Article Text

Abstract
Objective (1) Identify and review current policies for the cardiovascular screening of athletes to assess their applicability to the paediatric population and (2) evaluate the quality of these policy documents using the Appraisal of Guidelines for Research & Evaluation II (AGREE II) tool.
Design Systematic review and quality appraisal of policy documents.
Data sources A systematic search of PubMed, MEDLINE, Scopus, Web of Science, SportDiscus and CINAHL.
Eligibility criteria for selecting studies An article was included if it was a policy/position statement/guideline/consensus or recommendation paper relating to athletes and cardiovascular preparticipation screening.
Results and summary Of the 1630 articles screened, 13 met the inclusion criteria. Relevance to paediatric athletes was found to be high in 3 (23%), moderate in 6 (46%) and low in 4 (31%), and only 2 provide tailored guidance for the athlete aged 12–18 years. A median 5 related citations per policy investigated solely paediatric athletes, with study designs most commonly being retrospective (72%). AGREEII overall quality scores ranged from 25% to 92%, with a median of 75%. The lowest scoring domains were rigour of development; (median 32%) stakeholder involvement (median 47%) and Applicability (median 52%).
Conclusion Cardiac screening policies for athletes predominantly focus on adults, with few providing specific recommendations for paediatric athletes. The overall quality of the policies was moderate, with more recent documents scoring higher. Future research is needed in paediatric athletes to inform and develop cardiac screening guidelines, to improve the cardiac care of youth athletes.
- Athletes
- Cardiology
- Pediatrics
- Adolescent
- Heart
Statistics from Altmetric.com
What is already known?
Cardiovascular screening of young athletes is supported by most leading sporting organisations and governing bodies around the world.
Numerous policy documents exist yet guidance on how to perform cardiac screening has predominantly focused on adult athletes.
Clear evidence-based guidance on how to perform cardiac screening in paediatric athletes is paramount to successful implementation and ensuring the health and well-being of this population, yet no methodological appraisal of current policies has been conducted.
What are the new findings?
Available policy documents for the cardiovascular screening of athletes typically have low to moderate relevance to the paediatric athlete, with only two policies providing specific guidance for the paediatric athlete: highlighting the need for new research and specific recommendations for this population.
Data referenced within the policies were mostly derived from cohorts of adults only or combined cohorts of adult and paediatric athletes, suggesting caution is warranted in applying findings specifically to the paediatric athlete.
The overall quality of the policies had a median score of 75%, with the lower scoring domains being rigour of development and stakeholder involvement. Methodology that follows the Appraisal of Guidelines for Research & Evaluation II instrument is needed in the planning and creation of athlete cardiac screening guidelines.
Introduction
In the search to identify underlying cardiac pathology that may predispose an individual to sudden cardiac death (SCD), preparticipation cardiovascular screening of young athletes has long been advocated by the American Heart Association (AHA) and the European Society of Cardiology (ESC).1 2 Among athletes with underlying pathology, exercise may trigger fatal arrhythmias, resulting in the 2.8–5.3 times greater incidence of SCD than their non-athletic peers.3 4 SCD can affect young athletes of any age. While studies have typically reported an incidence of 1.25–2.5 per 100 000,5 a recent study of UK adolescent footballers reported a sudden cardiac arrest (SCA) incidence of 6.8/100 000 person-years.6
Over the past decade, there has been a notable increase in the awareness of SCD, the adoption of preparticipation cardiovascular screening and the professionalisation of youth sport.7 Today, most major sports organisations and governing bodies are advocating for or mandating cardiac screening. However, debate surrounds what defines an athlete, who should be screened and from what age.
Children are not ‘miniature adults’, and age-specific normative values for cardiac testing are necessary to increase diagnostic accuracy as adult recommendations cannot be applied unequivocally.8 Paediatric athletes do show physiological remodelling of the heart in response to exercise9; but owing to factors such as maturational development and variable disease penetrance and aetiology, the grey zone between physiological and pathological adaptation may be further blurred. In contrast to adults, children suffering a SCD event are more often found to have a structurally normal heart.10 This may be a result of the growth and hormonal changes needed during adolescence to unmask genetic cardiac disease. In other words, prior to full biological maturation it could be more difficult to identify the early phenotypic manifestation of associated conditions.8
Concerns exist around the preparticipation evaluation of young athletes and whether current guidelines are suitable. To date, the guidance on how to perform cardiac screening in athletes has predominantly used data from elite adult athletes.8 Numerous international sports and medicine organisations have issued guidance on athlete screening, with variable degrees of overlap in the recommendations. Although age is now tentatively considered within athlete ECG11 and echocardiogram guidelines,12 13 few policies consider paediatric athletes separately, and fewer target children specifically. The primary aim of this study was to review the current recommendations, guidelines, consensus and position papers on athlete screening, with a focus on their relevance to the paediatric population. The secondary aim was to evaluate the quality of these policies using the Appraisal of Guidelines for Research & Evaluation II (AGREE II) tool and identify potential areas of improvement.
