Article Text

Abstract
Background With the continuous improvement of people’s material living standards, the consumption of alcoholic beverages is increasing. Alcohol dependence caused by alcohol addiction has become a widespread concern in society. As the brand-new medical and health model created by the modern biomedical technology revolution and the information technology revolution, mobile health has been used more and more widely in the field of medical health with the characteristics of convenience, rapidity and generalisability. With the general use of the social software WeChat, it is feasible to implement mobile health on the WeChat platform.
Aim We aimed to explore the clinical effect of WeChat platform used in the cognitive behavioural therapy (CBT) on the maintenance period of alcohol dependence and addiction.
Methods Seventy alcohol-dependent patients in the withdrawal maintenance stage admitted into our hospital were randomly divided into the CBT on WeChat platform group (the experiment group, n=35) and the general clinical treatment using sertraline group (the control group, n=35) with block randomisation grouping. They were evaluated with the Severity of Alcohol Dependence Questionnaire (SADQ-C) before the treatment, at the end of the fourth week, at the end of the eighth week and at the end of the twelfth week of treatment. In addition, Zung’s Self-Rating Anxiety Scale (SAS) and Self-Rating Depression Scale (SDS) were employed to evaluate the degree of anxiety and depression of the two groups.
Results The SADQ-C, SAS and SDS scores of the two groups after treatment decreased markedly compared with those before treatments, and the differences were statistically significant. Between-group comparison: the SADQ-C scores of the experiment group at the end of the fourth, eighth and twelfth weeks were lower than those of the control group, and the difference was statistically significant, which indicated that the score reduction in the experiment group was larger than that in the control group. The SAS and SDS scores of the experiment group at these time points were not significantly different from those of the control group, which indicated that these two treatment methods were comparable in treating patients’ anxiety and depression.
Conclusion The CBT intervention using WeChat may improve the subjectively reported severity of alcohol dependence of patients who had completed detoxification. It is conducive to prevention of relapse, and is convenient for patients. It is worthy of clinical application and further study.
- Wechat platform
- alcohol dependent
- cognitive behavioral therapy
- effectiveness
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Alcohol dependence (AD) is a chronic recurrent mental disorder. Consuming a large amount of alcohol over a long period of time can cause impairments in individual parts of the whole body, and it can also harm families. In addition, AD has also become an important factor that affects the stability of society. AD has become the third most common mental disorder, after schizophrenia and mental retardation.1 Therefore, rational treatment for AD has become the focus of much research.
Currently, mobile health is being promoted and used continuously. Research institutions around the world are gradually focusing more on mobile medical technologies related to mental illness.2 As WeChat, the social software, is widely used in China, it is feasible to implement mobile health on the WeChat platform.
Cognitive behavioural therapy (CBT) can rectify the wrong and irrational cognitions of patients with AD, thereby reducing their rate of relapse. Multiple studies3 4 have shown that mobile health can perform psychological interventions on patients and it has certain effectiveness. The present study explored CBT for patients with AD in the withdrawal maintenance stage on the WeChat platform and observed its effectiveness.
