Comparative efficacy of interventions for reducing symptoms of depression in people with dementia: systematic review and network meta-analysis
BMJ 2021; 372 doi: https://doi.org/10.1136/bmj.n532 (Published 24 March 2021) Cite this as: BMJ 2021;372:n532Linked Opinion
Social prescribing may help reduce symptoms of depression in people with dementia

- Jennifer A Watt, geriatrician and assistant professor12,
- Zahra Goodarzi, geriatrician and assistant professor345,
- Areti Angeliki Veroniki, statistician and senior research fellow167,
- Vera Nincic, research coordinator1,
- Paul A Khan, research coordinator1,
- Marco Ghassemi, research coordinator1,
- Yonda Lai, research coordinator1,
- Victoria Treister, research coordinator1,
- Yuan Thompson, research assistant1,
- Raphael Schneider, neurologist and assistant professor8910,
- Andrea C Tricco, scientist and associate professor111,
- Sharon E Straus, physician in chief and professor1211
- 1Knowledge Translation Program, Li Ka Shing Knowledge Institute, St Michael’s Hospital, Toronto, ON, Canada
- 2Division of Geriatric Medicine, Department of Medicine, University of Toronto, Toronto, ON, Canada
- 3Department of Medicine, University of Calgary, Foothills Medical Centre, Calgary, AB, Canada
- 4Hotchkiss Brain Institute, University of Calgary, Calgary, AB, Canada
- 5O’Brien Institute of Public Health, University of Calgary, Calgary, AB, Canada
- 6Department of Primary Education, School of Education, University of Ioannina, Ioannina, Greece
- 7Institute of Reproductive and Developmental Biology, Department of Surgery and Cancer, Faculty of Medicine, Imperial College, London, UK
- 8Division of Neurology, Department of Medicine, University of Toronto, Toronto, ON, Canada
- 9Institute of Medical Science, University of Toronto, Toronto, ON, Canada
- 10St Michael’s Hospital, Toronto, ON, Canada
- 11Institute for Health Policy, Management and Evaluation, University of Toronto, Toronto, ON, Canada
- Correspondence to: J A Watt jennifer.watt{at}utoronto.ca (or @jennannwatt on Twitter)
- Accepted 15 February 2021
Abstract
Objective To describe the comparative efficacy of drug and non-drug interventions for reducing symptoms of depression in people with dementia who experience depression as a neuropsychiatric symptom of dementia or have a diagnosis of a major depressive disorder.
Design Systematic review and meta-analysis.
Data sources Medline, Embase, the Cochrane Library, CINAHL, PsycINFO, and grey literature between inception and 15 October 2020.
Eligibility criteria for study selection Randomised trials comparing drug or non-drug interventions with usual care or any other intervention targeting symptoms of depression in people with dementia.
Main outcome measures Pairs of reviewers screened studies, abstracted aggregate level data, and appraised risk of bias with the Cochrane risk of bias tool, which facilitated the derivation of standardised mean differences and back transformed mean differences (on the Cornell scale for depression in dementia) from bayesian random effects network meta-analyses and pairwise meta-analyses.
Results Of 22 138 citations screened, 256 studies (28 483 people with dementia) were included. Missing data posed the greatest risk to review findings. In the network meta-analysis of studies including people with dementia without a diagnosis of a major depressive disorder who were experiencing symptoms of depression (213 studies; 25 177 people with dementia; between study variance 0.23), seven interventions were associated with a greater reduction in symptoms of depression compared with usual care: cognitive stimulation (mean difference −2.93, 95% credible interval −4.35 to −1.52), cognitive stimulation combined with a cholinesterase inhibitor (−11.39, −18.38 to −3.93), massage and touch therapy (−9.03, −12.28 to −5.88), multidisciplinary care (−1.98, −3.80 to −0.16), occupational therapy (−2.59, −4.70 to −0.40), exercise combined with social interaction and cognitive stimulation (−12.37, −19.01 to −5.36), and reminiscence therapy (−2.30, −3.68 to −0.93). Except for massage and touch therapy, cognitive stimulation combined with a cholinesterase inhibitor, and cognitive stimulation combined with exercise and social interaction, which were more efficacious than some drug interventions, no statistically significant difference was found in the comparative efficacy of drug and non-drug interventions for reducing symptoms of depression in people with dementia without a diagnosis of a major depressive disorder. Clinical and methodological heterogeneity precluded network meta-analysis of studies comparing the efficacy of interventions specifically for reducing symptoms of depression in people with dementia and a major depressive disorder (22 studies; 1829 patients).