Methods
Study design
This systematic review was designed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.14 University of York/PROSPERO was contacted prior to starting the review process, where they cited that registration was not required.
Study eligibility
Inclusion criteria were: (1) Pertaining to athletes, defined as ‘One who participates in an organised team or individual sport that requires regular competition against others as a central component, places a high premium on excellence and achievement, and requires some form of systematic (and usually intense) training’15; (2) Policy, guidelines, scientific or consensus statement or recommendations paper by a medical organisation or sports governing body; (3) Relating to preparticipation screening and (4) English language.
Exclusion criteria were as follws: (1) Studies including individuals that do not meet the criteria for athlete status; (2) Prior versions of policies by an organisation regarding the same population that have since been updated; (3) Guidelines for non-athlete screening (including individuals with cardiovascular disease or general population); (4) Non-English language papers; (5) Editorials, letters to the editor, narrative reviews, theses, unpublished work and conference abstracts and (6) Papers not clearly authored, endorsed or supervised by a medical organisation or governing body.
Database search
PubMed, MEDLINE, Scopus, Web of Science, SportDiscus and CINAHL databases were searched from inception to April 2020 and repeated in October 2021. Search terms were mapped to relevant MeSH terms or subject headings relating to the concepts of “guidelines”, “athletes”, “cardiology” and “screening”. Terms within each section were combined with the Boolean operator ‘OR’, and then concepts were combined with the ‘AND’ operator to produce the search strategy (The full search strategy (April 2020 output) is available in the online supplemental table 1).
Supplemental material
Study selection and data extraction
Title, abstract and full-text screening were performed using the Covidence platform (Veritas Health Innovation, Melbourne, Australia), independently, by two reviewers (NRR and DMD). Data extraction was conducted independently by NRR and DMD and included paper and methodology description, data on the target population, the relevance to paediatric athletes and level of evidence the policies are based on.
Relevance to paediatric athletes
Relevance to paediatric athletes, defined as under 18 years old or mostly of high-school age, was evaluated by several methods, for each guideline, by two researchers (NRR and DMD). An overall relevance grading was based on the rounded average of three items, scored from 1 to 3. An average of 0–1 was considered ‘low relevance’, 1.1–2 was ‘moderate relevance’ and 2.1–3 was ‘high relevance’ to paediatric athletes.
First, we determined whether the policies targeted the paediatric athlete: (1) no stated mention of paediatric athletes in the policies remit, (2) included in a broader age range and (3) paediatric athletes included in the policies remit. Second and third scores counted the number of paediatric references related to the topics of SCD and screening. Intervals were chosen arbitrarily, based on average number of references – 1 (1–4 references), 2 (5–9 references) and 3 (≥10 references). The topic of ‘SCD’ comprised all references evaluating the epidemiology, incidence and/or aetiology of SCA/SCD. ‘Screening’ comprised all references evaluating the implementation, suitability and/or effectiveness of screening using any assessment modality. A reference could be assigned to both topics, if appropriate. The total number of original research papers referenced that included any paediatric athletes were counted, and a percentage from the total number of references per policy was calculated.
To evaluate the type of referenced studies, all original research papers were classified according to study design: case series (targeted population, no comparator), cross sectional, case–control, retrospective cohort, prospective observational, interventional (including randomised clinical trial), systematic reviews/meta-analysis and economical simulation studies. Prospective observational studies were not further categorised, to avoid over-omplicating the classification. The total mentions of paediatric related terms (“child*”, “adolescen*”, “p(a)ediatric”, “boy*/girl*”, “(high)school”) were counted.
All classifications were reviewed by NRR and DMD. In all steps above, a third reviewer (GP) arbitrated disagreements, and any discrepancies were resolved through team consensus.
