Article Text

Abstract
Objective Investigate whether hyoscine patch or glycopyrronium liquid is more effective and acceptable to treat drooling in children with neurodisability.
Design Multicentre, single-blind, randomised controlled trial.
Setting Recruitment through neurodisability teams; treatment by parents.
Participants Ninety children with neurodisability who had never received medication for drooling (55 boys, 35 girls; median age 4 years). Exclusion criteria: medication contraindicated; in a trial that could affect drooling or management.
Intervention Children were randomised to receive a hyoscine skin patch or glycopyrronium liquid. Dose was increased over 4 weeks to achieve optimum symptom control with minimal side-effects; steady dose then continued to 12 weeks.
Primary and secondary outcomes Primary outcome: Drooling Impact Scale (DIS) score at week-4. Secondary outcomes: change in DIS scores over 12 weeks, Drooling Severity and Frequency Scale and Treatment Satisfaction Questionnaire for Medication; adverse events; children’s perception about treatment.
Results Both medications yielded clinically and statistically significant reductions in mean DIS at week-4 (25.0 (SD 22.2) for hyoscine and 26.6 (SD 16) for glycopyrronium). There was no significant difference in change in DIS scores between treatment groups. By week-12, 26/47 (55%) children starting treatment were receiving hyoscine compared with 31/38 (82%) on glycopyrronium. There was a 42% increased chance of being on treatment at week-12 for children randomised to glycopyrronium relative to hyoscine (1.42, 95% CI 1.04 to 1.95).
Conclusions Hyoscine and glycopyrronium are clinically effective in treating drooling in children with neurodisability. Hyoscine produced more problematic side effects leading to a greater chance of treatment cessation.
Trial registration numbers ISRCTN75287237; EUDRACT: 2013-000863-94; Medicines and Healthcare Products Regulatory Agency: 17136/0264/001-0003
- drooling
- saliva
- treatment
- children
- neurodisability
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this subject?
Drooling saliva is common in children with neurodevelopmental disorders. Negative consequences include skin breakdown, dehydration, damage to clothing and equipment and social embarrassment.
Most UK paediatricians prescribe hyoscine first and glycopyrronium second. There is no comparative evidence about the effectiveness, side effects or patient acceptability of these medications.
What this study adds?
Hyoscine and glycopyrronium are both clinically effective in treating problematic drooling in children with neurodisability.
Hyoscine is associated with more problematic side effects than glycopyrronium and is less likely to be tolerated by children and parents.
Where either medication might be used, glycopyrronium should be the medication of first choice—the opposite situation to current UK prescribing practice.
Introduction
Drooling saliva is a common problem in children with neurodisability.1–3 The negative consequences of drooling include skin breakdown on the child’s chin and damage to clothing and equipment. Children and family members experience social embarrassment due to the physical appearance of drooling.4–6 Bibs or wristbands may be used to soak up saliva and clothing changes with extra washing loads are required.4 7
Anticholinergic medication is used to treat problematic drooling. In a UK clinical practice survey,8 98% of paediatricians reported using such medication: 85% used hyoscine delivered by skin patch as first-line treatment and glycopyrronium liquid second. Other treatments for drooling are used but have drawbacks.9 10 There is inadequate evidence about the relative effectiveness of hyoscine or glycopyrronium.11 12 Both medications have predictable, dose-dependent side effects and reported neurological effects.4 As there are limited data about how children and parents balance side effects against reduction in drooling, it is difficult for children, parents and doctors to decide which medication to use, at what dose. Comparative effectiveness trials of different treatment approaches are needed in child health generally and in paediatric neurodisability.13
We report a randomised comparative effectiveness trial designed to investigate increasing dosages of medication to treat problematic drooling (hyoscine skin patches and liquid glycopyrronium). We aimed to identify whether, at maximal tolerated dose, one medication achieved a better balance than the other between effectiveness and side effects and make recommendations for future standards of care for children with significant drooling.
Methods
The Drooling Reduction Intervention (DRI) trial protocol is an open access publication.14 Key elements are summarised briefly.