Clinical data
General data
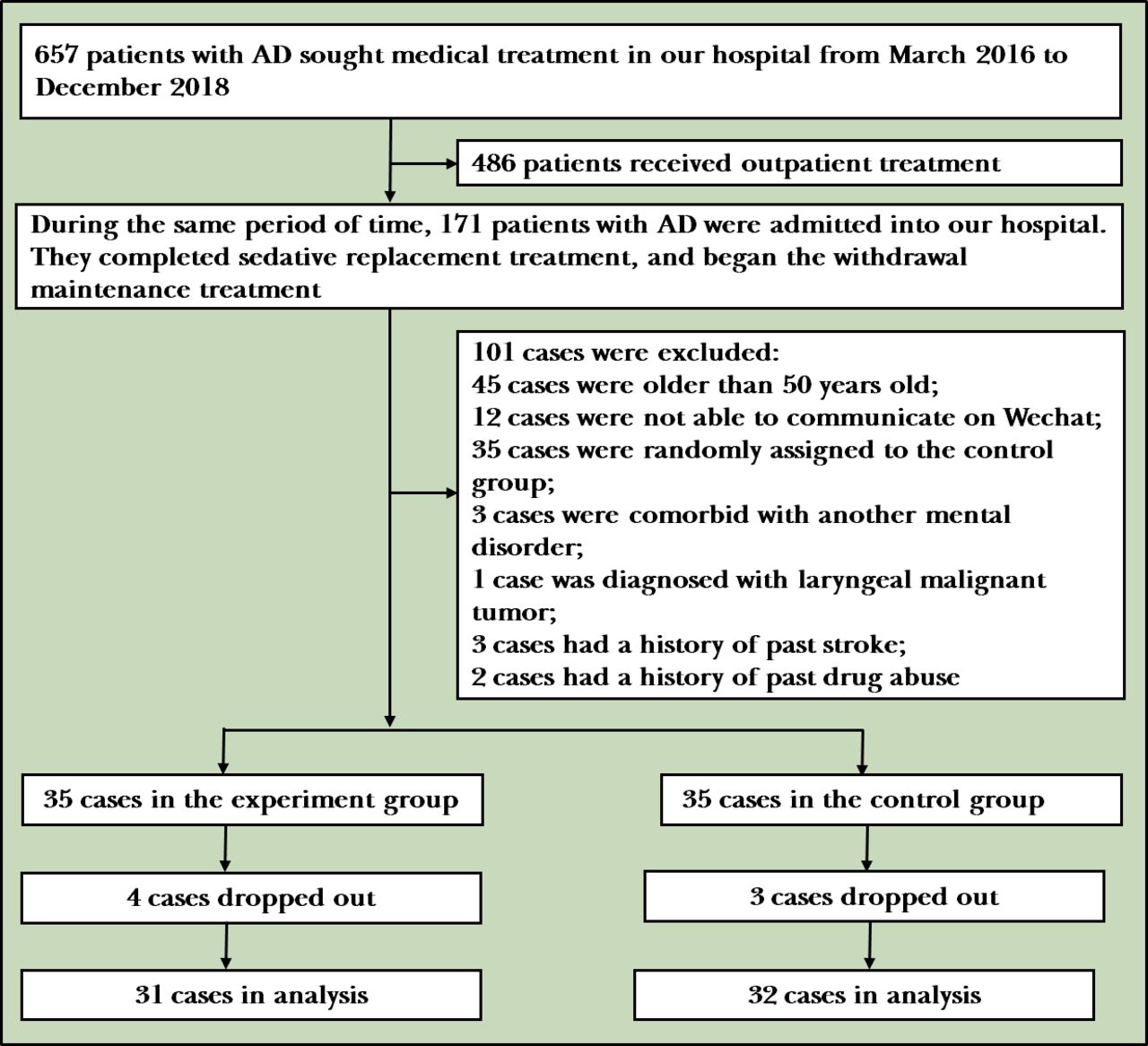
There were 171 patients with AD in total, admitted into our hospital from March 2016 to December 2018. During their hospitalisation, they had completed the sedative replacement therapy and entered the withdrawal maintenance stage,5 (ie, patients have passed the withdrawal state with stable vitals, and the main purpose of this stage is detoxification). Among these patients, 70 of them met the inclusion criteria as subjects (67 men and 3 women). All patients who enrolled were divided into a CBT on WeChat platform treatment group (the experiment group) and a general clinical treatment using sertraline group (the control group) with 35 subjects in each group (figure 1).
{kind=link}
Flowchart of the study. AD, alcohol dependence.
There were 34 men and 1 woman in the experiment group with the mean age being 41.4 years old. Their years of drinking ranged from 5 years to 26 years with the mean being 17.6 years. Their daily alcohol consumption was equivalent to pure alcohol 131–346 g with the mean being 231 g.