Conclusions In this systematic review, non-drug interventions were found to be more efficacious than drug interventions for reducing symptoms of depression in people with dementia without a major depressive disorder.
Systematic review registration PROSPERO CRD42017050130.
Introduction
Fifty million people worldwide have a diagnosis of dementia.1 About 16% of people with dementia also have a diagnosis of a major depressive disorder, but 32% of those with dementia will experience symptoms of depression (as part of the neuropsychiatric symptoms of dementia) without a formal diagnosis of a major depressive disorder.23 In people with dementia, symptoms of depression manifest clinically as physical (eg, poor appetite, low energy) and behavioural (eg, irritability, social isolation, sadness) signs.45 Although those with dementia and symptoms of depression might not fulfil all the criteria of a major depressive disorder, these symptoms nonetheless have an impact on people with dementia and their care givers.678 Symptoms of depression in people with dementia are associated with adverse health outcomes, including lower quality of life, functional decline, and increased risk of death67891011 and are also associated with increased distress, burden, and depression in care givers.78
Drug (eg, antidepressants, antipsychotics) and non-drug (eg, reminiscence therapy, exercise) interventions are used to treat both major depressive disorders and symptoms of depression in people with dementia.1213141516 Increasing evidence of harm associated with antidepressant use in those with dementia (eg, from falls and fractures), and growing interest in social prescribing—linking patients with non-drug interventions in their community—as an effective treatment to combat symptoms of depression, loneliness, and isolation, has led to a renaissance for non-drug interventions.1718 Randomised trials directly comparing the efficacy of drug and non-drug interventions are, however, rare, which creates uncertainty in clinical decision making about selection of optimal evidence based interventions for treating symptoms of depression in people with dementia.
We determined the comparative efficacy of drug and non-drug interventions for reducing symptoms of depression in people with dementia who were experiencing depression as a neuropsychiatric symptom of dementia or had a diagnosis of a major depressive disorder. Network meta-analysis (NMA) was used to fill this critical knowledge gap created by a paucity of head-to-head randomised controlled trials.
Methods
We registered and published our protocol, which contains details of the literature search strategy.19 Our systematic review and NMA manuscript is written in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) extension statement for reporting systematic reviews incorporating NMA.20
Data sources and searches
We searched Medline, Embase, the Cochrane Library, CINAHL, and PsycINFO for citations published in any language from inception to 15 October 2020.19 We also searched grey literature and reviewed reference lists of included studies and related systematic reviews.19
Study selection
Eligible studies for inclusion were randomised controlled trials of drug and non-drug interventions used to treat symptoms of depression in people with dementia experiencing depression as a neuropsychiatric symptom of dementia or with a diagnosis of a major depressive disorder. Dementia (eg, medical history of dementia or Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-V)) and major depressive disorder (eg, DSM-V) were defined by study authors.6 Eligible drug interventions required final approval from the US Food and Drug Administration or Health Canada, as of our literature search date. Eligible comparators included usual care, placebo, or another drug and non-drug intervention. Studies reporting symptoms of depression using any outcome measure (eg, geriatric depression scale or Cornell scale for depression in dementia) were considered suitable for inclusion (see supplementary table 1).45 After pilot testing, pairs of reviewers (JAW, ZG, VN, PAK, MG, YL, VT, YT, RS) independently screened all citations and full text articles. No language restrictions were applied. Discrepancies in study inclusion were resolved by deliberation within the reviewer pairs or with input from a third reviewer.
