Article Text

Abstract
Background Ongoing education of health professionals in rheumatology (HPR) is critical for high-quality care. An essential factor is education readiness and a high quality of educational offerings. We explored which factors contributed to education readiness and investigated currently offered postgraduate education, including the European Alliance of Associations for Rheumatology (EULAR) offerings.
Methods and participants We developed an online questionnaire, translated it into 24 languages and distributed it in 30 European countries. We used natural language processing and the Latent Dirichlet Allocation to analyse the qualitative experiences of the participants as well as descriptive statistics and multiple logistic regression to determine factors influencing postgraduate educational readiness. Reporting followed the Checklist for Reporting Results of Internet E-Surveys guideline.
Results The questionnaire was accessed 3589 times, and 667 complete responses from 34 European countries were recorded. The highest educational needs were ‘professional development’, ‘prevention and lifestyle intervention’. Older age, more working experience in rheumatology and higher education levels were positively associated with higher postgraduate educational readiness. While more than half of the HPR were familiar with EULAR as an association and the respondents reported an increased interest in the content of the educational offerings, the courses and the annual congress were poorly attended due to a lack of awareness, comparatively high costs and language barriers.
Conclusions To promote the uptake of EULAR educational offerings, attention is needed to increase awareness among national organisations, offer accessible participation costs, and address language barriers.
- Nursing
- Occupational therapy
- Health services research
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Health professionals in rheumatology (HPR) are a heterogeneous group of professionals with different roles, responsibilities and scopes of practice. Their training differs depending on the level of professional qualification and varying health systems across countries.
Educational needs of HPR differ considerably across countries and professions.
WHAT THIS STUDY ADDS
While health professionals in rheumatology (HPR) in Europe have a solid knowledge about the existence of the European Alliance of Associations for Rheumatology (EULAR), they have little awareness about its educational offerings: approximately 90% do not know the ‘Teach the Teacher Course’, up to 80% are not aware of travel bursaries.
English as the primary language in educational offerings of EULAR is a significant obstacle for more than 50% of HPR whose mother tongue is not English. Even among HPR who, ‘felt comfortable taking a course in English’, would prefer educational offerings in the national language (52%).
Higher educated HPR and HPR with more extended work experience are more likely to attend the annual EULAR congress, whereas HPR with less work experience are more likely to take up EULAR School of Rheumatology offerings.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Better-educated HPRs provide better care.
Increasing awareness and use of EULAR educational offerings can increase up-to-date knowledge of HPR, promote research and collaboration and, ultimately, contribute to better patient outcomes.
Active involvement of national HPR organisations is needed to ensure the leading role of EULAR in educational opportunities in rheumatology.
Background
Millions of people worldwide lack access to high-quality healthcare because of shortages, the uneven geographical distribution of service provision and not sufficiently trained health professionals.1 Higher education of health professionals contributes to better patient outcomes; a study even demonstrated that a higher number of nurses with a bachelor’s degree (compared with a diploma or an associate degree) reduced hospital mortality rates.2 To ensure that health professionals continue their education and training over a more extended period of their working life and, thus, contribute to a high quality of healthcare, many countries decided to make continuing education mandatory. As a result, health professionals are increasingly required to participate in continuing education after completing their basic training.3
Health professionals in rheumatology (HPR) play a critical role in the care of people with rheumatic and musculoskeletal diseases (RMDs). HPR are from different professions and include nurses, occupational therapists, physical therapists, social workers, psychologists, pharmacists and others. The EULAR definition of HPR does not include registered medical practitioners. Basic training varies across countries, and harmonised postgraduate education could guarantee that patients with similar diseases receive similar quality of care in different countries.4 5 Vliet Vlieland et al4 conducted an educational needs survey in 2015, being the first inventory of the educational needs of HPR in Europe. However, after the EULAR School of Rheumatology (ESOR) was launched in 2017, the educational needs of HPR were not reassessed, and EULAR’s new educational offerings for HPR have not yet been evaluated. In addition, changes in the legislation in some countries, such as the mandatory registration (and reregistrations) of HPR in Austria, Croatia, Cyprus, Ireland, Serbia, the UK and others and the need for accreditation of postgraduate courses in some countries, may also have led to changes in educational requirements. Compared to 2015,4 national offerings may have also changed over time. Moreover, the COVID-19 pandemic has significantly changed some of the didactic preferences of postgraduate education. For example, it has made online access to high-level specialists, unbound by time and space, more widely accepted. This study aimed to (1) determine current HPR educational readiness, needs and preferences, (2) identify barriers to taking part in postgraduate education and (3) ask for feedback on the current offerings and activities of ESOR for HPR.
