
Abstract
Background
The purpose of this study was to examine the frequency, pattern, and predictive factors associated with occult level II lymph node (LN) metastases in papillary thyroid carcinoma (PTC) patients with clinically metastatic lymph nodes in the lateral neck (level III, IV, and/or V) by preoperative ultrasonography.
Methods
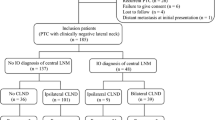
We retrospectively reviewed the medical records of 52 PTC patients with clinically positive neck lymph nodes in level III, IV, and/or V based on preoperative ultrasonography, who underwent therapeutic lateral neck dissection (ND) (level II–V) between March 2004 and October 2009. All patients had no suspicion of clinically positive neck nodes in level II. Histopathological analysis of neck specimens according to each node level of the neck was performed, with special attention given to level II.
Results
Forty-two (81%), 41 (79%), and 6 (12%) patients had histologically positive lymph nodes in level III, IV, and V, respectively. Occult metastases in level II were observed in ten (19%) patients. Patients without suspicious positive LNs in both neck level III and IV by preoperative ultrasonography, and patients without pathologic LN metastases in level III, had no occult LN metastases occurrence to level II. Based on multivariate analysis, presence of more than four metastatic LNs was an independent predictive factor for occult level II metastases [P = 0.022, odds ratio (OR) = 7.738].
Conclusions
Prophylactic level II LN dissection may be omitted in PTC patients with clinically positive neck nodes if suspicious positive lymph nodes in level III are absent during preoperative ultrasonography.
Similar content being viewed by others


References
Shaha AR. Prognostic factors in papillary thyroid carcinoma and implications of large nodal metastasis. Surgery. 2004;135:237–9.
Mazzaferri EL, Jhiang SM. Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am J Med. 1994;97:418–28.
Kupferman ME, Patterson M, Mandel SJ, et al. Patterns of lateral neck metastasis in papillary thyroid carcinoma. Arch Otolaryngol Head Neck Surg. 2004;130:857–60.
Sivanandan R, Soo KC. Pattern of cervical lymph node metastases from papillary carcinoma of the thyroid. Br J Surg. 2001;88:1241–4.
Machens A, Hinze R, Thomusch O, Dralle H. Pattern of nodal metastasis for primary and reoperative thyroid cancer. World J Surg. 2002;26:22–8.
Shaha AR. Management of the neck in thyroid cancer. Otolaryngol Clin North Am. 1998;31:823–31.
Bhattacharyya N. Surgical treatment of cervical nodal metastases in patients with papillary thyroid carcinoma. Arch Otolaryngol Head Neck Surg. 2003;129:1101–4.
Shaha AR, Shar JP, Loree TR. Patterns of nodal and distant metastasis based on histologic varieties in differentiated carcinoma of the thyroid. Am J Surg. 1996;172:692–4.
Shah MD, Hall FT, Eski SJ, Witterick IJ, Walfish PG, Freeman JL. Clinical course of thyroid carcinoma after neck dissection. Laryngoscope. 2003;113:2102–7.
Caron NR, Tan YY, Ogilvie JB, Triponez OF, Reiff ES, Kebebew RE, et al. Selective modified radical neck dissection for papillary thyroid cancer-Is level I, II and V dissection always necessary? World J Surg. 2006;30:833–40.
Terrell JE, Welsh DE, Bradford CR, Chepeha DB, Esclamado RM, Hoqikyan ND, et al. Pain, quality of life, and spinal accessory nerve status after neck dissection. Laryngoscope. 2000;110:620–6.
Shah JP. Pattern of cervical lymph node metastasis from squamous carcinomas of the upper aerodigestive tract. Am J Surg. 1990;160:405–9.
Ito Y, Tomoda C, Uruno T, et al. Preoperative ultrasonographic examination for lymph node metastasis: usefulness when designing lymph node detection for papillary microcarcinoma of the thyroid. World J Surg. 2004;28:498–501.
González HE, Cruz F, O’Brien A, et al. Impact of preoperative ultrasonographic staging of the neck in papillary thyroid carcinoma. Arch Otolaryngol Head Neck Surg. 2007;133:1258–62.
Stulak JM, Grant CS, Farley DR, et al. Value of preoperative ultrasonography in the surgical management of initial and reoperative papillary thyroid cancer. Arch Surg. 2006;141:489–94.
Roh JL, Park JY, Kim JM, Song CJ. Use of preoperative ultrasonography as guidance for neck dissection in patients with papillary thyroid carcinoma. J Surg Oncol. 2009;99:28–31.
Wada N, Duh QY, Sugino K, et al. Lymph node metastasis from 259 papillary thyroid microcarcinoma: frequency, pattern of occurrence and recurrence, and optimal strategy for neck dissection. Ann Surg. 2003;237:399–407.
Turanli S. Is the type of dissection in lateral neck metastasis for differentiated thyroid carcinoma important? Otolaryngol Head Neck Surg. 2007;136:957–60.
Cheng PT, Hao SP, Lin YH, et al. Objective comparison of shoulder dysfunction after three neck dissection techniques. Ann Otol Rhinol Laryngol. 2000;109:761–6.
Inoue H, Nibu K, Saito M, Otsuki N, Ishida H, Onitsuka T, et al. Quality of life after neck dissection. Arch Otolaryngol Head Neck Surg. 2006;132:662–6.
Acknowledgment
This work was supported by Konkuk University.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Koo, B.S., Seo, ST., Lee, GH. et al. Prophylactic Lymphadenectomy of Neck Level II in Clinically Node-Positive Papillary Thyroid Carcinoma. Ann Surg Oncol 17, 1637–1641 (2010). https://doi.org/10.1245/s10434-010-0958-7
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-010-0958-7