. Survival after discharge was 98.4% at 30 days and 94% at 12 months.
Conclusion: Atlantic Canada’s sole surgical extraction centre achieved high extraction success with a low complication rate. Lead extraction in an operative setting provides for immediate surgical intervention and is essential for the survival of patients with complicated cases. Surgeons must weigh the risks versus benefits in patients older than 60 years who have chronically implanted leads (> 1 yr) and infection.
The rate of internal cardiac pacemaker implantation has accelerated in recent years with more than 200 000 patients living with pacemakers in Canada (2012).1,2 The complexity of the implanted hardware has also increased; single-chamber pacemakers are being replaced by multichamber, rate-responsive pacemakers, which are capable of both pacing and cardioversion as well as cardiac resynchronization therapy.3 Similarly, the number of implantable cardioverter defibrillator (ICD) implantations has increased in parallel with pacemaker implantations in recent years (increase of 160% for ICDs v. 31% for pacemakers, 1993–2009) as a result of increased understanding of cardiac arrhythmia in the population.4
The increasing number of implantations has also resulted in a huge growth in the number of indications for explanting pacemaker and ICD devices.5,1 The most common indication for device and/or lead extraction remains device-related infection (≥60%),4 with the most commonly associated pathogen belonging to the Staphylococcus genus of bacteria.5,6 Other common indications for extraction are lead or device malfunction, device upgrade, pain and/or discomfort associated with the cardiac implanted electronic device (CIED) as well as congestion (i.e., a large number of electrodes in the heart and surrounding vasculature, which hamper both the insertion and removal of leads).
Lead and device extraction has been associated with potentially serious major and minor complications. Major complications include death and cardiac or vascular perforation resulting in a sternotomy.7,8 Minor complications include, but are not limited to, pericardial effusion, hemothorax, hematoma, thrombosis, lead migration, pneumothorax and pulmonary embolism, with some requiring surgical intervention.7,8
Given the above risks, CIED lead extraction procedures are routinely conducted in specialized cardiac centres, specifically in either an operating room (OR) by an experienced surgeon or in an electrophysiology (EP) laboratory with a team of cardiologists along with support staff as well as a cardiac surgical unit in case of serious complications.9 Traditional traction-only extractions are effective for cases of acutely implanted leads (< 1 yr); however, such extractions have exhibited limited effectiveness for chronically implanted leads (> 1 yr).10 Laser-power sheaths with a locking style are increasingly implemented to facilitate highly effective procedures with low complication rates (complete success: 94% with laser-assisted extraction v. 64% with simple traction).5,11
The present study examined the initial experience of all consecutive patients undergoing lead extraction using a laser-powered system within a regional program serving Atlantic Canada. We provide a comprehensive analysis of the outcomes and benefits associated with performing the laser lead extraction procedure at the sole referral centre serving Canada’s 4 Atlantic provinces, New Brunswick, Nova Scotia, Prince Edward Island, and Newfoundland and Labrador.
Methods
Patient population
The patient population analyzed consisted of all consecutive patients who underwent pacemaker or ICD laser lead extraction procedures at the Halifax Infirmary between Sept. 1, 2006, and May 31, 2015. This included only extraction in which a laser-powered system was needed. As such, all extraction procedures using manual only traction and those that did not use any powered extraction sheath(s) were excluded from the study. All patients were identified using a mandatory record of use of the laser system. The study was approved by the institution research ethics review board and followed all usual standard guidelines.
Lead extraction procedure
All extraction procedures at the Halifax Infirmary were conducted in a cardiac surgery operating room with the primary operator being a cardiac surgeon specializing in arrhythmia and CIED surgery. All interventions were conducted using general anesthesia with central venous access, continuous transesophageal echocardiography and continuous blood pressure monitoring.
All surgeons gained expertise in this operation by visiting 2 high-volume centres, the Montreal Heart Institute and the Cleveland Clinic, as both perform this procedure frequently. The Spectronetics Company provided clinical support during the initial cases to allow experience to be gained. The electrophysiologists do not have an active role in the extraction program, but provide invaluable expertise in device system management and work collaboratively with many of these patients.