Guideline quality assessment
The quality and variability of policies were assessed independently by NRR and DMD by using the AGREE II tool.16 This tool evaluates 23 items (Q1-Q23) grouped in six domains (Scope and Purpose, Stakeholder Involvement, Rigour of Development, Clarity of Presentation, Applicability, Editorial Independence), and an overall score, ranked on a 7-point scale. Domain scores from individual appraisers are summed and then scaled to a percentage of the maximum possible score for that domain using the formula (reviewer 1 score+reviewer 2 score − minimum possible score) / (maximum possible score−minimum possible score)×100.
Statistical analysis
Categorical data are presented as frequency and proportion, while continuous values (including AGREE II domain scaled scores), are presented as median and range. Data were summarised according to the Synthesis without meta-analysis guidelines.17 Descriptive statistical analyses were conducted using STATA/SE V.12 (Stata).
Results
After abstract and full-text screening, 13 policies were included (figure 1).2 18–29 These were from a variety of organisations, ranging from general medicine, paediatrics, cardiology, sports medicine and athletic committees. Most were published after 2010 (n=10), two between 2000–2010 and one before 2000. Only one used systematic literature search methodologies, only two had paediatric specific recommendations, eight offer recommendations on the frequency of preparticipation screening, with most discussing medical history, physical exam and/or ECG as screening modalities. Due to a lack of interventional randomised control trials or meta-analyses of randomised control trials, none of the policies have a high grade level of evidence (see table 1).

PRISMA flow chart of screened, included and excluded studies. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Characteristics of included guidelines
Relevance to paediatric athletes
Among all 13 included policies, there was considerable variance in the relevance to paediatric athletes. Ten (77%) had low-moderate relevance (figure 2A). Four included the paediatric athlete within their remit, but just two provided specific direction for screening athletes between 12 and 18 years. Only one policy cited more than 10 articles based on paediatric only populations for both topics of athlete screening and SCD.

