Posttraumatic Stress Disorder-Associated Cognitive Deficits on the Repeatable Battery for the Assessment of Neuropsychological Status in a Veteran Population
Nathan Hantke is a Clinical Neuropsychologist in the Mental Health and Clinical Neuroscience Division at the US Department of Veterans Affairs (VA) Portland Health Care System in Oregon. Dana Waltzman is a Postdoctoral Fellow, Jennifer Kong is a Clinical Director, John Ashford is the Director, and Jerome Yesavage is the Executive Director; all at the War Related Illness and Injury Study Center; Lisa Kinoshita is a Clinical Neuropsychologist at the VA Memory Clinic; Tong Sheng is a Program Analyst in Polytrauma System of Care; Sherry Beaudreau is an Investigator in the Sierra Pacific Mental Illness Research, Education, and Clinical Center (MIRECC): J. Kaci Fairchild is an Associate Director, Jerome Yesavage is the Director; all at the MIRECC; Maheen Adamson is a Clincial Research Senior Scientific Director in the Rehabilitation Service, all at the VA Palo Alto Health Care System in California. Art Noda is a Research Data Analyst, J. Kaci Fairchild, Sherry Beaudreau, John Ashford, Jerome Yesavage, and Laura C. Lazzeroni are Professors, Dana Waltzman is a Postdoctoral Fellow, all in the Stanford Department of Psychiatry and Behavioral Sciences; Maya Yustis is a Clinical Neuropsychologist and Clinical Assistant Professor (affiliated) in the Stanford Neuroscience Institute, and Maheen Adamson is a Clinical Associate Professor in the Department of Neurosurgery, all at Stanford University School of Medicine in California. Nathan Hantke is an Assistant Professor in the Department of Neurology at Oregon Health and Science University in Portland. Correspondence: Nathan Hantke (hantke@ohsu.edu) *Colead authors.
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies.
Background: Posttraumatic stress disorder (PTSD) is a frequent problem of veterans receiving care and is often associated with cognitive deficits. The Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) is a well-validated cognitive screening measure often used in the US Department of Veterans Affairs (VA), particularly in neurorehabilitation settings. However, the influence of PTSD on RBANS performance is unclear, particularly within a heterogeneous VA outpatient population in which PTSD and traumatic brain injury (TBI) may not be the primary focus of care.
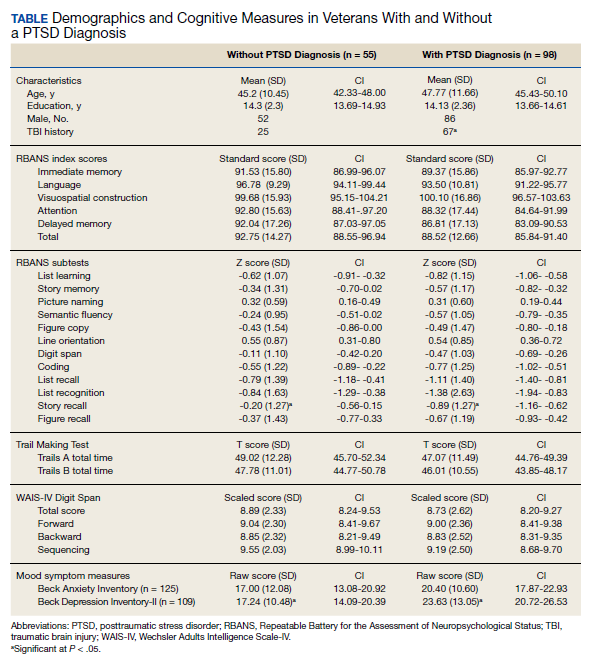
Methods: Participants included 153 veterans with complex deployment-related health problems, including a diagnosis of PTSD (n = 98) and a history of TBI (n = 92). All veterans completed a targeted cognitive battery that included the Wechsler Test of Adult Reading, the Wechsler Adults Intelligence Scale, measure assessing processing speed, attention, and cognitive flexibility, and RBANS.
Results: A diagnosis of PTSD was associated with worse performance on the Story Recall subtest of the RBANS, but not on any other cognitive measures. A diagnosis of mild TBI, or co-occurring PTSD and TBI did not predict cognitive performance on any measures.