Lead extractions at the Halifax Infirmary were conducted using a stepwise approach, where extraction via simple traction was initially attempted. If simple traction was not sufficient, a locking stylet (LLD Spectronetics) was then used for assistance. This was followed by the use of an appropriately sized laser manual dissection sheath (Spectronetics) under fluoroscopic guidance. All extraction procedures aimed for the complete removal of all targeted leads. If a fragment of lead remained mobile, an additional approach, such as a snare catheter, was used.
In patients who were pacemaker-dependent, a temporary pacemaker was positioned from the right internal jugular vein, or a single lead active fixation permanent pacemaker was placed on the opposite side; the choice was left to surgeon preference.
Definitions
Clinical and procedural criteria were defined according to the LExICon lead extraction study.12 Procedural success was divided into 2 subcategories: complete and partial. Complete success was defined as the total removal of all lead material from a patient’s vascular space. Partial success was defined as the removal of all lead material except for a small portion of the lead; retained lead material could incorporate the lead tip (electrode) and 4 cm or less of lead coil and/or insulation. Procedural failure was defined as the retention of more than 4 cm of lead material that could not be removed safely. Clinical success was defined as the resolution of all preoperative indications and symptoms associated with lead removal and the absence of major complications and/or lack of pacing control. Clinical failure was defined as the inability to resolve preoperative lead extraction indications and/or the development of major complications; specifically, the occurrence of in-hospital death and the necessity for a sternotomy were considered the criteria for clinical failure.
Complications were defined using the laser lead extraction guidelines of the Canadian Heart Rhythm Society Device Advisory Committee.13 A complication was classified as major if the outcome or potential outcome was directly life-threating, including death, surgical intervention (i.e., sternotomy) and/or an acute or chronic disability. Any suboptimal event that was not immediately or directly life-threating was deemed to be a minor complication, including the development of cardiac arrhythmia, arm swelling, pericardial effusion or pulmonary embolism not requiring surgical intervention.
Data collection and characteristics
We retrospectively collected lead extraction data from the Central District Health Authority’s patient medical database (Horizon Patient Folder). The specific data collected pertained to the patients’ demographic characteristics, clinical presentation and characteristics, extraction processes and procedural complications.
Statistical analysis
We performed a univariate analysis of pertinent patient variables. Additionally, a Kaplan–Meier survivorship analysis was conducted using Prism software version 6 (GraphPad Sofware Inc.).
Results
Patient population
In a study population of 108 consecutive patients, a total of 218 leads were extracted in 111 consecutive primary procedures using a laser sheath and locking stylet between Sept. 1, 2006, and May 31, 2015. All 111 procedures were performed in an operating room setting with transesophageal echocardiography guidance and fluoroscopy. The mean age of patients was 67.2 ± 12.8 years, with the majority of patients (40.7%) between 70 and 79 years of age. The explanted leads were on average 7.5 ± 6.8 years old, and the average number of leads explanted per patient was 2.1 ± 1.0. The majority of patients were from Nova Scotia (47.2%), followed by New Brunswick (39.8%), Newfoundland and Labrador (8.3%), Prince Edward Island (4.7%), and from outside of Atlantic Canada (0.9%). Patient demographic characteristics are summarized in Table 1. A significant number of patients were pacemaker-dependent (54.9%) and had atrial fibrillation (46.1%), previous myocardial infarction (MI; 25.5%) and diabetes (42.5%). The most common indication for extraction was infection (84.3%) and included patients with endocarditis (9.2%), pocket infection (3.7%) or erosion (56.5%). Additional indications included nonfunctional devices or leads (4.6%), elective or required upgrade (13.0%), and pain or associated device irritation (0.9%).
