Article Text

Abstract
Objective The goal of this study was to evaluate if addition of adjuvant chemotherapy to radiation therapy improves overall survival in patients with high-intermediate risk stage I endometrial carcinoma with lymphovascular invasion.
Methods Patients diagnosed between January 2010 and December 2015 with FIGO (International Federation of Gynecology and Obstetrics) stage I endometrioid endometrial carcinoma with lymphovascular invasion who underwent hysterectomy with lymphadenectomy and met the GOG-99 criteria for high-intermediate risk were identified in the National Cancer Database. Patients who received adjuvant radiotherapy with or without adjuvant chemotherapy (administered within 6 months of surgery) and had at least 1 month of follow-up were selected for further analysis. Overall survival was compared with the log-rank test following stratification by type of radiation treatment. A Cox model was constructed to control for a priori selected confounders.
Results A total of 2881 patients who met the inclusion criteria were identified; 2417 (83.9%) patients received radiation therapy alone while 464 (16.1%) received chemoradiation. Rate of adjuvant chemotherapy administration was comparable between patients who received vaginal brachytherapy alone (16.2%), and external beam radiation therapy (with or without vaginal brachytherapy) (15.8%), p=0.78. Rate of chemoradiation was higher for patients with grade 3 (28.8%) tumors compared with those with grade 2 (9.9%) and grade 1 (8.3%) tumors, p<0.001. After controlling for confounders for patients receiving external beam radiation, addition of chemotherapy was not associated with improved overall survival (HR 0.90, 95% CI 0.56 to 1.46). For patients receiving vaginal brachytherapy addition of chemotherapy was associated with better overall survival (HR 0.644, 95% CI 0.45 to 0.92). Benefit was limited to patients with grade 3 tumors, p=0.026; 4-year overall survival rate was 81.1% versus 74.9%.
Conclusions In patients with high-intermediate risk FIGO stage I endometrioid endometrial carcinoma and lymphovascular invasion, addition of chemotherapy to radiation therapy was associated with a survival benefit for patients with grade 3 tumors receiving vaginal brachytherapy.
- Uterine Cancer
- Radiotherapy
Data availability statement
Data may be obtained from a third party and are not publicly available. Data obtained from American College of Surgeons.
Statistics from Altmetric.com
HIGHLIGHTS
16% of patients with high-intermediate risk endometrial cancer and lymphovascular invasion received adjuvant chemotherapy in addition to radiotherapy.
For patients receiving external beam radiation, chemotherapy was not associated with a survival benefit.
For patients with grade 3 tumors receiving brachytherapy, addition of chemotherapy was associated with better overall survival.
Introduction
Endometrial cancer is the most prevalent gynecological malignancy in the United States and has an increasing overall incidence secondary to the obesity epidemic.1 Most patients will be diagnosed with endometrioid tumors confined to the uterus and have an excellent prognosis following hysterectomy.2 The GOG-99 and PORTEC trials identified a high-intermediate risk group that benefits from the administration of adjuvant radiation therapy, with a decreased relapse risk.3 4 Presence of lymphovascular invasion, even in the absence of lymph node metastases, has been identified as an independent negative prognostic factor in several studies.5–9 Patients with lymphovascular invasion have a higher risk of distant recurrences, indicating possible hematogenous dissemination, with certain authors advocating the utilization of chemotherapy.5–9 Lymphovascular invasion also has a negative impact on oncological outcomes independent of molecular subtype.10
A recent multi-center study that included 405 patients with high-intermediate risk early-stage endometrioid tumors and lymphovascular invasion demonstrated that adjuvant treatment improves both progression-free and overall survival.11 However, compared with vaginal brachytherapy alone, external beam radiation therapy and the addition of chemotherapy did not improve oncological outcomes.11 For patients with grade 3 tumors, a retrospective study demonstrated that adjuvant chemotherapy with or without radiation (n=45) improved progression-free survival compared with observation (n=21) or radiation alone (n=59).12 The current ESGO (European Society of Gynaecological Oncology)/ESMO (European Society of Medical Oncology) guidelines state that adjuvant chemotherapy could be considered for high-intermediate risk patients with high-grade tumors and/or substantial lymphovascular invasion (category 2).13 However, in the current National Comprehensive Cancer Network guidelines, addition of adjuvant systemic therapy to radiation therapy may be considered only for patients with stage IB grade 3 endometrioid tumors (category 2) regardless of the presence of lymphvascular invasion.14
The aim of the present study was to investigate the utilization and outcomes of adjuvant chemoradiation for patients with high-intermediate risk endometrioid endometrial carcinoma with lymphovascular invasion using a large hospital-based database reflecting real-world practice.