Conclusions: The RBANS best captured cognitive deficits associated with PTSD compared with a history of mild TBI or co-occurring mild TBI and PTSD. These findings may provide insight into the interpretation and attribution of cognitive deficits in the veteran population.
Posttraumatic stress disorder (PTSD) affects about 10 to 25% of veterans in the US and is associated with reductions in quality of life and poor occupational functioning.1,2 PTSD is often associated with multiple cognitive deficits that play a role in a number of clinical symptoms and impair cognition beyond what can be solely attributed to the effects of physical or psychological trauma.3-5 Although the literature on the pattern and magnitude of cognitive deficits associated with PTSD is mixed, dysfunction in attention, verbal memory, speed of information processing, working memory, and executive functioning are the most consistent findings.6-11Verbal memory and attention seem to be particularly negatively impacted by PTSD and especially so in combat-exposed war veterans.7,12 Verbal memory difficulties in returning war veterans also may mediate quality of life and be particularly disruptive to everyday functioning.13 Further, evidence exists that a diagnosis of PTSD is associated with increased risk for dementia and deficits in episodic memory in older adults.14,15
The PTSD-associated cognitive deficits are routinely assessed through neuropsychological measures within the US Department of Veteran Affairs (VA). The Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) is a commonly used cognitive screening measure in medical settings, and prior research has reinforced its clinical utility across a variety of populations, including Alzheimer disease, schizophrenia, Parkinson disease, Huntington disease, stroke, and traumatic brain injury (TBI).16-24
McKay and colleagues previously examined the use of the RBANS within a sample of individuals who had a history of moderate-to-severe TBIs, with findings suggesting the RBANS is a valid and reliable screening measure in this population.25However, McKay and colleagues used a carefully defined sample in a cognitive neurorehabilitation setting, many of whom experienced a TBI significant enough to require ongoing medical monitoring, attendant care, or substantial support services.
The influence of PTSD-associated cognitive deficits on the RBANS performance is unclear, and which subtests of the measure, if any, are differentially impacted in individuals with and those without a diagnosis of PTSD is uncertain. Further, less is known about the influence of PTSD in outpatient clinical settings when PTSD and TBI are not necessarily the primary presenting problem. The purpose of the current study was to determine the influence of a PTSD diagnosis on performance on the RBANS in an outpatient VA setting.
Methods
Participants included 153 veterans who were 90% male with a mean (SD) age of 46.8 (11.3) years and a mean (SD) education of 14.2 (2.3) years from a catchment area ranging from Montana south through western Texas, and all states west of that line, sequentially evaluated as part of a clinic workup at the California War Related Illness and Injury Study Center (WRIISC-CA). WRIISC-CA is a second-level evaluation clinic under patient primary care in the VA system dedicated to providing comprehensive medical evaluations on postdeployment veterans with complex medical concerns, including possible TBI and PTSD. Participants included 23 Vietnam-era, 72 Operation Desert Storm/Desert Shield-era, and 58 Operation Iraqi Freedom/Enduring Freedom-era veterans. We have previously published a more thorough analysis of medical characteristics for a WRIISC-CA sample.26
A Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM IV) diagnosis of current PTSD was determined by the Clinician-Administered PTSD Scale (CAPS-IV), as administered or supervised by a licensed clinical psychologist during the course of the larger medical evaluation.27 Given the co-occurring nature of TBI and PTSD and their complicated relationship with regard to cognitive functioning, allveterans also underwent a comprehensive examination by a board-certified neurologist to assess for a possible history of TBI, based on the presence of at least 1 past event according to the guidelines recommended by the American Congress of Rehabilitation Medicine.28,29Veterans were categorized as having a history of no TBI, mild TBI, or moderate TBI. No veterans met criteria for history of severe TBI.Veterans were excluded from the analysis if unable to complete the mental health, neurological, or cognitive evaluations. Informed consent was obtained consistent with the Declaration of Helsinki and institutional guidelines established by the VA Palo Alto Human Subjects Review Committee. The study was approved by the VA Palo Alto and Stanford School of Medicine institutional review boards.