Article Text

Abstract
The outbreak of COVID-19 in Wuhan, China and its declaration as a global pandemic by WHO has left the medical community under significant pressure to rapidly identify effective therapeutic and preventative strategies. Chloroquine (CQ) and its analogue hydroxychloroquine (HCQ) were found to be efficacious against SARS-CoV-2 when investigated in preliminary in vitro experiments. Reports of success in early clinical studies were widely publicised by news outlets, politicians and on social media. These results led several countries to approve the use of these drugs for the treatment of patients with COVID-19. Despite having reasonable safety profiles in the treatment of malaria and certain autoimmune conditions, both drugs are known to have potential cardiotoxic side effects. There is a high incidence of myocardial injury and arrhythmia reported with COVID-19 infection, and as such this population may be more susceptible to this side-effect profile. Studies to date have now demonstrated that in patients with COVID-19, these drugs are associated with significant QTc prolongation, as well as reports of ventricular arrhythmias. Furthermore, subsequent studies have failed to demonstrate clinical benefit from either drug. Indeed, clinical trials have also been stopped early due to safety concerns over HCQ. There is an urgent need for credible solutions to the global pandemic, but we argue that in the absence of high-quality evidence, there needs to be greater caution over the routine use or authorisation of drugs for which efficacy and safety is unproven.
- pharmacology
- arrhythmias
- QT interval
- infection
- clinical trials
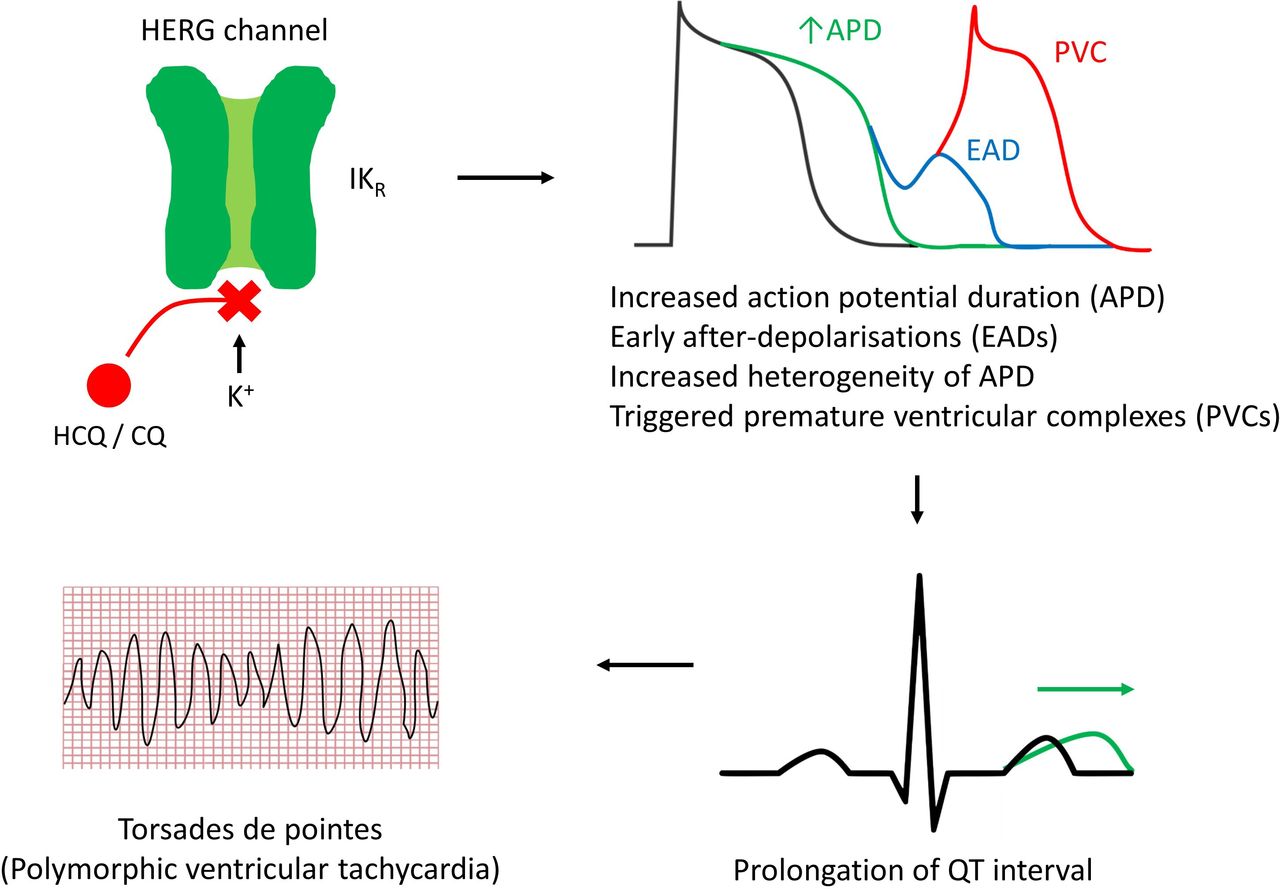