Design
Multisite, prospective, single-blind, pragmatic, randomised controlled comparative effectiveness trial of treatment with hyoscine skin patch or glycopyrronium liquid for children with neurodisability and problematic drooling.
Trial population
Ninety children from 15 UK National Health Service (NHS) neurodevelopmental teams recruited over 17 months. Inclusion criteria: children with no progressive deterioration of neurological function; no previous medical/surgical treatments for drooling (treatment naïve); requiring medication to reduce drooling; no contraindication to either medication; age >35 months to <16 years; weight ≥10 kg. Exclusion criteria: Children who had received treatments for drooling; parents unable to follow study protocol or complete a telephone call in English; previous study withdrawal; in a trial of medication that could interact with drooling management; pregnant.
Identification and recruitment of participants
Recruitment of participants was by consultant neurodevelopmental paediatricians through routine UK NHS care. Written consent was taken. Assent was sought from children where appropriate. Participants could withdraw and return to usual local clinical care.
Randomisation and blinding
Participants were randomised using the Newcastle Clinical Trials Unit web-based service. Participants were allocated to hyoscine or glycopyrronium (ratio 1:1), stratified by recruitment site and drooling severity using the modified Mier classification: saliva usually on lips and chin or saliva on lips chin and clothes.15 Medication type was not known to the ‘outcome assessor’.
Intervention
Children received hyoscine patches or glycopyrronium liquid according to an escalation protocol.14 16 Medication was increased weekly from week-1 to week-4 to the dose needed to stop drooling or to the maximum allowed dose or to the maximum associated with tolerable adverse effects. Thereafter, participants remained on the week-4 medication dose for 8 weeks.
Children randomised to hyoscine received the following regime: week-1: ¼ patch; week-2: ½ patch; week-3: ¾ patch; week-4: full patch. The patch was typically placed below an ear with an occlusive dressing applied over and replaced every 3 days, alternating sites to minimise local skin reaction risk. The plastic patch backing was cut to expose the prescribed portion of the patch; the patch itself was not cut to avoid leakage of product from the non-loculated reservoir. Children randomised to glycopyrronium liquid received three doses per day: week-1: 40 µg/kg/per dose; week-2: 60 µg/kg/per dose; week-3: 80 µg/kg/per dose; week-4: 100 µg/kg/per dose to a maximum 2 mg per dose. Medication was given orally or by feeding tube.
Outcome measures
Primary outcome: Drooling Impact Scale (DIS) score at 4 weeks (range 0–100, SD 13).17 It is a parent-reported outcome measure, addressing psychosocial impacts and drooling itself.
Secondary outcomes: change in DIS and Drooling Severity and Frequency Scale (DSFS) scores between baseline, week-4 and week-12 and difference between groups in the Treatment Satisfaction Questionnaire for Medication (TSQM) score at week-4 and week-12. The DSFS18 captures parent report of drooling severity and drooling frequency. The TSQM19 has four domains: effectiveness, side effects, convenience and global satisfaction.
Trial procedures
Medication was prescribed locally (see table 1 14). Parents received: medication; parent information sheets; occlusive dressings (hyoscine) or syringes (glycopyrronium). Parents received telephone calls to week-12 from a trial paediatrician with expertise in drooling management (ET/JP/AC). Information about drooling reduction and side effects was sought using a standardised report form (available from the author). Questions covered predictable side effects16: unable to use/tolerate the patch or medication; skin reactions (hyoscine); constipation; dry mouth/respiratory secretions; vision difficulties; urinary side effects; skin flushing/dryness; vomiting; seizures; drowsiness; dizziness. Non-predictable side effects were also recorded. Participants with significant side effects had medication decreased to the previous dose; briefly interrupted or stopped. The trial paediatrician completed with parents the TSQM.
Baseline characteristics of the 90 children randomised
Parents were telephoned by an outcome assessor (SN and LP), blind to treatment arm, who completed with parents the DIS and DSFS at baseline, week-4 and week-12 or when medication stopped. Parents were informed in the information sheet and reminded at telephone calls that outcome assessors were blind to medication type.
