


Abstract
Background: The introduction of 4-joint operating rooms (ORs) to meet provincial wait time targets represented a major change in practice, providing an opportunity to optimize patient care within an OR time allotment of 8 hours. We reviewed our success rate completing 4 joint replacements within 8 hours and defined benchmarks for successful completion.
Methods: We reviewed the surgeries performed in the 4-joint ORs between May and October 2012. Using prospectively collected data from the Surgical Information Management System, each surgery time was divided into the following components: anesthesia preparation time (APT), surgical preparation time (SPT), procedure duration, anesthesia finishing time (AFT) and turnover time. We defined success as 4 joint replacements being completed within the allotted time.
Results: We reviewed 49 4-joint OR days for a total of 196 joint surgeries. Of the 49 days, 24 (49%) were successful. Only 2 surgeons had a success rate greater than 50%. Significant predictors of success were APT (odds ratio 1.09, 95% confidence interval [CI] 1.02–1.16), procedure duration (odds ratio 1.02, 95% CI 1.00–1.05) and AFT (odds ratio 1.19, 95% CI 1.06–1.34). We calculated probabilities for each component and derived benchmark times corresponding to the probability of 0.60. These benchmarks were APT of 9 min, SPT of 14 min, procedure duration of 68 min, AFT of 4 min and turnover of 15 min.
Conclusion: We established benchmark times for the successful completion of 4 primary joint replacements within an 8-hour shift. Targeted interventions could maximize OR efficiency and enhance multidisciplinary care delivery.
There is no doubt that joint replacement surgery improves the quality of life of patients with arthritis.1 In recent years, research has focused on registry data to determine trends in patient profiles and to form a quality control process for assessing the success rate of various implant designs. In addition, institution and government agencies are paying closer attention to readmission rates, rates of superficial wound infection and overall quality of care delivery within that context.2 Overall efficiency is also being examined by these multiple stakeholders. This is particularly relevant in a single payer system like Canada’s, in which public funds are the sole source of financing and increasing demand is coupled with increasing government deficits. Capacity to increase delivery of joint replacements must be accomplished without increasing costs. In 2005, based on the National Health Services initiative, the Canadian government mandated through the National Wait Times Initiative (NWTI) that patients receive their hip or knee replacement within 6 months of the decision for surgery.3 The most recent data from the Canadian Institute of Health Information (CIHI)4 show there is still considerable room for improvement, with most provinces being under the 90% goal despite funding directed specifically to decrease wait lists (Fig. 1).4
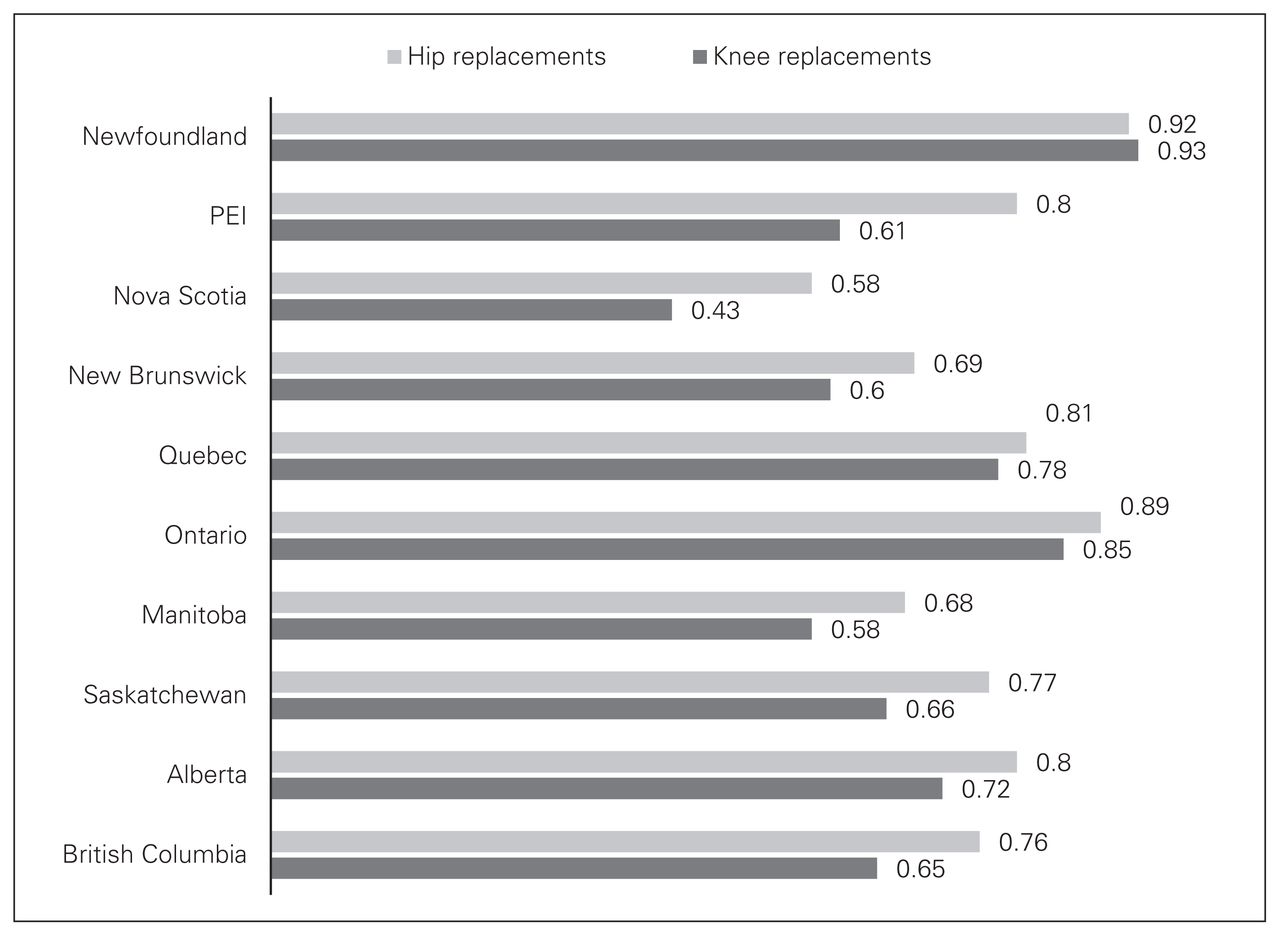