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Following the initial outbreak of COVID-19 in Wuhan, China and its declaration as a worldwide pandemic, there have been significant efforts to rapidly identify effective therapeutic and preventative strategies.1 Several treatments have been proposed and are currently under investigation.2–5 Most recently, dexamethasone has been reported to reduce mortality in patients with COVID-19 requiring supplemental oxygen or invasive mechanical ventilation.6 There are, however, inherent concerns with regards to the application of drugs for which efficacy and safety has yet to be established. The antimalarial drug chloroquine (CQ) and its analogue hydroxychloroquine (HCQ) have been shown to have antiviral actions against SARS-CoV-2 infection in vitro.7 Based on anecdotal experiences and a small number of clinical studies,8 9 these drugs have received widespread media attention.10 These early results led to a number of healthcare systems trialling them as treatment for patients with COVID-19 with varying reports of success.11 12 The addition of azithromycin (AZT), a macrolide antibiotic, has also been advocated despite limited evidence for its efficacy.2 Although HCQ and CQ appear to be safe in the treatment of some autoimmune diseases and malaria,13 14 it is unclear if this safety profile can be extrapolated to patients with COVID-19 and specific concerns have been raised over potential cardiovascular toxicity.
Mechanism of action of HCQ and CQ
The mechanism underlying the cardiotoxicity of both HCQ and CQ is the blockade of the human ether-à-go-go related gene (hERG) potassium channel.15 This voltage-gated ion channel mediates the rapid component of the delayed rectifier potassium current, IKr, which is crucial for the repolarisation of cardiac action potentials (figure 1). Therefore, blockade of this channel lengthens ventricular repolarisation which manifests as a prolonged QT interval on the surface ECG.16 This may also generate