Interviews with children
Children able to self-report were interviewed by ET about their experiences of drooling medications after week-12. Children were asked: to rate on a five-point scale ‘how bad their drooling was currently and before starting medication’; if medication helped them and how; how they felt while taking medication. Pictures of body parts and home settings assisted discussions.
Statistical methods
Statistical analyses were undertaken in Stata20 following a statistical plan agreed before data were unblinded. Analyses were based on two populations: intention-to-treat group (ITT) of all patients, retaining children in their randomised treatment groups; treatment-tolerated group (TT) of all patients who were still on their starting treatment at 12 weeks.
The primary analysis of the primary outcome measure used the ITT group. DIS scores recorded 26–35 days inclusive from the start of treatment were included. If one or two components of the child’s DIS score at week-4 were missing, their total DIS score was scaled proportionately; if three or more components were missing, their DIS score was excluded. DIS scores for the two randomised groups are presented with 95% CIs for the mean difference between groups. A bias corrected bootstrap was applied using 5000 bootstrap replicates. Analysis of covariance was used to compare week-4 DIS scores between treatment groups adjusted for the stratification factor of baseline drooling severity, reporting the coefficient (SE) for the stratification factor and adjusted treatment effect.
Secondary analysis of the primary outcome measure was adjusted for the stratification factor baseline drooling severity and covariates age, sex and baseline DIS score. Repeated measures analysis of variance investigated the DIS over time. Secondary outcomes DSFS and TSQM are reported descriptively.
Sample size: The study was powered to detect a clinically significant difference of 10 points in mean DIS score at 4 weeks between groups, assuming previously reported SD of 13, representing parents views as the difference between ‘very good to excellent’ and ‘good’ in a global rating.17 To detect this difference with 90% power and type 1 error of 5%, required a minimum of 36 children per group. Inflated for a 20% loss to follow-up yielded a target of 90 children.
Trial management, quality assurance and regulatory issues
The trial was managed through the Newcastle Clinical Trials Unit. Medicines and Healthcare Products Regulatory Agency approval was obtained: 17136/0264/001–0003. A Data Monitoring Committee monitored efficacy and safety endpoints using unblinded interim data and reported to an independent Trial Steering Committee.
Results
Ninety children were randomised, 55 (61%) boys and 35 girls, median age 4 years (range 3–14). Recruitment per site ranged from 1 to 15 children (median 6). In 78 children (87%), drooling affected their clothing and in 12 drooling only affected the lips and face. Forty-nine children were randomised to hyoscine and 41 to glycopyrronium (table 1). Baseline mean DIS scores were similar in both arms (hyoscine 57.9 (SD 15.5, range 26, 85) vs glycopyrronium 52.1 (SD 12.7, range 25, 75)). Children’s diagnoses were: cerebral palsy 22; developmental delay/disorder 22; genetic conditions 14; autism spectrum disorder 12; learning/intellectual disability 10; structural brain disorders 6; Down syndrome 5; miscellaneous 14. Three-quarters had multiple diagnoses (up to seven per child) and two-thirds took one or more medications (up to seven per child).
Following randomisation, 85 children started treatment: 47 hyoscine, 38 glycopyrronium (figure 1). By week-4 and week-12 children randomised to hyoscine were less likely be on medication than children randomised to glycopyrronium due to unacceptable side effects (reported below). By week-12, 26/47 (55%) children starting treatment were receiving hyoscine compared with 31/38 (82%) on glycopyrronium. There was a 42% increased chance of still being on treatment at week-12 for children randomised to glycopyrronium relative to hyoscine (risk=1.42, 95% CI 1.04 to 1.95).