The education level of 28 subjects in the experiment group was junior high school or above, and that of 7 of them was elementary school. There were 33 men and two women in the control group with the mean age being 42.5 years. Their years of drinking ranged from 5 years to 28 years with the mean being 18.3 years. Their daily alcohol consumption was equivalent to pure alcohol 124–360 g with the mean being 238 g. The education level of 29 subjects in the control group was junior high school or above, while that of 6 of them was elementary school. The general data of two groups were not significantly different from each other after comparisons.
Inclusion criteria and exclusion criteria
Inclusion criteria: (1) patients who met the diagnostic criteria for AD in the International Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10);6 (2) patients whose ages ranged from 20 years to 50 years; (3) patients who could communicate on WeChat; (4) patients who had completed the sedative replacement therapy and begun the withdrawal maintenance therapy; (5) patients with no contraindications related to the use of sertraline; (6) patients whose legal guardians had signed the consent forms for the present study. Exclusion criteria: (1) patients with other mental disorders; (2) patients with a history of abusing other substances; (3) pregnant and lactating patients; (4) patients with major medical conditions in the central nervous system and cardiovascular system.
Dropout criteria
Dropout criteria: patients who had other complications during treatment; patients whose legal guardians withdrew their consent; patients who were considered necessary to drop out of the study based on researchers’ collective discussion.
Methods
The present study employed block randomisation grouping with the time of seeking treatment as the grouping factor, and divided groups by grouping every five patients who were adjacent in terms of the time of the visit as a block. A parallel controlled trial was conducted on 70 patients with AD who were divided into CBT on the WeChat platform treatment group (the experiment group, n=35) and general clinical treatment with sertraline group (the control group, n=35). Every patient in both groups was added as WeChat friends. Tasks that every member should manage to do were: registering and filling out consent forms with real names; patients in the experiment group completing CBT treatment and evaluation scales; patients in the control group being available to complete an intake and complete evaluation scales. Researchers were forbidden from sending information irrelevant to the treatment to patients in both groups and they were instructed to protect the patients’ privacy.
Measurement tools
The Severity of Alcohol Dependence Questionnaire (SADQ-C)7 was employed to evaluate the degree of patients’ AD before treatment, at the end of the fourth week, at the end of the eighth week and at the end of the twelfth week of treatment. Zung’s Self-Rating Anxiety Scale (SAS) and Self-Rating Depression Scale (SDS)8 were employed to evaluate patients’ degrees of anxiety and depression.
SADQ-C was used to evaluate the craving for drinking of patients with AD syndrome. This scale has relatively good reliability and validity in studies both inside China and internationally.7 This scale includes 20 question items, and every item is rated on a scale of 4 levels: 0=almost never, 1=sometimes, 2=often, 3=nearly always. A SADQ-C score of more than 30 indicates severe AD, a SADQ-C score between 16 and 30 indicates moderate AD, and a SADQ-C score below 16 indicates mild or no AD.
As common evaluation tools in China, SAS and SDS are characterised with large capacity, comprehensive reflection of symptoms and accurate depiction of subjects’ self-conscious symptoms, and their high validity and reliability have been demonstrated.9 SAS and SDS include 20 question items, and every item is rated on a four-point scale: 1=a little of the time, 2=some of the time, 3=good part of the time, 4=most of the time. In SAS, 15 items are rated in the forward direction of 1–4, and 5 items are rated in the backward direction of 4–1. In SDS, 10 items are rated in the forward direction of 1–4, and 10 items are rated in the backward direction of 4–1. The total score is the summation of the scores of 20 questions, and the standard score is the integer of the total score multiplied by 1.25. The scoring standards: the cut-off value of SAS is 50: 50–59 indicating mild anxiety, 60–69 indicating moderate anxiety, 70 or above indicating major anxiety. The cut-off value of SDS is 53: 53–62 indicating mild depression, 63–72 indicating moderate depression and 72 or above indicating major depression.
Methods of measurement
SADQ-C, SAS and SDS were made into questionnaires. SADQ-C, SAS and SDS were sent to patients to measure their status by clinicians via Wenjuanxing software on WeChat. The measurement was conducted with questionnaires and completed by patients independently.
