
Abstract
Two main factors have been implicated in the mechanism underlying the pathogenesis of acquired aplastic anemia: environmental factors and genetic susceptibility. Individuals vary in their ability to metabolize several DNA-damaging agents due to polymorphisms of biotransforming enzymes. Genetically determined differences in the expression of these enzymes could explain interindividual risks in developing acquired aplastic anemia. The aim of the study was to characterize the genetic polymorphism of biotransforming phase I (p450-cyp2E1) and phase II [microsomal epoxide hydrolase (mEh), glutathione S-transferase (GST)] enzymes in pediatric patients with acquired aplastic anemia. The GSTT1 null genotype (absence of both alleles) was associated with a significantly increased risk for acquired aplastic anemia (odds ratio, 2.8; 95% confidence interval, 0.15–5.7). In contrast, the GSTM1 null genotype or polymorphisms within the p450-cyp2E1 and mEh genes was not significantly different in patients and controls. Multivariate analysis was performed to assess whether the enzymes together or with other variables as age, gender, or response to therapy may have any significant association with the tested genotypes. In no combinations of the mentioned parameters was an association found with acquired aplastic anemia. GST are mainly involved in metabolizing hematotoxic and mutagenic substrates such as benzene derivatives. The GSTT1 null genotype may modulate the metabolism of exogenous pollutants or toxic intermediates. The absence of the GSTT1 enzyme, leading to genetic susceptibility toward certain pollutants, might determine the individual risk for development of acquired aplastic anemia in children.
Similar content being viewed by others

Main
The common feature of AA is an empty bone marrow and pancytopenia in the peripheral blood (1, 2). Although the causes for aplastic anemia are multiple, with the majority of cases remaining idiopathic, the pathogenic mechanism leading to the disease might be limited to two main pathways: environmental factors (3, 4) and genetic susceptibility (5, 6). Environmental factors include viral infections (7, 8), exposure to radiation (9), drugs (10), and chemicals (11–13). They may cause DNA damage on the level of the hematopoietic progenitors (14) or lead to an activation of autologous immunologic mechanism (15), also resulting in damage on the level of the hematopoietic progenitors (16–18). However, a history of a massive exposure to environmental pollutants will rarely be described in the history of a Caucasian child suffering from AA. Individuals vary in their ability to metabolize several DNA-damaging agents because of polymorphism of detoxifying enzymes. Variability in the expression or efficiency of these enzymes could explain interindividual risks for development of aplastic anemia in the presence of the above-mentioned environmental agents. Three of the most important biotransforming enzymes, CYP isoenzymes, mEh, and GST, show genetic polymorphisms. p450-cyp2E1 metabolizes a wide variety of drugs and chemicals, with preference for small molecules such as aldehydes, ketones, alcohols, and aromatic compounds (19). A number of polymorphisms have been described in the p450-cyp2E1 gene (20), with the Pst I/ Rsa I polymorphism in the 5′ flanking region being best defined (21). The C2/C2 variant leads to an enhanced transcription of the (C2) p450-cyp2E1 gene, which increases enzyme activity compared with the C1/C1 variant (21).
Among the phase II enzymes, mEh is involved in the first-pass metabolism of highly reactive epoxide intermediates and oxygen radicals. Two polymorphisms of mEH with a broad substrate spectrum (22, 23) have been found to be associated with susceptibility for several malignant diseases (24–26). The exon 3 point mutation T to C results in a tyrosine to histidine shift at position 113 (His 113), with a 50% reduced enzyme activity (slow allele), and the A to G transition leading to a histidine to arginine shift at position 139 (Arg 139), with a 25% faster enzyme activity (fast allele) (27, 28).
GST represent a group of xenobiotic detoxifying enzymes (29, 30), with GSTM (31–34), -T (35, 36), and -P (37) being polymorphs. A null genotype is characterized by the absence of the respective GST protein (38). The GSTM1 null genotype has been shown to be associated with an increased risk of smoke-induced cancers (39–41), breast cancers (42), and hepatocellular carcinoma (43, 44). The GSTT1 null genotype has been shown to be associated with an increased risk for MDS (44–46). However, further studies on MDS have revealed conflicting results (44, 47–49).