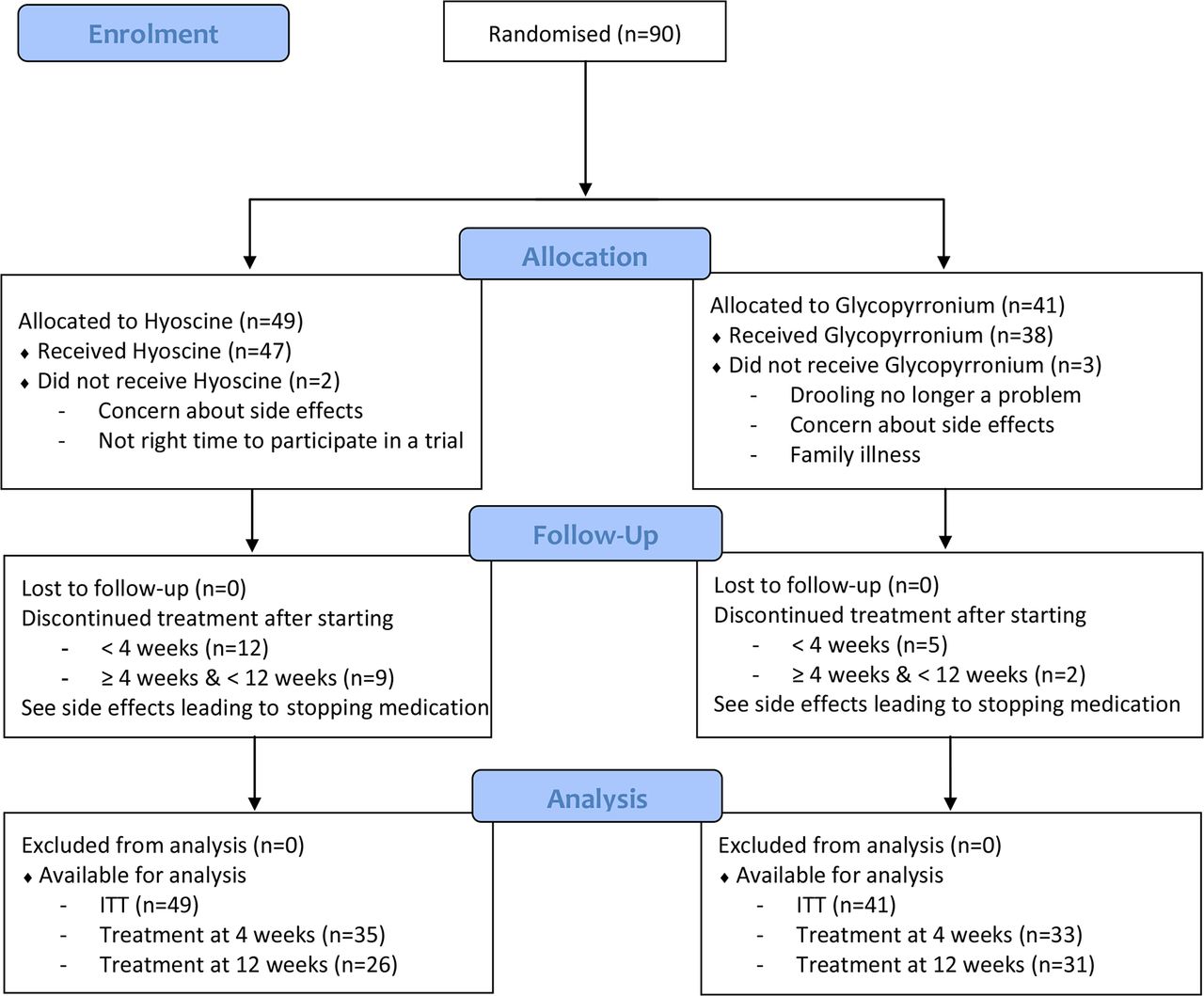
Consort diagram. ITT, intention to treat.
Primary outcome measure
Seventy children (78%) had week-4 DIS assessments at 26–35 days inclusive. Thirteen children (14%) had assessments outside the required window and two started treatment but stopped before week-4.
