Article Text

Abstract
Background Feedback is an effective pedagogical tool in clinical teaching and learning, but the actual perception by learners of clinical feedback is often described as unsatisfactory. Unlike assessment feedback or teaching sessions, which often happen within protected time and space, clinical feedback is influenced by numerous clinical factors. Little is known about clinical teachers’ motivations to provide feedback in busy clinical settings. We aimed to investigate the motivations behind feedback being given in emergency departments (EDs).
Methods A qualitative analysis of semi-structured interview data was conducted between August 2015 and June 2016. Eighteen attending physicians were purposively sampled from three teaching hospital EDs in Taiwan. Data were thematically analysed, both inductively (from the data) and deductively (using self-determination theory (SDT)). Themes were mapped to the different motivation types identified by the SDT.
Results and discussion Despite working in busy clinical settings, Taiwanese ED clinical teachers reported being motivated to provide feedback when they felt responsible for their learners, when they understood the importance of feedback (patient safety and partner building), or simply because they were committed to following a tradition of passing on their clinical knowledge to their juniors. Suggestions to facilitate the internalisation of external motivations are proposed.
Conclusions In this qualitative study, motivations for clinical feedback were identified. Although the motivations are mostly extrinsic, the elicitation of internal motivation is possible once true satisfaction is fostered during the feedback-giving process. This understanding can be used to develop interventions to enable clinical feedback to be provided in a sustained manner.
- emergency department
- qualitative research
- education, teaching
Data availability statement
Data in its original language are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this subject
Feedback is an effective pedagogical tool in the emergency or resuscitation settings, but is often described as unsatisfactory.
Clinical teachers are often faced with competing demands from their clinical duties.
Little is known about the motivations that drive faculty members to provide feedback in a very busy clinical setting.
What this study adds
In this qualitative study in Taiwan, we found that faculty members in the emergency departments are motivated to provide feedback when they feel a responsibility towards their learners, when they understand the importance of feedback, or simply because they are committed to follow a tradition of passing on their clinical knowledge to their juniors.
Introduction
Feedback, often defined as ‘Specific information about the comparison between a trainee’s observed performance and a standard, given with the intent to improve the trainee’s performance’, is recognised as an essential element in clinical education.1 2 Learners identify their strengths and weaknesses through feedback given by their instructors,3 with both positive and negative feedback acting as potent stimuli that motivate learners and improve their performance.4 Feedback has also been regarded as an effective pedagogical tool in the emergency or resuscitation settings, where timely and appropriate feedback enhances medical knowledge and clinical skills in the emergency department (ED).5 6 However, the busy environment and time constraints that exist in the clinical settings do pose challenges to clinical teachers when giving feedback.7
In clinical education, a large proportion of feedback is integrated as an essential component of formative assessments. This formal assessment feedback is usually provided within protected time and space, and it has become a norm for both the provider and the receiver to engage in the process of feedback exchange. Another approach is feedback that is given dynamically in the clinical setting, where learners receive feedback after their patient encounters, after their teachers have reviewed their medical or drug prescription decisions, or after their overall clinical performance has been examined by their teachers over a period of time. This kind of clinical feedback is sometimes informal, and often incidental and influenced by many clinical factors.8 Previous research suggests that ED clinical teachers carefully select their moments for feedback provision while ensuring patient safety at the same time. Furthermore, there may be a threshold at which feedback is provided, and the decision is dependent on how teachers weigh the observed performance of the learner against the severity of the clinical situation.8
Little is known about the motivations that drive faculty members to provide feedback in a busy clinical setting, especially when they are faced with competing demands from their clinical duties, and when there are often no clear regulations as to the frequency or duration of clinical feedback that should be given. Most clinical teachers initially begin as trainees, and obtain opportunities for supervision gradually, sometimes unnoticed. At times, clinical teachers are also presented with challenges between prioritising feedback provision and their clinical duty.9 The literature regarding the motivations of clinical teachers to teach have demonstrated that the underpinnings of their external motivations are usually derived from their own systems expectations and personal values, and their desire for knowledge sharing.10 11 However, there exist differences between planned teaching sessions and incidental clinical feedback. Clinical feedback is often situational, characterised by unprotected time and space, the need for direct observation in the clinical setting, and having to deal with the consequences of negative feedback being provided. The above characteristics make clinical feedback unpredictable, and might lead to the practice of feedback being sacrificed at times.