Lower-extremity arthroplasties by Canadian province, 182-day success rate. PEI = Prince Edward Island.
Various models with set benchmarks (e.g., centralized intake clinics that separate wait times into multiple components: time to consult, time to surgical decision and finally time to surgery) have been introduced to improve access to joint replacement care.5 In addition, how to best improve operating room (OR) efficiency has been a subject of much interest in order to meet the increasing demand for joint replacement putting a substantial burden on the hospital system owing to limited resources. Although several groups have looked at OR inefficiencies, such as turnaround time and dedicated teams,6,7 there is still a lack of established benchmarks to successfully maximize OR efficiency without increasing resources.8,9
In 2004, a 4-joint OR initiative was instituted within our hospital to minimize wait times for joint replacements by improving overall throughput while minimizing the need to increase the number of OR days to perform joint replacement surgery. As part of this initiative, team leaders, customized joint instrument trays and patient selection parameters (i.e., body mass index [BMI] < 35, American Society of Anaesthesiologists [ASA] score of 2 or less, no prior joint surgery) were established. The purpose of the present study was to look at the overall success of our high-volume ORs for performing primary joint replacements and to define the factors that are associated with successful completion of 4-joint OR cases within a standard 8-hour shift.
Methods
Four-joint OR data from May 1 to Oct. 31, 2012, were analyzed retrospectively for surgical times. We obtained approval from our institutional ethics committee before the study began.
The goal of the 4-joint room initiative was to complete the cases within a standard 8 hour shift (i.e., 7:30 am to 3:30 pm). All joint replacements were completed by 5 arthroplasty surgeons and 27 different anesthesiologists. Spinal and general anesthetic are both commonly used for lower extremity reconstruction, and the anesthesiologist decided on the method of anesthesia in consultation with the patient. Our institution does not have a block room and, as such, all spinal anesthetics were administered after the patient entered the operating theatre. All surgical time data were prospectively entered using the Surgical Information Management Systems (SIMS). The surgical time intervals were defined using the following events as outlined by the American Association of Clinical Directors, with modifications noted by asterix: anesthesia preparation time (APT; patient in room* to anesthesia ready), surgical preparation time (SPT; anesthesia ready to procedure start), procedure duration (procedure start time to procedure finish), anesthesia finish time (AFT; procedure finish to patient out of room*), and turnover time (room cleanup start to patient in room).10 The APT immediately follows turnover time during the day, as a smooth transition into the room is expected once the room is ready.
