Article Text

Abstract
Introduction Special Operations Forces conduct military activities using specialised and unconventional techniques that offer a unique and complementary capability to conventional forces. These activities expose Special Operations Forces personnel to different injury risks in comparison with personnel in the conventional forces. Consequently, different injury patterns are expected in this population. The purpose of this research is to establish high-level evidence informing what is known about musculoskeletal injury epidemiology in Special Operations Forces.
Methods A systematic review was conducted using three online databases to identify original studies reporting musculoskeletal injury data in Special Operations Forces. A critical appraisal tool was applied to all included studies. Descriptive data were extracted for demographics, study design details and injuries (eg, injury frequency, injury type, body part injured, activity, mechanism, severity). Results were narratively synthesised.
Results Twenty-one studies were included. Trainees conducting qualification training had the highest injury frequency, up to 68% injured in a training period. The ankle, knee and lumbar spine were the most common body parts affected. Parachuting caused the most severe injuries. Physical training was the most common activity causing injury, accounting for up to 80% of injuries. Running and lifting were common injury mechanisms. Injury causation information was frequently not reported. Partially validated surveillance methods limited many studies.
Conclusions Injuries are prevalent in Special Operation Forces. Future research should prioritise identifying injury causation information that supports prevention. Focus on improving surveillance methods to enhance the accuracy and comparison of results across cohorts is also recommended.
- epidemiology
- musculoskeletal disorders
- occupational & industrial medicine
- preventive medicine
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Statistics from Altmetric.com
Key messages
Musculoskeletal injuries are prevalent across all Special Operations Forces (SOF) populations.
SOF trainees are a priority for injury prevention measures.
Physical training is the most commonly known injury cause.
Static-line parachuting causes the most severe injuries.
