
Abstract
Objective
To develop a model to identify women at very low risk of recurrent early-onset preeclampsia.
Methods
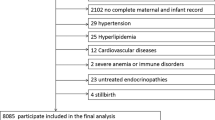
We enrolled 407 women who had experienced early-onset preeclampsia in their first pregnancy, resulting in a delivery before 34 weeks’ gestation. Preeclampsia was defined as hypertension (systolic blood pressure ≥140 mm Hg and/or diastolic blood pressure ≥90 mm Hg) after 20 weeks’ gestation with de novo proteinuria (≥300 mg urinary protein excretion/day). Based on the previous published evidence and expert opinion, 5 predictors (gestational age at previous birth, prior small-for-gestational-age newborn, fasting blood glucose, body mass index, and hypertension) were entered in a logistic regression model. Discrimination and calibration were evaluated after adjusting for overfitting by bootstrapping techniques.
Results
Early-onset disease recurred in 28 (6.9%) of 407 women. The area under the receiver operating characteristic (ROC) curve of the model was 0.65 (95% CI: 0.56-0.74). Calibration was good, indicated by a nonsignificant Hosmer-Lemeshow test (P = .11). Using a predicted absolute risk threshold of, for example, 4.6% (ie, women identified with an estimated risk either above or below 4.6%), the sensitivity was 100%, with a specificity of 26%. In such a strategy, no women who developed preeclampsia were missed, while 98 of the 407 women would be regarded as low risk of recurrent early-onset preeclampsia, not necessarily requiring intensified antenatal care.
Conclusion
Our model may be helpful in the identification of women at very low risk of recurrent early-onset preeclampsia. Before widespread application, our model should be validated in other populations.
Similar content being viewed by others

References
Hernandez-Diaz S, Toh S, Cnattingius S. Risk of pre-eclampsia in first and subsequent pregnancies: prospective cohort study. BMJ. 2009;338:b2255. doi: 10.1136/bmj.b2255.
Hauth JC, Ewell MG, Levine RJ, et al. Pregnancy outcomes in healthy nulliparas who developed hypertension. Calcium for Preeclampsia Prevention Study Group. Obstet Gynecol. 2000;95(1):24–28.
Vatten LJ, Skjaerven R. Is pre-eclampsia more than one disease? BJOG. 2004;111(4):298–302.
Witlin AG, Sibai BM. Magnesium sulfate therapy in preeclampsia and eclampsia. Obstet Gynecol. 1998;92(5):883–889.
Khan KS, Wojdyla D, Say L, Gulmezoglu AM, Van Look PF. WHO analysis of causes of maternal death: a systematic review. Lancet. 2006;367(9516):1066–1074.
Lain KY, Roberts JM. Contemporary concepts of the pathogenesis and management of preeclampsia. JAMA. 2002;287(24):3183–3186.
van Rijn BB, Hoeks LB, Bots ML, Franx A, Bruinse HW. Outcomes of subsequent pregnancy after first pregnancy with early-onset preeclampsia. Am J Obstet Gynecol. 2006;195(3):723–728.
Redman CW, Sargent IL. Latest advances in understanding preeclampsia. Science. 2005;308(5728):1592–1594.
Dekker GA. Risk factors for preeclampsia. Clin Obstet Gynecol. 1999;42(3):422–435.
Sibai B, Dekker G, Kupferminc M. Pre-eclampsia. Lancet. 2005;365(9461):785–799.
Duckitt K, Harrington D. Risk factors for pre-eclampsia at antenatal booking: systematic review of controlled studies. BMJ. 2005;330(7491):565.
Wagner LK. Diagnosis and management of preeclampsia. Am Fam Physician. 2004;70(12):2317–2324.
Hnat MD, Sibai BM, Caritis S, et al. Perinatal outcome in women with recurrent preeclampsia compared with women who develop preeclampsia as nulliparas Am J Obstet Gynecol. 2002;186(3): 422–426.
Sep SJ, Smits LJ, Prins MH, Spaanderman ME, Peeters LL. Simple prepregnant prediction rule for recurrent early-onset hypertensive disease in pregnancy. Reprod Sci. 2009;16(1):80–87.
Brown MA, Lindheimer MD, de Swiet M, Van Assche A, Moutquin JM. The classification and diagnosis of the hypertensive disorders of pregnancy: statement from the International Society for the Study of Hypertension in Pregnancy (ISSHP). Hypertens Pregnancy. 2001;20(1):IX–XIV.