Cognitive behavioural therapy
The therapists who performed CBT are qualified with psychiatrist licenses and national vocational certificates of second-level psychological counsellors. CBT was conducted as a group therapy on the WeChat platform. The whole session was conducted by one therapist.
The CBT treatment procedure was as follows. First, the therapist built a good therapeutic alliance relationship with patients on the WeChat platform. The therapist started with fully accepting, understanding and supporting patients on the basis of care, understanding and effective communication, and added patients as WeChat friends. The therapist then achieved a comprehensive understanding of patients’ medical history and psychosocial factors, including family environments, work, study and life experience. Meta-analyses of adult psychological therapy studies10 indicate that there is a continuing moderate correlation between therapeutic alliance and treatment results, and that the influence of the therapeutic alliance is consistent in different types of psychological therapies. For the cognitive interventions the therapist understood the deep causes of patients’ AD by using Socratic questions, and helped them understand the physical mechanism of AD, the metabolic process of alcohol in human bodies and the harm of alcohol to the human body.11 The therapist conducted deep psychological interaction with patients, and employed individualised methods to help patients correct their series of negative cognitions towards AD and alcohol beverages, improve their ability to adjust, change their cognitive patterns and face reality with rational emotions and faith based on the specific circumstances of each patient. Cognition has a guiding role in behaviour, so cognitive intervention is the key intervention of this treatment. Behavioural interventions were conducted by targeting patients’ negative cognitions, and this included turning family members into patients’ supervisors and supporters by communicating with them, building a good family-society support system, and eliminating the creation of an alcohol drinking atmosphere. When patients wanted to drink alcohol, they contacted the therapist in time. The therapist encouraged patients to cooperate with the treatment and overcome the disease by communicating with them, and changed their focus of attention by rewarding them spiritually or materially based on their preference. The therapist conducted appropriate amounts of relaxation training and self-control enhancing methods to alleviate anxiety and depression, and to correct alcohol-drinking behaviour. Finally, the therapist evaluated the target gains, handled the end of treatment, communicated with patients to prevent relapses, and achieved the ultimate goal by applying psychological principles.
The CBT described above persisted for 12 weeks, and was conducted 12 times in all with an average frequency of once a week. Every session lasted about 1–1.5 hours, and the specific length depended on the task of every session. Every session’s content and practice were recorded accordingly.
Medicine treatment
The medicine treatment group was given sertraline with a daily dose of 50–100 mg. The average dose was 75 mg/day. The maintenance treatment persisted for 12 weeks.
The standards for effectiveness
According to the SADQ-C reduction rate evaluating effectiveness of the treatment standard the clinical effectiveness of treatment on patients with AD was evaluated by a reduction rate ≥50% indicating recovery, ≥35% indicating marked improvement, ≥20% indicating improvement and below 20% indicating invalidity.
Statistical methods
SPSS V.17.0 was employed to conduct the analysis. For continuous variables, the overall difference of two groups’ SADQ-C scores, SAS scores and SDS scores at different time points were compared with repeated measures analysis of variance, and comparison analyses were conducted to compare whether the differences of scores’ changes at the baseline, the fourth week, the eighth week and the twelfth week of the treatment were significant or not. A value of p<0.05 indicates a statistically significant difference.
Results
Dropout conditions
During treatment, 7 out of 70 patients with AD in the withdrawal maintenance stage of two groups dropped out with a dropout rate of 10%. Among them, four came from the experiment group and three came from the control group. There were 31 in the experiment group and 32 in the control group who actually completed the treatment. The effective collection rate of the scales was 90%. The data of patients who dropped out were not included in the analysis (table 1).