In this study, we analyzed three different enzymes in pediatric AA patients. p450-cyp2E1, mEh, and GST (M1 and T1) were chosen with regard to their substrate specificity, including hematotoxic and mutagenic DNA/damaging agents as aromatic compounds, radicals, and reactive oxygen.
PATIENTS AND METHODS
Patients.
The majority of patients suffering from AA were recruited between 1996 and 1999 through the pediatric cooperative multicenter study SAA-94, involving 37 centers in Germany and Austria. Some were tested independently from the study, as their diagnosis was before the beginning of the study. The diagnosis for AA was performed following the Camitta criteria and confirmed by bone marrow biopsy. Most of the patients suffered from VSAA (polymorphonuclear cells <200/μL) or SAA (polymorphonuclear cells <500/μL). Three patients had marked chromosomal abnormalities (+19, −7, +8) without morphologic signs of acute myeloid leukemia (AML) or MDS. Patients were ineligible if they showed clinical signs of paroxysmal nocturnal hematuria, Fanconi anemia, MDS, or congenital bone marrow failure disorders, or had undergone radiation, chemotherapy, or pretreatment with antilymphocyte globulin, cyclosporine A, or granulocyte colony-stimulating factor. The patients' ages ranged between 1 and 16 y, with a median age of 9.6 y; 38 girls and 53 boys were analyzed. Details concerning the patients of the SAA-94 study, the treatment, and results are described by Fuhrer et al.(50). The research protocol was approved by the ethics committee of the Ludwig-Maximilians University, Munich, and the Heinrich Heine University, Duesseldorf. Nonrandom controls were obtained from pediatric stem cell donors: four were siblings of patients suffering from solid tumors (one neuroblastoma, two non-Hodgkin's lymphoma, and one Hodgkin's lymphoma), four were siblings of patients suffering from X-linked severe combined immunodeficiency, one was a sibling of a patient suffering from adrenoleukodystropy, and six were siblings of patients diagnosed for relapsed acute leukemia. There was no increased incidence of cancer in the medical history of the families. The other donors were healthy Caucasian volunteers, whose samples were obtained from the blood bank. As all results obtained from controls' samples fit perfectly to the results from larger patient collectives, we believe that they are representative. The study has been approved by the ethics committee of the University of Munich as part of the SAA-94 study and by the ethics committee of the Heinrich Heine University, Duesseldorf. Informed consent was signed by the parents or the patients.
DNA isolation.
DNA was prepared from whole blood or bone marrow specimens using the DNAeasy kit (QIAGEN, Hilden, Germany).
p450-cyp2E1 polymorphism.
p450-cyp2E1 alleles were determined in 91 AA patients and 235 controls by their melting curve differences in a light cycler (Roche Molecular Biochemicals, Mannheim, Germany). Some controls were analyzed parallel to patients' samples. Other control data were established in the same laboratory by the same method in a separate research project. Approximately 100 ng of genomic DNA were used for each PCR reaction. The following primers were used: forward primer: 5′ CCCGTGAGCCAGTCGAGT 3′; reverse primer: 5′ CAGACCCTCTTCCACCTTCTAT 3′ (5 μM each); Rsa I sensor: 5′ CATAAAGATTCATTGTTAATATAAAAGTACAAAATTX 3′ (1.5 μM); Rsa anchor: 5′-LCRes 540 CAACCTATGAATTAAGAACTTATATATATTGCCAG ph-3′ (1.5 μM). The PCR reaction contained 1 μL of DNA, 1 μL of each primer, 1.2 μL 25 mM MgCl2, 1 μL of the manufacturer's PCR mix [including Taq polymerase and nucleoside 5′-triphosphate (NTP); Roche Molecular Biochemicals]. PCR was performed in 35 cycles at 45°C and 72°C and the melting curves were generated by the equipment.
mEh polymorphisms.