Proportion of policies by relevance to paediatric athlete’s score (A). Proportion of original research citations including paediatric athletes from total, sorted from highest to lowest (B).
Citations of original related research including any paediatric athletes in their cohort ranged from 5 to 80 (median 27 per policy), a number representing between 10% and 53% (median 26%) of the total references in each policy (figure 2B). Of these, the most commonly referenced studies were retrospective in design, (median 16 per policy; range 2–62), followed by prospective observational (median 7 per policy; range 1–13), (table 2). The study design of this referenced paediatric original research differed considerably by topic and policy (figure 3A).
Relevance to paediatric athletes
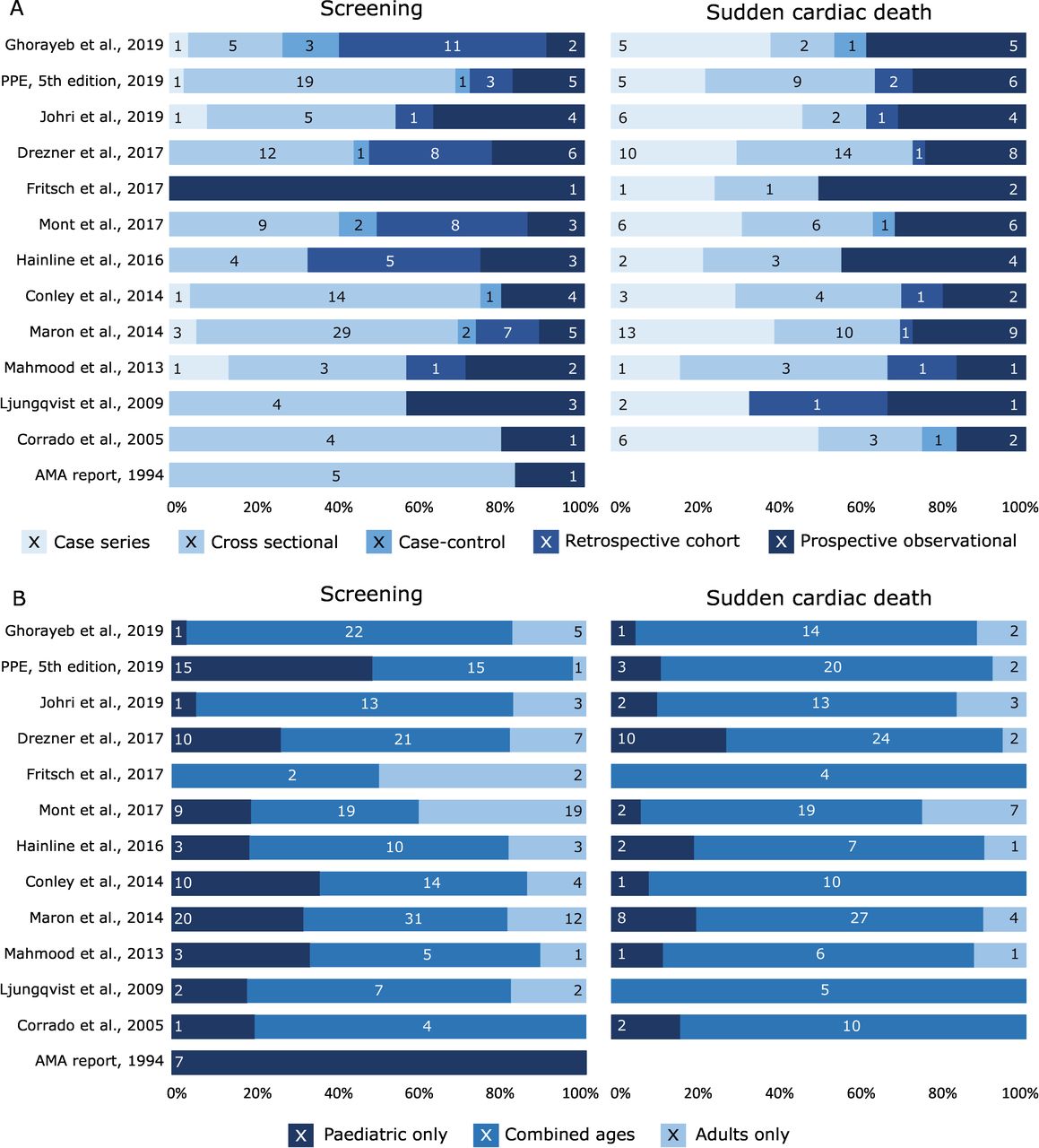
Proportion and number of original related research citations by study design (A), and by age group (B), on the topic of screening (left side) and sudden cardiac death (right side). Overlaid values are the number of citations, with the horizontal scale representing percentage from topic relevant citations. AMA, American Medical Association; PPE, preparticipation physical evaluation.
A median of 5 citations per policy comprised only paediatric athletes (range 0–26). While comparable to that of adult only studies (median 4, range 0–24), it was lower than those using cohorts combining both paediatric and adult athletes (median 22 per policy, range 0–54), (figure 3B). The median proportion of paediatric only references was higher in the screening topic (19%, range 0%–100%) than in the SCD topic (5%, range 0%–14%).
Mention of terms related to paediatrics ranged from 1 to 183 per policy (median 10 per policy), with the most common terms used being ‘adolescent’ and ‘school/high school’ (median 2 per policy; range 0–83). The terms ‘paediatric’ and boy/girl were used rarely (median 0 per policy; range 0–11).
All data related to the relevance of paediatric athletes, type of research referenced, study designs and topics are summarised in table 2.