Statistical comparisons of two groups’ SADQ-C scores’ mean (SD) at different stages of the treatment
Analysis on the effectiveness of treatment
As shown in table 1, the changes in SADQ-C scores of the experiment group over the treatment stage were significantly different from those of the control group, and the difference had statistical significance (Fbetween-group =5.23, p=0.026, Ftime =162.17, p<0.001, Ftime*between-group =9.38, p=0.001). The post hoc analyses of repeated measures analysis of variance showed that the changes in SADQ-C scores of the two groups before the treatment and at the end of the fourth week were not significantly different from each other (Ftime between-group =0.05, p=0.82), and it had no statistical significance; while the changes in SADQ-C scores of two groups at the end of the eighth week (Ftime*between-group =4.65, p=0.03) and at the end of the twelfth week (Ftime*between-group =5.91, p=0.02) were markedly different from each other, and it was statistically significant. In the experiment group, there were 14 cases of recovery, 7 cases of significant improvement, 5 cases of improvement and 5 cases were invalid. Effectiveness of treatment includes recovery, significant improvement and improvement. Therefore, in the experiment group, the rate of effectiveness was 83.87% and the rate of recovery was 45.16%. On the other hand, in the control group, there were 7 cases of recovery, 8 cases of significant improvement, 6 cases of improvement and 11 cases were invalid with a rate of effectiveness of 65.62% and a rate of recovery of 21.87%.
As shown in tables 2 and 3, both SAS and SDS scores in two groups decreased compared with those before the treatment. According to the statistical comparison of the two groups’ SAS scores at the end of the fourth week, at the end of the eighth week and at the end of the twelfth week and before the treatment, the values of F were 5.47, 259.25 and 118.70, respectively, and the values of p were 0.023, <0.001, and <0.001, respectively, and the difference was statistically significant. According to the statistical comparison of two groups’ SDS scores at the end of the fourth week, at the end of the eighth and at the end of the twelfth week and before the treatment, the values of F were 13.64, 182.23 and 163.05 respectively, and the values of p were <0.001, <0.001 and <0.001, respectively, and the difference was statistically significant. As the treatment time prolonged, patients’ SAS and SDS scores decreased (the values of Ftime were 42.18 and 65.38, p<0.001). According to the overall SAS and SDS scores of two groups (the values of Fbetween-group were 1.04 and 1.44, and the values of p were 0.36 and 0.23; the values of Ftime*between-group were 1.04 and 0.85, and the values of p were 0.35 and 0.43), the difference was not significant. At the same time point, SAS and SDS scores of the two groups were not significantly different from each other (the values of p were all above 0.05). Therefore, after CBT and pharmacological treatments, the anxiety and depression of the two groups improved and the effectiveness of treatment was good. In addition, after CBT and pharmacological treatments, the incidence of anxiety and depression in the two groups reduced significantly and the effectiveness of treatment was the same.
Comparisons of means (SDs) of SAS scores of the two groups at different stages of the treatment
Comparisons of means (SDs) of SDS scores of the two groups at different stages of the treatment
The main adverse reactions in the pharmacological treatment group were three cases of diarrhoea and indigestion, one case of light-headedness, one case of tremor, two cases of insomnia and one case of nausea. All the symptoms improved after the treatment.
Discussion
Main findings
The present study found that after two groups of patients with AD in the withdrawal maintenance stage who either received 12 weeks of CBT or general clinical treatment of sertraline were contacted via the WeChat platform, their SADQ-C, SAS and SDS scores improved after the treatment, but the scores of the patient group were better than those of the control group. The effectiveness of the CBT treatment is comparable to that of general clinical treatment of setralline on the patients with anxiety and depression.
WeChat was employed to conduct general and deep communication with patients and build a relatively reliable therapeutic alliance, thereby changing patients’ negative cognitions and achieving the goal of quitting drinking. The CBT intervention given by WeChat may improve the subjective reporting severity of alcohol-dependent patients who had completed detoxification. It will be conducive to prevention of relapse, and will bring convenience to patients. Therefore, it will be convenient to contact patients from the two groups, and the compliance of patients could be better with a low dropout rate. This result is in accordance with the report by McTavish.12
Limitations
In the present study, we analysed the data of 63 patients who received 12 weeks of CBT or general clinical treatment of medicine. Since we did not collect enough data on the long-term effectiveness of treatment of patients, this aspect was not analysed. This topic should be explored in future research. The time range in the present study is 12 weeks which is the time range of the general paradigm. However, if the observed time of the study is prolonged, it might affect the effectiveness of treatment, which should be observed further in the future. In the present study, the selection of treatment drugs in the control group is not the preferred treatment, which may have a certain impact on the results. In addition, the limited sample size might influence the results, and should be expanded in future studies.