Data abstraction and quality assessment
Pairs of reviewers (JAW, ZG, VN, PAK, MG, YL, YT, RS) abstracted aggregate level data from each included full text article and appraised each randomised controlled trial using the Cochrane risk of bias tool.21 For studies that reported two or more outcome measures for the same outcome, we established a hierarchy for determining the data to be abstracted. The Cornell scale for depression in dementia was the most commonly reported scale, followed by the geriatric depression scale and then the neuropsychiatric inventory-depression subscale.45 The Cornell scale for depression in dementia was preferentially abstracted, when reported. If this scale was not reported, but the geriatric depression scale or neuropsychiatric inventory-depression subscale was reported, we preferentially abstracted these scales before others. In one case we preferentially abstracted the geriatric depression scale as opposed to the neuropsychiatric inventory-depression subscale.22 Otherwise, in five cases we preferentially abstracted the Montgomery-Åsberg depression rating scale, Hamilton depression rating scale, major depression rating scale, and Sandoz clinical assessment-geriatric-depressed mood scale.2324252627 We contacted study authors for additional information about the study methods and reported outcomes. Discrepancies about data abstraction and quality assessment were resolved by deliberation within reviewer pairs or with input from a third reviewer.
Data synthesis and analysis
Two clinicians (JAW and ZG) coded all interventions according to the intervention or interventions described by study authors—that is, if the authors named an intervention as usual care but the intervention included providing educational materials to care givers in addition to usual care then the intervention was coded as “care giver education” (see fig 1 and supplementary table 2 for node definitions). Usual care was defined as appropriate access to healthcare (eg, doctor or nurse practitioner visits) and social care (eg, support for activities of daily living, such as bathing), based on patient needs and preferences. A placebo was defined as an inert intervention that was otherwise identical to an active comparator (eg, pill, sham intervention).

Descriptions of highly efficacious non-drug interventions in people with dementia
{kind=link}
We assessed network connectivity using a network diagram (STATA, version 15.1).28 Network transitivity was assessed by visual inspection of a table containing categorised study characteristics: mean study duration, mean patient age, mode proportion of women (≥50% or <50%), mode study setting (eg, nursing home or clinic), mode dementia type, mode outcome measure reported, mode severity of dementia, and mode of two items from the risk of bias assessment (incomplete outcome data and blinding of outcome assessment). When two risk of bias categories had the same number of randomised controlled trials (eg, two trials were at low risk of bias from missing data and two were at high risk of bias from missing data), we reported the risk of bias category associated with the greater risk of bias.
We conducted a bayesian random effects NMA in OpenBUGS, version 3.2.3.29 When more than one study existed for a treatment comparison, we conducted bayesian random effects pairwise meta-analysis. In these models, we assumed a common within network heterogeneity variable between studies and between data types (ie, contrast based or arm based data) because all interventions were aimed at alleviating similar symptoms in people with dementia. We chose random effects models because we anticipated between study clinical and methodological heterogeneity. Informative prior distributions were implemented for all between study heterogeneity variables (log(τ2) ~t(–3.85,1.932,5)).30 Vague prior distributions were implemented for trial baselines and treatment effects (normal(0,1000)). Because several different scales were used across studies, we report outcomes as posterior standardised mean differences with 95% credible intervals and predictive intervals. We back transformed standardised mean differences