Quality assessment with the AGREE II tool
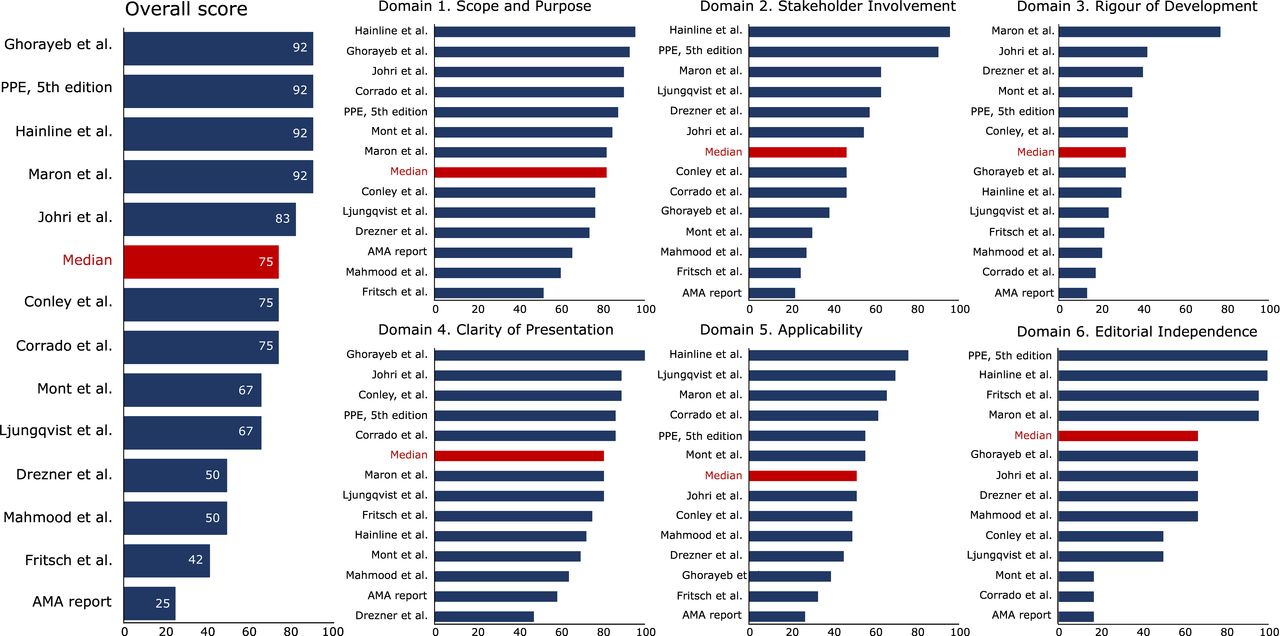
The overall quality of the policies was between 25% and 92%, with a median score of 75%. The higher scoring domains were Scope and Purpose (53%–97%, median 83%) and clarity (47%–100%, median 81%), with most guidelines being well presented in a clear and concise manner. The lowest scoring domains were rigour of development (14%–78%, median 32%) and stakeholder involvement (22%–97%, median 47%), owing to almost no use of systematic search methodologies and a lack of inclusion of non-medical stakeholders (All domain scores are shown in figure 4 and online supplemental table 2).
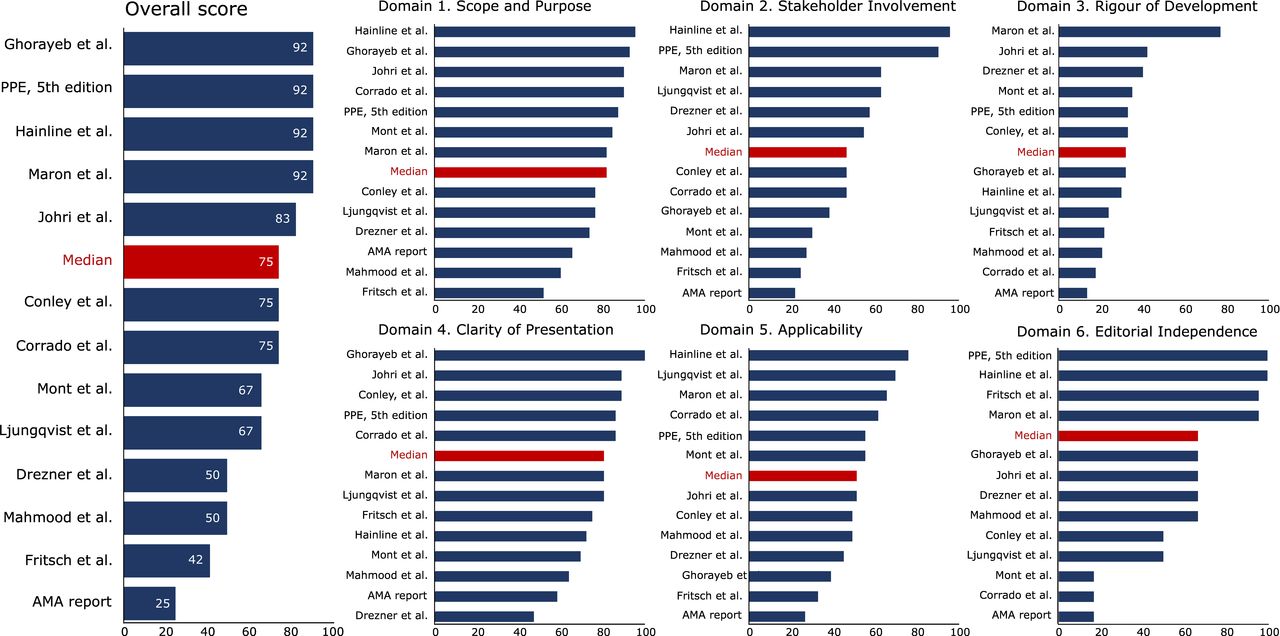
Quality appraisal scores calculated using the AGREE II instrument.16Overall scores (left panel), each of the six domain subscores (right panel). Sorted from highest to lowest, with median value in red. AGREE II, Appraisal of Guidelines for Research & Evaluation II.