Current injury surveillance methods are inconsistent, are likely to underestimate the burden of injury and lack sufficient detail to direct prevention planning.
Introduction
Special Operations Forces (SOF) are military units which are specially designated and equipped to conduct military activities using unconventional techniques and employment modes.1 Special Operations Forces perform strategic tasks in high-risk environments using clandestine techniques, such as special reconnaissance and precision strike operations.1 In doing so, SOF provides a unique capability that is complementary to the capabilities of conventional forces. The activities undertaken by SOF are often physically arduous, such as open water swimming, airborne operations, small squad raids and prolonged exposure to load carriage.2 Subsequently, due to the nature of these activities, SOF personnel are exposed to different injury risks in comparison with conventional forces personnel. Consequently, different musculoskeletal injury patterns and different requirements to prevent injury in this population are expected.
Understanding injury epidemiology is essential in working towards strategic injury reduction to preserve military capability.3 4 While there is a growing body of epidemiological evidence drawing attention to the existing injury problems in conventional forces, by comparison, far less is known about injury epidemiology in SOF.5–9 It is important to distinguish the epidemiology of injuries in SOF to identify the aetiological risks that are representative of this population. With epidemiology evidence, prevention programmes can be prioritised, and interventions can be explicitly designed to protect the health of SOF personnel.3 4
Currently, there is no high-level evidence analysing injury epidemiology in SOF populations. The purpose of this study is to establish high-level evidence informing what is currently known about musculoskeletal injury epidemiology in SOF populations. The findings are important to monitor health problems and to generate information for prevention planning.10
Methods
Protocol and registration
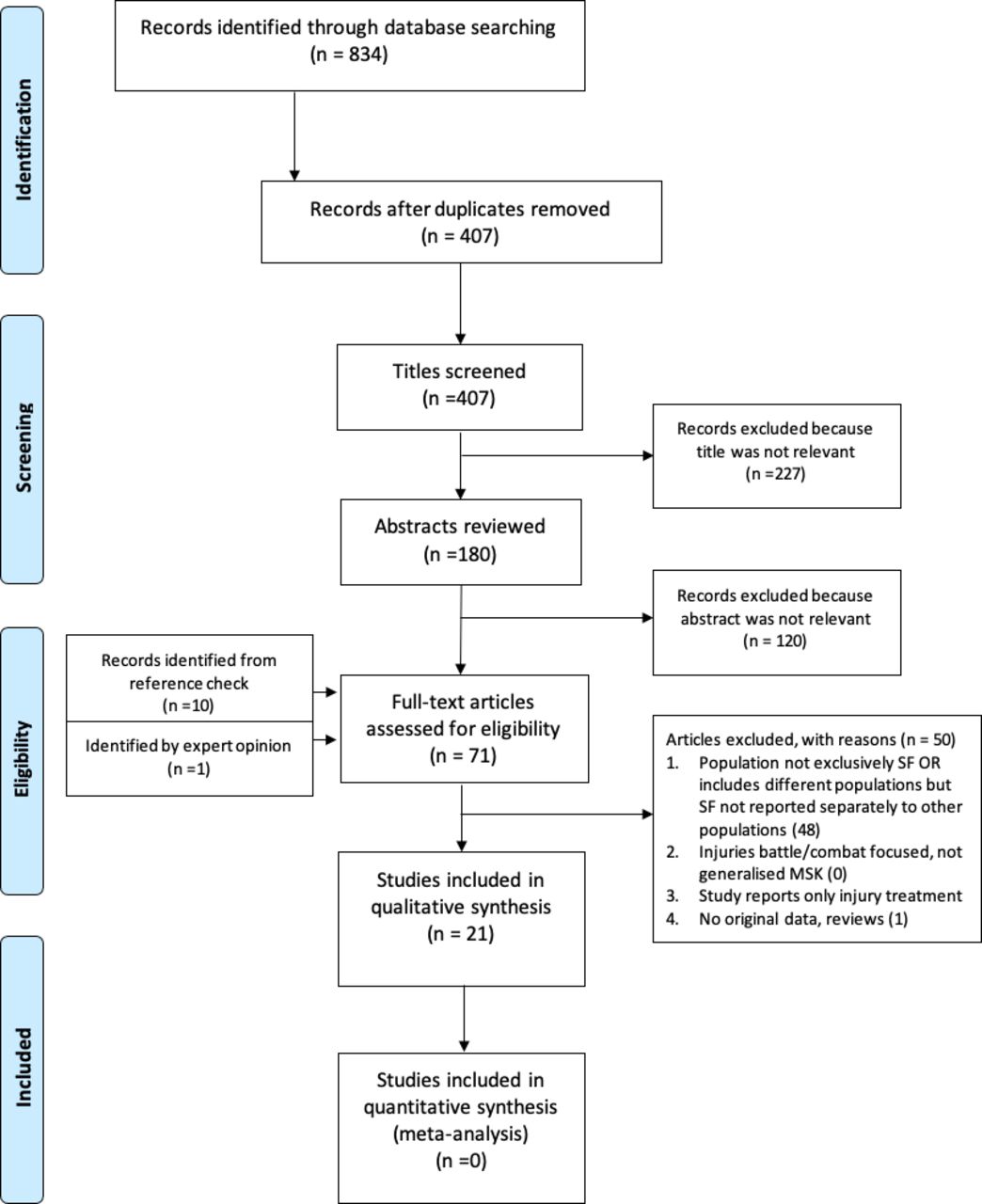
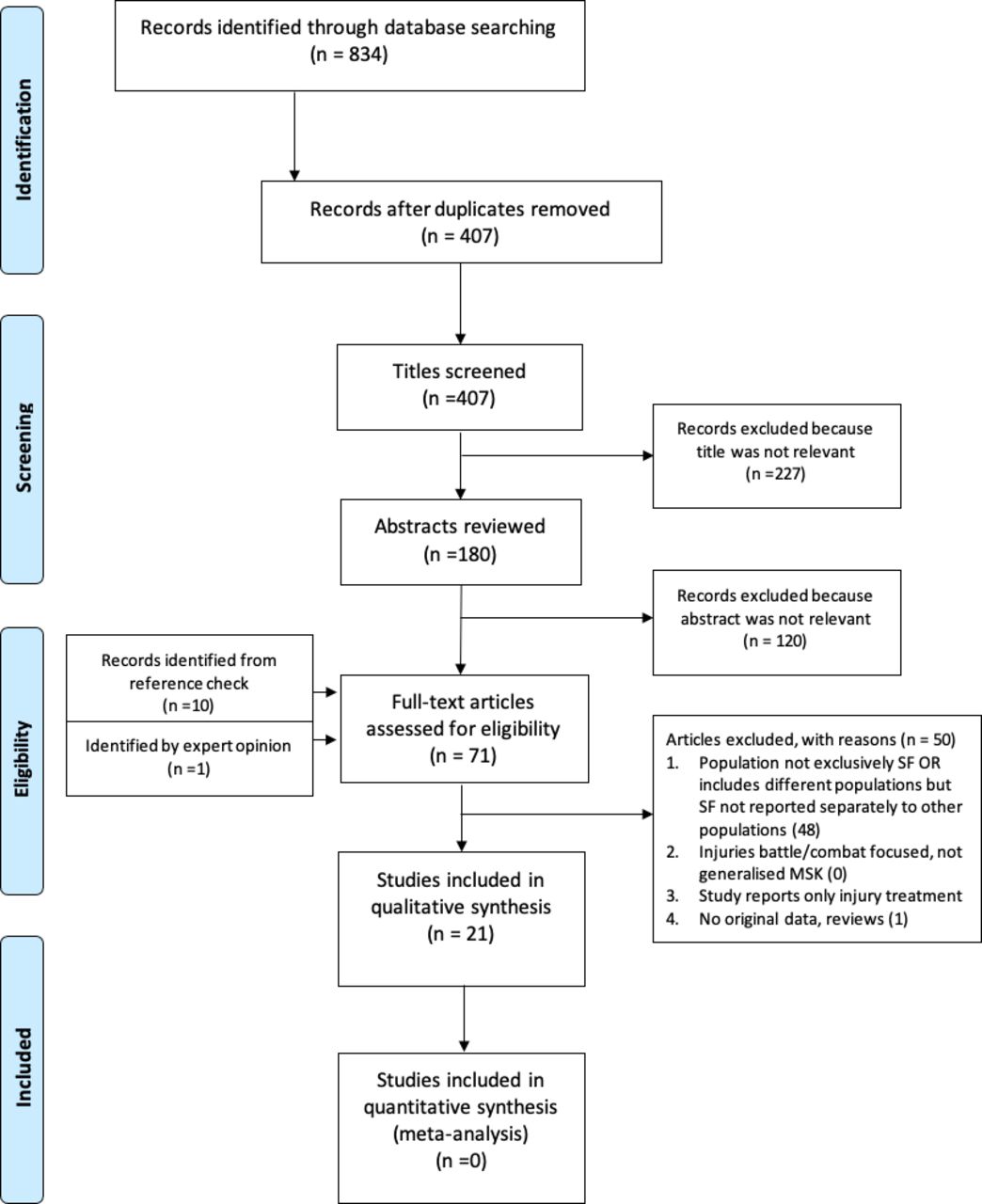
This systematic review is reported following the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA).11 The PRISMA flowchart is depicted in Figure 1.11 The systematic review was registered on the international prospective register of systematic reviews (CRD42020159639).12