to mean differences, measured on the Cornell scale for depression in dementia, by multiplying the pooled standard deviation (derived from baseline mean Cornell scale for depression in dementia values of treatment arms in parallel randomised controlled trials that reported symptoms of depression measured with the scale) by each standardised mean difference.31 We compared mean differences with a minimum clinically important difference derived using a distribution based approach.31 To approximate the minimum clinically important difference, we derived estimates at 0.4 and 0.5 standard deviations of the pooled standard deviation.31 We ranked treatments using surface under the cumulative ranking curve values and accounted for their uncertainty in interpretation. Global inconsistency was assessed by comparing deviance and deviance information criterion statistics between consistency and inconsistency models.32 The loop specific approach was used to assess local inconsistency in each closed network loop.33 We planned to conduct subgroup analyses based on the following effect modifiers: study setting (residence in a nursing home or assisted living facility versus community or clinic setting), mean age of study population (≥80 years or <80 years), proportion of women (≥50% or <50%), whether standardised criteria were used to diagnose dementia, history of Alzheimer’s disease, study size (omitting studies with <50 patients enrolled), dementia severity (mild-moderate or moderate-severe), and intervention duration (≥11 weeks or <11 weeks). We also planned to conduct sensitivity analyses based on two components of the quality assessment that posed the greatest risk to the validity of study findings: missing outcome data and blinding of outcome assessment. However, additional analyses were possible only in these NMAs of interventions that were connected: standardised criteria used to diagnose dementia, mean age of study population <80 years, community study setting, mild-moderate dementia severity, intervention duration ≥11 weeks, low risk of bias from missing outcome data, and low or unclear risk of bias from missing outcome data. All other subgroup and sensitivity analyses were presented as pairwise meta-analyses. We completed a network meta-regression based on study publication year. A sensitivity analysis was conducted using a weakly informative prior distribution for between study standard deviation (τ ~N(0,1), τ >0) in our primary analysis. A comparison adjusted funnel plot was used to assess small study effects, where treatments were ordered by expected efficacy (eg, we would expect reminiscence therapy to be more efficacious than usual care) (STATA, version 15.1).28
Patient and public involvement
Twelve dementia care partners (nurses, allied health professionals, doctors, and a care giver) participated in an outcome prioritisation exercise.19 They independently ranked commonly reported neuropsychiatric symptoms (eg, aggression, agitation, depression, sleep disturbances) in descending order of importance.1931 These care partners selected change in symptoms of depression as an outcome of interest; therefore, our systematic review and NMA compares the efficacy of interventions for reducing symptoms of depression in people with dementia.19
Results
Overall, 22 138 citations and 3542 full text articles were screened (fig 2) and 256 articles (28 483 people with dementia) included in the systematic review (see supplementary references). Of 29 study authors emailed, 12 responded (41%): two provided additional data and one clarified study methods.343536 The Cornell scale for depression in dementia was the most reported outcome measure (table 1 and supplementary table 1). Most studies enrolled at least 50% of women and the mean age in most studies was at least 70 years. Studies were most often conducted in community and clinic settings (table 1 and supplementary tables 3a, 3b, 4a, and 4b).

Flow of studies in the review. CCTR=Cochrane Controlled Trials Register; CDSR=Cochrane Database of Systematic Reviews; DARE=Database of Reviews of Effectiveness
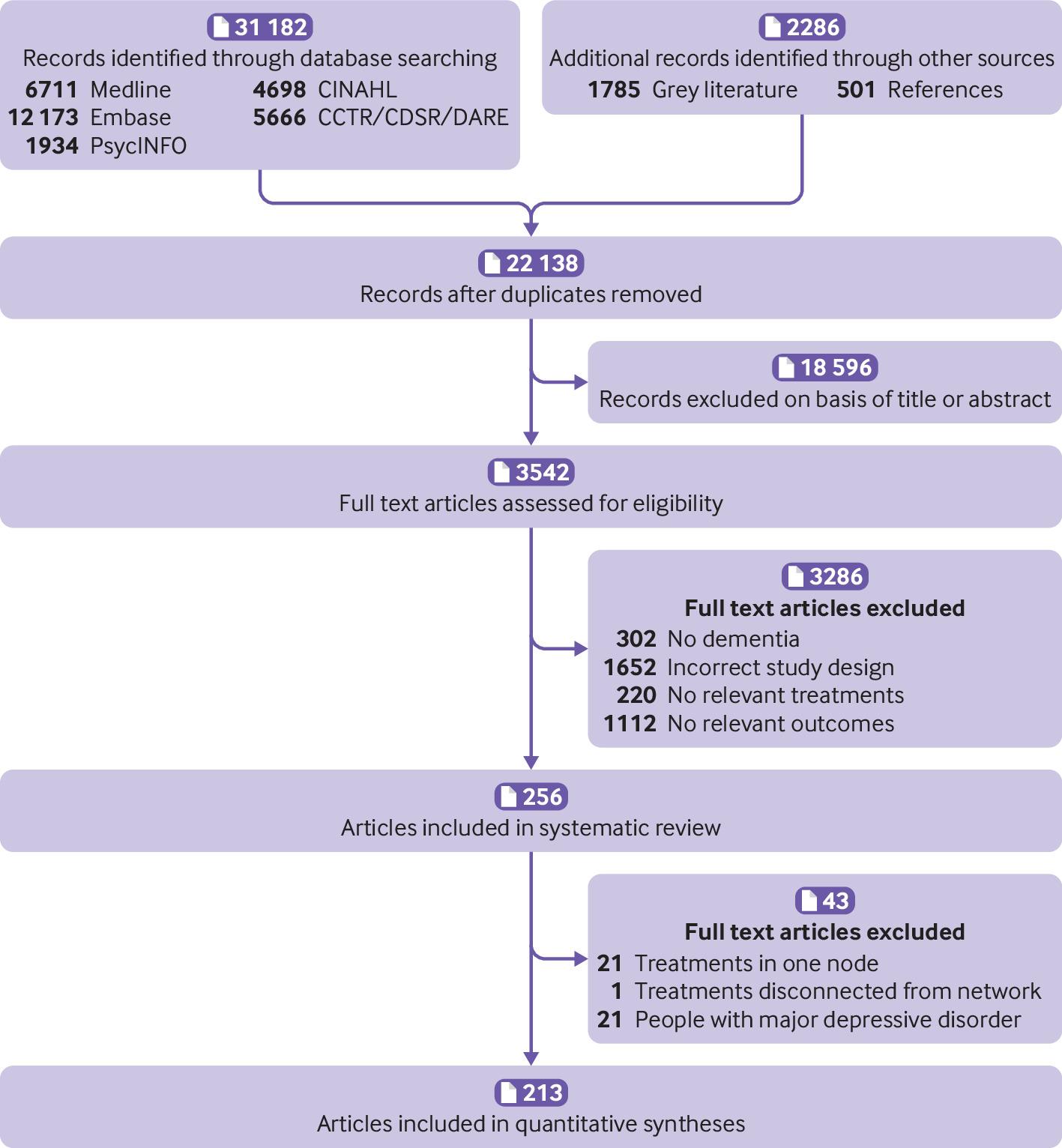{kind=link}
Characteristics of the included studies