Domain 1: scope and purpose
The median score in this domain was 83% (53%–97%), with only one policy paper19 being assessed with a low score of 53%. Lower scores were generally due to lack of clarity in defining the target population (Q3), especially in clearly defining the target age (with uses of undescriptive terms such as ‘young’ or ‘student’) or the type of athletic participation (amateur vs professional), but less so due to defining the clinical question or objectives discussed (Q1 and Q2).
Domain 2: stakeholder involvement
The median score in this domain was 47% (22%–97%), with two policies achieving high scores, of over 80%.21 29 Various medical professions were well represented, still limited to sports medicine/connected professions in some cases (Q4). The input from public, patient or non-medical groups was sought in just 3/13 guidelines (Q5), while 6/13 policies had issues in clearly defining the professional target group (Q6).
Domain 3: rigour of development
The median score in this domain was 32% (14%–78%), with one policy scoring a satisfactory 78%.24 Only one policy described a systematic approach to the literature search (Q7), presented clear criteria for selecting included studies (Q8) or the methodology for selecting the recommendations (Q10). The strengths and limitations of the discussed literature was generally mentioned in all policies, but only in 3/13 was this written in a clear, separate subsection (Q9). Benefits, risks and side effects were discussed in most policies, and in 5/13 this was conducted in clearly identifiable sections or paragraphs (Q11). Just two policies linked key references or offered level of evidence data for each individual recommendation. In all other cases it was either generally discussed in the text or otherwise difficult to assess (Q2). Although most of the policies were published in peer review journals, in just two instances was external peer review before publication explicitly mentioned in the manuscript. (Q13). None of the included policies offered any clear framework for updates, at most suggesting discussions for future directions (Q14).
Domain 4: clarity of presentation
The median score in this domain was 81% (47%–100%). Two policies scored low, under 70%,27 28 attributed to ambiguously formulated recommendations (Q15), which were not clearly separated from the majority of the discussions (Q17). An issue present in most policies was the lack of an exhaustive discussion regarding all screening modalities and relevant issues, but rather limiting this to physical examination and ECG (Q16).
Domain 5: applicability
The median score in this domain was 52% (27%–77%), with two policies scoring satisfactory.21 26 In only 3/13 policies were facilitators and barriers to implementing the recommendations clearly discussed in a separate section, while in most other statements this featured throughout the text (Q18). Tools for aiding recommendations were either provided or referenced in 7/13 policies (Q19). There was a separate discussion of the resource utilisation in 6/13 of the policies, with most other still tangentially discussing the topic (Q20). In only two guidelines was there any mention of mechanisms for overseeing the implementation of the recommendations (Q21).
Domain 6: editorial independence
The median score in this domain was 67% (17%–100%), with three policies scoring very low.2 25 28 The scores varied significantly due to missing editorial independence statements from the supporting organisation in 8/13 cases (Q22) and incomplete documentation of the conflict of interest of authors in 4/13 cases (Q23). As such, these scores did not reflect a lack of editorial independence but rather a lack of uniform documentation in the published manuscript.
Discussion
In this systematic review of available policies published in the peer-reviewed literature for the cardiovascular screening of athletes, we demonstrate that out of the 13 included, just 3 were found to be highly relevant to paediatric athletes. The quality judgement of the policy, as evaluated using the AGREE II tool, varied greatly, with particular improvement needed in the Rigour of Development, Applicability and Stakeholder involvement domains, which concurs with the limitations found regarding paediatric relevance. Newer documents did score better overall, but as these findings show, more work is required both in conducting original research and the methodology to develop consensus to improve athlete screening recommendations for paediatrics (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Summary of review process, key findings, and future considerations. AGREE II, Appraisal of Guidelines for Research & Evaluation II.