The two distinct mEh polymorphisms were analyzed in 75 patients and 96 controls by the PCR/restriction length polymorphism (RFLP) technique. Due to technical problems and, thus, high consumption of DNA, not all 91 probes could be analyzed. For amplification of the polymorphic exon 3, 1 μM of the primers 5′ CCTTGTGCTCTGTCCTTCCCATCCC and 3′ AATCCTAGTCTTGAAGTGACGGT +, 0.15 μM dNTP, 0.15 μM Taq polymerase, 1 mM 10× buffer, and 5 μL Q - solution (QIAGEN) were added to 2.5 μM DNA. Thirty-five PCR cycles were run for 10 s at 94°C, 30 s at 45°C, and 45 s at 72°C. The PCR products were digested with Asp I for 1 h at 37°C. A restriction enzyme site is present in the wild type only, giving a 209-bp fragment, whereas the mutant is not digested and shows 231-bp band. The exon 4 polymorphism site was amplified with 5′ GGGGTGCCAGAGCCTGACCGT and 3′ AACACGGGGCCCACCCTTGGC as described and digested with Rsa I for 1 h at 37°C. The enzyme cuts the mutant allele, giving a 174-bp fragment, whereas the wild type shows a larger 295-bp band. The characteristic restriction products for exon 3 and exon 4 polymorphisms are depicted in Figure 1.

Genotype analysis of mEh. Exon 3 (left panel): (a) fragment patterns expected in individuals homozygous or heterozygous for mEh polymorphism. The restriction digest using Asp I reveals 209-bp and 20-bp fragments in homozygous wild-type individuals and a 231-bp fragment in homozygous mutant individuals. Heterozygous individuals display all bands. (b) Typical electrophoresis gel showing the mEh-specific DNA fragments. Only the relevant 231- and 209-bp fragments are shown. Exon 4 (right panel): (a) fragment patterns expected in individuals homozygous or heterozygous for mEh polymorphism. The restriction digestion using Rsa I reveals a 295-bp fragment in homozygous wild-type individuals and 174-bp and 62-bp fragments in homozygous mutant individuals. Heterozygous individuals display all bands. (b) Typical electrophoresis gel envisioning the mEH-specific DNA fragments. Only the relevant 295- and 174-bp fragments are shown.
GSTM1 and GSTT1 polymorphisms.
To analyze the polymorphism of GSTM1 and -T1 genes, we developed a multiplex PCR detecting GSTM1 and -T1 as well as an internal β-globin control in a one-tube reaction. Samples from 78 patients and 122 controls were analyzed. Due to technical problems and high consumption of DNA, only 78 of 91 probes were analyzed. Briefly, GSTM1 was amplified using primers corresponding to the 3′-coding region of the human GST: 5′ GAACTCCCTGAAAAGCTAAAG and 5′ GTTGGGAAATATACGGTG. Primers coding for the human GSTT1 were 5′ TTCCTTACTGGTCCTCACATCTC and 5′ TCACCGGATCATGGCCAGCA. The housekeeping gene β-globin was amplified using the primers 5′ CAACTTCATCCACGTTCACC and 5′ GAAGAGCCAAGGACAGGTAC. The PCR reaction was carried out by heating to 94°C for 4 min, followed by 34 cycles of 1 min at 94°C, 60°C, and 72°C. A final run at 72°C for 7 min was included. To exclude systematic errors, 14 samples were analyzed repetitively. An example is given in Figure 2.

Genotype analysis of GSTM1 and GSTT1. The frequency of GSTT1 and GSTM1 null genotype was analyzed in pediatric patients with AA and in healthy controls. The results of a multiplex PCR amplifying GSTM1, GSTT1 and the β-globin housekeeping gene in a one-tube reaction are shown. The 270-bp lane shows the β-globin control, the ??-bp lane the GSTT1 gene, and the ??-bp lane the GSTM1 gene. Lane 1 shows the DNA size-standard; in lane 2, the β-globin product and the GSTM1 gene is shown (GSTT1 could not be detected). In lane 3, only β-globin was detected and both GSTT1 and GSTM1 were lacking. In lane 4, the β-globin and GSTT1 gene are shown, and GSTM1 is absent. In lane 5, both analyzed GST genes are detected.
Sensitivity of the PCR reaction was 8.6 ng/μL DNA, as tested by stepwise dilution of GSTT1- and GSTM1-positive DNA. The PCR reaction was performed in the presence of 1 ng β-globin DNA as a standard control.
Statistics.
Statistical analyses were performed using SPSS statistical software (version 7.5, SPSS Inc., Chicago, IL, U.S.A.). Significance was measured by Fisher's exact test (two-tailed), χ2 test (two-tailed), and the Bonferoni method. Odds ratios (OR) were calculated and given within the 95% confidence interval (CI). Unconditional multivariate analysis was performed separately for each genotype. Age, gender, severity of acquired aplastic anemia, and therapeutic response were analyzed as co-variables for each locus and in combinations. Statistical analyses were performed with the help of the Institute for Statistics at the Heinrich Heine University, Duesseldorf.