Methods and participants
Design and participants
The Educational Subcommittee of the EULAR Committee of HPR, in collaboration with the EULAR Committee of Education and Training and the Paediatric Rheumatology European Society, developed an online survey. The questionnaire was adapted from the 2015 version by Vliet Vlieland et al4 and extended to include questions asking for feedback on current courses. The following main topics were covered in the survey: (1) characteristics of the respondents, current educational needs in terms of clinical practice and theoretical knowledge, RMDs that should be addressed in the courses, wishes and expectations regarding the organisation of EULAR/ESOR courses, (2) barriers for participation in the courses, familiarity and awareness of the educational offerings from EULAR/ESOR, and (3) feedback on the current educational offerings of EULAR/ESOR.
The online survey was distributed using a free software programme (www.soscisurvey.com). It was tested in advance by the Educational Sub-Committee of the EULAR Committee of HPR, and the feedback was used to adapt the questionnaire. We intended to distribute the questionnaire in as many European countries as possible. For this reason, we translated the questionnaire into 24 languages (Czech, Croatian, Danish, Dutch, English, Estonian, Finnish, French, German, Greek, Hungarian, Italian, Norwegian, Polish, Portuguese, Romanian, Russian, Serbian, Slovak, Slovenian, Spanish, Swedish, Turkish and Ukrainian). With these languages, we could cover the 25 national member organisations of EULAR and, at the same time, the 20 most populous European countries. Each translation was peer debriefed by at least two native-speaking HPR. The English version of the questionnaire is found in the supplement (online supplemental table A). The entire questionnaire, with all translations and response options, can be requested by the corresponding author.
Supplemental material
The questionnaire was distributed at the end of June 2021 via networks of the national professional organisations, the EULAR HPR Newsletter, participants in previous EULAR HPR activities, national liaison persons, national HPR associations, universities and other educational institutions with a request to forward it to all health professionals in the field of rheumatology. A similar invitation/reminder to participate in the questionnaire was sent in September 2021. Reporting of the results followed the ‘Checklist for Reporting Results of Internet E-Surveys’ guideline.6
Data analysis
The responses of all participants were recorded anonymously. Absolute frequencies and percentages were given for categorical data. Ordinal variables were reported with median and IQR, metric variables with mean and SD as well as median and IQR, both for the whole study population and subgroups (HPR in adult care (HPR-A) and HPR in paediatric care (HPR-P)). As a final step, we conducted subgroup analyses for the three most prominent professional groups (nurses, physiotherapists, occupational therapists) and the North, South, East and Central European regions.7
We used natural language processing and the Latent Dirichlet Allocation (LDA)8 9 to analyse the questionnaire’s free text fields (feedback on current EULAR/ESOR offerings). LDA is a technique used for unsupervised generative probabilistic topic modelling. It aims to extract the meanings of a predefined number of topics. Each topic is characterised by high-frequency words and words that are best suited to distinguish it from other topics. To perform LDA, we created a semantic space by downloading and translating all the answers into English. Then, we took the following steps: stemming the words, removing stop words, casting the text into lowercase only and removing punctuations, names and personal references. We then explored the frequency of words and correlations between the co-occurrence of words and extracted five topics based on LDA. The number of topics was determined by examining the heatmaps and the coherence of the words in the topics. Heatmaps are a popular graphical method for visualising high-dimensional data. In a heatmap, tables of data are coded as coloured cells. The matrix’s rows and columns are arranged, so patterns become highlighted. The dendrogram reflects the inter-relationships of the topics and shows similarities between responses.