Relevance of current policies to paediatric athletes
‘We recognise that young competitive athletes (<18 years) require specific expertise in the evaluation, interpretation of findings and management’.26
This statement from the International Olympic Committee in 2009 shows that for over a decade the need for paediatric specific guidance has been apparent. Yet within our review in 2022, there is still ambiguity with the applicability of screening recommendations for this age group, as only two provide specific guidance for athletes aged 12–18 years. The remaining documents either failed to state the age range or included one that incorporated both children and adults. One reason for the limited tailoring of the policies to the paediatric athlete is the sparse availability of research data to provide evidence-based guidance. Concurrently, there is also a lack of a systematic approach in the literature search, with seven policies citing less than four original articles investigating cardiac screening in this age group.
Quality appraisal of current screening policies
The 13 policies we identified in the present review performed generally well in each domain, yet the limited search strategies used within the policies was highlighted in finding that ‘rigour of development’ was the poorest performing domain within the AGREE II analysis. This domain assesses the processes used to gather and synthesise the evidence, and the methods used to formulate the recommendations. When formulating recommendations, the Institute of Medicine describes literature searching as the key step in developing valid guidelines.30 Yet the search strategy was reported in only one policy within our review. Not performing a systematic review to guide policy creation may ultimately introduce certain biases, such as selective citation, producing less valid, reliable and accurate recommendations.31 The 2014 AHA policy,24 which according to the organisations methodology manual, did include a systematic search, cites 20 articles directly relating to the screening of paediatric athletes, emphasising that more recent policies have failed to account for sections of the available literature.
We also identified several aspects for improvement, particularly in relation to document development and rigour, applicability and stakeholder involvement. Prior to formulating any document, a key question here is who should participate.32 Despite dissent and discussion being stated as the foundations on how we improve science,33 just one policy22 reported areas of disagreement among the panel. There have also been calls for panel members to disclose their personal leaning on contentious issues prior to consensus meetings.34 One policy that did this was that of Drezner et al,27 by purposefully selecting the panel to provide a balanced view on ECG utilisation. Beyond panellists with different views, a multidisciplinary panel is also necessary to limit any issues of equity, diversity and inclusivity.32 This is particularly important within athlete screening policies where there are numerous stakeholders involved. Yet only the AHA policy addressed the important role of both patient and legal representation.24
Do we need separate paediatric guidelines?
Up to 40% of all children are registered in official teams,35 with the paediatric age group representing the largest population of all athletes. Despite this representation, of the research cited in the policies that included paediatric athletes, 77% used cohorts that included a combined sample of paediatric and adults. This action of grouping young athletes into the broad category of 12–35 years is common not only in the available literature but the policies themselves. Thus, care must be taken in applying these findings to the specific paediatric cohort, as there is no indication that they are transferable, and may even mask potentially important nuances that arise in the maturing athlete.
Child athletes can develop profound physiological cardiac remodelling9; and like the adult athlete, create the diagnostic dilemma of differentiating between physiological and pathological adaptation. Age is now considered within the athlete ECG11 and echocardiogram guidelines,12 13 and although we know that the paediatric athlete differs in several aspects to the mature adult athlete, no policy discussed in any detail the nuances of screening this population; with mention of paediatric related terms being as infrequent as one per policy.
Adolescence is a period when genetic cardiac disease may present for the first time, however, the beginning of the adolescent growth spurt can range from 9.5 to 16 years,36 37 while skeletal maturation may not be reached until the age of 19 years or beyond.38 Together with the unpredictability of disease penetrance during adolescence,39 it means that a single screening before this time may allow a cardiac condition to go undetected.6
In addition, to ensure diagnostic accuracy for this age group, age-specific normative values and tailored approaches to disease management are also needed.8 40 One such consideration is that of biological maturation. While not acknowledged within any screening policy, using biological instead of chronological age may improve diagnostic accuracy substantially.41 While caution is warranted in applying ECG and echocardiographic criteria without due attention to maturational status, its assessment is not without challenges. The Tanner assessment is easily conducted but has ethical and child-protection considerations, while the wrist X-ray of biological assessment elicits exposure to radiation42 and would require increased resource utilisation, introducing potential barriers to access.