RESULTS
p450-cyp2E1 polymorphism.
The frequency of the p450-cyp2E1 alleles is given in Table 1. The prevalence for homozygosity of the rarer C2 was comparable in AA, with 0 of 91 (0%) analyzed samples and 1 of 235 (0.4%) controls with (OR, 1.6; 95% CI, 0.7–4.1; p > 0.28; NS). Heterozygous C1/C2 were found in 8 of 91 (9%) patients with AA and 12 of 235 (5.1%) controls (NS). The wild-type C1/C1 alleles were comparable in 83 of 91 (91%) patients with AA and 222 of 235 (94.5%) controls (NS). The respective prevalence in healthy controls was comparable to data from other studies that analyzed Caucasian patients (20, 21, 43). These data exhibit no association of p450-cyp2E1 polymorphism with a risk for AA in children.
mEH polymorphism.
The frequency of mEh polymorphism is given in Table 2. The prevalence of the respective alleles in our controls was comparable to other studies (49). Forty-one of 75 (55%) patients showed the tyrosine (Tyr) 113 polymorphism in exon 3 and 52 of 96 controls (53%) showed the Tyr 113 polymorphism in exon 3 (NS). The slow allele [histidine (His) 113] variant of exon 3 was found in 15 of 75 (20%) patient samples and in 15 of 96 (16%) control samples (NS). The slow allele (His 139) variant of exon 4 was found in 47 of 75 (63%) patient samples and in 65 of 96 (68%) control samples. The fast allele [arginine (Arg) 139] of exon 4 was found in 4 of 75 (5%) patient samples and in 2 of 96 (2%) control samples (NS). The respective prevalence for each analyzed allele in healthy controls was comparable to data from other studies that analyzed Caucasian patients (45, 49, 51). Transfer of the genotypes into putative phenotypes revealed no significant difference between the two alleles (Table 3).
GST polymorphism.
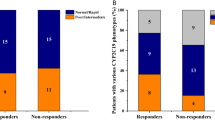
The frequencies of GSTT1 and GSTM1 alleles for all patients and their respective controls are given in Table 4. The incidence of GSTT1 was significantly increased in AA cases compared with controls. Among the patients, 34 of 78 (39%) children were negative for the GSTT1 gene compared with 24 of 122 (20%) controls. We found a significantly increased risk for AA in children with a GSTT1 null genotype (OR, 2.8, 95% CI, 1.5–5.7; p < 0.004).
The GSTM1 null genotype occurred in 34 of 78 (44%) patients and in 66 of 122 (54%) controls (NS). The GSTM1 null genotype was not associated with an increased risk for AA. Nine of 78 patients (12%) and 3 of 122 controls (8%) were found to be negative for both GST alleles (NS). The prevalence in healthy controls was comparable to data from other studies that analyzed Caucasian patients.
Interaction among the genetic polymorphisms.
To assess the combined effects of these polymorphisms, interactions between the GSTT1 null genotype and the other polymorphisms were analyzed by multivariate analysis. This analysis did not show a significant increase in the risk for developing AA for either of the tested interactions with the GSTT1 null genotype (data not shown).
Variables such as age or gender, the phenotype of the aplastic anemia (NSAA, SAA, and VSAA), response to immunosuppressive therapy, frequency of relapse, duration of the disease (data not shown), and development of a malignant disease (data not shown) were tested for correlation with either of the analyzed genotypes. However, none of these parameters showed a significant correlation.