{kind=link}
PRISMA protocol flowchart demonstrating the flow of information through each phase of the systematic review.
Search strategy
The search for peer-reviewed publications was conducted in December 2019 through online databases PubMed, Medline and Cumulative Index of Nursing and Allied Health Literature (CINAHL). A predefined search strategy was developed using musculoskeletal injury and SOF military-related keywords (online supplemental appendix A).
Supplemental material
Study selection
Following the removal of duplicates, all articles from the initial search strategy were screened for suitability according to the pre-established eligibility criteria (Table 1). Two reviewers independently screened all articles’ titles and abstracts. Where the reviewers disagreed, the article was retained for full-text review. One reviewer screened the references of all remaining articles, and if a reference was considered relevant, the study was included for further screening. The full texts of all remaining articles were reviewed, and those eligible were retained for analysis.
Article inclusion and exclusion criteria
Risk of bias in individual studies
In the absence of a gold standard appraisal tool for injury epidemiology research, three tools recommended by the Cochrane Collaboration were trialled against similar, but not included, studies.13–16 From this exercise, the ‘Risk of Bias’ (RoB) tool was deemed most applicable.14 Minor tool modifications were made to improve the suitability to a military context (online supplemental appendix B). The modified RoB tool was applied to all studies independently by two reviewers, with deliberation on the results. A third independent reviewer moderated for selected articles when there was a discrepancy.
Data extraction
One reviewer independently extracted data from the included studies based on predetermined variables. A second reviewer confirmed all data output. Descriptive data were extracted for demographics, study design details and injuries (injury frequency, injury type, body part injured, activity, mechanism, severity). In the instances where many results were reported, such as injury classification by body part, injury type and the activity causing injury, the top three results by percentage were extracted. Results were summarised as a narrative synthesis.