Statistical analysis
We report basic descriptive statistics (mean, median, standard deviation and range) as appropriate. For the analysis of surgical time components, we used t tests to compare surgical intervals on successful and unsucessful days. Success was defined as the last patient (fourth case) of the day leaving the operating theatre within the allotted 8-hour shift. We performed logistic regression analysis to determine significant predictors for success of 4-joint ORs. Furthermore, we used the following equation to calculate predicted probabilities (p) for each time component, averaged per day: p = e ^ (a + bTime)/(1 + e ^ (a + bTime)).
Results
During the study period, 196 joint replacements were completed in 49 4-joint OR days: 80 (40.8%) total hip arthroplasties (THA), 55 (28%) total knee arthroplasties (TKA), 38 (19.4%) hip resurfacing (HR) and 23 (11.7%) unicompartmental knee arthroplasties (UKA). The mean age of patients was 62 (range 25–87) years; 85 patients were men and 111 were women (Table 1). The mean BMI was 29.6 (range 20.5–48.3), and the median ASA score was 2 (range 1–3). Twenty-four patients received a general anesthetic, and 164 had a spinal anesthetic. There were 8 cases of converted spinal to general anesthetics.
Patient demographic and clinical characteristics
The overall success rate for completion of 4-joint OR days within the allotted time was 49% and varied from 0% to 80% among surgeons. The mean procedure duration for all procedures was 70 (range 33–113) min (Table 2). Each surgical time interval is reported in Table 3, with mean, maximum and minimum values. The mean procedure duration for days that were successful versus unsuccessful were 68.6 ± 13.2 and 72.2 ± 12.4 min, respectively (95% confidence interval [CI] −7.2 to −0.01, p = 0.05). Procedures were slightly shorter on successful days for 3 of the 4 surgeons (surgeons A, C and D) who had more than 1 successful day, although this difference for each surgeon was not significant (Table 4).
Procedure duration, by procedure and surgeon
Interval durations
Procedure durations for successful and unsuccessful days by surgeons
