
Abstract
Background
Surgical site infections (SSIs) lead to increased patient morbidity and healthcare costs. Our objective was to decrease the SSI rate following gynecologic surgery.
Methods
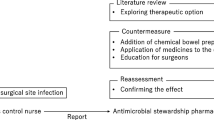
Adult patients undergoing abdominal surgery for gynecologic malignancy or benign disease received the following: patient education; preoperative antibacterial soap; appropriate antibiotic prophylaxis; change of gloves and use of clean instruments at surgical closure; surgical dressing for 48 h; and a post-discharge phone call. The baseline SSI rate was determined retrospectively (1 April 2014–30 June 2014), while the post-intervention SSI rate was determined prospectively (16 February 2015–15 October 2015). The main outcome was the overall SSI rate with secondary outcomes, including the rate of superficial, deep, incisional and organ space infection, as well as the cost effectiveness of the bundle.
Results
A total of 232 baseline and 555 post-intervention patients were included in the study. No differences were observed between the baseline and post-intervention groups with regard to median body mass index (BMI), surgical approach, receipt of preoperative chemotherapy and/or radiation therapy, and cases including bowel surgery. Overall, the SSI rate decreased significantly from baseline [12.5 %] to post-intervention [7.4 %] (odds ratio [OR] 0.56, 90 % confidence interval [CI] 0.37–0.85; p = 0.01). A 40 % decrease was noted in the rate of superficial and deep infections (9.5 vs. 5.9 %; OR 0.60, 90 % CI 0.38–0.97; p = 0.04) and SSIs after open surgery (21.4 vs. 13.2 %; OR 0.56, 90 % CI 0.34–0.92; p = 0.03). The estimated cost of the intervention was $19.26/case and the net total amount saved during the post-intervention period was $65,625 month.
Conclusions
This bundled intervention led to a significant decrease in the overall SSI rate and was cost effective. The largest decreases in SSIs were in incisional infections and following open surgery.

Similar content being viewed by others


References
Tran CW, McGree ME, Weaver AL, et al. Surgical site infection after primary surgery for epithelial ovarian cancer: predictors and impact on survival. Gynecol Oncol. 2015;136(2):278–84.
Kirkland KB, Briggs JP, Trivette SL, Wilkinson WE, Sexton DJ. The impact of surgical-site infections in the 1990s: attributable mortality, excess length of hospitalization, and extra costs. Infect Control Hosp Epidemiol. 1999;20:725–70.
Itani KF. Care bundles and prevention of surgical site infection in colorectal surgery. JAMA. 2015;314(3):289–90.
de Lissovoy G, Fraeman K, Hutchins V, Murphy D, Song D, Vaughn BB. Surgical site infection: incidence and impact on hospital utilization and treatment costs. Am J Infect Control. 2009;37(5):387–97.
Alexander JW, Fischer JE, Boyajian M, Palmquist J, Morris MJ. The influence of hair-removal methods on wound infections. Arch Surg. 1983;118(3):347–52.
Bullock R, van Dellen JR, Ketelbey W, Reinach SG. A double-blind placebo controlled trial of perioperative prophylactic antibiotics for elective neurosurgery. J Neurosurg. 1988;69(5):687–91.
Page CB, Bohnen JM, Fletcher JR, McManus AT, Solomkin JS, Wittmann DH. Antimicrobial prophylaxis for surgical wounds. Guidelines for clinical care. Arch Surg. 1993;128(1):79–88.
ACOG committee on practice bulletins. ACOG practice bulletin no. 74. Antibiotic prophylaxis for gynecologic procedures. Obstet Gynecol. 2006;108(1):225–34.
Rodrigues AL, Simões Mde L. Incidence of surgical site infection with pre-operative skin preparation using 10 % polyvidone-iodine and 0.5 % chlorhexidine-alcohol. Rev Col Bras Cir. 2013;40(6):443–48.
Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. The Hospital Infection Control Practices Advisory Committee. Guideline for prevention of surgical site infection, 1999. Hospital Infections Program, National Center for Infectious Diseases, Centers for Disease Control and Prevention, Public Health Service, US Department of Health and Human Services. Infect Control Hosp Epidemiol. 1999;20(4): 274.
Eaglstein WH, Davis SC, Mehle AL, Mertz PM. Optimal use of an occlusive dressing to enhance healing effect of delayed application and early removal on wound healing. Arch Dermatol. 1988;124:392–95.
Girabaldi RA. Prevention of intraoperative wound contamination with chlorhexidine shower and scrub. J Hosp Infect. 1988;11:5–9.
Keenan JE, Speicher PJ, Thacker JM, Walter M, Kuchibhatla M, Mantyh CR. The preventive surgical site infection bundle in colorectal surgery: an effective approach to surgical site infection reduction and health care cost savings. JAMA Surg. 2014;149(10):1045–52.