after-depolarisations through the reactivation of inward calcium depolarising currents, which can trigger premature ventricular contractions, polymorphic ventricular tachycardia and torsades de pointes (TdP). QTc intervals of more than 500 ms have been demonstrated to increase the risk of TdP events by twofold to threefold17 and if sustained can degenerate into ventricular fibrillation and cause sudden cardiac death.18 AZT has also been associated with both QTc prolongation19 and TdP20; therefore, the combination of these agents has been an area of interest.14
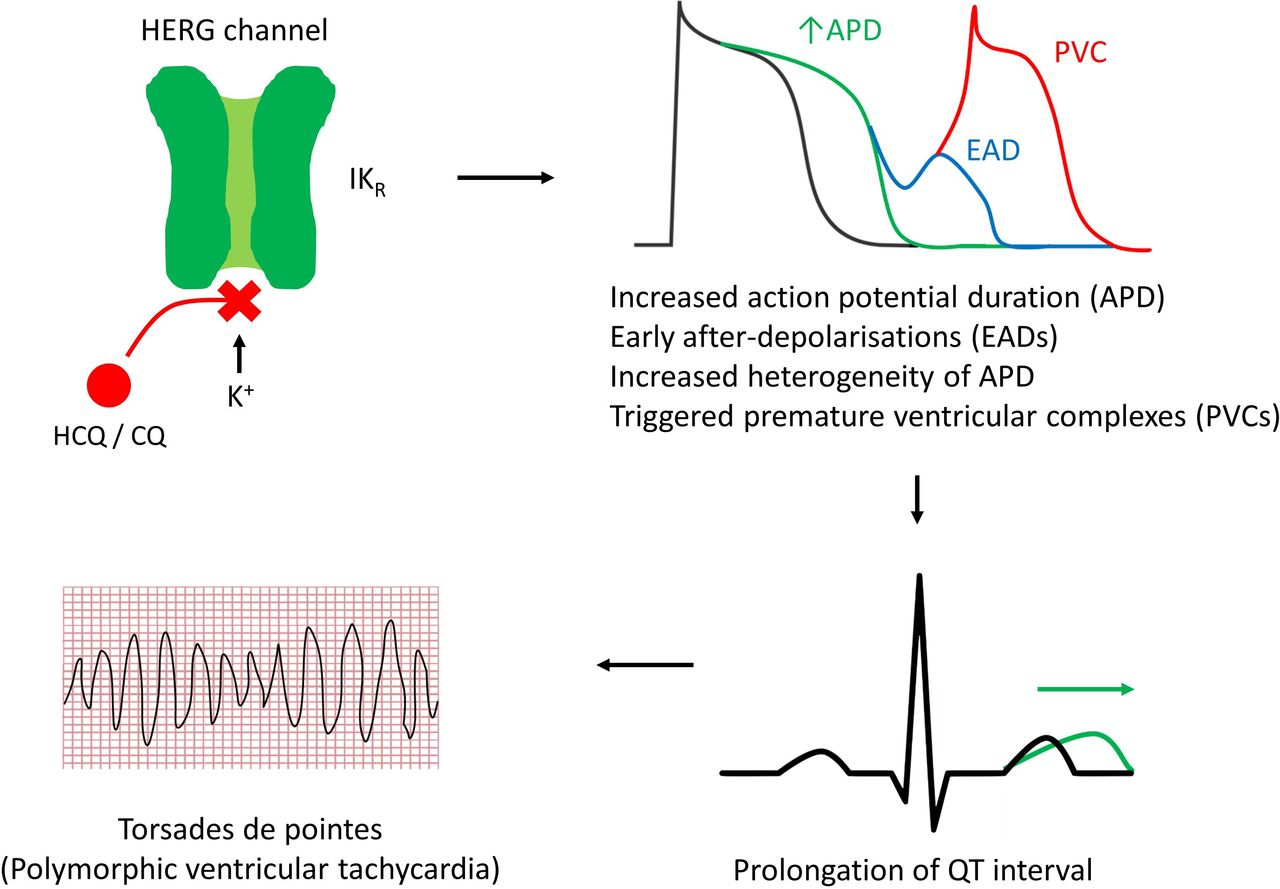
Mechanism of cardiotoxicity of hydroxychloroquine (HCQ) and chloroquine (CQ).
Is there any evidence of cardiotoxicity?
Patients with more severe phenotypes of COVID-19 disease, defined by requirement for intensive care support, have a higher incidence of cardiac arrhythmias.21 An infrequent but dangerous manifestation of COVID-19 is myocarditis.22 23 Myocarditis is a pro-arrhythmogenic condition24 and therefore the administration of QTc-prolonging drugs may exacerbate this underlying significant risk of arrhythmia. A retrospective case series of 187 patients with confirmed COVID-19 hospitalised in Wuhan, China showed that an elevated plasma troponin-T level (defined as serum levels above the 99th percentile upper reference limit) was associated with a higher mortality rate (59.6% vs 8.9%; p≤0.001) with inflammation proposed as a potential mechanism for myocardial injury.25 Interestingly in this study, these patients with an elevated troponin-T level also exhibited a higher incidence of sustained ventricular tachycardia or ventricular fibrillation compared with those with normal levels (11.5% vs 5.2%; p≤0.001). Therefore, patients with COVID-19 with evidence of cardiac inflammation appear to be particularly susceptible to arrhythmias.