Mean week-4 DIS scores were 32.1 (SD 19.4) in 41 children receiving hyoscine and 25.3 (SD 14.1) in 29 children receiving glycopyrronium. There was no significant difference in week-4 DIS scores between treatment groups. Both hyoscine and glycopyrronium led to statistically significant reductions in DIS scores from baseline to week-4 (Bonferroni corrected p<0.0001) with similar reductions in both treatment arms. Mean change in DIS from randomisation to 4 weeks was 25.0 for hyoscine (SD 22.2, 95% CI 18.0 to 32.0) and 26.6 for glycopyrronium (SD 16.0, 95% CI 20.5 to 32.7).
The mean week-4 DIS score was higher for hyoscine than for glycopyrronium with an unadjusted estimate of the difference in mean scores of 6.8 (95% CI −1.6 to 15.3) (table 2, Model 1). Children with more severe drooling at baseline tended to have higher week-4 DIS scores, mean difference of 5.9 (95% CI −8.0 to 19.8) (table 2, Model 2). Controlling for drooling severity, age at randomisation and baseline DIS score the adjusted estimate of the difference in mean week-4 DIS scores between randomised groups was 4.0 (95% CI −4.4 to 12.5) (table 2, Model 3).
Adjusted estimates of the treatment effect of DIS at week-4
There was a risk that 4-week data collected just outside the 26–35-day window (eg, some people were inevitably difficult to contact due to illness or holidays) would not be used and might influence interpretation. Therefore, a sensitivity analysis of the primary outcome at week-4 was conducted, based on the ITT group and including those whose DIS had been collected outside the protocol window. This did not alter the conclusions.
Secondary outcome measures
For the ITT group, mean week-12 DIS scores were 31.0 (SD 19.3) in 38 hyoscine patients and 23.8 (SD 17.5) in 33 glycopyrronium patients. No difference was observed between week-4 and week-12 DIS scores for either the hyoscine and glycopyrronium groups: mean hyoscine change 1.4 (SD 25.5), mean change glycopyrronium −1.1 (SD 15.8) (figure 2). A sensitivity analysis compared the TT group week-12 DIS scores for the medication and did not alter conclusions. This was important to conduct since the ITT group at 12 weeks could include children who had stopped their trial medication and been changed to the medication of the other trial arm by their local paediatrician to whom care had been returned.

{kind=link}
{kind=link}
Mean Drooling Impact Scale scores at baseline, week-4 and week-12 for the intention-to-treat group (with 95% CI).
Mean DSFS scores at baseline were similar (table 1) (mean 7.5 (SD 1.1) for hyoscine, mean 7.6 (SD 1.1) for glycopyrronium) and were reduced for both hyoscine and glycopyrronium at week-4 (mean 5.1 (SD 1.8), 4.7 (SD 1.9), respectively), with similar reductions at week-12 (mean 4.7 (SD 1.6), 4.7 (SD 1.9), respectively).
There were no observed differences in mean TSQM domain scores between hyoscine (n=33) and glycopyrronium (n=31) at week-4: Effectiveness (79.5 (SD 17.2), 86.8 (SD 9.8)); Side Effects (96.0 (SD 13.4), 98.1 (SD 5.1)); Convenience (79.1 (SD 15.2), 85.8 (SD 12.0)). A somewhat lower week-4 Global score for hyoscine (74.5 (SD 15.6), 86.3 (SD 13.5)) may reflect reduced hyoscine compliance. Week-12 scores for all domains were similar.
Predictable side effects
Predictable side effects were reported less frequently by parents of children who received hyoscine 22/47 (46.8%) than glycopyrronium 24/38 (63.2%). Those most commonly reported for hyoscine and glycopyrronium respectively were: unwell 14/47 (29.8%) vs 15/38 (39.5%); constipation 5/47 (10.6%) vs 12/38 (31.6%); excessive drying of respiratory/oral secretions 3/47 (6.4%) vs 7/38 (18.4%); skin flushing/dryness 8/47 (17.0%) vs 3/38 (7.9%). Other side effects were seen in less than two children per treatment arm.