DISCUSSION
Immunologic mechanisms and/or oxidative DNA damage are widespread means of induction in the pathogenesis of AA (41). Bone marrow protection from xenobiotics depends on an intact detoxification pathway. Individual differences in expression of biotransforming enzymes may lead to susceptibility to toxic agents. We analyzed genetic polymorphisms of biotransforming enzymes and correlated the data with the risk for AA. We found a significantly higher frequency of the GSTT1 null genotype among children with AA, whereas p450-cyp2E1, mEh, and GSTM1 were not correlated. However, the statistics show that GST may play a secondary role in the pathogenesis of AA in childhood. Viewing the literature, many factors have been associated with aplastic anemia, and the GSTT1 null genotype may be one risk factor among others. GSTT1 determines the ability to conjugate reactive components (44) such as monohalomethanes (52) and ethylene oxide (53, 54) and metabolism of low-molecular-weight-halogenated xenobiotics or reactive epoxides. GSTT1 is expressed in erythrocytes and lymphocytes (51, 52) and hence acts in the hematopoietic system. The importance of GSTT1 in the protection of hematopoietic cells from environmental pollutants has been proven in a population exposed to 1,3-butadiene—the in vitro sister chromatid exchange in human lymphocytes in the presence of 1,3-butadiene was 16-fold higher in cells from individuals lacking the GSTT1 gene expression (55, 56). With regard to benzene detoxification, which is highly important in context with AA, GSTT1 is a major protection factor of individual susceptibility to benzene-induced chromosomal damage (51) and induces the urinary excretion of benzene metabolites with higher excretion of t,tMA (57).
Proving a direct causative coincidence between exogenous pollutants and marrow failure is difficult because the onset of marrow failure cannot be dated accurately. The delay in marrow disease after exposure to pollutants may be variable, and individuals with a genetic susceptibility due to an enzyme deficiency may be at greater risk than individuals with normal enzyme levels in the presence of environmental factors, even at low exposures. The GSTT1 null genotype may modulate the metabolism of exogenous pollutants or endogenous DNA-damaging processes. A genetic susceptibility toward certain pollutants might determine the individual risk against common levels of mutagenic pollutants.
Abbreviations
- AA:
-
acquired aplastic anemia
- CYP:
-
cytochrome p450
- GST:
-
glutathione S-transferase
- MDS:
-
myelodysplastic syndrome
- mEh:
-
microsomal epoxide hydrolase
- NSAA:
-
non-severe aplastic anemia
- SAA:
-
severe aplastic anemia
- VSAA:
-
very severe aplastic anemia
References
Alter BP, Young NS 1993 The bone marrow failure syndromes. In: Nathan DG, Oski FA (eds) Hematology of Infancy and Childhood. WB Saunders, Philadelphia, 100–132.
Young NS 1999 Acquired aplastic anemia. JAMA 282: 271–278
Sharpe WD 1993 Benzene, artificial leather and aplastic anemia: Newark, 1916–1928. Bull NY Acad Med 69: 47–60
Young N 1988 Drugs and chemicals as agents of bone marrow failure. In: Testa N, Gale RP (eds) Hematopoiesis. Marcel Dekker, New York, 131–159.
Morley A, Trainor K, Seshradi R, Sorelli J 1978 Is aplastic anemia due to abnormality of DNA?. Lancet 48: 9–11
Turner DR, Morley AA, Seshardi RS 1981 Lymphocyte DNA in aplastic anemia. Br J Haematol 48: 207–215
Young NS Mortimer 1993 Viruses and bone marrow failure. Blood 63: 75–80
Dilloo D, Josting A, Göbel U 1991 CMV-associated bone marrow suppression: the role of CMV infection in modulation of interleukin-6 production in vitro. Eur J Pediatr 150: 716–721
Fliedner TM, Nothdurft W, Calvo W 1986 The development of radiation late effects to the bone marrow after single and chronic exposure. Int J Radiat Biol 49: 35–46