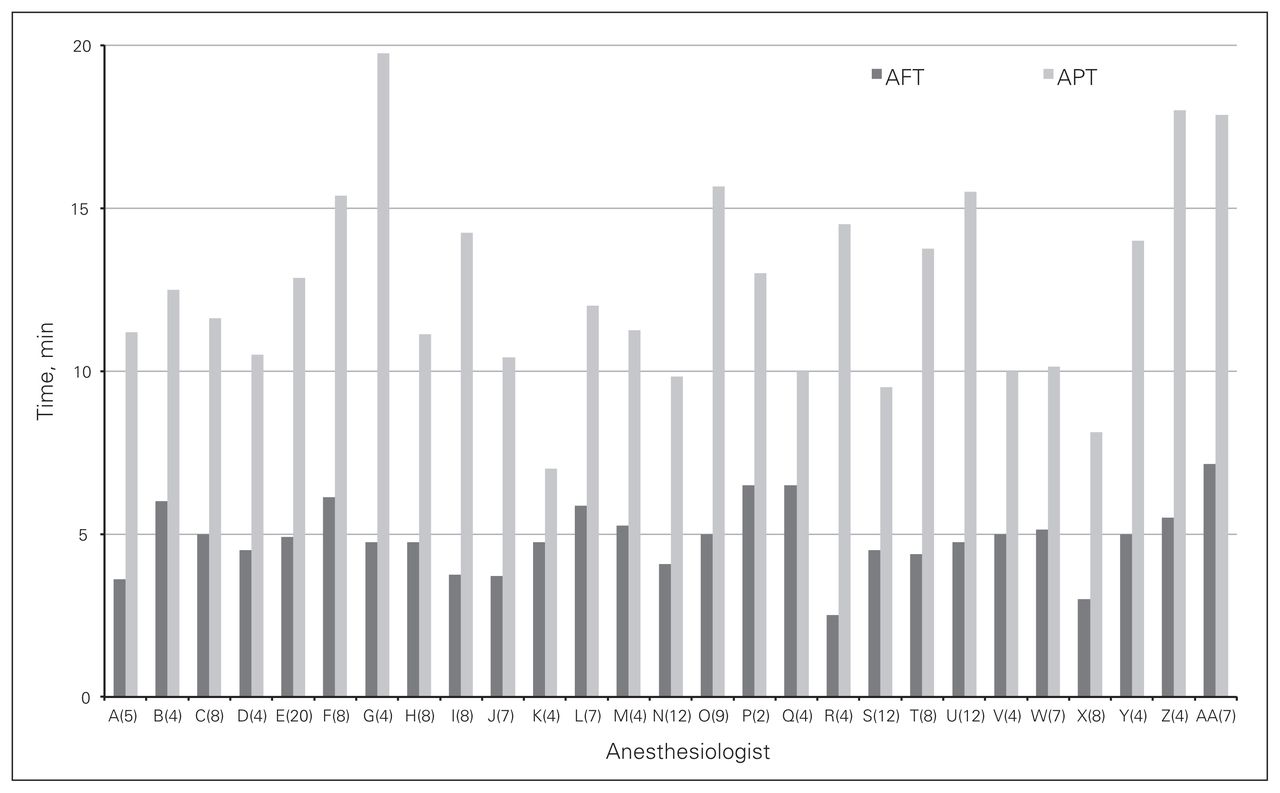
Each temporal component was averaged per day, and we used logistic regression to calculate predicted probability of success (Table 5 and Table 6). The maximum probabilities of success for the temporal components ranged from 0.6 to 0.902. Owing to this variability, approximate times that corresponded to the predicted probability of 0.60 were arbitrarily chosen as benchmark estimates. Five anesthesiologists met the average APT benchmark of 9 min, with the range for daily averages spanning 7–20 min. Reaching the benchmark was common, with 32% of cases having an APT of less than 9 min; however, daily averages were much more difficult for the various physicians to achieve. Five of 27 anesthesiologists were able to meet the AFT target of 4 min, with the range of daily averages spanning 2.5–7.8 min. Individual results are shown in Figure 2.
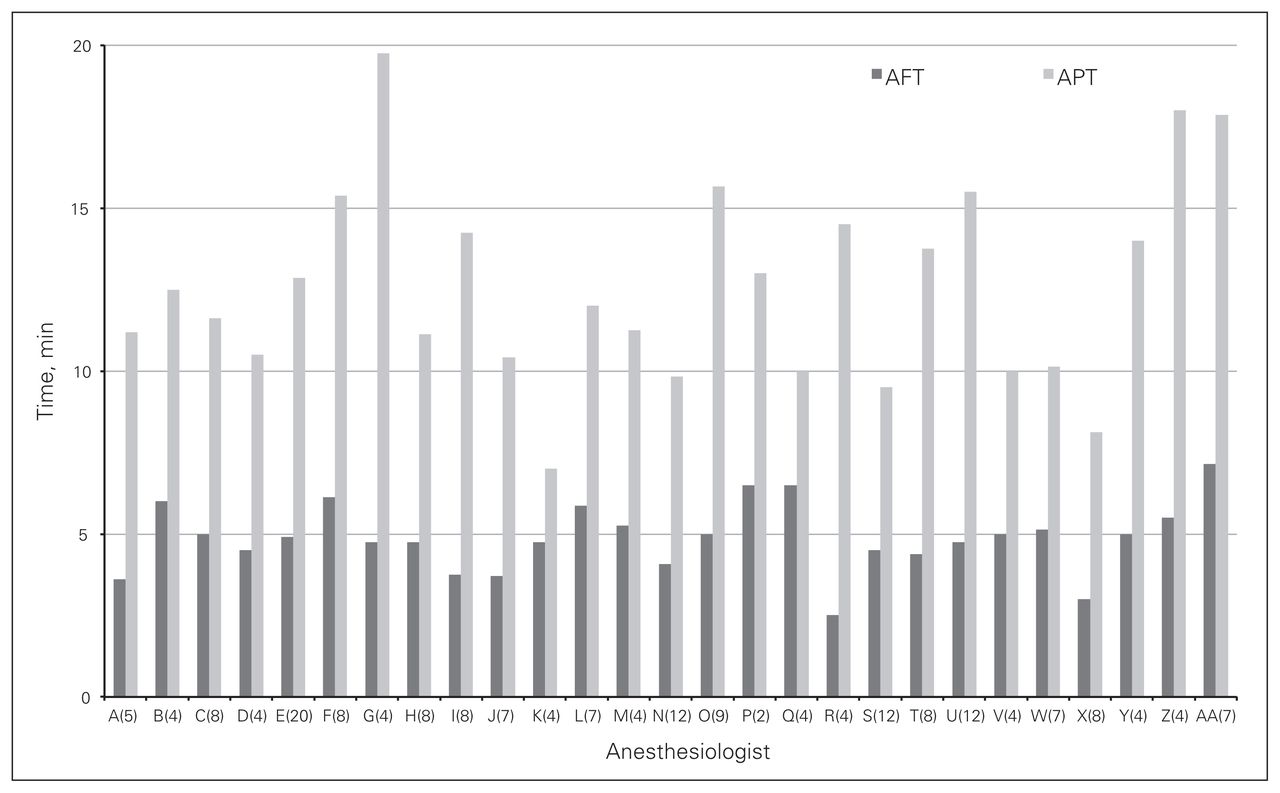
Breakdown of average anesthesia preparation time (APT) and anesthesia finishing time (AFT) by anesthesiologist with number of cases completed in a 4-joint operating room during the study period in brackets beside the identifier.
Maximum surgical interval times that correspond to 60% success rate (benchmark) and their odds for predicting success
Comparison between successful and unsuccessful days
In order to determine factors that contribute to success, we performed a logistic regression analysis with various surgical (procedure type, surgeon, anesthesiologists) and temporal components. Only the following temporal components emerged as significant predictors of success: APT (odds ratio 0.92, 95% CI 0.86–0.98), procedure duration (odds ratio 0.98, 95% CI 0.95–1.00) and AFT (odds ratio 0.84, 95% CI 0.74–0.94).
Discussion
The demands on the Canadian health care system to do more and better with less are growing, and although some may say that there is no more capacity within our system, there are health care organizations that are succeeding. One model that has been applied with success is that of Lean, which originates from the automotive industry.11 In addition, not only did we find that variability in both surgeon and anesthesiologist had a significant impact on successful completion, we were also able to delineate other steps (i.e., SPT and AFT) affecting OR efficiency.