Sibai BM. Diagnosis, controversies, and management of the syndrome of hemolysis, elevated liver enzymes, and low platelet count. Obstet Gynecol. 2004;103(5)(Pt 1):981–991.
Barton JR, Sibai BM. Prediction and prevention of recurrent preeclampsia. Obstet Gynecol. 2008;112(2)(Pt 1):359–372.
Dildy GA 3rd, Belfort MA, Smulian JC. Preeclampsia recurrence and prevention. Semin Perinatol. 2007;31(3):135–141.
Rasmussen S, Irgens LM, Albrechtsen S, Dalaker K. Predicting preeclampsia in the second pregnancy from low birth weight in the first pregnancy. Obstet Gynecol. 2000;96(5) (Pt 1):696–700.
Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis J Clin Epidemiol. 1996;49(12): 1373–1379.
Moons KG, Royston P, Vergouwe Y, Grobbee DE, Altman DG. Prognosis and prognostic research: what, why, and how? BMJ. 2009;338:b375. doi: 10.1136/bmj.b375.
Royston P, Moons KG, Altman DG, Vergouwe Y. Prognosis and prognostic research: developing a prognostic model. BMJ. 2009;338:b604. doi: 10.1136/bmj.b604.
O’Brien TE, Ray JG, Chan WS. Maternal body mass index and the risk of preeclampsia: a systematic overview. Epidemiology. 2003;14(3):368–374.
Montoro MN, Kjos SL, Chandler M, Peters RK, Xiang AH, Buchanan TA. Insulin resistance and preeclampsia in gestational diabetes mellitus. Diabetes Care. 2005;28(8):1995–2000.
Scioscia M, Gumaa K, Rademacher TW. The link between insulin resistance and preeclampsia: new perspectives. J Reprod Immu-no/. 2009;82(2): 100–105.
The Netherlands Perinatal Registry [homepage on the internet]. Bilthoven: NPR-foundation; [cited 2010 October 1]. http://www.perinatreg.nl/
Rubin DB. Inference and missing data Biometrika. 1976;63(3): 581–592.
Donders AR, van der Heijden GJ, Stijnen T, Moons KG. Review: a gentle introduction to imputation of missing values. J Clin Epidemiol. 2006;59(10):1087–1091.
Frank E, Harrell J. Regression Modeling Strategies. New York, NY: Springer; 2001.
Steyerberg EW. Clinical Prediction Models. New York, NY: Springer; 2009.
Hanley JA, McNeil BJ. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology. 1983;148(3):839–843.
Hosmer DW, Lemeshow S. Applied Logistic Regression. New York, NY: John Wiley; 2000.
Steyerberg EW, Harrell FE Jr, Borsboom GJ, Eijkemans MJ, Vergouwe Y, Habbema JD. Internal validation of predictive models: efficiency of some procedures for logistic regression analysis. J Clin Epidemiol. 2001;54(8):774–781.
Harrell FE Jr. Regression Modeling Strategies. New York, NY: Springer; 2001.
Greenland S. Quantifying biases in causal models: classical confounding vs collider-stratification bias. Epidemiology. 2003;14(3):300–306.
Smits LJ, Van Kuijk SMJ, Peeters LL, Prins MH, Sep SJ. Collider-stratification bias complicates estimation of the strength of risk factors of disease recurrence. Submitted.
Steyerberg EW. Clinical Prediction Models. New York, NY: Springer; 2009.
Facchinetti F, Marozio L, Frusca T, et al. Maternal thrombophilia and the risk of recurrence of preeclampsia. Am J Obstet Gynecol. 2009;200(1):46. e41–e45.
Aardenburg R, Spaanderman ME, van Eijndhoven HW, de Leeuw PW, Peeters LL. A low plasma volume in formerly preeclamptic women predisposes to the recurrence of hypertensive complications in the next pregnancy. J Soc Gynecol Investig. 2006;13(8):598–603.
Delahaije DH, van Kuijk SM, Dirksen CD, et al. Cost-effectiveness of recurrence risk guided care versus care as usual in women who suffered from early-onset preeclampsia including HELLP syndrome in their previous pregnancy (the PreCare study). BMC Pregnancy Childbirth. 2010;10:60.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
van Kuijk, S.M.J., Nijdam, ME., Janssen, K.J.M. et al. A Model for Preconceptional Prediction of Recurrent Early-Onset Preeclampsia: Derivation and Internal Validation. Reprod. Sci. 18, 1154–1159 (2011). https://doi.org/10.1177/1933719111410708
Published:
Issue Date:
DOI: https://doi.org/10.1177/1933719111410708