People with dementia without a major depressive disorder
Two hundred and thirty five studies reported outcomes for interventions that targeted symptoms of depression in people with dementia without a diagnosis of a major depressive disorder. Of these studies, 213 (25 177 people with dementia) were included in pairwise meta-analysis and NMA. The network contained 61 connected intervention nodes: 70% of direct treatment comparisons involved usual care or placebo (fig 3). There were 45 triangular loops and seven quadratic loops. In most treatment comparisons, studies assessed symptoms of depression using the Cornell scale for depression in dementia and enrolled more women than men. Non-drug interventions were studied in 70% of trials. Nine studies compared the efficacy of an antidepressant with placebo and two studies compared the efficacy of an antidepressant with an antipsychotic.12132537383940414243 Risk of bias from missing data and blinding of outcome assessors posed the greatest risk to review findings: 42% of randomised controlled trials were at high risk of bias from missing data and 37% of trials were at unclear or high risk of bias from lack of assessor blinding (see supplementary table 5a and figure 1a). Differences were found in effect modifiers across 94 direct treatment comparisons—namely in terms of study setting, intervention duration, type of dementia, dementia severity, and risk of bias from missing data and lack of assessor blinding (see supplementary table 6). Standard deviation values associated with baseline mean Cornell scale for depression in dementia scores were included from 70 randomised controlled trials in the derivation of minimum clinically important differences. The estimated minimum clinically important difference for the Cornell scale for depression in dementia was 2.0 at 0.4 standard deviations and 2.5 at 0.5 standard deviations.

Network diagram for a network of interventions targeted at reducing symptoms of depression in people with dementia without a major depressive disorder. Nodes represent individual interventions, and nodes connected by lines indicate that the two connected interventions were directly compared in a study. Nodes are weighted by the number of studies that evaluated the treatment, and lines are weighted by the number of studies that evaluated the treatment comparison. ADL=activities of daily living modification; ANM=animal therapy; APSY=antipsychotics, ARO=aromatherapy, CG SUP=care giver support; CHEI=cholinesterase inhibitor; COG=cognitive rehabilitation; COMT=catechol-O-methyltransferase inhibitor; CST=cognitive stimulation; DBS=deep brain stimulation; DEP=antidepressant; DMQ=dextromethorphan-quinidine; EDU+SUP CG PWD=education and support of person with dementia and care giver; EDU CG=care giver education; EDU CG PWD=education of care giver and person with dementia; EDU PWD=education of person with dementia; ENV=environmental modification; ETA=etanercept; EXE=exercise; HR=hormonal therapy; HYP=antihypertensive; LIG=light therapy; LIP=lipid lowering therapy; MAS=massage therapy; MDC=multidisciplinary care; MEM=memantine; MIC=antimicrobial; MSS=multisensory stimulation; MUS=music therapy; ORT=reality orientation; OT=occupational therapy; PLA=placebo; PRED=prednisone; PSY=psychotherapy; REC=recreation therapy; REX=relaxation therapy; REM=reminiscence therapy; SOC=social interaction; STA=mood stabiliser; STIM=stimulant; TCS=transcutaneous stimulation; UC=usual care
{kind=link}
Supplementary table 7 reports the pairwise meta-analysis and NMA outcomes. The between study variance (τ2) in the primary NMA was moderate (0.23, 95% credible interval 0.17 to 0.31). A consistency rather than an inconsistency model provided a better model fit (see supplementary table 7). Two closed network loops were inconsistent in the primary NMA (2/52 loops, 4%): usual care-social interaction-animal therapy (inconsistency factor 1.88, 95% confidence interval 0.93 to 2.84) and music therapy-social interaction-cognitive rehabilitation (1.33, 0.08 to 2.58) (see supplementary figure 2a). No evidence was found of small study effects (see supplementary figure 3).