Demographic and clinical characteristics of study patients
Procedural success
The overall procedural success with respect to extracted leads was 96.8%, with a total of 203 (93.1%) targeted leads completely extracted and 8 (3.7%) leads partially extracted; 7 leads (3.2%) failed to be extracted. Procedural success was 93.5%, with a total removal rate of 89.8% (97 patients) and a partial removal rate of 3.7% (4 patients); the procedure failure rate was 6.5% (7 failures; Table 2). Clinically, 105 (97.2%) procedures resulted in favourable outcomes, with complete resolution of preoperative indications in which the extraction indication was predominantly infection (i.e., all infected device material was extracted without complication; Table 2). In the present study, 3 (2.8%) patients had unfavourable procedure outcomes, which we defined as the need or decision to perform a sternotomy to complete the extraction or to deal with a life-threatening procedural complication (Table 2). One patient required sternotomy due to vascular perforation of the innominate vein (or brachiocephalic vein) and hemodynamic instability. In contrast, an elective sternotomy was performed in 2 patients electively owing to inability to remove all infected lead material. A single patient died in hospital several days postoperatively due to arrhythmia-related complications. Therefore, in-hospital mortality was less than 1%.
Procedural and clinical outcomes
The most common minor complications were pleural effusion (21.3%), pneumothorax (4.6%) and pocket hematoma (2.8%), none of which required interventions, such as drainage or tube placement. Ventricular arrhythmias occurred postoperatively in 7 patients, with 2 (1.9%) instances of ventricular fibrillation; a single patient died in hospital 9 days postoperatively following a ventricular tachycardia (VT) arrest. There were 3 (2.8%) instances of lead fragment migration that did not require further intervention. Median length of hospital stay for all consecutive patients was 5 (range 2–7.25) days. Major and minor complications are summarized in Table 3. Of the 3 cases of major complications in which further