According to Ryan and Deci,12 ‘Motivation concerns all aspects of activation and intention, involving energy, direction and persistence’. Among the several contemporary theories of motivation, the evidence behind the self-determination theory (SDT) has been gaining ground in the field of education.13 The application of SDT and its implications in clinical education settings has been demonstrated in previous studies.14 15 Developing an understanding of the factors that drive faculty members to give feedback, would enable the formulation of strategies to allow and encourage clinical teachers to provide feedback. The aim of this study is to understand the motivation for feedback provision in the context of a day-to-day, real-life ED clinical settings.
Methods
Study design and setting
This is a secondary analysis of qualitative data collected from semi-structured individual interviews looking at barriers to feedback in the clinical setting.8 Patients and the public were not involved. The study was conducted between August 2015 and June 2016 at the EDs of three teaching hospitals of various sizes in Northern Taiwan: a tertiary medical centre with a 3600-bed capacity (site A); a district hospital with a 300-bed capacity (site B) and a regional hospital with a 1000-bed capacity (site C). The total number of faculty members (clinical teachers) across these three branches is 65 attending physicians (52 male).
Participants and data collection
The participants were recruited through purposive sampling. They were selected to be representative of the seniority, gender, number of physicians at each ED site, and the frequency of clinical shifts assigned with residents at the study sites. Written consents were obtained from all the participants. A total of 18 interviews were completed, at which point data saturation was reached. Eighteen attending physicians consisted of 11 males and 7 females with between 5 and 20 years of clinical experience. The proportion of females among the participants were slightly disproportionate compared with the underlying population, which was a decision in order to gain variability of experiences and perspectives around the topic of clinical feedback. The detailed demographic results of the participants are listed in table 1.
Demographic results of participants (n=18)
One-on-one, semi-structured interviews were conducted with the participants using predetermined interview guides (see online supplementary file 1).8 This type of interview was selected in order to collect in-depth qualitative data in a structured manner while allowing the room for flexibility and while maintaining privacy.16 The interviews took place in a private meeting room during the participants’ off-duty hours and were conducted in Mandarin by an experienced researcher with a nursing and qualitative research background. The interview data were recorded, transcribed and managed via the computer-assisted qualitative data analysis software ATLAS.ti. Transcripts were reviewed by the participants for its correctness before analysis.
Supplemental material
Data analysis
Thematic analysis was used for data analysis following the guides provided by Braun and Clarke.17 Coding began shortly after the interviews and proceeded concurrently. A total of four researchers participated in the initial coding process. Two researchers looked through the data separately to identify quotations that illustrated the act of motivation. The quotations were then consolidated to be jointly analysed. SDT12 18 was used deductively, where the motivations were divided into ‘extrinsic’ or ‘intrinsic’ motivations. According to SDT, motivation is categorised as intrinsic if an activity is performed because of the genuine enjoyment or satisfaction that is derived from it. Extrinsic motivations on the other hand are actions undertaken to achieve a separable outcome or when driven by an external factor. Extrinsic motivation can be further divided into four categories according to their types of regulation and relative autonomy: external regulation, introjected regulation, identified regulation and integrated regulation (figure 1).19 The four types of external motivations are explained in figure 2, using the act of running for illustration. From the quotations, the major themes were developed, and the categorisation of the quotations was thereafter done by consensus. Internal and external member checks were done to ensure the validity of this study.

Illustration of the self-determination theory and corresponding themes mapped accordingly.

The four categories of external motivations illustrated using the act of running.
Patient and public involvement
No patients involved.
Results
Four themes were identified according to their various degrees of self-determination: (1) responsibility; (2) patient safety; (3) partner building and (4) a tradition of commitment. These themes were mapped to the categories of motivations under the SDT and summarised in figure 1. Illustrative quotes are used where appropriate and are labelled as follows: (gender; participant number). Square brackets are used for contextual additions.