Efficiency in the OR is not only increasing case volume, but also using the same or fewer resources. Given the fixed nature of resources and the inability to expand owing to budget and physical plant restrictions, increasing efficiency is paramount to survival in the modern health care environment. Our study provides a guide for efficient utilization of resources within a standard OR shift to increase throughput of primary arthroplasty cases without increasing the budgetary demands by using overtime, extra personnel or added resources, such as block rooms. While other strategies, such as block rooms, have been shown to increase the volume of operations, their role in increasing efficiency is less clear.5 More importantly, the increased efficiency requires buy-in from all team members, including the anesthesiology team (e.g., the anesthesiologist will often meet the patient outside the OR during turnover time, allowing a smooth transition into APT from turnover time).
In addition, the benchmarks we developed and the methods we used to determine them can be spread to other specialties, such as bariatric and thoracic surgery, where a step-wise procedure is carried out with high-volume and predictable pre-, intra- and postoperative processes in a given setting. More importantly, the predictors of success were examined as individual markers, so if all 4 successful benchmarks (APT of 9 min × 4, SPT of 11 min × 4; procedure duration of 66 min × 4; AFT of 4 min × 4; turnaround time of 15 min × 3) were combined, the 4-joint OR day would be completed in 6.75 hours, leaving room for unpredictable delays, such as a difficult induction and/or surgical exposures as well as teaching. By knowing where the workday is against the benchmarks, the surgeon can allocate various responsibilities to residents/fellows and predictably know that the day will finish on time. More importantly, one can better integrate additional resources (e.g., block rooms, possibly a fifth case) to maximize efficiency.