Regression analysis
We used multiple logistic regression models to determine higher postgraduate educational readiness factors. We operationalised educational readiness by means of four variables: first, in terms of knowledge (Have you ever heard of EULAR/ESOR?) and second, in terms of action taken (Have you ever attended the annual EULAR Congress/ESOR offerings?). The independent variables were selected from participants’ personal data (age, gender, occupation, work with children/adults, the highest level of education completed, work experience with people with RMD and time spent working in clinical patient care/research/organisational roles). All variables were tested for multicollinearity prior to the regression analysis.10 11 All analyses were conducted using R (http://www.r-project.org).12
Results
Response rate
In total, the questionnaire was viewed 3589 times, and 998 times it was started to be filled in. Of these, 667 HPR (66.8%) from 34 European countries completed the questionnaire (figure 1 and table 1).
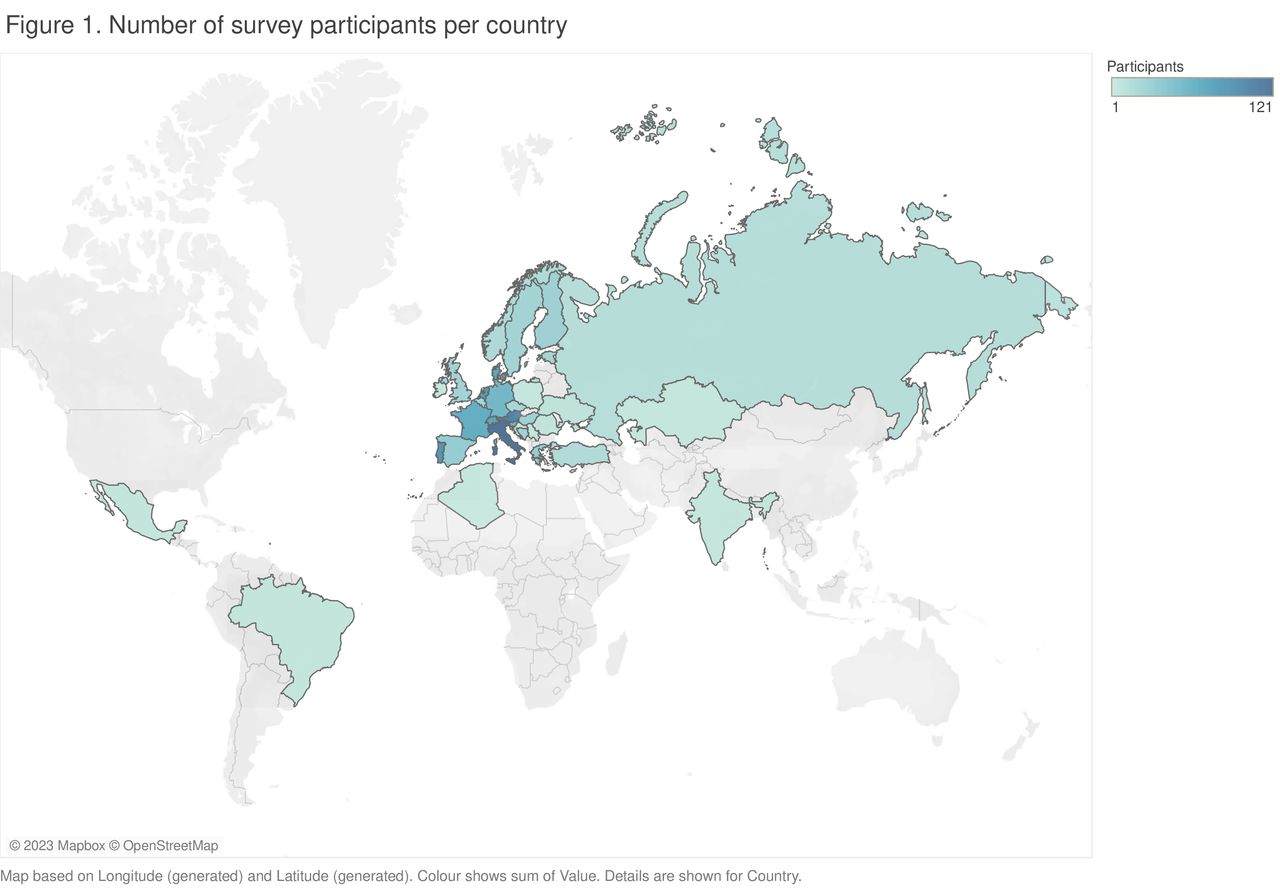
European map of the respondents in this survey. The graph below shows the distribution of the HPR' responses according to the geographical distribution. HPR, health professionals in rheumatology.