Problematic side effects leading to stopping medication
Hyoscine was associated with more problematic predictable side effects leading to children stopping medication than glycopyrronium. Seventeen parents from the hyoscine arm reported a predictable side effect that led to cessation of their child’s medication (11 with skin reactions to patches (redness, blistering, swelling, skin breakdown, some of which only started after many weeks in the trial), one with dry mouth, one with pupil dilation and four repeatedly pulled off their patches). This compares to only six parents reporting a predictable side effect leading to cessation of glycopyrronium (two with dry mouth, two with constipation and two with skin dryness or rash).
Children receiving hyoscine also stopped medication due to non-predictable side-effects more frequently than those receiving glycopyrronium. Seven children on hyoscine stopped medication (three with unsteady walking, two with hyperactivity, one with floppiness, one with increased seizure activity). One child on glycopyrronium stopped medication due to hyperactivity. Some parents cited more than one side effect as the reason for stopping medication.
Interviews with children and young people
Interviews were conducted with two children receiving hyoscine and four receiving glycopyrronium. All communicated verbally. All rated their drooling as bad or very bad before medication. One child stopped taking glycopyrronium at 3 days because her mouth dried and she thought she was going to choke when eating. The five children still on medication when interviewed rated their drooling as ‘good’ or ‘very good’ and said their chin was dry and no longer sore and their clothes remained dry. Other positive observations were: friends no longer tease me (n=2); school work and computers remain dry (n=1); no saliva spray when talking (n=1). Negative observations were the hyoscine patch caused itching and glycopyrronium having an unpleasant taste.
Discussion
The randomised DRI trial is the first to use a protocol with standard dose escalation and side effect monitoring, to compare directly the effectiveness of hyoscine and glycopyrronium for the treatment of drooling in children with neurodisability. For both medications, the improvement in the DIS score was statistically and clinically significant. While hyoscine patches were well tolerated by some children, almost half parents stopped medication (21/47, 45%)—significantly higher than for glycopyrronium which was associated with fewer problematic side effects and was better tolerated. Skin reactions to hyoscine and intolerance of the patches frequently caused difficulties. Predictable and non-predictable side effects made hyoscine less acceptable to parents than glycopyrronium whose side effects were self-limiting or could be treated (eg, increasing doses of constipation medication). Hyoscine treatment by patch has been favoured by some because it is effective and they think it is a more convenient method of administration than three times daily oral medication.8 Further, glycopyrronium has only hitherto been available as a 1 mg/5 mL solution with a 28-day shelf life. As there are now also 1 mg/mL preparations with a shelf life of 1 year and a licensed preparation for children, we think our study shows glycopyrronium liquid should be the medication of first choice.
Regarding study strengths, this multicentre, prospective, pragmatic, randomised, controlled trial recruited children across the UK from regions with varying deprivation and population characteristics. Paediatricians deliver high-quality assessments of children with neurodisability and advise on management.21 22 Participants in the trial arms were comparable at baseline. Trial blinding was effective because none of the parents divulged the child’s treatment group to the blinded outcome assessor. Both medications are in routine NHS use. Data were systematically gathered using methods designed with parents.14 Five out of 90 (5.5%) of families did not start medication; there was no loss to follow-up.
Regarding study limitations, we relied on parent report of side effects; in children with limited communication ability, this may have underestimated such effects.23–25 The trial was blinded where possible; however, parents were not blind to the medication they received; their experience of medication might have affected their responses to outcome assessor questionnaires. As the TSQM focuses on information about side effects and satisfaction, these data were gathered by the non-blinded trial paediatrician; it is possible this could introduce bias. Individual diagnostic neurodisability groups were too small for subgroup analysis. We recruited families where parents could speak sufficient English by telephone. We are not able to comment on the representativeness of the children recruited; however, the range of diagnoses, other conditions and other medications received was in line with our expectations from clinical practice.