Results
Study selection
The initial search yielded 834 articles, from which 60 titles/abstracts were considered relevant, as seen in the PRISMA flow chart (Figure 1). A further 10 titles were identified from reference screening these 60 articles. One additional text was identified by a content expert.17 Following a full-text review, 21 studies were retained for analysis.17–37 The main reason for study exclusion was due to other occupation types in the sample population, and the results were not reported separately to provide data exclusive to a SOF population.
Risk of bias
Table 2 presents the critical appraisal of the studies. A third reviewer was required to appraise seven articles due to unclear reporting of study methods. Many studies had sampling bias, used partially validated surveillance methods and had incomplete reporting.
Risk of bias assessment of individual studies (n=21)
Study and demographic data
Fourteen studies were descriptive epidemiological designs, and seven were analytical study designs (Table 3). Most of the studies were Army affiliated (n=11, 52.4%) followed by Navy (n=5, 23.8%), Marine (n=2, 9.5%) and Airforce (n=1, 4.8%). Two studies did not specify a name to identify a SOF component or an associated military service other than being SOF.27 32 Eighteen of the 21 studies were from the USA. The remaining studies were from Belgium, the Netherlands and Australia.17 18 26
Study designs and the data collection methods of individual studies (n=21)
Table 4 identifies the demographic data extracted from individual studies. Seventeen studies included fully qualified personnel and four studies involved trainees completing qualification training. Seven studies reported on sex within the sample population of which all were male-only. Two studies analysed musculoskeletal injuries in military conflicts and one during a pre-deployment phase.21 25 28 The remaining studies were conducted with participants in garrison.
Demographic data from individual studies (n=21)
Injury occurrence
Table 5 presents all musculoskeletal injury information. Between 20% and 50% of qualified personnel sustained at least one injury within a 12-month period.29 33 34 36 Among trainees, between 17% and 68% sustained an injury during a training period.17 33 The Royal Netherlands Marine Corps identified that 23% of trainees did not complete qualification training due to injury.17 Trainees conducting Sea, Air and Land (SEAL) qualification training were reported to have the highest overall injury rate of 29.7 injuries per 100 trainee months.19 Airforce-affiliated SOF had the highest injury frequency overall among qualified personnel with 84.6 injuries per 100 persons per year.35 Parachuting-related injuries were reported to be between 0.3 and 2.2 cases per 100 jumps.22 23
Musculoskeletal injury epidemiological data extracted from individual studies (n=21)
Body part injured
Seventeen studies reported injury anatomical locations. Three studies grouped their analysis by body regions of which the lower extremity and spine were the most common regions affected.25 32 34 Fourteen studies analysed by specific body parts of which the ankle, knee and lumbar region were the most frequently affected sublocations.
Injury type
Thirteen studies reported injury type. Seven studies used a recognised injury classification tool to categorise by pathology.17 19 20 30 34 36 37 The remaining six studies did not describe their injury type categorisation methods. Injury type was categorised inconsistently between studies, resulting in 19 different injury types identified in the data extraction process. The most common injury types were ‘sprains and strains’, followed by fractures and injuries categorised as ‘pain and spasm’.
Activity causing injury
Twelve studies reported activities when injured. Seven studies investigated injuries resulting from specific tactical activities.18 21–26 One study analysed the prevalence of injuries concerning operations conducted by Special Boat Operators in the Naval Special Warfare.24 In this study, 66% of injury events were attributed to mission-related causes; however, the study did not specify further detail on the type of mission activities.24
Six studies exclusively analysed injuries sustained from military parachuting, of which five reported on static-line parachuting, and one did not specify a parachuting type.18 21–23 25 26 All parachuting studies reported their injury outcomes differently. One study identified lower injury rates in paratroopers who used a parachuting ankle brace in comparison with those who did not, 1.31 and 1.67 injuries per 100 jumps, respectively.23 Landing terrain also influenced injury rates with dirt strips being more hazardous than water, fields or airports.22 26 Two studies demonstrated increased injuries associated with increased paratrooper weight.18 26 One study identified that almost 90% of injuries sustained in a combat mission resulted from a static-line parachuting insertion.21
Four studies analysed activities more broadly.29 31 33 35 These studies used secondary data collected from medical documents or electronic health systems, which were limited by missing or insufficiently detailed information. One study reported ‘unknown’ and ‘other’ as the two most common injury causes, collectively accounting for 44% of injuries.31 Physical training was the most commonly known activity reported to cause injury, causing between 19% and 80% of injuries sustained.27 31 Physical training–related injuries were the highest in SEAL qualification trainees, accounting for 68% of injuries.33
Two studies investigated the association of musculoskeletal injury risk and certain intrinsic factors, such as movement patterns or lifestyle factors.30 34 Teyhen et al identified that previous history of injury, smoking, prior surgery and asymmetry of ankle mobility were associated with increased risk of acute and overuse injuries.30 Heebner et al demonstrated a weak increased injury risk associated with reduced strength of knee extension and shoulder retraction.34 Neither study recorded activity exposure information, such as military or physical training activities, to provide insight into other confounding variables.