Nagao T, Maurer AM 1969 Concordance for drug induced aplastic anemia in identical twins. N Engl J Med 218: 7–11
Snyder R, Witz G, Goldstein BD 1993 The toxicology of benzene. Environ Health Perspect 100: 172–181
Sanchez-Medal L, Castanedo JP, Garcia-Rodas F 1963 Insecticides and aplastic anemia. N Engl J Med 269: 1365–1370
Fleming LE, Timmeny W 1993 Aplastic anemia and pesticides. An etiologic association?. J Occup Med 35: 1106–1116
Maciejewski JP, Hibbs JR, Anderson S, Katevas P, Young NS 1994 Bone marrow and peripheral blood lymphocyte phenotype in patients with bone marrow failure. Exp Hematol 22: 1102–1110
Frickhofen N, Liu JM, Young NS 1990 Etiologic mechanisms of hematopoietic failure. Am J Pediatr Hematol Oncol 12: 385–395
Torok-Storb B 1990 Etiological mechanisms in immune-mediated aplastic anemia. Am J Pediatr Hematol Oncol 12: 396–401
Mentzel U, Vogt H, Rossol R, Geissler RG, Maurer A, Ganser A, Trommer WE, Hoelzer D 1993 Analysis of lymphocyte subsets in patients with aplastic anemia before and during immunosuppressive therapy. Ann Hematol 66: 127–129
Marsh JCW, Chang J, Testa NG, Hows JM, Dexter TM 1991 In vitro assessment of marrow stem cell and stromal cell function in aplastic anemia. Br J Haematol 78: 258–267
Lieber CS 1997 Cytochrome p-4502E1, its physiological and pathological role. Physiol Rev 77: 517–544
Uematsu F, Kikuchi H, Ohmachi T, Sagami I, Motomiya M, Kamataki T, Komori M, Watanabe M 1991 Two common RFLPs of the human CYP2E1 gene. Nucleic Acids Res 19: 2803
Watanabe J, Hayashi S-i, Nakachi K, Imai K, Suda Y, Sekine T, Kawajiri K 1990 Pst and Rsa I RFLPs in complete linkage disequilibrium at the CYP2E gene. Nucleic Acids Res 18: 7194
Omiecinski CJ, Hassett C, Hosagrahara V 2000 Epoxide hydrolase—polymorphism and role in toxicology. Toxicol Lett 112–113: 365–370
Seidegard J, De Pierre JW, Guenther TM, Oesch F 1986 The effects of metyrapone, chalcone epoxide, benzol, clotrimazol and related compounds on the activity of microsomal epoxide hydrolase in situ, in purified form and in reconstituted systems toward different substrates. Eur J Biochem 159: 415–423
Snyder R, Chepiga T, Yang CS, Thomas H, Platt K, Oesch F 1993 Benzene metabolism by reconstituted cytochromes p450 2B1 and 2e1 and its modulation by cytochrome b5, microsomal epoxide hydrolase, and glutathione transferases: evidence for an important role of microsomal epoxide hydrolase in the formation of hydroquinone. Toxicol Appl Pharmacol 122: 172–181
Lancester JM, Brownlee HA, Bell DA, Futreal PA, Marks JR, Berchut A, Wiseman RW, Taylor JA 1996 Microsomal epoxide hydrolase polymorphism as a risk factor for ovarian cancer. Mol Carcinog 17: 160–162
McGlynn KA, Rosvold EA, Lustbader ED, Hu Y, Clapper ML, Zhou T, Wild CP, Xia XL, Baffoe Bonnie A, Ofori Adjei D 1995 Susceptibility to hepatocarcinoma is associated with genetic variability in the enzymatic detoxification of aflatoxin B1. Proc Natl Acad Sci USA 92: 2384–2387
Hassett C, Aicher L, Sidhu JS, Omiencinski CJ 1994 A human microsomal epoxide hydrolase: genetic polymorphism and functional expression in vitro of amino acid variants. Hum Mol Genet 3: 421–428
Hassett C, Robinson KB, Beck NB, Omienski CJ 1994 The human microsomal epoxide hydrolase gene (EPHXI): complete nucleotide sequence and structural characterization. Genomics 23: 433–442
Smith CAD, Harrison DJ 1997 Association between polymorphism in gene for microsomal epoxide hydrolase and susceptibility to emphysema. Lancet 350: 630–633
Pickett CB, Lu AYH 1988 The structure, genetics and regulation of soluble glutathione s-transferases. In: Sies H, Ketterer B (eds) Glutathione Conjugation: Its Mechanisms and Biological Significance. Academic Press, San Diego, 137–145.