These trial results indicate that where neither medication is contraindicated or definitely preferred, glycopyrronium should be the drug of first choice. In the future, additional data gathered systematically from clinical samples about the medications will add to the evidence base. We consider introduction of medication using a stepped protocol should be undertaken before considering other treatments.10 11 The protocol of weekly phone calls for 4 weeks to adjust dosage in the light of drooling response and side effects was acceptable to parents and can be used by clinical teams (protocol is freely available from the corresponding author). Such a protocol should be considered for incorporation into guidance for drooling treatment. Evaluation of the effectiveness of a telephone delivered stepped protocol should be undertaken, to show whether it is feasible and useful to clinicians, parents and children in clinical practice.
Acknowledgments
The trial was conceived by the Strategic Research Group of the British Academy of Childhood Disability (BACD-SRG) and taken forward by Parr, Pennington and Colver with the BACD’s ‘Drooling Development Group’. The authors are grateful to colleagues for their early input into the development work and trial design. We acknowledge the support of the National Institute for Health Research Clinical Research Network and the Medicines for Children Research Network. We thank: The Principal Investigators at each site who are not also coauthors; Drs Jonny Cardwell (Northumbria NHS Foundation Trust), Helen Clements (Sherwood Forest Hospitals NHS Foundation Trust), Chelvi Kukendra (North West London Hospitals NHS Foundation Trust), Anne Ferguson (Central Manchester University Hospitals NHS Foundation Trust), Melissa Gladstone (Alder Hey Children’s NHS Foundation Trust), Neil Harrower (Sheffield Children’s NHS Foundation Trust), Neal McCathie (Birmingham Community Health Care Trust), Leighton Philips (Musgrove Park NHS Foundation Trust), Alison Rennie (NHS Greater Glasgow and Clyde), Gill Robinson (Leeds Community Healthcare NHS Trust), Sarah Steele (Norfolk and Norwich University Hospitals NHS Foundation Trust); Research nurses, pharmacists and Research and Development staff at all recruiting sites; Newcastle upon Tyne Hospitals Clinical Trials Pharmacy staff, in particular Yan Hunter-Blair, David Caulfield and Anne Black. Newcastle Clinical Trials Pharmacy purchased hyoscine patches and manufactured glycopyrronium liquid. On receiving six-month stability data for glycopyrronium (later extended to 12 months on confirmation of extended stability), the Medicines and Healthcare Products Regulatory Agency granted permission for use of both medications according to the trial protocol. Newcastle Upon Tyne Hospitals NHS Foundation Trust for their Sponsorship of the Trial. We also thank Newcastle University staff including Sarah Nolan the main outcome assessor; Jane Tilbrook for administrative support. Members of the Data Monitoring and Ethics Committee: Professor Nicol Ferrier (Chair), Dr Adi Sharma, Dr Nick Embleton Dr Barbara Gregson; Members of the Trial Steering Committee: Professor Sunil Sinha (Chair), Mr Simon Leuthwaite; Staff of the Newcastle Clinical Trials Unit: Professor Elaine McColl (Director), Jo Morrison, Dr Nick Steen, Dr Gillian Libby, Chris Speed, Lesley Lane, Nicola Howe, Sarah Dunn and Mark Palmer.
References
Footnotes
Contributors JRP was the chief investigator and planned and led the trial. ET undertook most of the telephone consultations to adjust medication and fielded enquires from families (supported by JRP and AFC, who also discussed management with families). DS supervised statistical analyses and wrote statistical aspects of the manuscript. MC contributed to statistical analysis. LP contributed to planning, led on the qualitative work and undertook some discussions with families. JC and CT recruited patients. AEO’H and JW were involved in study design and recruited patients. AC planned the study and was involved in recruiting sites and managing the study. All authors had full access to all of the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis. All authors critically reviewed the manuscript and approved the final version.
Funding The Castang Foundation; WellChild; The British Academy of Childhood Disability (Polani Fund) and The Children’s Foundation.
Competing interests None declared.
Ethics approval Newcastle and North Tyneside1 Research Ethics Committee: 13/NE/0078.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Patient level data and full dataset will be available from the corresponding author once all planned data analysis is complete. Participants’ consent for sharing identifiable data was not obtained; the presented data are anonymised and risk of identification is very low.