Characteristics of HPR who participated in the survey
Participant characteristics
The respondents were mainly women (n=762; 76.4%), and the mean age was 40.53 (±11.5) years. More than 50% of the participants had a bachelor’s degree or similar, 24.9% (n=245) had a master’s degree and 9.1% (n=90) had a PhD (table 1). Physiotherapists (n=350; 34.8%), nurses (n=248; 25.0%) and occupational therapists (n=189; 18.8%) were the most frequent professions who responded to the questionnaire. Of all responses, n=913 (91.5%) came from HPR working with adults, and n=85 (8.5%) from HPR in children’s/youth’s care.
Educational readiness
In terms of knowledge, familiarity with EULAR or ESOR was mainly associated with being a nurse, being older (in years), having more experience in the field of rheumatology, having a formally higher level of education and being more involved in research. We observed a similar pattern in participation at the annual EULAR congress. Nurses and HPR with higher levels of education and increased research activities were also associated with taking part in the congress. This result contrasts with attendance in ESOR courses. In particular, people with less work experience seem to feel more addressed by the offer than more experienced people (OR 0.91, CI 95% 0.81 to 0.99) (online supplemental table C).
Supplemental material
Educational needs: differences between health professionals in adult and paediatric care
The highest-rated educational need in terms of clinical practice was professional development for paediatric HPR (3.91; on a scale of 1 to 5) and prevention for HPR in adult care (3.70). ‘Clinical characteristics’ were rated as the most important theoretical knowledge for both HPR-A and HPR-P (3.62 and 4.00, respectively). Practice organisation and management were rated lowest by HPR-A (3.08), and training in diagnostic assessments by HPR-P (2.78). According to the ratings provided by HPR-A and HPR-P, the RMDs that need to be covered in the courses received all high scores, ranging from 3.76 to 4.49 (tables 2 and 3).
Educational needs
RMDs that should be addressed in the courses
Course organisation: live courses and prerecorded (online) lectures were preferred
Live courses taking place face-to-face (n=463; 38.6%) and prerecorded online lectures accessible without time constraints (n=338; 28.2%) were preferred over other modalities. Almost half of the participants (n=377; 44.0%) considered a course duration of 1–2 days optimal, and two-thirds of HPR preferred the organisation of the courses by EULAR compared with national organisations. However, following the responses of the HPR, offerings should be available in national languages rather than in English (table 4). Even among HPR who said they ‘felt comfortable taking a course in English’ (n=419), more than half would still prefer courses in the national language (n=219; 52.3%).
Course organisations
Barriers: lack of awareness of educational offerings and content
Lack of awareness of the educational offerings (3.30; ±1.49) and lack of knowledge of the content of the offerings (3.51; ±1.50) were mentioned as the most important barriers to non-participation in EULAR/ESOR educational offerings (on a scale of 1–5). Likewise, the participants perceived the costs of ESOR courses (3.29; ±1.36) and the annual congress (3.46; ±1.34) as too high. Participants reported that despite their interest in EULAR’s educational offerings, they did not receive support in the form of time resources during work hours from their employers to attend the courses (3.32; ±1.39). The technical requirements for participation in an online course, such as the availability of computers, laptops or tablets, and an internet connection, were not considered obstacles to participation in the courses or classes (table 5).
