Article Text

Abstract
We investigated if contrast-enhanced ultrasound (CEUS) may differentiate community acquired pneumonia (CAP) from lung cancer (LC). Among 1374 patients admitted in a 5-year period for lung opacities, 728 (329 CAP and 399 LC) were investigated by CEUS, comparing the time of appearance, disappearance, duration and pattern of distribution of contrast enhancement (CE). The patients with CAP and LC did not differ in terms of age, time of CE appearance, disappearance and duration or CE distribution. Our data show that the timing and pattern of CE detected by chest CEUS does not distinguish between CAP and LC and overly optimistic beliefs on this matter should be abandoned.
- Lung Cancer
- Pneumonia
- Imaging/CT MRI etc
Statistics from Altmetric.com
Contrast-enhanced ultrasound (CEUS) is a real-time ultrasound technique evaluating tissue perfusion using an ultrasound (US) contrast agent. An injected suspension of gas microbubbles amplifies the backscatter signal, enhancing the echogenicity of the intravascular ‘blood pool’. After obtaining a basal image of a lesion, this is scanned dynamically during contrast enhancement (CE). Registered indications in Europe are cardiac, macrovascular, liver and breast lesions.1 ,2 The possible application of CEUS to pleural/lung conditions has recently been claimed as a safe (only deserving caution in heart failure), repeatable, cheap, radiation-free and complementary approach to differentiate inflammatory and cancerous pulmonary lesions.3 ,4 However, despite the fact that guidelines2 defined its non-hepatic application, a role for CEUS in lung diseases is far from established. We compared CEUS characteristics of community acquired pneumonia (CAP) and lung cancer (LC) lesions in a large sample of patients with chest radiograph opacities consecutively admitted to our Department of Internal Medicine.
Methods
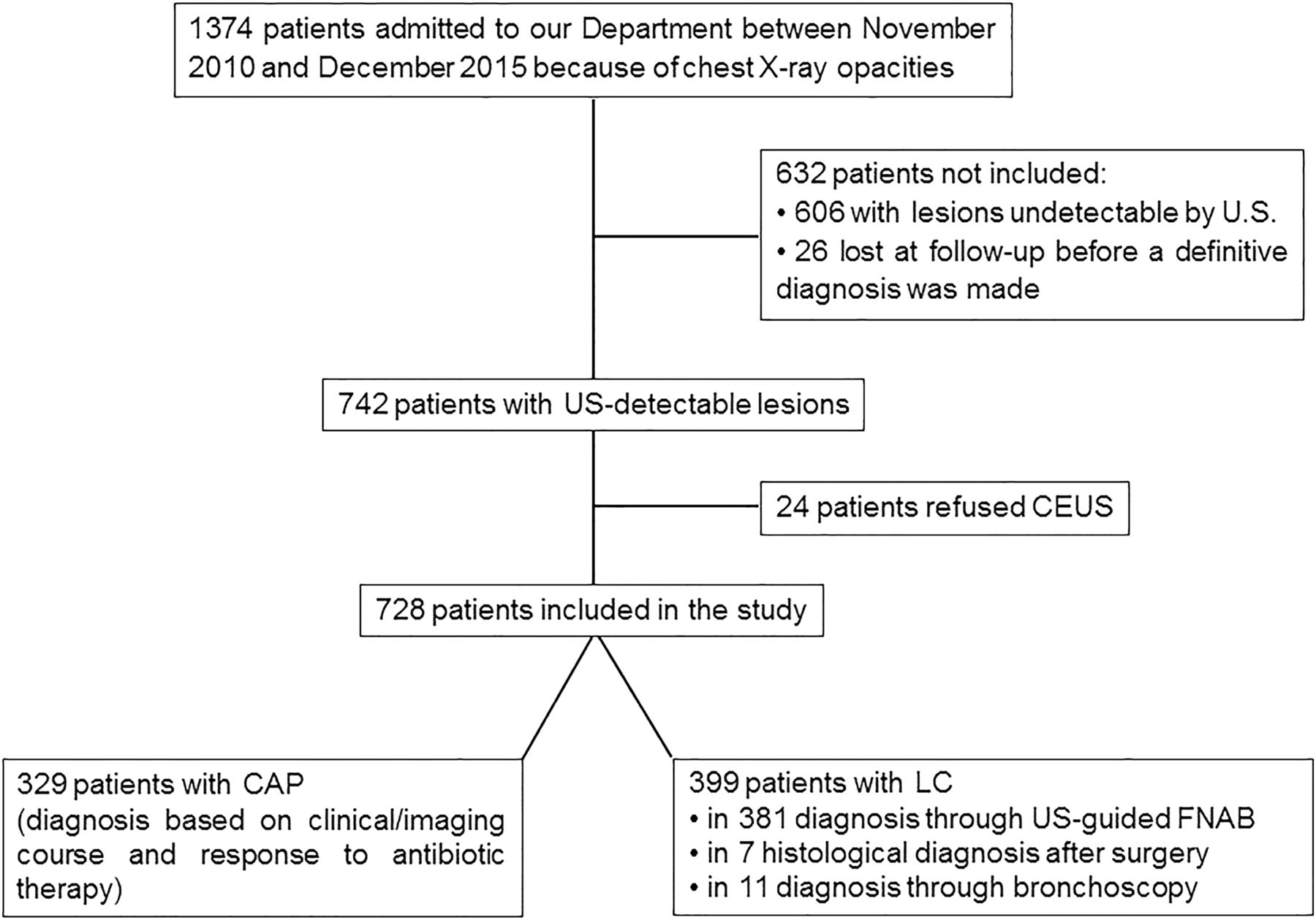
Between November 2010 and December 2015, for 1374 patients admitted to our department because of opacities on chest radiographs, the usual management was supplemented by an US scan of the chest performed shortly after admission. Among the 742 patients with lesions adherent to the pleura (amenable to be adequately explored by US), 728 patients (527 men and 201 women) finally diagnosed with CAP or LC underwent CEUS examination (figure 1). Their results were then compared in light of the definitive diagnosis of CAP or LC, which was not known at the time of CEUS examination. All patients gave informed consent and the study was approved by the local ethics committee.