Mechanism of injury
Very few studies (n=5) reported injury mechanisms to identify the specific events or mechanics involved in the injury event.18 29 31 33–35 Information on injury mechanism was often missing and instead categorised as ‘unknown’.29 31 33 Of the studies that reported known injury mechanisms, running was the most common, followed by lifting and direct trauma. Running-related injuries were reported to be between 12% and 23%.29 33 Special Forces Group had the most running-related injuries accounting for 23% of injuries, followed by SEAL trainees with 17%.29 33 Lifting accounted for 8%–21% of injury mechanisms.31 35 Lifting-related injuries occurred most commonly in Airforce Special Operations Command Operators in which almost all were attributed to weight lifting.35 One study assessing parachute landing injuries identified increased injury with the increasing weight of paratroopers.18 Two studies discussed that parachuting-related injuries could occur at any stage between exiting the plane, mid-air or on landing; however, neither included an injury mechanism analysis in their study.25 26
Severity of injury
Ten studies reported various metrics to indicate injury severity (Table 5). Eight studies reported severity by time loss, such as restricted duty days.17 21–24 27 28 Studies investigating parachuting-related injuries used reporting metrics that indicated greater injury severity than other studies, such as rates of hospitalisation and surgical intervention.25 26 Hospitalisation and surgical intervention resulted from 1.8% and 1.7% of parachute-related injuries, respectively.25 26 One study assessing static-line parachuting reported an average of 71 limited duty days per ankle injury.23 Another study identified that 57% of parachute-related injuries resulted in greater than 72 hours of restricted duty, and 19% caused a total loss of work.22 Significant loss of soldier availability was also identified in another study investigating a parachute insertion into a combat environment, of which 21% of parachute-related injuries resulted in soldiers deemed no longer fit for combat.21
Special Warfare Combat Crewman in the Naval Special Warfare recorded the highest cumulative time loss of 4223 restricted duty days for 121 injury events; however, it is not clear over which timeframe this was.24 Another study by Reynolds et al identified that within 12 months, a total of 3170 injury-related restricted duty days occurred in a SOF cohort of just 162 individuals.27 In this study, the average limited duty days was three times greater in SOF in comparison with other combatant military cohorts. No studies assessed injury severity concerning physical training or assessed medical discharge rates in qualified personnel.
Discussion
Injuries appear to be prevalent across all SOF populations. There were considerable variances of injury frequency between SOF populations which indicate some demographic subgroups, such as trainees, may be at more risk of injury than others. The lower extremities and spine were the most commonly affected anatomical locations. The majority of injuries were physical training related. There was a growing number of studies published within the last 5 years, which likely reflects the increasing recognition and the need to understand injuries better to sustain a capable workforce.
Trainees appear to be particularly vulnerable to injury, as indicated by higher injury occurrence and attrition rates.17 33 The Air Force Special Operations Command Special Operations Wing recorded the highest injury incidence in qualified operators.35 It remains unknown if other demographic variables, such as age, years of military experience, rank or sex, can influence injury patterns in SOF populations. Women gained the equal opportunity for SOF employment in the USA in 2016, which is likely why sex is not reported in earlier studies.38 Research in the regular Army has indicated that women have higher risks of injury than men.39 Future research should report injuries in relation to sex, age and rank as subgroup analyses to understand how these may influence injuries in these populations. Such research will inform whether additional injury precautions are required for specific personnel.