Board P, Coggan M, Johnston P, Ross V, Suzuki T, Webb G 1990 Genetic heterogeneity of the human glutathione transferases: a complex of gene families. Pharmacol Ther 48: 357–364
Mannervik B, Alin P, Guthenberg C, Jensson H, Tahir MK, Warholm M, Jörnvall H 1985 Identification of three classes of cytosolic glutathione transferases common to several mammalian species: correlation between structural data and enzymatic properties. Proc Natl Acad Sci USA 82: 7202–7206
Islam MQ, Platz A, Szpirer J, Szpirer C, Levan G, Mannervik B 1989 Chromosomal localisation of human glutathione transferases genes of classes α, μ, φ. Hum Genet 82: 338–345
Brockmoller J, Kerb R, Drakoulis N, Nitz M, Roots I 1993 Genotype and phenotype of glutathione S-transferase class mu isoenzymes mu and psi in lung cancer patients and controls. Cancer Res 53: 1004–1011
Mannervik B, Awasthi YC, Board PG, Hayes JD, Di Ilio C, Ketterer B, Listowsky I, Morgenstern R, Muramatsu M, Pearson WR, Pickett CB, Widersten M, Wolf CR 1992 Nomenclature for human glutathione transferases. Biochem J 282: 305–306
Schroder KR, Hallier E, Meyer DJ, Wiebel FA, Muller AM, Bolt HM 1996 Purification and characterization of a new glutathione S-transferase, class theta, from human erythrocytes. Arch Toxicol 70: 559–566
Harries LW, Stubbins MJ, Forman D, Howard GC, Wolf CR 1997 Identification of genetic polymorphisms at the glutathione S-transferase Pi locus and association with susceptibility to bladder, testicular and prostate cancer. Carcinogenesis 18: 641–644
Pemble SE, Wardle AF, Taylor JB 1996 Glutathione S-transferase class Kappa: characterization by the cloning of rat mitochondrial GST and identification of a human homologue. Biochem J 319: 749–754
Okkels H, Sigsgaard T, Wolf H, Autrup H 1996 Glutathione S-transferase mu as a risk factor in bladder tumours. Pharmacogenetics 6: 251–256
Nakajima T, Elovaara E, Anttila S, Hirvonen A, Camus AM, Hayes JD, Ketterer B, Vainio H 1995 Expression and polymorphism of glutathione S-transferase in human lungs: risk factors in smoking-related lung cancer. Carcinogenesis 16: 707–711
Nakachi K, Imai K, Hayashi S, Kawajiri K 1993 Polymorphisms of the CYP1A1 and glutathione S-transferase genes associated with susceptibility to lung cancer in relation to cigarette dose in a Japanese population. Cancer Res 53: 2994–2999
Ambrosone CB, Freudenheim JL, Graham S, Marshall JR, Vena JE, Brasure JR, Laughlin R, Nemoto T, Michalek AM, Harrington A 1995 Cytochrome P4501A1 and glutathione S-transferase (M1) genetic polymorphisms and postmenopausal breast cancer risk. Cancer Res 55: 3483–3485
Murray GI, Paterson PJ, Weaver RJ, Ewen SW, Melvin WT, Burke MD 1993 The expression of cytochrome P-450, epoxide hydrolase, and glutathione S-transferase in hepatocellular carcinoma. Cancer 71: 36–43
Rollinson S, Roddam P, Kane E, Roman E, Cartwright R, Jack A, Morgan GJ 2000 Polymorphic variation within the glutathione S-transferase genes and risk of adult acute leukaemia. Carcinogenesis 21: 43–47
Chen H, Sandler DP, Taylor JA, Shore DL, Liu E, Bloomfield CD, Bell DA 1996 Increased risk for myelodysplastic syndromes in individuals with glutathione transferase theta 1 (GSTT1) gene defect. Lancet 347: 295–297
Sasai Y, Horiike S, Misawa S, Kaneko H, Kobayashi M, Fujii K Kashima, Tanuwaki M 1999 Genotype of glutathione S-transferase and other genetic configurations in myelodysplasia. Leuk Res 23: 975–981
Basu T, Gale RE, Langabeer S, Linch D 1997 Glutathion, S-transferase theta (GSTT) gene defect in myelodysplasia and acute myeloid leucemia. Lancet 349: 1450
Preudhomme C, Nisse C, Hebbar M, Vanrumbeke M, Brizard A, Lai JL 1997 Glutathione s transferase theta gene defects in myelodysplastic syndrome and their correlation with karyotype and exposure to potential carcinogens. Leukemia 11: 1580–1582