Methods
The National Cancer Database was accessed and patients with no history of another tumor diagnosed between January 2010 and December 2015 with a pathologically confirmed endometrioid adenocarcinoma of the uterus (International Classification of Disease 3 histology codes 8380/3, 8382/3 and 8383/3) and known tumor grade were identified. Patients with FIGO stage I disease who underwent hysterectomy with lymphadenectomy (as determined from the pathology report), had lymphovascular invasion present, received adjuvant radiation therapy (defined as external beam radiation therapy and/or vaginal brachytherapy administered within 6 months from surgery) and had at least 1 month of follow-up were identified. Patients deemed high-intermediate risk according to the GOG-99 criteria (similar to prior analysis of the National Cancer Database),15 who did and did not receive adjuvant chemotherapy (defined as chemotherapy administered within 6 months from surgery) were selected for further analysis. Patients with unknown interval between surgery and chemotherapy or radiotherapy and those who received neoadjuvant radiation or neoadjuvant chemotherapy were excluded. Online supplemental figure 1 depicts the patient selection flowchart.
The National Cancer Database is a hospital-based database capturing approximately 70% of all malignancies diagnosed in the United States. The American College of Surgeons and the Commission on Cancer have not verified and are not responsible for the analytical or statistical methodology employed, or the conclusions drawn from these data. The present study was deemed exempt from Institutional Board Review from Penn Medicine (Protocol No 829268).
Demographic and clinico-pathological patient characteristics were extracted from the deidentified dataset. Patient age was categorized into <65 and >65 years to identify an older patient population while the presence of comorbidities was evaluated from the Charlson-Deyo Comorbidity index and classified as absent (score 0) or present (score >1) and used as a surrogate for functional status. The frequency of distribution of categorical variables was compared with the χ2 test and continuous variables with the Mann-Whitney U test. Overall survival defined as time from diagnosis to death or censoring was assessed following generation of Kaplan-Meier curves and compared with the log-rank test. A Cox model was constructed to control for a priori selected confounders known to be associated with overall survival. Statistical analysis was performed following stratification by type of radiation therapy received (external beam radiation with or without vaginal brachytherapy and vaginal brachytherapy alone) while further exploratory analysis based on tumor grade was planned. Statistical analyses were performed with the Statistical Package for the Social Sciences v.27 (International Business Machines Corporation, Armonk, New York) and the α level of statistical significance was set at 0.05.
Results
A total of 2881 patients who met the inclusion criteria were identified; 2417 (83.9%) patients received radiation therapy alone while 464 (16.1%) received chemoradiation. (Online supplemental figure 1) summarizes the patient selection flowchart. Median time to radiotherapy was 56 days (IQR 30) while median time to chemotherapy was 46 days (IQR 30). The majority of patients (n=2058, 71.5%) received brachytherapy while 18.8% (n=543) received external beam radiation therapy, and 9.7% (n=280) received a combination of external beam and vaginal brachytherapy. For patients receiving chemotherapy, most (n=286) received chemotherapy first followed by radiation therapy (median interval from chemotherapy to radiotherapy initiation 69.5 days, IQR 40.3), while 20% (n=93) received concurrent chemoradiation and 18.3% (n=85) received radiation therapy followed by chemotherapy (median interval from radiotherapy to chemotherapy initiation 31 days, IQR 35.5).