Barriers to participating in educational offerings
Feedback on the current offerings of ESOR for HPR
Although almost two-thirds of HPR-A and half of HPR-P were familiar with EULAR, they reported little awareness or use of EULAR’s offerings for HPR. Three-quarters of HPR only had limited or no knowledge of travel bursaries, and 85% (HPR-A), respectively, 97% (HPR-P), were not aware of the Teach the Teacher Course. Sixty to 80% have never visited the EULAR/ESOR communication platforms, and 73.9% (HPR-A), respectively 90.7% (HPR-P) had never participated in the annual EULAR congress (table 6).
Feedback on EULAR
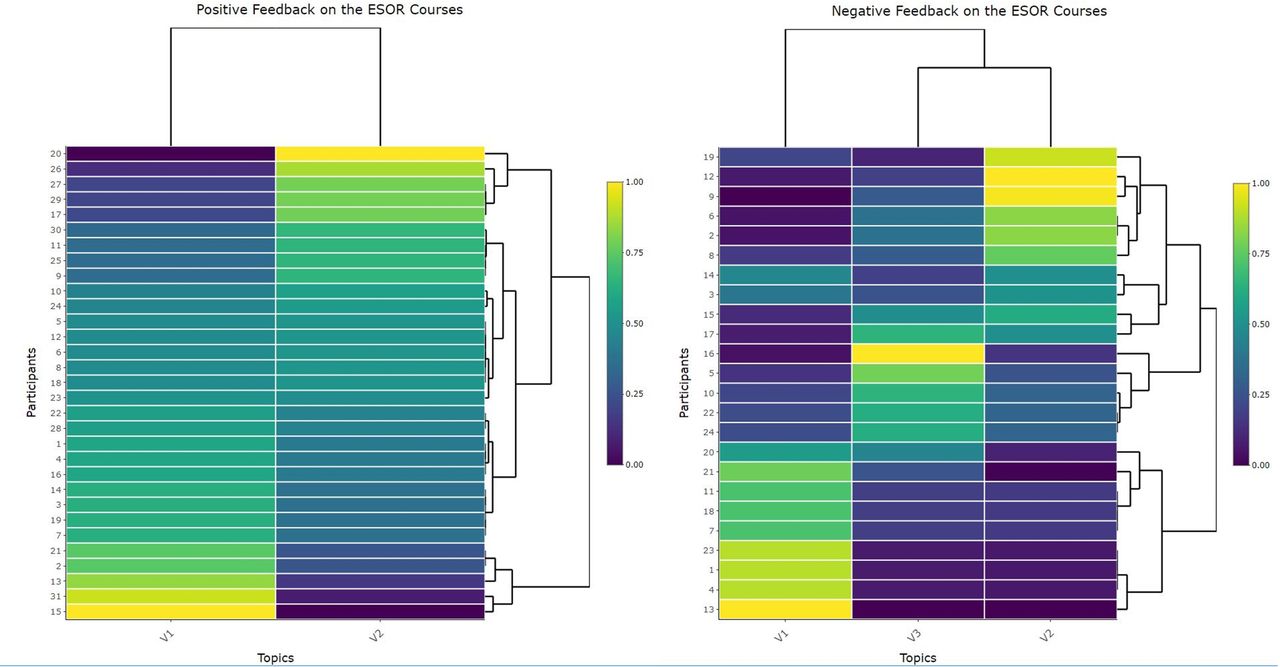
Using LDA, we generated two topics from positive feedback and three from negative feedback (figure 2 and online supplemental table B). The comprehensive and up-to-date course content, along with the flexibility to attend classes without any time restrictions, were highly valued, resulting in overall positive responses (online courses offer time flexibility and the possibility to complete the course at your own pace). Barriers to participation in training were: uncertainty if there would be a profession-specific gain from participating in interdisciplinary courses (The online course should have a clear benefit for the respective professional groups, even if it is a multidisciplinary course), language limitations during the classes (English is challenging in classes, especially when you want to ask questions) and problems with the English language in the final exams (English is challenging, especially in the exams).