The pool of patients eligible for a joint replacement is not a perfectly homogeneous population, but some trends are present. We initially intended to include only patients with an ASA score of 2 or less and a BMI of 35 or less to allow for successful completion of our 4-joint OR days; however, this was not an attainable booking strategy as too high a percentage of arthroplasty patients were excluded by these restrictions. Whenever possible, these physical parameters were maintained; however, the incidence of increased BMI and ASA score was not significantly different between successful and unsuccessful days in the data analyzed for the present study.
Limitations
One of the limitations of our study is that the recording of the data within the SIMS system was done by different individuals, potentially introducing variability in the accurate assessment of the different time points. Having said that, the data were collected in the same fashion for all cases, consequently minimizing the possible bias in data gathering. More importantly, all members of the OR team were unaware that these data would be later analyzed, making our analysis a real-life assessment and preventing a Hawthorne effect. Another limitation of our study is the lack of specialized teams (i.e., anesthesiologists), making unclear the potential impact of a specialized team on the various benchmarks. However, because of this lack of specialized teams, our findings are likely more applicable to a wider community of surgeons across the country. Hospitals that already have specialized anesthesiology and nursing teams may be able to more efficiently implement our benchmarks to ensure successful completion of their lists, whereas community hospitals in which human resources are more limited may be able to work toward specialized teams to make their resources go further. Within that context, it is unknown whether a minimum number of joint replacements is required or desired to institute high-efficiency joint replacement ORs. Finally, the level of success was set relatively low at 60%; most individuals and institutions would set higher targets for success at 80%–90%. The low level of success in our study is because of the relatively small number of cases with an associated high variability for the different time points. Having said that, with both groups (successful v. unsuccessful 4-joint ORs) being comparable in regards to procedure type, BMI and sex, this certainly permitted us to focus on the surgical workflow, making our findings applicable to most institutions.
Interestingly when looking at the impact of procedure duration, surgeon D’s average duration did not differ between successful and unsuccessful days, highlighting the importance of the team and other time points, such as AFT, for the completion of the 4 cases within an 8-hour timeframe. All too often, the surgeon scrubs out once the wound is closed and goes on to complete other administrative tasks, which may give the impression that the “case” is finished and everyone can take a break. Because the SIMS software did not capture the time of departure of the surgeon, we cannot analyze the impact of the surgeon leaving the OR before the patient on overall room efficiency, but this is a possible next step for analysis. As our study has shown, completing this task of exiting the room in an efficient and coordinated manner is as critical as other key aspects of surgical workflow. Similarly the importance of specialized teams is highlighted by the large variability in APT with the 27 anesthesiologists, which contrasts relative grouping of the mean procedure durations within our surgeon group (Table 6). Because the number of arthroplasties to be done per year is capped, it is unlikely that a sufficient number of cases would be available for all 27 anesthesiologists to reach the proficiency required. More importantly, the benefits of an integrated team approach as well as the capacity to provide interprofessional feedback and sustaining the gains in efficiency are lost. The benefits of dedicated teams of highly specialized individuals who share a common goal in improving efficiency in ORs, including academic joint replacement rooms, are well known6,7 and, in turn, permit the maximization of other workflow efficiency measures, such as block/induction rooms, which despite requiring increases in physical resources may permit a greater number of cases to be performed and the patient selection criteria to be expanded (e.g., higher BMI).
Conclusion
Joint replacement programs are the cause of a large part of both a hospital’s expenditures and revenue.9 By breaking down the delivery of this service in a stepwise fashion, we were able to identify predictive measures to allow the successful completion of 4 primary joint replacements in a standard 8-hour OR day. These benchmarks can facilitate targeted group interventions to improve efficiency and provide direct feedback in regards to individual performances. More importantly, the presence of dedicated teams will ensure the sustainability of these efforts.
Acknowledgements
The authors thank Dr. Tim Ramsay at the Ottawa Hospital Research Institute Methods Centre for his statistical advice, Ms. Suham Alexander for providing SIMS data and Mrs. Paula Doering for administrative support at The Ottawa Hospital.
Footnotes
Competing interests: None declared.
Contributors: P. Beaulé designed the study. A. Frombach acquired and analyzed the data, which JJ Ryu also analyzed. A. Frombach wrote the article, which all authors reviewed and approved for publication.
- Accepted July 14, 2015.
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.