Supplemental material
Rate of adjuvant chemotherapy administration was comparable between patients who received vaginal brachytherapy alone (16.2%) and external beam radiation therapy (with or without vaginal brachytherapy) (15.8%), p=0.78. Patients who received chemoradiation were younger (median 62 vs 65 years, p<0.001), and more likely to have private insurance (56.3% vs 43.8%, p<0.001), and have deep myometrial invasion (75% vs 67.9%, p<0.001). In addition, rate of chemoradiation was higher for patients with grade 3 tumors (28.8%) compared with those with grade 2 (9.9%) and grade 1 (8.3%) tumors, p<0.001. A higher rate of chemoradiation was also noted for patients who had more than 20 lymph nodes removed (20.7%) compared with those who had 1–9 (13.6%) and 10–20 (15%) lymph nodes removed, p<0.001. However, rate of chemoradiation utilization was comparable between academic and non-academic centers (16.6% vs 15.6%, p=0.47). Table 1 summarizes the clinic-pathological characteristics of patients who received adjuvant chemoradiation and radiation only stratified by type of radiation treatment. By binary logistic regression after controlling for patient age, insurance status, presence of comorbidities and extent of lymphadenectomy, patients with grade 3 tumors (OR 4.52, 95% CI 3.62 to 5.63), stage IB disease (OR 2.04, 95% CI 1.59 to 2.63) and those who received vaginal brachytherapy (OR 1.62, 95% CI 1.27 to 2.08) were more likely to receive adjuvant chemotherapy.
Clinico-pathological characteristics based on receipt of adjuvant chemotherapy