In the primary NMA, cognitive stimulation, cognitive stimulation combined with a cholinesterase inhibitor, exercise combined with social interaction and cognitive stimulation, massage and touch therapy, multidisciplinary care, occupational therapy, and reminiscence therapy were found to be more efficacious than usual care for reducing symptoms of depression in people with dementia without a diagnosis of a major depressive disorder (table 2 and supplementary table 7). In pairwise meta-analysis, animal therapy, exercise, and psychotherapy combined with reminiscence therapy and environmental modification were also found to be more efficacious than usual care for reducing symptoms of depression in people with dementia (table 2 and supplementary table 7). Except for massage and touch therapy, cognitive stimulation combined with a cholinesterase inhibitor, and cognitive stimulation combined with exercise and social interaction, which were found to be more efficacious than some drug interventions, there was no statistically significant difference in the comparative efficacy of drug and non-drug interventions for reducing symptoms of depression in people with dementia without a diagnosis of a major depressive disorder (see supplementary table 7). These findings were unchanged when a minimally informative prior was implemented for the heterogeneity variable. Based on surface under the cumulative ranking curve values, the most highly ranked interventions were cognitive stimulation combined with exercise and social interaction (98.3%, 88.3% to 100%), cognitive stimulation combined with a cholinesterase inhibitor (98.3%, 95% credible interval 86.7% to 100%), and massage and touch therapy (95.0%, 86.7% to 100%). When a minimally informative prior was implemented for the heterogeneity variable, the most highly ranked interventions were cognitive stimulation combined with a cholinesterase inhibitor (98.3%, 88.3% to 100%), cognitive stimulation combined with exercise and social interaction (98.3%, 86.7% to 100%), and massage and touch therapy (95.0%, 85.0% to 100%).
Efficacy of interventions for reducing symptoms of depression in people with dementia without a diagnosis of major depressive disorder
In the NMA of studies with dementia diagnosed using standard criteria (eg, DSM-V), a consistency rather than inconsistency model provided a better model fit, and no inconsistent loops of evidence were found (see supplementary figure 2d). As in the primary NMA, cognitive stimulation, cognitive stimulation combined with a cholinesterase inhibitor, cognitive stimulation combined with exercise and social interaction, massage and touch therapy, multidisciplinary care, occupational therapy, and reminiscence therapy were found to be more efficacious than usual care (table 3 and supplementary tables 8 and 9). In this NMA of studies where dementia was diagnosed using standard criteria, massage and touch therapy, cognitive stimulation combined with a cholinesterase inhibitor, and cognitive stimulation combined with exercise and social interaction were found to be more efficacious than some drug interventions (see supplementary table 8). An antidepressant combined with a cholinesterase inhibitor was found to be more efficacious than care giver support (mean difference −9.2, 95% credible interval −18.3 to −0.08) in this subgroup of studies, but no statistically significant differences were found when the efficacy of other drug and non-drug interventions were compared (see supplementary table 8).