Supplemental material

{kind=link}
{kind=link}
Heatmaps. Results of the Latent Dirichlet Allocation (LDA) model regarding the positive and negative feedback on the current ESOR Courses. On the right side, the participants are listed with their IDs. V1, V2 and V3 are the topics that LDA generated from the responses. The number of topics has resulted from the generated patterns. The more a linkage point appears in yellow, the more strongly a participant’s statement is linked to that topic. The dendrograms on the sides show how the variables and rows are clustered independently. ESOR, EULAR School of Rheumatology.
Differences in educational preferences but not the delivery method
As expected, our subgroup analysis revealed differences in educational preferences related to course content across professions and countries. However, we found surprisingly limited variation in the preferences for the delivery method of educational offerings. The most common selection for live/on-site courses lasting 1–2 days and being conducted in the national language remained consistent across professions and countries. The only tendency found (not significant, p=0.056) was that Eastern countries favoured discipline-specific content (37.1% to 34.3% multidisciplinary) compared with the other countries. Nurses were more likely to attend the EULAR Congress (36.3%) than other professional groups (PT 16.9%, OT 12.6%; OR 2.35 CI 95% 0.98 to 5.87, p=0.05). Detailed results of the subgroup analysis are found in appendices E-I and J-O.
Discussion
This study aimed to identify the educational needs of HPR in paediatric and adult care. For the first time, we anonymously asked for feedback on the current educational offerings of EULAR/ESOR in 34 countries and described current barriers to the attendance of EULAR/ESOR offerings.
It is already widely recognised that the successful implementation of postgraduate HPR education is of great importance to ‘increase the quantity, quality and relevance of health professionals, and in so doing strengthen the country health systems and improve population health outcomes’.13
Our study’s two most important findings were that (1) EULAR only succeeds in reaching a minority of HPRs in Europe and (2) that services do not appeal equally to the broad range and different educational levels of HPRs. Our study found that higher age, more professional experience, being a nurse, and a higher level of education contributed significantly to the knowledge of EULAR and ESOR and attendance at the annual EULAR congress. In terms of higher education level, we were able to show, for example, that having a PhD increases the likelihood of knowing about ESOR (OR 3.70) and whether one has ever attended the EULAR congress (OR 7.50). Accordingly, the EULAR congress is (more) attractive to older and formally more educated HPR. However, we observed a contrasting picture with the ESOR offerings. The courses were more likely to be attended by HPRs with less experience in the field of rheumatology (OR 0.91).
Several strategies can be derived from our findings on how to achieve a better use of educational offerings among HPR in Europe. Our findings suggest that several strategies can be implemented to enhance the utilisation of educational offerings among HPR in Europe. For instance, educational providers could target HPR at earlier stages of their career or those with less formal education by reviewing their existing offerings to identify which groups of HPR are being addressed. This would enable providers to develop tailored educational programmes that meet the specific needs of these groups, thereby increasing their engagement and participation.
To address the varying educational qualification levels of HPR in Europe, educational courses could be developed at different levels to lower the access barrier for early career HPR while also providing more formally educated and later career HPR with opportunities to continue their education at a higher level.13 This could be achieved by involving national organisations in disseminating educational offerings through their networks in national languages. Strengthening these organisations would increase the accessibility of educational opportunities to HPR in different regions of Europe. To minimise costs for EULAR while enhancing the utilisation of its course offerings in national countries, a ‘franchise’ model could be considered in addition to the teach-the-teacher courses. Under this model, EULAR would act as a ‘franchisor’ and permit national organisations to use its brand and course offerings. In exchange, national organisations would agree to pay a franchise fee to EULAR.