Median follow-up of the present cohort was 42.6 months (95% CI 41.29 to 43.93) with 396 deaths observed. For patients who received external beam radiation (with or without vaginal brachytherapy), there was no difference in overall survival between patients who did and did not receive chemotherapy, p=0.80; the 4-year overall survival rates were 81.1% and 83.2%, respectively (Figure 1). After controlling for patient age, race, insurance status, presence of comorbidities, tumor grade, depth of myometrial invasion, and extent of lymphadenectomy, chemoradiation was not associated with better overall survival compared with external beam radiation therapy alone (HR 0.90, 95% CI 0.56 to 1.46). No overall survival benefit was found following stratification by tumor grade; overall survival of patients who did and did not receive adjuvant chemotherapy was comparable for patients with grade 1 (p=0.81; 4-year overall survival rate 90.9% vs 93.5%), grade 2 (p=0.47; 4-year overall survival rate 92.4% vs 89.1%) and grade 3 tumors (p=0.62; 4-year overall survival rate 75.5% vs 74%) (Figure 2). Similarly, no survival benefit was found following stratification by disease stage for patients with stage IA (p=0.89; 4-year overall survival rate 81.2% vs 88.2%) and stage IB disease (p=0.92; 80.9% vs 81.9%).
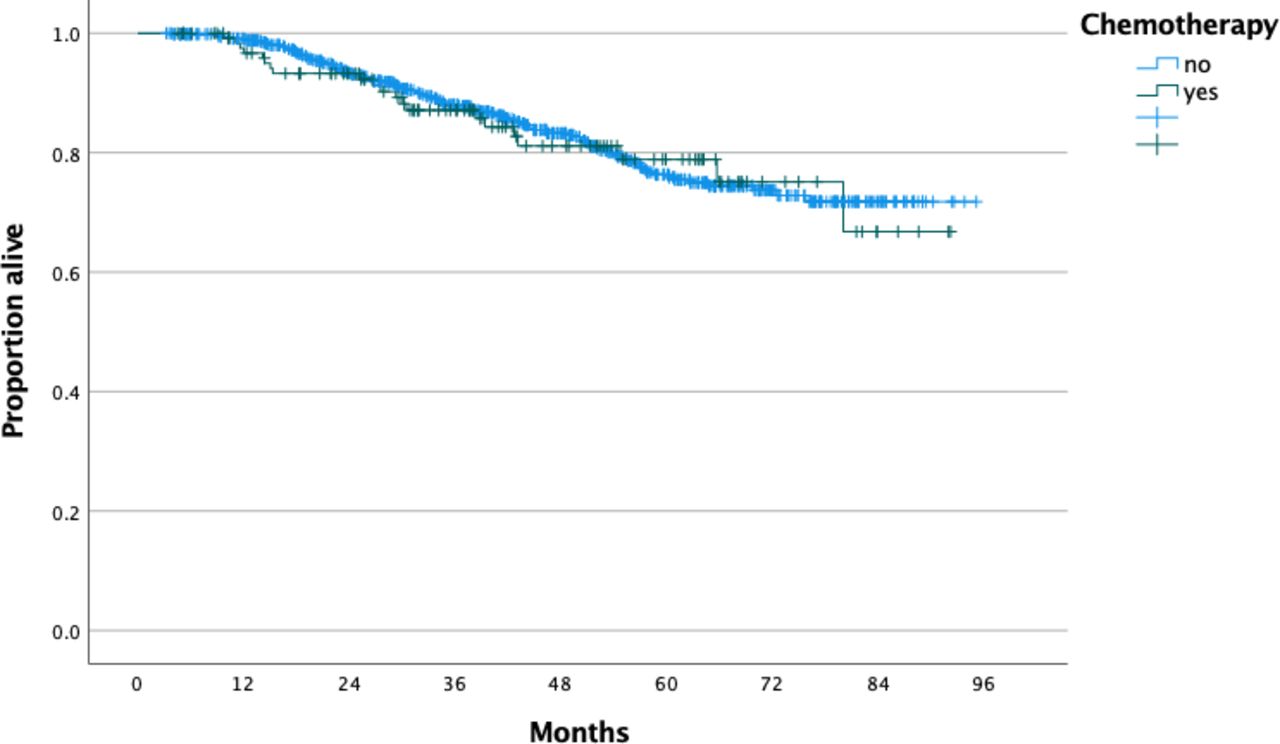
Overall survival of patients with high-intermediate risk endometrioid endometrial cancer and lymphovascular invasion who received external beam radiation therapy stratified by receipt of chemotherapy.
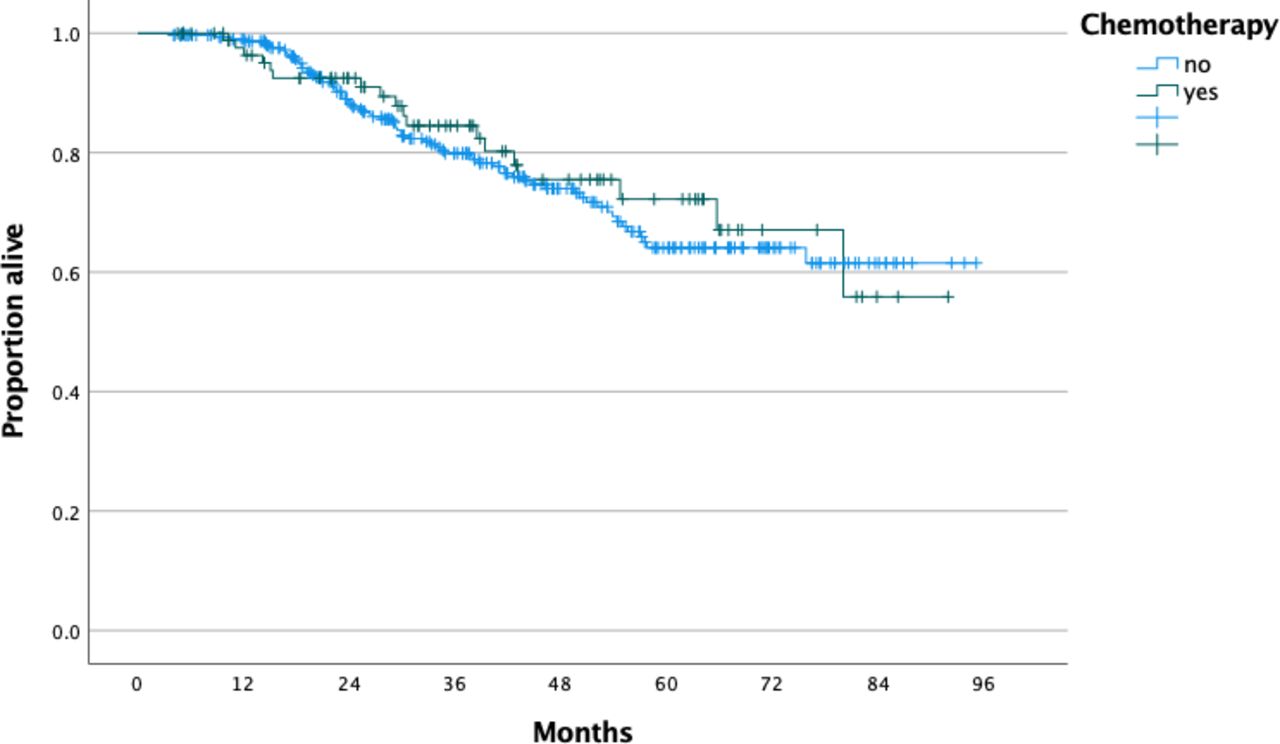
Overall survival of patients with high-intermediate risk grade 3 endometrioid endometrial cancer and lymphovascular invasion who received external beam radiation therapy stratified by receipt of chemotherapy.