There is emerging evidence that HCQ or CQ may be independently associated with cardiotoxicity in patients with COVID-19. Studies to date demonstrated that in patients with COVID-19 infection, both HCQ26 27 and CQ27 prolong the QTc interval (table 1). Pooled data from the available studies suggest that a significant proportion of patients with COVID-19 (ranging from 11% to 23%) developed QTc intervals greater than 500 ms.11 26–30 This is known to be associated with a twofold to threefold increased risk of TdP and multiple patients have required discontinuation of treatment due to QTc prolongation.29–31 A smaller proportion of patients (ranging from 0% to 4%) developed ventricular arrhythmias while on treatment,11 31 and there was one reported episode of TdP in the literature.28 Given the potential for QTc prolongation and increased risk of ventricular arrhythmia following treatment, it is advised that these medications be initiated in a hospital setting with regular ECG monitoring.
QTc prolongation and ventricular arrhythmia or mortality in trials using hydroxychloroquine (HCQ) or chloroquine (CQ) in combination with azithromycin (AZT)
There is some evidence that CQ/HCQ cardiotoxicity may be dose dependent. CQ doses in COVID-19 trials have typically involved a loading dose followed by daily doses between 500 and 600 mg and a total treatment duration of 5 days.28 31 A randomised controlled trial by Borba et al11 evaluating higher doses of CQ underwent an unplanned interim analysis of 81 patients as a result of safety concerns raised by their independent drug and safety monitoring board. This demonstrated that higher doses (600 mg twice daily for 10 days vs 450 mg twice daily for 1 day then once daily for 5 days) were associated with increased mortality rates and higher rates of patients developing QTc intervals greater than 500 ms (table 1). It should be noted that the high-dose group were older (54.7 years vs 47.4 years) and had a significantly higher prevalence of pre-existing cardiac conditions including heart failure and coronary artery disease (17.9% vs 0%). These differing population characteristics potentially confound the results and limit any conclusions which can be drawn. Nevertheless, the safety concerns raised by these data led to the immediate interruption of the high dosage arm of this trial.
The combination of HCQ or CQ with AZT has been compared with monotherapy, and studies have shown that this combination of treatment has an augmented effect on the QTc interval (table 1).29 31 There is therefore concern that this strategy carries a higher risk of malignant arrhythmias and death and indeed, one patient prescribed this combination developed TdP.31
Is it worth the risk?
Despite the initial reported success,2 subsequent studies have failed to show any significant benefit of either CQ or HCQ. Two observational studies of HCQ showed no reduction in either of the primary outcomes of death or the need for mechanical ventilation.3 30 In one study, treatment with HCQ alone was associated with increased overall mortality.12 An article that critically appraised the recent literature on the use of CQ or HCQ in the treatment of patients with COVID-19 concluded that the overall methodology was poor and that results were tempered by selection bias and residual confounding bias.32 Patient-important outcomes were poorly reported, in particular the incidence of QTc prolongation or cardiac arrhythmia. Included in this was the initial study on which several treatment recommendations were made. In this, it was reported that 600 mg HCQ daily resulted in significant reduction in viral carriage.2 This is a questionable primary outcome as efficacy would be better demonstrated through reduced mortality, reduction in need for mechanical ventilation or reduction in duration of hospital stay. Furthermore, there was no control arm. Worryingly, six patients were excluded from the primary analysis, including three patients who were transferred to intensive care and one patient who died. Excluding these patients from the analysis clearly biases the results as it potentially excludes patients with more severe phenotypes. There was no mention on the effects of the drugs on QTc interval or on the incidence of arrhythmia. These criticisms led to an official statement by the International Society for Antimicrobial Chemotherapy that this study did not meet their expected standards.33 As a consequence, based on this evidence, the efficacy or safety of these drugs in patients with COVID-19 remains unclear.