Within this systematic review, just the policy of Ghorayeb et al,20 provides tailored guidance specifically for the paediatric athlete with the recommended use of ECG. These recommendations from Brazil, however, do not discuss their tailored approach to age in detail, and cite just one article related specifically to the screening of paediatric athletes.43 It is outside the scope of this review to assess the quality of the research cited, however, we found the majority of cited literature to be of a cross sectional design. With robust data lacking that asserts cardiac screening to be effective in reducing the incidence of SCD, in not only paediatric but adult athletes, the debate between screening approaches continues. This is exemplified by a clear continental split in policies recommending (5) vs not recommending (7) the use of ECG with the screening remit. In such situations where there is conflicting evidence, it has led to current policies generally coming from consensus or position statements, as opposed to clinical practice guidelines.44 45
Moving forward
As found in our review, the timing of initial cardiac screening varies significantly depending on the policy, with a potential 9-year discrepancy. Several policies recommend cardiac screening to begin at the onset of competitive activity, meaning athletes as young as 5–8 years old would be screened.46–48 Overall, the lack of consensus is evident in our systematic review, with little guidance on the topic. In addition, some recommendations altered their own lower age range from 14 to 12 years old, despite no change in the research base.11 49
With policies recommending screening to be undertaken in the preadolescent years, a thorough understanding of the issues relevant to paediatric cardiac screening is required, including the rapid yet highly variable pubertal changes, legal responsibilities of sports governing bodies and managing the complex relationship between physician, parent and patient. Both the ESC50 and AHA51 have outlined core curricula required for effective sports cardiology practice, yet these do not involve documenting competency in the evaluation of paediatric athletes. While American College of Cardiology curriculum51 does state that collaboration with paediatric cardiologists is needed, there is a distinct lack of such specialists available to interpret all paediatric screenings.24 52 Consequently, forming valid and reliable guidelines together with certified educational pathways is imperative (table 3).
Future policy recommendations for the screening of paediatric athletes
Limitations
By including only policies written in the English language, some national policies may have been omitted. There is currently no validated methodology of performing systematic searches of non-indexed sources, and therefore, policies that were not published, peer-reviewed, or indexed would not have been included. This may have been overcome by implementing an online search of known sporting organisations, yet this would be logistically difficult to avoid selection bias. To account for this, it may be prudent for sporting organisations to hereafter publish their screening policies; to not only allow for inclusion in future systematic reviews but to publicise their policy more broadly. The method of evaluating relevance was not based on previous work, nevertheless, we sought to adopt a more objective way of quantifying how the general body of literature was used in each policy paper, and how the paediatric subset of work was used. Finally, the AGREE II tool was designed to evaluate the quality of guideline papers, with a goal to ensure uniformity in approach and reporting. Having found areas scoring poorly among the papers reviewed in this study, it is less a reflection of the authors and more a reflection of the limitations of the field, which extends to the referencing of the original research. Identifying these limitations, and showcasing how more recent documents have improved, may encourage future work is of even higher quality.
Conclusion
Cardiac screening policies predominantly focus on adult athletes, with the data guiding these recommendations chiefly coming from studies that involve cohorts of athletes that combine both children and adults. There is an immediate need for paediatric specific research that accounts for age, sex, training status and maturation, to develop a database of normal and abnormal findings that inform screening guidelines. Expanding paediatric cardiology expertise in the care of young athletes and ensuring the development of certified educational pathways in cardiac screening for primary care and sports medicine physicians should be considered. For future guidelines, more robust development methods are needed in their planning and creation, using systematic and reproducible methodologies, with involvement of all key stakeholders, to improve cardiac care for paediatric athletes.
Ethics statements
Patient consent for publication
Acknowledgments
Dr Nathan R. Riding is supported by a Canon Medical Systems fellowship in sports cardiology. Dr Dan M. Dorobantu is supported by a doctoral scholarship (grant MR/N0137941/1 for the GW4 BIOMED DTP, awarded to the Universities of Bath, Bristol, Cardiff, and Exeter from the Medical Research Council (MRC)/UKRI. Prof. Guido E. Pieles is director of the sports cardiology consulting company 'Cardiac Health and Performance'. AGS is Medical Director of 'Sports Cardiology UK'—a company, which specialises in the assessment and management of athletes with cardiovascular problems.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Nathan_Riding, @ag_stuart
Contributors The review was conceptualised by NRR and GP, with NRR DMD and GP contributing to the design. NRR applied the search strategy. NRR, DMD and GP applied the selection criteria, performed the data extraction and the guideline assessment. NRR and DMD analysed the data. NRR and DMD drafted the manuscript. All authors contributed to data interpretation and critically revised the manuscript. The corresponding author confirmed that all authors met authorship criteria.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.