surgical intervention was required, 2 patients initially presented with device-related infections, whereas the third patient required a device upgrade owing to a nonfunctioning lead. The single patient who died in hospital presented with device-associated infection and underwent laser lead extraction, but uncontrollable VT developed and the patient died 9 days postoperatively. One should note that all major adverse events, including lead extraction failures, occurred in the earlier part of the study (2007–2011), with no cases of major adverse events occurring from 2012 onward. Specific characteristics of procedural failure cases are detailed in Table 4 to provide some insight into the characteristics that may predict failures.
Complications associated with extraction of cardiac implantable electronic device and leads
Procedural and treatment details pertaining to major adverse events and procedural failures
Device and lead characteristics
Of the 105 devices explanted from 108 patients that had available designations, the vast majority were pacemaker devices (70.5%), followed by ICDs (23.0%) and biventricular devices (6.7%). Of the 218 leads extracted, 214 (97.2%) leads had available information pertaining to the duration of implantation: 65 (30.4%) leads were 5–10 years old and 46 (21.5%) leads were older than 10 years (Table 5). The leads were on average 7.5 ± 6.8 years old (median 6 [interquartile range 2–10] years old).
Explanted device (n = 105) and lead characteristics
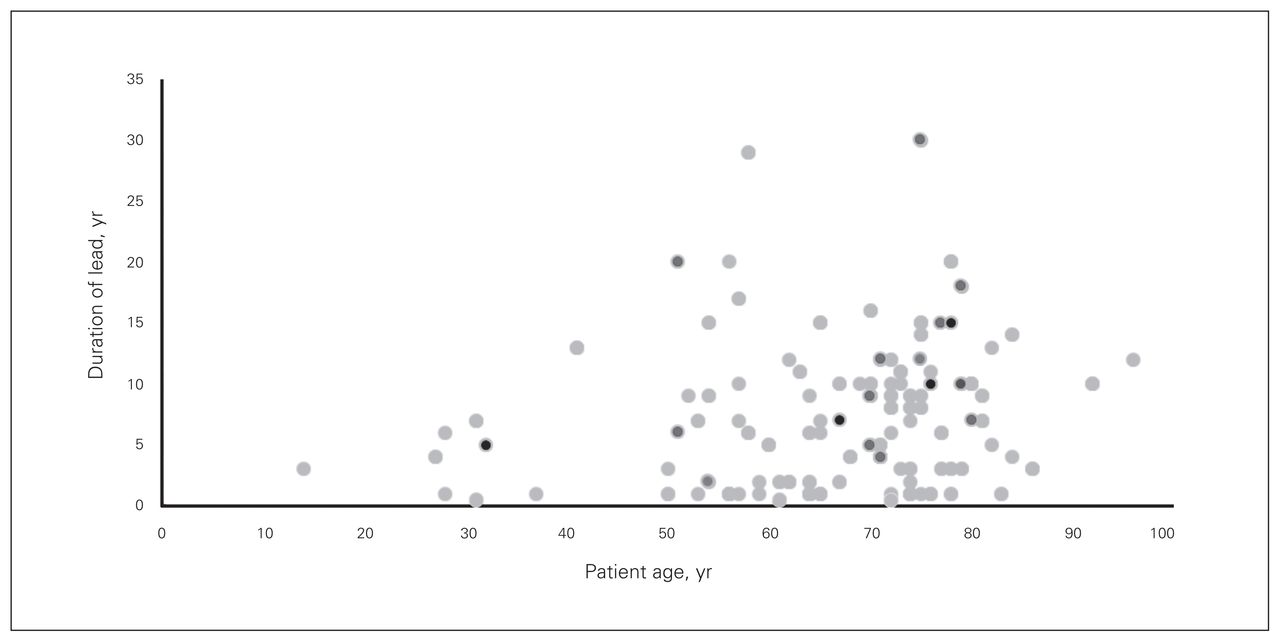
Patient age versus the duration of implanted devices is represented in Figure 1, where the previously stated characteristics are demonstrated visually. This figure illustrates how a significant number of leads were more than 10 years old, with some as old as 20–30 years.
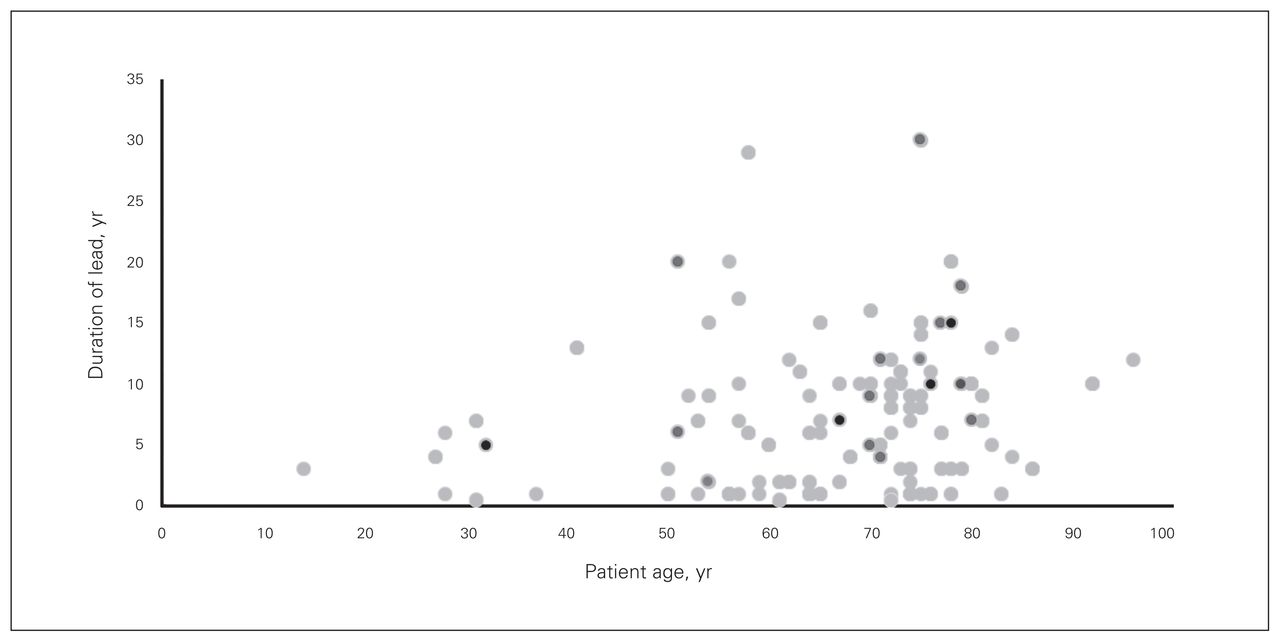
Lead implant duration versus respective patient age. Light grey circles represent leads that were successfully extracted without complication, dark grey circles represent leads for which major complications occurred during extraction, and black circles represent targeted leads that were not extracted.