Another important finding of our survey was that English as an educational and examination language is a major barrier for HPR, whose native language is not English. Between 40% and 55% of all respondents indicated they did not feel comfortable taking a course in English. This problem was particularly cited when HPR were under time pressure and had to ask questions or take an exam in English. Even among HPR who reported having sufficient English competence to feel comfortable taking a course in English, more than half would still prefer their national language. HPR from northern countries (Estonia, Denmark, Finland, Norway, Sweden) were more likely to consider themselves advanced or fluent in English than HPR from other countries; however, the majority of them (58.8%) still preferred their national language. Therefore, one feasible approach to increase attendance in EULAR courses could be to translate the content (and exams) or offer courses with subtitles in the national language. English as a language was also identified in the first Education Needs Survey as an important barrier to using EULAR offerings.4 Apparently, this has not changed in the last 7 years. One lesson learnt from the survey is that EULAR messages/evidence may need to be translated into other languages to facilitate their implementation in clinical care across Europe.
A strength of our study was that we also analysed the free text entries (positive and negative feedback to the ESOR classes) with a natural language processing tool. We applied an unsupervised generative probabilistic method specifically designed for short text inputs, such as those typically found in questionnaires.8 The results of our project go beyond the interests of EULAR and ESOR. Although the findings are initially based on EULAR’s existing educational programme, they can also be useful for national education providers, for example, with regards to preferences in course content or delivery methods.
We are aware that our study has certain limitations. Although we translated the questionnaire into 24 languages, we could not exceed the overall response rate of the 2015 survey.4 Our study had limited representation from northern and eastern European countries. One reason may have been the timing during the (summer) vacations and/or the COVID-19 pandemic, which limited overall opportunities for training and education and may have changed the priorities for HPR. The results of our survey show that the proportions of some professions were different across the countries. In Portugal and Denmark, for example, more nurses participated compared with other countries, such as Austria or Italy. Such differences could limit the generalisability of our results. In addition, we had some missing data because it was not made mandatory to answer all questions in the survey. We decided not to make the responses mandatory because we wanted to give HPR as much freedom as possible in responding to the questions. However, the missing data could, of course, distort the results. Due to the study design and the partly unequally distributed responses in terms of country and profession, the sample’s representativeness is not given, and the results should be generalised only with caution.
Conclusion
HPR is often involved in supporting people with RMD in managing their disease. Their knowledge directly impacts people’s well-being and is critical to utilising other health resources. Therefore, ongoing education and training for the various healthcare professions are essential to ensure optimal care. Improving awareness of educational offers among national organisations and the challenge of reducing costs and language barriers are points of attention to promote future dissemination. EULAR and other international postgraduate training providers could use a ‘franchise’ model of their offerings tailored to local contexts.
Supplemental material
Supplemental material
Supplemental material
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Submission to an ethics committee was not required as we collected only anonymous data from experts and did not include any health-related data.
Acknowledgments
We would like to thank Siniša Grabovac for translating the questionnaire into Croatian and Serbian.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @v_ritschl, @DavergneT, @FerEstevezLopez, @FerreiraRJO, @ndosie, @jetteprimdahl1, @ankarausch
Contributors VR, EM, MRA, A-KRO, JC, TPMVV, TS built the first draft of the questionnaire. All authors reviewed the questionnaire and translated it into their respective languages. All authors distributed the questionnaire within their country and networks. VR, LS, EM and TS analysed and interpreted the data. All authors suggested and agreed upon the research questions. VR, LS, EM and TS wrote the first draft of the manuscript. All authors read and gave feedback to the manuscript and made contributions to the text. All authors approved the final version of the manuscript. TS and VR are the guarantor of the study. They accept full responsibility for the work and the conduct of the study, had access to the data, and controlled the decision to publish.
Funding This project was funded by EULAR.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests VR, LS, MRRA, MB, CB, JC, TD, JdlT, AdT, AD, FE-L, RJOF, GEF, JG, KK, MLK, CM-B, AM, JM, RHM, ElM, ErM, CN-S: no competing interest to declare. RD: Speaker fees from Abbvie, Elly Lilly, EwoPharma, Sandoz, and Novartis, all outside the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.