Révélation atypique d´un lymphome B diffus à grandes cellules par une lésion ulcérée
Nouama Bouanani, Mounia Bendari
Corresponding author: Nouama Bouanani, Hematology and Stem Cell Transplant Department, Blood Transfusion and Cellular Therapy, Cheikh Khalifa International University Hospital, Casablanca, Morocco 
Received: 08 Jun 2020 - Accepted: 24 Jul 2020 - Published: 18 Aug 2020
Domain: Oncology
Keywords: Lymphome B diffus à grandes cellules, abcès cutané, chimiothérapie
©Nouama Bouanani et al. PAMJ - Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Nouama Bouanani et al. Révélation atypique d´un lymphome B diffus à grandes cellules par une lésion ulcérée. PAMJ - Clinical Medicine. 2020;3:176. [doi: 10.11604/pamj-cm.2020.3.176.24143]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com/content/article/3/176/full
Images in clinical medicine 

Révélation atypique d´un lymphome B diffus à grandes cellules par une lésion ulcérée
Révélation atypique d´un lymphome B diffus à grandes cellules par une lésion ulcérée
Atypical revelation of diffuse large B-cell lymphoma by a skin abscess
Nouama Bouanani1,2,&, Mounia Bendari1,2
&Auteur correspondant
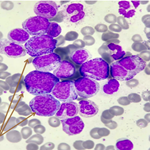
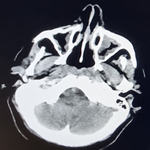
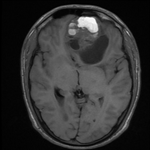
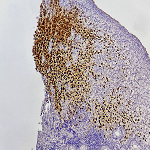
We report a rare case about a 80-years-old Moroccan woman with a past medical history of hypertensive heart disease, admitted to the emergency department with skin abscessed evolving for 1 month in the lower third of the left leg gradually increasing in volume, not responding to anti staphylococcal treatment (local and oral), complicated by deep ulceration with loss of substance. The initial examination found the patient in good general condition, performance status was at 2, with a hard lesion of the lower third of the left leg (4/3 cm) ulcerated, edematous, painful, oozing and inflammatory reaction. The rest of the physical examination was normal. Laboratory testing revealed anemia at 10 g/dl, high serum viscosity (40 mm/h). C reactive protein at 80 mg/l, with negative procalcitonin. Serum protein electrophoresis showed inflammatory syndrome without hypogammaglobulinemia, lactate dehydrogenase (LDH) at 276 IU/L. The radiological assessment of the affected limb showed a mass of the soft parts without bone lysis, the Ultrasound for Lower Extremity Deep Venous was normal. Skin biopsy concluded to diffuse large B cell lymphoma non-germinal center type, radiographic imaging (computed tomography and PET) were negative, the international prognostic index was at 3. To date, the patient has received 2 cycles of R-mini-CHOP (rituximab, cyclophosphamide, doxorubicin, prednisone, vincristine) with an onset of healing of the lesion, and it is planned to make 6 cycles with radiological evaluation halfway.
Key words: Diffuse large B-cell lymphoma, skin abscess, chemotherapy

Nous rapportons l´observation d´une patiente de 80 ans, connue hypertendue sous traitement, non diabétique. Qui s´est présentée en consultation pour lésion abcédée évoluant depuis 1 mois intéressant le tiers inférieur de la jambe gauche augmentant progressivement de volume, ne répondant pas au traitement anti staphylococcique (locale et oral), compliquée d´une ulcération profonde avec perte de substance, évoluant dans un contexte de conservation de l´état général. L´examen initial a retrouvé une patiente en bon état général, performans statut à 2, avec une lésion indurée du tiers inférieur de la jambe gauche (4/3 cm) ulcérée, douloureuse, suintante avec réaction inflammatoire. Le reste de l´examen somatique était normal. Le bilan biologique initial était normal avec un LDH à 276 UI/L. Une protéine C-Réactive à 80 mg/ L avec une pro calcitonine négative, une vitesse de sédimentation accélérée à 40 mm la première heure, une électrophorèse des protéines sériques en faveur d´un syndrome inflammatoire, sans hypogammaglobulinémie. Le bilan radiologique du membre atteint a montré une masse des parties molles sans atteintes osseuses en regard. La biopsie de la lésion était en faveur d´un Lymphome B Diffus à grandes cellules de type non centre germinatif. Le bilan d´extension était négatif. L´index pronostique International était à 3. L´écho-doppler veineux du membre inférieur atteint n´a pas retrouvé de thrombose veineuse profonde, le bilan pré thérapeutique était correct. La patiente a reçu à ce jour 2 cures de chimiothérapie (R-mini-CHOP), avec un début de cicatrisation de la lésion, et il est prévu de faire 6 cures avec évaluation radiologique à mi-chemin.
Figure 1: tuméfaction ulcérée du tiers inférieur de la jambe gauche
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures

Article metrics
Recently from the PAMJ-CM