Responsibility
Several participants explained that they gave feedback because they saw it as being part of their responsibilities in performing the duties that were required of them as faculty members in teaching hospitals. It is mandatory that teaching hospitals provide clinical education to junior learners, as such faculty teaching is assessed regularly based on anonymous reviews. Further the participants reported that one of the performance indicators of their faculty income is dependent on the ratings they receive from the learners. As feedback is integral to clinical teaching, the various settings in which faculty members come into interaction with learners require feedback to be provided. For instance, feedback is integrated as a mandatory part of the formative assessments that are performed on a daily basis. Some physicians stated quite straightforwardly:
I work in a teaching hospital, … I think that giving them feedback is part of my job in a teaching hospital, but as to how much time I should spend [on giving feedback], that is another matter. (M13)
When they come to [work in] the emergency department, they come in the role as a learner, so it would be your responsibility [to give them feedback]. (M15)
Feedback provision is therefore construed as a responsibility or obligation to the job function and represents externally sourced motivation (figure 1). However, whether regulation is external or introjected depends on whether the rewards and punishments are externally (the income) or internally (being regarded as a good teacher) regulated.
Patient safety
There were also clinical teachers who viewed providing feedback as enhancing the management of clinical workflow, in that while learners are paired with supervising attending physicians for clinical training, they also act as extra pair of hands in the ED. As such, there is utility in providing feedback to the learners not only because it is innately useful for their learning but from our participants’ perspectives, better-equipped learners would enhance the productivity in the ED, while also improving patient safety and the quality of care:
If [the residents’] patients develop any complications during this shift, it is my responsibility, so if I want to be able to get off work knowing that the patients are safe, I have to keep giving [the residents] feedback and reminding [them of what to do]. (M16)
So if you do not give them timely feedback, they might keep making the same mistakes, and might think they are alright, not only is this bad for the residents, it is also bad for the patients. (M01)
We mapped this theme to the concept of identified regulation (figure 1) because the clinical teachers have internalised the importance of providing feedback in how it could produce beneficial outcomes, in this instance, in improving the healthcare quality and patient safety in the ED.
Partner building
Participants in our study explained that a unique element of emergency medicine practice is teamwork. Teamwork is necessary because resuscitations cannot be done by a single person, and because patients might require long stays which also necessitate conscientious handovers. Patients would often be managed by several physicians of different levels of experience during their ED stay. Participants explained that learners, especially residents, are therefore regarded as partners and may become future faculty members to whom patients will be handed over. Providing feedback has a functional purpose during clinical training because this conversation will enhance the team dynamics:
We train our residents because we hope that in future they will become our good work partners. … If I do not teach them properly now, it will be difficult to handover in the future. …. (F04)
…when you give feedback, they will become better, and when they get better, the whole team will also become better.…. (M13)
This third theme would also fall under identified regulation as the participants recognised and internalised the importance of giving feedback in how it helps to form stronger partnerships.
A tradition of commitment
In Chinese culture, colleagues are often referred to as seniors or juniors instead of calling names, in reciprocal relationships whereby seniors are accorded respect and juniors are nurtured: particularly so in certain professions, such as in the military or medicine. Most participants reported that because they received feedback from their seniors in the past, they were in turn motivated to do the same for their juniors:
Because in the past our seniors taught us, so of course we have to continue to pass these things on… (M12)
Many of the participants explained plainly, ‘It is just what we have to do for our juniors’, or stressed the importance of ‘passing on the experience’. For this last theme, having a tradition of commitment in passing on knowledge, skills or experience, could be classified as either identified (recognising the importance of passing on the experience) or integrated (I shall pass the baton on during a relay race) regulation depending on the level of internalisation by the participants. Furthermore, if this commitment becomes one which induces inherent satisfaction, it could be classified as intrinsic motivation. Indeed, this commitment to pass on knowledge is not culturally specific although certain cultures might facilitate the internalisation of this commitment more than others.