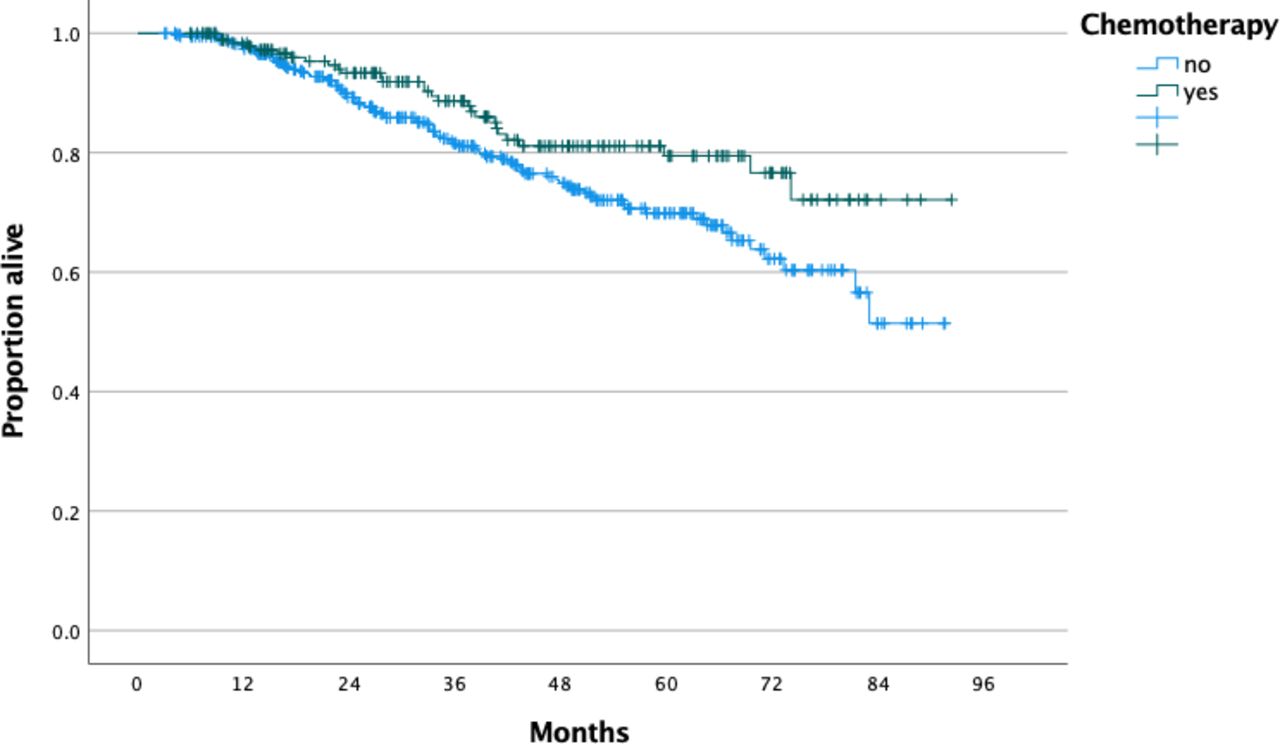
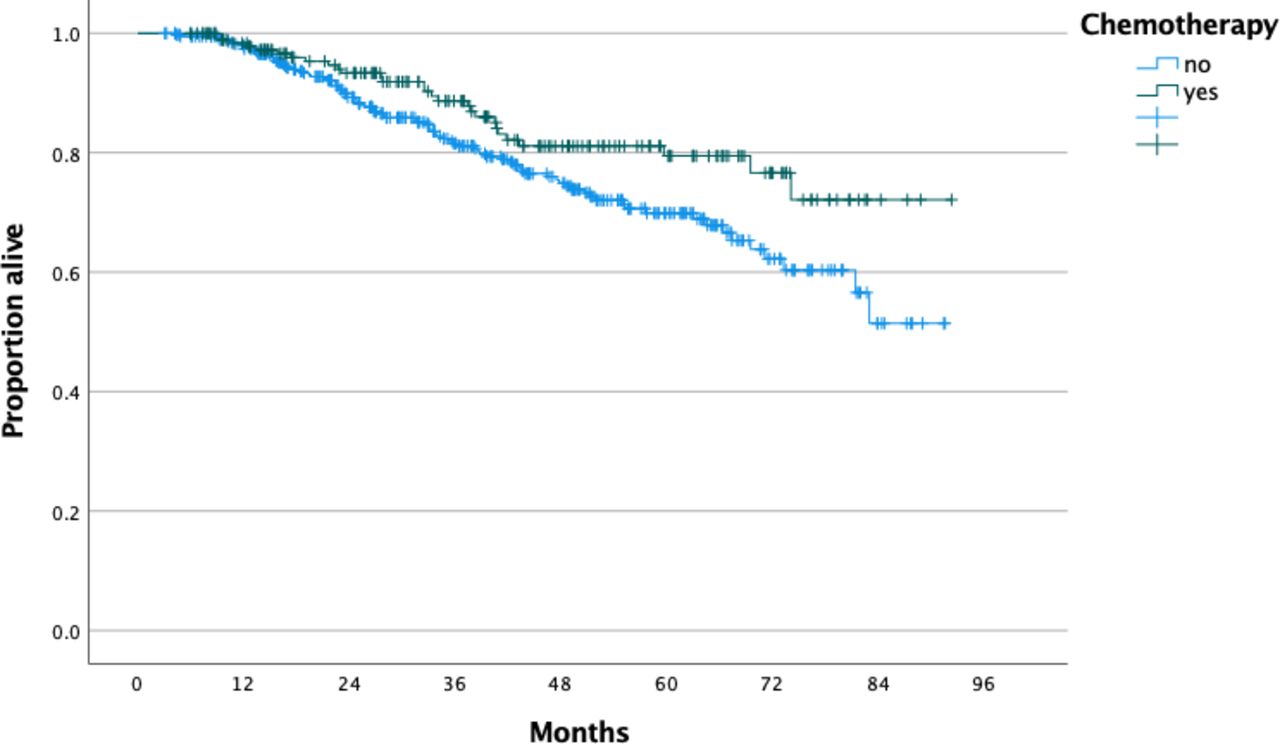
For patients who received vaginal brachytherapy alone, there was no overall survival difference between those who did and did not receive chemotherapy, p=0.23; 4-year overall survival rate 85.9% and 85.3%, respectively (Figure 3). However, after controlling for patient age, race, insurance status, presence of comorbidities, tumor grade, depth of myometrial invasion, and extent of lymphadenectomy, chemoradiation was associated with better survival compared with vaginal brachytherapy alone (HR 0.644, 95% CI 0.45 to 0.92). Following stratification by tumor grade, an overall survival benefit was found for patients with grade 3 tumors (p=0.026; 4-year overall survival rate 81.1% vs 74.9%) (Figure 4) and not for patients with grade 2 (p=0.16; 4-year overall survival rate 91.3% vs 87.1%) or grade 1 (p=0.40; 4-year overall survival rate 96% vs 92.6%) tumors. For patients with grade 3 tumors who received vaginal brachytherapy (without external beam radiation), administration of chemotherapy was associated with improved overall survival after controlling for confounders (HR 0.635, 95% CI 0.41 to 0.99). Following stratification by disease substage, there was no overall survival benefit for patients with stage IA disease (p=0.11; 4-year overall survival rate 90.7% vs 85.7%) and stage IB (p=0.54; 84.8% vs 85.3%).

Overall survival of patients with high-intermediate risk endometrioid endometrial cancer and lymphovascular invasion who received vaginal brachytherapy stratified by receipt of chemotherapy.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Overall survival of patients with high-intermediate risk grade 3 endometrioid endometrial cancer and lymphovascular invasion who received vaginal brachytherapy stratified by receipt of chemotherapy.