Efficacy of interventions for reducing symptoms of depression in subgroups of people with dementia without a diagnosis of major depressive disorder
People with dementia and a major depressive disorder
Twenty two studies (1829 people with dementia) reported outcomes for interventions aimed at reducing symptoms of depression in people with dementia and a major depressive disorder. The greatest risk to review findings was from missing data: 73% of studies were at high risk of bias from missing data (see supplementary table 5b and figure 1b). Too few studies and anticipated substantial heterogeneity among study characteristics and interventions precluded pairwise meta-analysis or NMA (see supplementary tables 3b and 4b). Studies were conducted in both community and non-community settings and enrolled participants with Alzheimer’s disease or unspecified types of dementia. Drug interventions included mirtazapine, sertraline, venlafaxine, fluoxetine, citalopram, escitalopram, desipramine, imipramine, clomipramine, amitriptyline, and paroxetine.164299100101102103104105106107108109 Seven randomised controlled trials reported the comparative efficacy of selective serotonin reuptake inhibitors (ie, sertraline, fluoxetine, citalopram, escitalopram) and placebo, with mixed conclusions.1699102103105106108 Neither mirtazapine nor venlafaxine were associated with improved symptoms of depression compared with placebo.16100 Multidisciplinary care was found to be more efficacious than usual care in one randomised controlled trial, but evidence supporting the efficacy of other non-drug interventions—namely, psychotherapy and exercise—was mixed.110111112113114115116117 Drug strategies for pain management (ie, paracetamol (acetaminophen) or buprenorphine) were not found to be superior to placebo.118
Discussion
Our systematic review and NMA showed that non-drug interventions were as, or more, efficacious than drug interventions for reducing symptoms of depression in people with dementia and without a diagnosis of a major depressive disorder. Ten interventions were found to be more efficacious than usual care in our primary pairwise meta-analyses and NMA: animal therapy, cognitive stimulation, exercise, massage and touch therapy, reminiscence therapy, multidisciplinary care, occupational therapy, cognitive stimulation and a cholinesterase inhibitor, exercise combined with social interaction and cognitive stimulation, and psychotherapy combined with reminiscence therapy and environmental modification. No drug intervention alone was found to be more efficacious than usual care. Intervention rankings suggest that non-drug interventions either alone or in combination with drug interventions are the best interventions for reducing symptoms of depression in people with dementia without a diagnosis of a major depressive disorder. Our findings further suggest a high probability that people with dementia will derive a clinically meaningful benefit from non-drug interventions.
Comparison with other studies
This systematic review and NMA compared the efficacy of drug interventions with non-drug interventions for reducing symptoms of depression in people with dementia. Previous systematic reviews found potential reductions in symptoms of depression associated with certain non-drug interventions.119120 Another systematic review showed limited and inconsistent evidence of benefit concerning the efficacy of drug interventions for reducing symptoms of depression in people with dementia.121 In our NMA we synthesised data for 61 interventions across 213 studies to bring together these two disparate bodies of literature and show the relative ranking of drug and non-drug interventions in terms of efficacy. Our study is important and timely given the growing interest in social prescribing—linking patients with non-drug interventions in their community—as a treatment regimen for mitigating symptoms of depression, loneliness, and social isolation.18 We identified efficacious non-drug treatment options (eg, cognitive stimulation, exercise, and reminiscence therapy) that clinicians can prescribe as part of an evidence based treatment plan to reduce symptoms of depression in people with dementia. Our finding that non-drug and multidisciplinary care approaches alleviate symptoms of depression in people with dementia builds on our recent finding that these approaches also reduce symptoms of aggression and agitation in people with dementia.31 However, cost effectiveness, scalability, and sustainability of efficacious non-drug and multidisciplinary interventions for reducing neuropsychiatric symptoms in people with dementia remain unclear and might vary by intervention.122123
Policy implications
Several effective non-drug interventions, including cognitive stimulation, multidisciplinary care, occupational therapy, and exercise are already accessible in some clinical and community settings; however, clinicians, policy makers, health services researchers, and implementation scientists must work together to ensure that all people with dementia have equitable access to these interventions, regardless of sex, geographical location (ie, rural or urban) or ethnicity; to teach patients and care givers about how these interventions can reduce symptoms of depression; and to study the impact of how enrolling patients in programmes that incorporate these interventions reduces symptoms of depression or other related symptoms of loneliness and social isolation.119 For example, the National Institute for Health and Care Excellence dementia care guideline recommends cognitive stimulation therapy to improve cognitive function, independence, and wellbeing.124 Moreover, cognitive stimulation therapy is available through National Health Service trusts in England. These cognitive stimulation sessions, encompassing activities to promote mental stimulation, reminiscence, social interaction, and orientation, could be further extended to reduce symptoms of depression in people with dementia.46
Strengths and limitations of this review
Our study has notable strengths. We reviewed more than 3000 full text articles because symptoms of depression, as with other neuropsychiatric symptoms in people with dementia, are often not reported in the title or abstract of articles. We presented our findings as back transformed mean differences on the Cornell scale for depression in dementia (a scale commonly used in clinical practice for capturing symptoms of depression in people with dementia) and probabilities of meeting a threshold for minimum clinically important difference to facilitate knowledge dissemination.