Cima R, Dankbar E, Lovely J, et al. Colorectal surgery surgical site infection reduction program: a national surgical quality improvement program—driven multidisciplinary single-institution experience. J Am Coll Surg. 2013;216(1):23–33.
Novetsky AP, Zighelboim I, Guntupalli SR, et al. A phase II trial of a surgical protocol to decrease the incidence of wound complications in obese gynecologic oncology patients. Gynecol Oncol. 2014;134(2):233–37.
Johnson MP, Kim SJ, Langstraat CL, et al. Using bundled interventions to reduce surgical site infection after major gynecologic cancer surgery. Obstet Gynecol. 2016;127(6):1135–44.
University Health System Consortium Clinical Database/Resource Manager. 2013. Available at: https://www.vizientinc.com/. Accessed 6 April 2016.
American College of Surgery National Surgical Quality Improvement Program SCR Operations Manual. 2016. Available at: http://www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf.
Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, 1999. Am J Infect Control. 1999;27(2):97–134.
Nelson RL, Gladman E, Barbateskovic M. Antimicrobial prophylaxis for colorectal surgery. Cochrane Database Syst Rev. 2014;(5):CD001181.
Veiga DF, Damasceno CA, Veiga-Filho J, et al. Randomized controlled trial of the effectiveness of chlorhexidine showers before elective plastic surgical procedures. Infect Control Hosp Epidemiol. 2009;30(1):77–79.
Bratzler DW, Dellinger EP, Olsen KM, et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Am J Health Syst Pharm. 2013;70(3):195–283.
The University of Texas publically available salary information compiled by the Texas Tribune. 2015. Available at: http://salaries.texastribune.org/the-university-of-texas-md-anderson-cancer-center/departments/gyn-onc-reproductive-med/positions/coord-research-data. Accessed 4 Feb 2016.
Singh A, Bartsch SM, Muder RR, Lee, BY. An economic model: value of antimicrobial-coated sutures to society, hospitals, and third-party payers in preventing abdominal surgical site infections. Infect Control Hosp Epidemiol. 2014;35(8):1013–20.
Gheorghe A, Roberts TE, Pinkney TD, Bartlett DC, Morton D, Calvert M. The cost-effectiveness of wound-edge protection devices compared to standard care in reducing surgical site infection after laparotomy: an economic evaluation alongside the ROSSINI trial. PLoS One. 2014;9(4):e95595.
Anthony T, Murray BW, Sum-Ping JT, et al. Evaluating an evidence-based bundle for preventing surgical site infection: a randomized trial. Arch Surg. 2011;146(3):263–69.
Al-Niaimi AN, Ahmed M, Burish N, et al. Intensive postoperative glucose control reduces the surgical site infection rates in gynecologic oncology patients. Gynecol Oncol. 2015;136(1):71–6.
Acknowledgments
The authors would like to acknowledge the following people for their contributions to this initiative: Katherine E. Cain, PharmD; Lynn M. Cloutier, RN, MSN, ACNP-BC; Shauna L. Fenton, RN, MSN; Linda S. Graviss, MT (ASCP), CIC; Cheryl A. Hubbs, RN; Deepthi A. James, MSN, RN, FNP-C; Johnrich R. Levine, MSN, MHA, MPA, BSN, RN, PNE-C; Keith N. Myers, BS; Anne K. Park, MS, MPH; Deandra Sandles, RN, MSN, CNOR; Tara N. Tatum, RN, MBA; Shital Vachhani, MD; Kathy M. Ware, RN.
Financial Support
This research was supported in part by the National Institutes of Health (NIH) through MD Anderson Cancer Center’s Support Grant CA016672. Dr. Taylor’s work on this project was supported by an NIH T32 grant, Training of Academic Gynecologic Oncologists, from the National Cancer Institute (5T32-CA101642). The funding source had no direct role in preparing or reviewing this study nor this manuscript.
Disclosure
Larissa A. Meyer has received honoraria from TRM Oncology, and research funding from AstraZeneca. Kathleen M. Schemler has received research funding from Cepheid, and patents, royalties or other intellectual property from UpToDate. Jolyn S. Taylor, Claire A. Marten, Mark F. Munsell, Charlotte C. Sun, Kimberly A. Potts, Jennifer K. Burzawa, Alpa M. Nick, Keith Myers, Diane C. Bodurka, Thomas A. Aloia, Charles F. Levenback, David R. Lairson, and Kathleen M. Schmeler report no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Taylor, J.S., Marten, C.A., Munsell, M.F. et al. The DISINFECT Initiative: Decreasing the Incidence of Surgical INFECTions in Gynecologic Oncology. Ann Surg Oncol 24, 362–368 (2017). https://doi.org/10.1245/s10434-016-5517-4
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-016-5517-4