Long-term outcomes
Follow-up after discharge was available for all patients in the first 12 months postoperatively, but for only 32 (29.63%) patients beyond 12 months postoperatively. The median follow-up after extraction in our study was 14 (range 6–16) months. Using Kaplan–Meier analysis the 30-day survival was 98.4% and 1-year survival was 94.0% (Fig. 2).

Kaplan–Meier analysis of 12-month survivorship among patients who underwent lead extraction.
Discussion
The aim of the present study was to illustrate the initial experience of a laser lead extraction program at the low-volume Maritime Heart Centre, which is the only referral centre for this procedure for Atlantic Canada and serves a population of approximately 2.4 million.14 Laser lead extraction is an increasingly common procedure throughout the world, but it is associated with potentially life-threatening complications (e.g., cardiovascular perforations, arrhythmias and death).1,2 Therefore, it was important for the Atlantic provinces to develop a program that consisted of experienced surgeons and support staff who could provide a superior standard of care in a timely manner — especially as the Atlantic provinces have the most elderly population and a large proportion of patients with chronically implanted leads and multiple simultaneous implanted leads, which are serious comorbidities in laser lead extraction patients.12,14,15
Together, our findings suggest that acceptable outcomes could be achieved in a low-volume centre using a standardized superior (subclavian) approach and concentrating the expertise to a limited number of operators. Similar procedural and clinical results have been reported in larger, multi-institutional studies, such as the LExICon study (n = 1449), which had procedural and clinical success rates of 96.5% and 97.7%, respectively.16 Likewise, a Canadian registry (n = 684) reported procedural and clinical success rates of 91.4% and 93.1%, respectively.9 Although it is difficult to compare our results to those of these large studies owing to the limited number of patients in our cohort, notably, we report consistent positive findings from patients who had leads in place for longer periods of time than those in other studies, and extended implantation periods is a known predictor of procedural failure or major complications.12 We reported an average duration of chronically implanted leads of 7.1 ± 6.0 years, with 51.9% of patients having leads older than 5 years and 21% having leads older than 10 years. This contrasts with the extracted lead duration of 5.7 ± 0.2 years reported in larger studies.9,16 The duration of a lead has been clearly shown to correlate with potentially difficult extractions and major adverse events, or to result in extraction failure.16,17 A single patient in our series sustained a major vascular injury (perforation of the innominate vein, or brachiocephalic vein) during an attempt to extract a 20-year-old lead, requiring an emergency sternotomy. An additional 2 patients had elective sternotomies because of the inability to extract all infected lead material in 18- and 30-year-old leads. The incidence of procedure-related minor complications was frequent, occurring in 50.9% of patients; however, none of these patients required additional interventions.
Device-related infection was the most common indication for laser lead extractions in our series.4,16,18 We found that 84.3% of patients had some form of device-related infection ranging from localized pocket infection to systemic infection, such as endocarditis. This finding contrasts those of many larger series in which infection was present in only 35%–62% of the patient population, making our study population unique.3,16,19 Nevertheless, infection is the leading indication for laser lead extraction in North America, with significant increases in the incidence of infection during the past several years.20 Device-related infection has been shown to be an important indicator of higher mortality, with a mortality as high as 66% reported in untreated patients versus 18% following extraction and antibiotic treatment.21 This potentially high mortality explains the drive behind the 2 patients in our series who underwent elective sternotomies to ensure complete removal and improve long-term survival.19,20 The removal of all infected devices and proximal material is vital to prevent reoccurrence of bacteremia or the development of endocarditis.21 To the best of our knowledge we have not seen long-term recurrence of infection in patients who underwent partial lead extraction, particularly patients in whom a small piece of lead material was left in the cardiac tissue or vasculature (n = 8). The median follow-up after extraction in our study was 14 (range 6–16) months, with 98.6% 30-day survival and 94% 1-year survival.