Discussion
Summary of Main Results
Based on data from a large hospital-based database, approximately 16% of patients with high-intermediate risk endometrioid endometrial carcinoma with lymphovascular invasion received adjuvant chemotherapy in addition to radiation therapy. The highest rate of chemotherapy utilization was observed for patients with grade 3 tumors (28.8%). Contrary to major guidelines, approximately 1 in 10 patients with grade 1 or grade 2 tumors received chemotherapy in addition to radiotherapy. The addition of adjuvant chemotherapy to radiotherapy did not improve overall survival of patients who received external beam radiation regardless of tumor grade. However, chemoradiation was associated with a survival benefit for patients with grade 3 tumors who received vaginal brachytherapy alone.
Results in the Context of Published Literature
Several studies have demonstrated that lymphovascular invasion is a negative prognostic factor for patients with early-stage endometrial cancer and is associated with a higher risk of distant relapses.5–9 16 However, when interpreting these results, performance of adequate lymph node staging is a key parameter since the incidence of lymph node metastases for patients with lymphovascular invasion is high.17 A recent analysis of the National Cancer Database demonstrated an overall incidence of lymph node metastases of 21% for patients with apparent stage I endometrioid tumors and lymphovascular invasion.17 Rate of lymph node metastases ranged from 11.4% for patients with inner half myometrial invasion grade 1 tumors to 24% for patients with outer half myometrial invasion and grade 3 tumors.17 Patients with lymph node metastases do benefit from systematic treatment with chemotherapy compared with radiation therapy alone as demonstrated by the results of PORTEC-3 randomized trial.18 While classification of endometrial cancer based on molecular signature is currently being investigated, presence of lymphovascular invasion has a negative prognostic value independent of The Cancer Genoma Atlas (TCGA) molecular signature.10
Given the relative high incidence of distant recurrences for patients with lymphovascular invasion, even in the absence of lymph node metastasis, certain authors support the utilization of adjuvant chemotherapy since radiation therapy cannot eliminate microscopic metastases outside the radiation field. In a recent survey among active members of the Spanish Society of Gynecology and Obstetrics, 47% of responders recommend the addition of systemic chemotherapy for patients with early-stage endometrial cancer in the presence of lymphovascular invasion.19 Nevertheless, to date, data from randomized trials such as PORTEC-3 and GOG-249 do not support the utilization of adjuvant chemotherapy for early-stage endometrioid tumors, regardless of tumor grade and lymphovascular invasion status.18 20 The GOG-249 trial randomized patients with high-intermediate and high-risk early-stage endometrial cancer to vaginal brachytherapy followed by three cycles of adjuvant chemotherapy or external beam radiation therapy alone.20 The trial included 444 patients with endometrioid tumors (106 grade 1, 212 grade 2, 125 grade 3 and 1 with unknown grade), and there was no difference in overall survival between the groups, while the rate of distant recurrences was comparable between the groups (HR 1.0, 95% CI 0.68 to 1.52).20 However, stratified analysis based on the presence and extent of lymphovascular invasion was not performed.
Contrary to the GOG-249 schema, in our study a significant number of patients received vaginal brachytherapy alone and had inferior survival compared with patients who had vaginal brachytherapy with chemotherapy.20 In addition, our study focused exclusively on endometrioid tumors while in the GOG-249 trial approximately 28% of patients had non-endometrioid histology (high-risk early stage). Nevertheless, in our study for patients who received external beam radiation, the addition of chemotherapy did not add an overall survival benefit, suggesting that external beam radiation is an adequate treatment option for patients with high-intermediate risk tumors. These results are in accordance with PORTEC-3 that failed to report a survival benefit for patients with stage I disease.18
In a recent multi-institutional retrospective study, Beavis et al 12 analyzed the oncological outcomes of 478 patients with high-intermediate risk FIGO stage I–II endometrioid endometrial carcinoma with lymphovascular invasion and compared the oncological outcomes of patients who did not receive adjuvant treatment (n=143), received radiation therapy only (n=232) or adjuvant chemotherapy with or without radiation (n=103).12 Similar to our study, patients who received chemotherapy were more likely to have grade 3 tumors (n=45, 43.7%) compared with those who had radiation alone (25.4%) or observation (14.7%), p<0.001.12 Among patients who experienced a relapse, the rate of distant recurrence appeared to be lower in the chemotherapy (n=10, 58.8%) group compared with those who received radiation alone (n=35, 79.5%). Similar to our results, by multivariable analysis, patients with grade 3 tumors who received chemotherapy had better progression-free survival compared with those who received radiation therapy alone (HR 0.25, 95% CI 0.12 to 0.52).12 On the other hand, after controlling for confounders, chemotherapy administration was not associated with superior overall survival (HR 1.07, 95% CI 0.75 to 1.50).12