Okada M, Okamoto T, Wada H, Tademoto Y, Kakishita E 1997 Glutathione S transferase theta gene (GSTT1) defect in Japanese patients with myelodysplastic syndromes. Int J Hematol 66: 393–395
Fuhrer M, Burdach S, Ebell W, Gadner H, Haas R, Harbott J, Janka-Schaub G, Klingebiel T, Kremens B, Niemeyer C, Rampf U, Reiter A, Ritter J, Schulz A, Walther U, Zeidler C, Bender-Gotze C 1998 Relapse and clonal disease in children with aplastic anemia (AA) after immunosuppressive therapy (IST): the SAA 94 experience. German/Austrian Aplastic Anemia Working Group. Klin Pädiatr 210: 173–179
Xu X, Wiencke JK, Niu T, Wang M, Watanabe H, Kelsey KT, Christiani DC 1998 Benzene exposure, glutathione S-transferase theta homozygous deletion, and sister chromatid exchanges. Am J Ind Med 33: 157–163
Hayes JD, Pulford DJ 1995 The glutathione S-transferase supergene family: regulation of GST and the contribution of the isoenzymes to cancer chemoprotection and drug resistance. Crit Rev Biochem Mol Biol 30: 445–600
Ploemen JH, Van Schanke A, Van Ommen B, Van Bladeren PJ 1994 Reversible conjugation of ethacrynic acid with glutathione and human glutathione S-transferase P1–1. Cancer Res 54: 915–919
Hallier E, Langhof T, Danappel D, Leutbecher M, Schroeder K, Goergens HW, Muller A, Bolt M 1993 Polymorphism of glutathione conjugation of methyl bromide ethylene oxide and dichloromethane in human blood influence on the induction of sister chromatid exchange (SCE) in lymphocytes. Arch Toxicol 67: 173–178
Bernadini S, Pelin K, Peltonen K, Jarventaus H, Hirvonen A, Neagu C, Sorsa M, Norppa H 1996 Induction of sister chromatid exchange by 3,4-epoxybutane-1,2-diol in cultured human lymphocytes of different GSTT1 and GSTM1 genotypes. Mutat Res 361: 121
Norppa H, Javentaus H, Uuskula M, Tasa G, Ojajarvi A, Sorsa M 1995 Role of GSTT1 and GSTM1 genotypes in determining individual sensitivity to sister chromatid exchange induction by diepoxybutane in cultured human lymphocytes. Carcinogenesis 16: 1261–1264
Rossi AM, Guarnier C, Rovesti S, Gobba E, Ghittori S, Vivoli G, Barale R 1999 Genetic polymorphism influence variability in benzene metabolism in humans. Pharmacogenetics 9: 445–458
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported by the Deutsche Forschungsgemeinschaft Sonderforschungsbereich (503), the Bundesministerium für Bildung, Wissenschaft und Technologie (BMBF) Germany BEO BioRegio 311661, the Dr. Mildred Scheel Stiftung der Deutschen Krebshilfe, and the Elterninitiative Kinderkrebsklinik Düsseldorf e.V. C.M. was a recipient of a “Deutscher Akademischer Austauschdienst” DAAD grant in 1999 at the Department of Pediatric Hematology and Oncology, Düsseldorf, Germany.
Rights and permissions
About this article
Cite this article
Dirksen, U., Moghadam, K., Mambetova, C. et al. Glutathione S Transferase Theta 1 Gene (GSTT1) Null Genotype Is Associated with an Increased Risk for Acquired Aplastic Anemia in Children. Pediatr Res 55, 466–471 (2004). https://doi.org/10.1203/01.PDR.0000111201.56182.FE
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/01.PDR.0000111201.56182.FE
This article is cited by
-
A hPSC-based platform to discover gene-environment interactions that impact human β-cell and dopamine neuron survival
Nature Communications (2018)
-
Association of GSTM1 and GSTT1 deletion polymorphisms with Pakistani aplastic anemia patients and controls and meta-analysis
Annals of Hematology (2015)
-
Glutathione S-transferase gene deletions and their effect on iron status in HbE/β thalassemia patients
Annals of Hematology (2010)
-
Reconstructing population exposures to environmental chemicals from biomarkers: Challenges and opportunities
Journal of Exposure Science & Environmental Epidemiology (2009)
-
Work of Breathing During Nasal Continuous Positive Airway Pressure in Preterm Infants: A Comparison of Bubble vs Variable-Flow Devices
Journal of Perinatology (2005)