Discussion
In the current qualitative study, the authors investigated the motivation to provide feedback in the ED. Similarities with other studies in different settings focused on teaching can be referenced in the literature. Dybowski and Harendza in their series of studies found a wide range of motivations to teach, from a sense of occupational duty to the intrinsic joy of teaching.20 21 In a questionnaire survey that looked into the motivations of family physicians in teaching undergraduate students, May et al reported the ‘interest to transfer knowledge’ to be the most prominent motive.11 In another study which was done within a relatively busy clinical specialty, surgeons were motivated to teach learners due to a sense responsibility and the relationship that they had formed with learners, and because of the enjoyment of it.22 However, our study has highlighted distinct differences between scheduled teaching sessions and giving clinical feedback, notably, that during clinical feedback, the focus on patient safety and enhancing the quality of care. Such a difference could be due to the context in which our study was undertaken, in terms of our participants being ED physicians and the ED environment being a fast-paced one, where students and trainees need to be supervised and taught without compromising patient safety and care. By understanding the motivations to provide feedback, together with faculty development and system support, clinical feedback provision can then be enhanced.
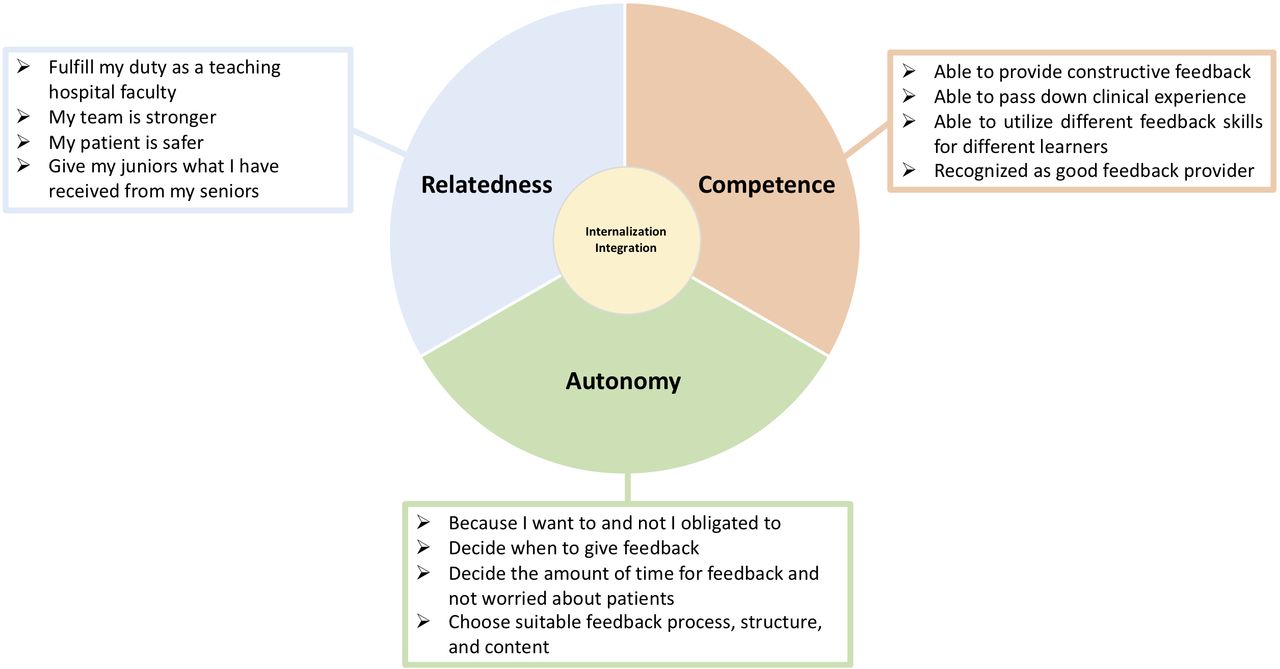
From our data, all four of the underlying motivations identified are extrinsic, although with different levels of self-determination. The question though is, how we can turn these extrinsic motivations into intrinsic ones. SDT emphasises the importance of the internalisation and integration of extrinsic motivations. Internalisation and integration are core socialisation processes. Internalisation refers to the process of absorbing an external value so that it becomes one’s own. Integration is about transforming the value and combining it with one’s own, so that it emanates from one’s self.12 23 There are three basic needs which could enable the internalisation and integration of motivations: autonomy, competence and relatedness (figure 3).14 24 In other words, the motivation to give feedback could be enhanced if faculty members are able to realise their autonomy and choice in whether or not to do so, when they feel competent or are recognised as competent feedback providers, or when they feel a sense of relatedness to the receiver of their feedback. As such, even though the outcomes of feedback provision (eg, stronger medical teams, safer patient care) might not have been the motivators for giving the feedback, these outcomes might work themselves into a feedback loop which may in turn increase the motivation of educators to provide feedback.