The majority of injuries affected the lower extremity and spine, specifically the ankle, knee and lumbar region. These anatomical locations are consistent with research in other military services which also report a high proportion of lower limb and spine injuries.5 36 40 The most common injury types were sprains and strains, fractures and ‘pain or spasm’ which are more consistent with acute-onset injuries. These greater acute injury patterns are different from those of conventional forces in which overuse injuries are more prevalent than acute-type injuries.27 41 42
Injury causation was often not assessed or was limited by insufficient data. Without this information, prevention opportunities cannot be prioritised as the activities leading to injury remain unknown. As such, future research should prioritise improving the recording of injury causation information. Static-line parachuting appears to result in more severe injuries than other activities. It is interesting to note that no other specific tactical skills were investigated, such as High-Altitude Low Opening parachuting, assault diving or close quarter combat fighting. It is unknown if this is because these activities are not considered to be a significant injury risk and therefore not a research priority. Of the available information, physical training was consistently the most common activity associated with an injury. These results are similar to the literature in conventional military services.6 Running, lifting and direct trauma were common injury mechanisms. Future research should prioritise these mechanisms to provide more evidence to inform injury prevention strategies.
Improving recording and reporting of injury in SOF
The risk-of-bias assessment identified consistent difficulties across the studies, which may influence conclusions on injury patterns.10 It was often not clear if the injury pattern variance was due to the research methods or the population within the individual studies. In addition, the inconsistent methods between studies made comparisons between studies difficult. Many studies were subjected to sampling bias which may result in the underestimation of injury prevalence. For example, some studies only recruited healthy participants from concurrent human performance studies.29 31 33–35 The majority of the studies used secondary data. Consequently, important epidemiology information was often missing. All studies used partially validated surveillance methods to collect injury epidemiological data, which may introduce misclassification bias and uncertainty on the validity of the results.10 This reiterates a currently established problem on the lack of taxonomy of musculoskeletal injury in a military context.5 41 43 44
Many studies did not record essential injury surveillance variables, such as injury causation.45 Subsequently, studies lacked sufficient evidence to inform injury prevention recommendations.3 Future research should consider improving the recording and reporting of essential injury surveillance variables and standardising methods to support and strengthen future research in a military context. In addition, it is recommended that future research use the Strengthening The Reporting Of Observational Studies In Epidemiology (STROBE) checklist of items to prevent inadequate or incomplete reporting of methods.46
Limitations of the systematic review
There were some limitations identified in our search strategy. It was noted that 10 studies were not identified by the search strategy terms but instead by screening the references of the full-text articles. We attribute this to the lack of consistent keywords applied to the manuscripts and that there are no available entry terms directly linking SOF to military-related Medical Subject Headings (MeSH). Subsequently, it is recognised that the search strategy was potentially not sensitive to detect all available literature. In future, research should allocate consistent keywords that can identify and delineate SOF populations.
Another limitation is that the critical appraisal tool used to evaluate the quality of individual studies is not formally validated. Subsequently, there are potential biases in the interpretation of study quality. To mitigate bias, the appraisal was conducted independently and collaboratively, and in some instances, a third reviewer was used to resolve discrepancies.
Conclusion
Musculoskeletal injuries are prevalent across all SOF populations. The available evidence indicates that physical training is the most common activity causing injury and that these injuries are most likely to occur from running or lifting. Parachute-related injuries appear to be the most severe, resulting in extended restricted duty and hospitalisation; however, the exact mechanism causing this is unknown. Overall, the epidemiological evidence suggests trainees are a priority subgroup for injury prevention and that further knowledge needs to be obtained as to why physical training and parachute-related injuries occur. Further research is essential to direct targeted injury prevention strategies and the allocation of resources, such as sport and exercise professionals, or improved parachuting equipment and training. Finally, it is recommended that future research should investigate the application of surveillance methods to a military context to improve the accuracy and consistency of future injury epidemiology research.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @lfortington
Contributors JS and LF jointly designed the project. JS led the data extraction, analysis and interpretation, and drafting of the manuscript, with ongoing review and input on each section by LF. Both authors approve the submitted version and are accountable for the accuracy and integrity of the work.
Funding This research was partially funded by the Defence Science Centre Western Australia (no grant number). This research was supported by an Australian Government Research Training Program (RTP) Fee-Offset Scholarship through Edith Cowan University (no award number).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.