Despite the inconclusive and concerning nature of the available evidence, several countries have started to approve the use of HCQ and CQ for the treatment of COVID-19.34 35 The United States Food and Drug Administration (FDA) issued an emergency use authorisation for HCQ and CQ permitting their use in certain hospitalised patients with COVID-19 where clinical trials were unavailable or participation was unfeasible.36 This was followed by reports of widespread stockpiling of the drugs, which then led to shortages of them for their approved indications.37 38
Given the concerns over the proposed routine use of these QTc-prolonging drugs, the Canadian Heart Rhythm Society released a statement emphasising the need for baseline ECGs in hospitalised patients.39 It highlighted the need to review and discontinue unnecessary medications which may prolong the QTc interval and also recommended expert consultation in those patients with a QTc greater than 500 ms. A joint statement was also issued by the heads of several American cardiology groups who recognised that these drugs may cause arrhythmias and warned against starting or continuing HCQ, CQ or AZT in patients with a QTc greater than 500 ms.40
The widespread use of HCQ and CQ was surprising given the lack of convincing data supporting their efficacy in COVID-19. The body of evidence suggesting no benefit and indeed harm was also growing. Support for these drugs began to dwindle following the release of data from a multinational registry analysis on 22 May 2020 by Mehra et al. They reported an increased risk of in-hospital mortality and ventricular arrhythmia associated with the use of HCQ or CQ with or without a macrolide for the treatment of COVID-19.41 It was unclear if the increased in-hospital mortality was directly related to their cardiotoxicity; however, it was felt this was plausible given the significant proportion of patients reporting ventricular arrhythmias. This damning data led to the suspension of the chloroquine arm of the WHO Solidarity trial (figure 2). This announcement was followed by controversy as several concerns were raised over the veracity of the primary hospital data and analyses included in the study. An independent third-party peer review was launched, but as they were refused access to the full data set by the company providing the data (Surgisphere Corporation), they were unable to complete this. This led to the retraction of the paper by the authors.42

{kind=link}
{kind=link}
Hydroxychloroquine, chloroquine and COVID-19. A timeline of events. FDA, United States Food and Drug Administration.
This unfortunate development is concerning and its implications are unclear. Despite this, evidence continues to be published raising further doubt as to the efficacy of these drugs. One study has reported no significant benefit of HCQ as post-exposure prophylaxis for COVID-1943 and on 5 June 2020, the chief investigators of the RECOVERY trial have also released a statement announcing that following an interim review of the HCQ arm of their trial, they have decided to stop enrolling participants with immediate effect.44 They state that their data “convincingly rules out any meaningful mortality benefit of HCQ in patients hospitalised with COVID-19”. Following these results, the United States FDA made to revoke the emergency authorisation of both CQ and HCQ for the treatment of patients with COVID-19.45 These are only preliminary data and full results are yet to be released; however, at the time of writing it appears the widespread routine use of these drugs is unjustified and may lead to harm.
HCQ and CQ are chiral compounds currently used as racemates and can be replaced by their single enantiomers in a step called ‘chiral switch’.46 Interactions with drug targets may exhibit stereoselectivity with one enantiomer having differing activity when compared with the other. Perhaps an avenue of future research could look into whether this could attenuate the off-target effect of HCQ and CQ on the hERG potassium channel, thereby improving clinical safety in terms of cardiotoxicity.47
Conclusion
We have discussed evidence that raises concerns over the cardiotoxicity of HCQ and CQ. While considered safe to use in other conditions, patients with COVID-19 represent a potentially more vulnerable population. Patients with COVID-19 with myocarditis may be especially susceptible to the cardiotoxic side-effect profile of these drugs. These concerns were significant enough to prompt various national advisory bodies to release warning statements regarding their use. Despite the widespread publicity of these drugs, the evidence at the time for their efficacy was limited and of poor quality. Following the first Hippocratic tenant of non-maleficence, in view of safety concerns that are now being realised, we have to question whether the widespread adoption of these agents in several healthcare systems was justified. Given that subsequent trials have failed to reproduce any of the reported early success in the use of these drugs, it is our opinion that the potential risk of cardiotoxicity is not justified. HCQ and CQ are still being investigated and there is the possibility that enantiomers may be more efficacious and less toxic; however, this is yet to be established. The medical community remains under significant pressure to identify rapid and credible solutions to the global pandemic, but unless there is high-quality evidence showing a favourable risk:benefit ratio with adequate reporting of adverse effects, there needs to be greater caution prior to the recommendation of new treatments on an indiscriminate basis.
References
Footnotes
Contributors All authors contributed to the design and drafting and have approved the final version for publication. AS and AK contributed equally to this paper as joint first authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. All data included in this review article are available in the public domain.