One of the possible reasons for the difference between the effectiveness of treatment in the two groups may be that sertraline only alleviates patients’ anxiety and depression instead of correcting their maladaptive cognitions concerning AD. Since it takes a gradual process to modify patients’ maladaptive cognitions, the difference between the two groups is statistically significant after long-term treatment (at the end of the eighth week).
Patients with AD have many psychological problems, and CBT can improve their negative cognitions, build positive thinking styles and alleviate their anxiety and depression. However, traditional CBT needs to be conducted in an environment where therapists and patients are face to face and alone. This lacks continuity of treatment. The effectiveness of treatment may be affected by this shortcoming. Currently, mobile apps are widely used for implementing CBT in the area of mental health.
Implications
In the era of mobile networks, various social platforms can be applied for in-depth communication with patients and to implement various treatment methods for therapeutic purposes, especially for patients with dependence on psychoactive substances13 and internet games addiction.14 15 Thornton et al examined the feasibility of recruiting participants for research on addiction via Facebook in 2016, in which they captured a great proportion of people with high-severity substance use and mental health issues. 16 Substance dependence is referred to as the chronic and recurrent disease of abusing a kind of addictive substance. In our study, WeChat is also one of the social platforms which can be used effectively in the addiction study. Patients with AD crave alcohol strongly. Studies about their attention bias indicate that they have significant attention bias which is manifested in being more focused on selectively processing alcohol-related clues, and this may abnormally activate the reward centre. We change patients’ attention bias with CBT to achieve the goal of recovery. Theories of the craving mechanism in AD syndrome state that alcohol is a negative reinforcement of the central nervous system to the reward system. In the meantime, patients with AD syndrome have incorrect cognitions about alcohol, and this irrational cognition is one of the factors causing the strong craving for alcohol; correcting these wrong and irrational cognitions can reduce the craving for drinking. This is also the basis of treating AD with CBT.
In summary, conducting CBT on the WeChat platform facilitates communication and interaction with patients, and has the following strengths:
Enhancing mental health awareness: patients with AD can be taught to use information resources to seek help in time by receiving mental health related messages on their phones to improve their understanding about the symptoms, treatments and prevention of AD.
Reducing stigma about AD: in China, the public still has a certain level of stigma towards AD, and many patients and their family members are unwilling to seek medical help or have never sought help, which causes the delay in treating this syndrome.15 Implementing CBT on the WeChat platform can let patients consult and seek treatments on their private mobile phones, so it can effectively decrease the stigma and the influence of related obstacles on their medical treatment. According to a public survey in Australia, 76% of the population is willing to use phones for monitoring mental health and for self-regulation.17
Improving the compliance of patients with AD and reducing their rate of relapse: the poor compliance and high rate of relapse of patients with AD have been troubling doctors and family members, but they can track the changes in patients’ conditions and treatments in real time and send timely reminders via mobile regulation platforms in the future. This will help more patients maintain good compliance and reduce the rate of relapse.
References
Jing Chen obtained her bachelor′s degree in clinical medicine from the Yun Yang Medical School, Hubei Province, China in 2001. Since 2004, she has been working as an associate chief physician in the Psychosomatic Department of the Third People’s Hospital of Huzhou City, China. Her research interest includes geriatric psychology.

Footnotes
Contributors CJ: designed the study and wrote the draft. QMC and LM: collected and analysed the data. SCH and TWL: collected the data.
Funding Huzhou Science and Technology Bureau (2016GYB03).
Competing interests None declared.
Patient consent for publication Informed consent was obtained from all patients in the study
Ethics approval Ethics Committee of Huzhou Third People's Hospital (ID number: (2016) ethics approval No. 7) in Zhejiang Province.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.