{kind=link}
{kind=link}
{kind=link}
The three basic needs which facilitate the internalisation (taking in a value to become one’s own) and integration (transformation of a regulation into one’s own so that it will subsequently emanate from one’s sense of self) of extrinsic motivations.
In addition, feedback provision performed under the basis of the tradition of passing on experience has the potential to turn from an extrinsic motivation into an intrinsic one, if the physician is able to find inherent satisfaction and enjoyment in the process of giving feedback. This is akin to the parent–child relationship, such as when a parent provides feedback while teaching their child how to ride a bike. If a parent witnesses that with each attempt, there is growth and improvement in the child’s ability to ride the bike, this might evoke an innate sense of joy or pride, which could in turn provide the parent with the impetus to continue investing their time in the act of giving feedback. A similar mechanism for how intrinsic motivations are also elicited during teaching activities has been previously shown.20 It should be noted that, however, the current study is conducted in a Confucian Asian country, where ‘A teacher for a day is a father for a lifetime’. Although the unpredictable teaching moments, critically ill patients, and fast-paced work environments may be similar in the EDs all around the world, relationships between feedback providers and receivers may vary across different cultural contexts. Further research may be needed to understand the transferability of our results, and how best to draw out intrinsic motivations to enable clinical teachers to provide feedback in a sustained manner.
Limitations
The first limitation to this study is that the participants were limited to a single country. EM is a relatively young specialty in Taiwan, recently celebrating the 20-year anniversary of emergency physician board certification. As a result, in the current study, the participants had 15 years of experience or less as attending physicians. The motivation or views about medical education could change as clinical teachers accumulate experience. Further research is needed to determine whether the conclusions of this study can be generalised to different ED or cultural settings. Second, as the interviews were performed in Chinese, there may be some loss in translation of the specifics of the viewpoints discussed between Mandarin and English. The third limitation regards the secondary analysis of the available qualitative dataset which was collected for a different question. The depth and comprehensiveness of the contents covered may be limited, and further qualitative or quantitative study is needed to clarify some of the issues raised in the current research.
Conclusion
We found that faculty members in the ED are motivated to provide feedback when they feel a responsibility towards their learners, when they understand the importance of feedback, or simply because of a commitment to pass on clinical knowledge to their juniors. With this understanding of why teachers would still provide feedback in spite of working in a busy clinical setting, we hope to be able to develop interventions that facilitate the integration of external motivations, and to explore ways in which genuine enjoyment can be innately produced.
Abstract translation
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.Data availability statement
Data in its original language are available on reasonable request.
Ethics statements
Ethics approval
This project was approved by the local institutional review board (Ref: 104–8510C).
References
Footnotes
Handling editor Simon Carley
Twitter @lynn.monrouxe
Contributors Funding acquisition: S-RY, C-HC. Conceptualisation: Y-CC, C-HC. Methodology: L-CC, C-HC. Software data management: S-RY, L-CC, C-HC. Formal analysis: S-RY, LVM, C-HC, Y-CC.Data coding: S-RY, C-HC, L-CC. Writing (original draft preparation): S-RY, Y-CC, C-HC. Writing (review and editing): Y-CC, C-HC, RYLN. LWriting (critical revision): C-HC, S-RY, LVM, Y-CC. Illustration sketching: RYLN. Project administration: S-RY, C-HC.
Funding This research was funded by Chang Gung Research Grant (CDRPG3E0081, CORPG1F0081), and Ministry of Science and Technology (MOST) grant (MOST 105–2511 S-182-016).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.