Our study also has limitations. Firstly, although we could derive estimates of intervention efficacy in people with Alzheimer’s disease, we could not explore the efficacy of interventions in other types of dementia because studies were too few. Secondly, we could not explore the impact of the severity of depression symptoms on the comparative efficacy of interventions because several different scales were included, not all of which have established thresholds for categorising symptom severity. Thirdly, the risk of bias from missing data was substantial in our systematic review and NMA; however, the number of people with missing data, by treatment group, was not explicitly reported in some studies, which meant we could not assess the impact of missing data on our results. Fourthly, moderate between study heterogeneity in our NMA meant that predictive intervals for some treatment effects were wide and therefore it is difficult to predict the efficacy of an intervention in a subsequent study. Lastly, we did not look at the potential costs or harms associated with implementing drug and non-drug interventions as a treatment for reducing symptoms of depression in people with dementia.
Conclusions
Our systematic review and NMA comparing the efficacy of drug interventions with non-drug interventions for reducing symptoms of depression in people with dementia showed that non-drug and multidisciplinary approaches are highly efficacious interventions from which people with dementia will derive benefit. Everyone has a role in translating our findings into practice: people with dementia and care givers can speak with clinicians about available non-drug interventions; clinicians can prescribe non-drug interventions to people with dementia and symptoms of depression; and policy makers can support people with dementia, care givers, and clinicians in choosing non-drug interventions by developing health services, systems, and policies that enable implementation.
What is already known on this topic
Interest is growing in social prescribing—linking patients with non-drug interventions in their community—to reduce symptoms of depression, isolation, and loneliness
Individual randomised trials have shown that non-drug interventions (eg, exercise) alleviate symptoms of depression in people with dementia
The comparative efficacy of drug and non-drug interventions for reducing symptoms of depression in people with dementia, with or without a diagnosis of a major depressive disorder, is, however, unknown
What this study adds
In this systematic review, non-drug approaches were associated with a meaningful reduction in symptoms of depression in people with dementia and without a diagnosis of a major depressive disorder
Drug approaches alone, however, were not more efficacious than usual care
Acknowledgments
We thank Jessie McGowan for creating our literature search strategy.
Footnotes
Contributors: JAW, ZG, ACT, AAV, and SES designed the study. JAW, ZG, VN, PAK, MG, VT, YL, YT, and RS screened articles and abstracted data. JAW, ZG, and AAV conducted data analyses. JAW drafted the first version of the manuscript. All authors contributed to the manuscript’s revision and interpretation of findings. JAW is the guarantor. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding: This study was funded by the Alberta Critical Care Strategic Clinical Network. The funder had no role in the study design; collection, analysis, and interpretation of data; writing of the report; or decision to submit the article for publication. All authors had full access to study data and can take responsibility for the integrity of the data and accuracy of the data analysis.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from the Alberta Critical Care Strategic Clinical Network; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work. ACT is funded by a tier 2 Canada research chair in Knowledge Synthesis. SES is funded by a tier 1 Canada research chair in knowledge translation. AAV is funded by a European Union’s Horizon 2020 grant (No 754936).
Ethical approval: Not required.
Data sharing: The full dataset and statistical code will be available upon reasonable request.
The manuscript’s guarantor (JAW) affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as originally planned (and, if relevant, registered) have been explained.
Dissemination to participants and related patient and public communities: We will disseminate our results to relevant knowledge user groups (eg, patients, care givers, healthcare managers, and clinicians).
Provenance and peer review: Not commissioned; externally peer reviewed.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.