Our study has reported an in-hospital mortality of 0.9%, which is similar to that reported in previous studies (0.7%–1.9%).5,7,9 What is unique about our program is that all procedures were performed by a cardiovascular surgeon in a dedicated operating room setting. This meant that all patients were ready for emergent sternotomy and extracorporeal bypass system on standby, as well as hemodynamic stability monitoring via atrial pressure and transesophageal echocardiography to facilitate rapid diagnosis of procedural complications. The present study was in no way designed to validate the use of an operating room with a surgeon present as opposed to a procedure room, such as catheterization laboratory (EP laboratory), without a surgeon. Operating room versus catheterization laboratory extraction outcomes have been examined and have been found to produce similar results.9 One should note that our standardized approach allowed for an efficient transition (without delay) from the lead extraction to emergent sternotomy in the patient who experienced a life-threatening perforation of the innominate vein, leading to sudden cardiovascular collapse. The patient had had previous coronary artery bypass graft, which increased the difficulty of the repeat sternotomy owing to the presence of scar tissue as well as blood loss. The success of her restorative surgery was possible only given the readiness of the surgical team (i.e., nursing, perfusion, anesthesiologist and surgeon) in the room. The patient survived without major sequelae. The length of stay in hospital after the procedure in our study was 8.2 ± 11.1 (median 5, range 2–7.25) days, which was longer than the typical 5–7 days reported previously.16,22 We speculate that the extended in-hospital period in our patient population correlates with the finding that most of the patients’ primary extraction indications had been infection (84.3%), which subsequently meant extended antibacterial treatment or wound care before discharge.4,20,22
We hope that this study serves as a stepping stone in terms of improving this program not only at the Maritime Heart Centre, but also at low-volume centres across Canada. Furthermore, following the promising results of this study, we also hope to expand our program by including more than only patients with class I indications and by incorporating different extraction techniques, such as a femoral extraction approach. This approach has been demonstrated to allow procedural and clinical success when a superior (subclavian) approach has failed and may allow the program to reduce the number of sternotomies for nonperforation-related complications (i.e., lead migration, lead fragmentation, or a congested heart).23,24 Additionally, as members of our operative team are currently collaborating to create a national registry for lead extraction, and as both surgeons and EP physicians are collaborating on uniquely Canadian laser lead extraction guidelines, it is our hope that our program will stay among the institutions at the forefront of medical innovation in Canada and provide the best possible care for patients with complex lead issues.
Limitations
An important limitation of this study is its small sample size. We specifically examined only patients who underwent laser-assisted extractions, excluding patients whose leads were removed via nonpowered counter-traction. As such, the present study focused only on leads that could not be removed by simple traction and focused on leads that were technically more challenging, which may explain why infection was a predominant indication.11,19 This study may not truly evaluate the clinical needs for lead extraction in Atlantic Canada, but it provides some insight into the incidence of device-related infections that require extraction for a particular patient population.
Compared with other extraction studies,17,25 our study tended to look at an exhaustive list of possible minor complications. Subsequently, the larger number of complication variables examined produced a higher minor complication rate than those reported in other studies. One should note that none of the minor complications reported resulted in additional interventions.
Conclusion
The impetus for the creation of the laser lead extraction program was based on a clinical need and the desire to avoid transferring patients to larger institutions in Montreal, Que. This study showed that a high success rate with a low complication rate and low mortality can be achieved in a low-volume centre serving a large geographical area. Patient comorbidities, such as chronically (> 1 yr) implanted leads, advanced patient age and arrhythmia, and complications, such as perforation and postoperative arrhythmia, were overcome by concentrating the technical expertise to a limited number of surgeons and dedicated cardiac nursing staff.
Footnotes
Funding: Division of Cardiac Surgery, Dalhousie University.
Competing interests: None declared.
Contributors: J-F. Légaré, K. Williams and S. O’Keefe designed the study. K. Williams and S. O’Keefe collected the data, which K. Williams analyzed. K. Williams wrote the article, which all authors reviewed and approved for publication.
- Accepted January 11, 2016.
References
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.