In another small retrospective study, among 29 surgically staged patients with stage I–II endometrioid carcinoma and lymphovascular invasion, 22 patients received adjuvant chemotherapy alone while seven did not receive any adjuvant treatment.21 Only three (13.6%) patients had recurrence in the chemotherapy group (two local and one distant relapse), while three (42.8%) distant recurrences were noted in the observation-only group.21 Matsuo et al 22 performed a case control study and included 70 patients with stage I–III endometrial carcinoma and lymphovascular invasion, 60% of whom received adjuvant chemotherapy (with or without radiation therapy).22 The authors demonstrated an increased risk of distant recurrence among patients with deep or extensive lymphovascular invasion only among patients who did not receive chemotherapy.22
Strengths and Limitations
A major strength of our study was the inclusion of a large number of patients derived from a multi-institutional database that reflects real work practice. In addition, we opted to include patients who underwent lymphadenectomy given the high risk of occult metastases and performed a stratified analysis based on the type of radiation treatment received. However, several limitations should be noted. First, given the absence of central pathology review, possible tumor and staging misclassifications cannot be excluded. Also, in the National Cancer Database lymphovascular invasion is reported as a binary outcome (present or absent) and is not coded using a three-tier system (absent, focal and substantial). In addition, while the original GOG-99 criteria included invasion of the outer third of myometrium since the exact depth of myometrial invasion is not available, we opted to use invasion of the outer half of myometrium (stage IB) similar to GOG-249 and a prior National Cancer Database analysis.15 Moreover, no data on tumor recurrence were collected, precluding us from analyzing differences in progression-free survival and patterns of relapse while specific details on the radiation therapy and chemotherapy regimen administered were not available. Lastly, unmeasured patient characteristics such as functional status and individual treating physician preferences may have influenced the decision to administer adjuvant chemotherapy.
Implications for Practice and Further Research
In a large cohort of patients with high-intermediate risk endometrioid endometrial carcinoma with lymphovascular invasion, the administration of adjuvant chemotherapy was associated with a survival benefit for patients with grade 3 tumors receiving vaginal brachytherapy. It should be underlined that two randomized trials (GOG-249 and PORTEC-3) failed to demonstrate a survival benefit with the addition of chemotherapy to adjuvant radiotherapy for patients with early-stage disease, but the patient population was heterogeneous. While our study examined a more homogeneous cohort (endometrioid histology only with lymphovascular invasion), given its retrospective nature the results should be regarded as hypothesis generating. Ad hoc analysis of GOG-249 could further clarify the role of adjuvant chemotherapy for patients with lymphovascular invasion and early stage disease. Moreover, further studies incorporating molecular data could identify a patient population with early-stage endometrial cancer that mostly benefits from the addition of chemotherapy to adjuvant radiation therapy. Potentially, patients with p53 mutations would most benefit from the addition of chemotherapy as demonstrated in a sub-analysis of the PORTEC-3 study.23
Conclusions
Approximately 16% of patients with high-intermediate risk FIGO stage I endometrial cancer received adjuvant chemotherapy in addition to radiation therapy. In the present cohort, adjuvant chemotherapy was most commonly administered to patients with grade 3 tumors and within that group was associated with an overall survival benefit only for those who received vaginal brachytherapy.
Data availability statement
Data may be obtained from a third party and are not publicly available. Data obtained from American College of Surgeons.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors DN: conception, data acquisition, data management, statistical analysis, critical analysis, drafting/final editing, guarantor. JO, EMK, AFH, LC, SK, RLG, MM: critical analysis, drafting/final editing. NL: supervision, critical analysis, drafting/final editing. All authors contributed significantly.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None related to this study. RLG: medical monitor for CAPRI trial by Astra Zeneca. AFH: GSK research fund, GSK advisory board, Honoraria: Axess ovarian cancer lecture.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.