Flowchart of the study. US, ultrasonography; CEUS, contrast-enhanced ultrasonography; CAP, community acquired pneumonia; LC, lung cancer; FNAB, fine needle aspiration biopsy.
An Esaote Technos MPX and Twice device (Genoa, Italy) using a multifrequency (3.5–5 MHz and 3–8 MHz) convex probe and the pre-setting for thoracic ultrasound in B mode and US contrast setting (low mechanical index) was used. In all patients, bilateral scans were performed in the sitting position through all ventral, posterior and lateral intercostal spaces to exclude the possibility of contrast uptake in other lesions potentially influencing the results. CEUS was then achieved on the US-detected lesion corresponding to the radiograph opacity by a second-generation contrast agent using phospholipid-stabilised microbubbles of sulfur hexafluoride (Sonovue, Bracco, Milan, Italy). A bolus of 4.8 mL of Sonovue followed by 10 mL regular saline was injected intravenously. A CEUS scan was performed with a mechanical index of ≤0.04. The following temporal characteristics of enhancement were detected by a chronometer included in the device: time between injection and appearance of microbubbles; time between injection and disappearance of microbubbles; duration of CE. The pattern of CE was simply categorised using a dichotomous visual score, defining lesions as homogeneous or non-homogeneous, according to the distribution of more or less than 50% within the lesion.5 ,6 A single physician with 25 years of experience in lung ultrasonography performed and digitally recorded all CEUS scans. The clips were blindly reviewed by another operator with 20 years of experience.
Results
The definitive diagnosis (based on clinical course, imaging and laboratory and/or histology tests) was CAP in 329 and LC in 399 patients. After normality testing, the mean times of beginning, end and duration of CE of CAP and LC were compared by the Mann-Whitney U test. There was no significant difference between the investigated parameters for patients with CAP and LC. The respective medians (25–75th IQR) were: age 66 (58–75) vs 65 (59–71) years, p=0.098; time of contrast appearance 24 (19–31) vs 23 (21–30) s, p=0.726; time of CE disappearance 247 (236–257) vs 249 (239–257) s, p=0.230; duration of CE 221 (211–232) vs 223 (213–233) s, p=0.169. A homogeneous distribution of CE was found in 242/329 (73.6%) CAP lesions and in 294/399 (73.7%) LC lesions whereas a non-homogeneous distribution was observed in 87/329 (26.4%) CAP lesions and 105/399 (26.3%) LC lesions. The distribution pattern did not differ significantly (p=0.969, χ2 test). Inter-reader agreement was excellent (Spearman's coefficient ≥0.90 for all parameters).
Discussion
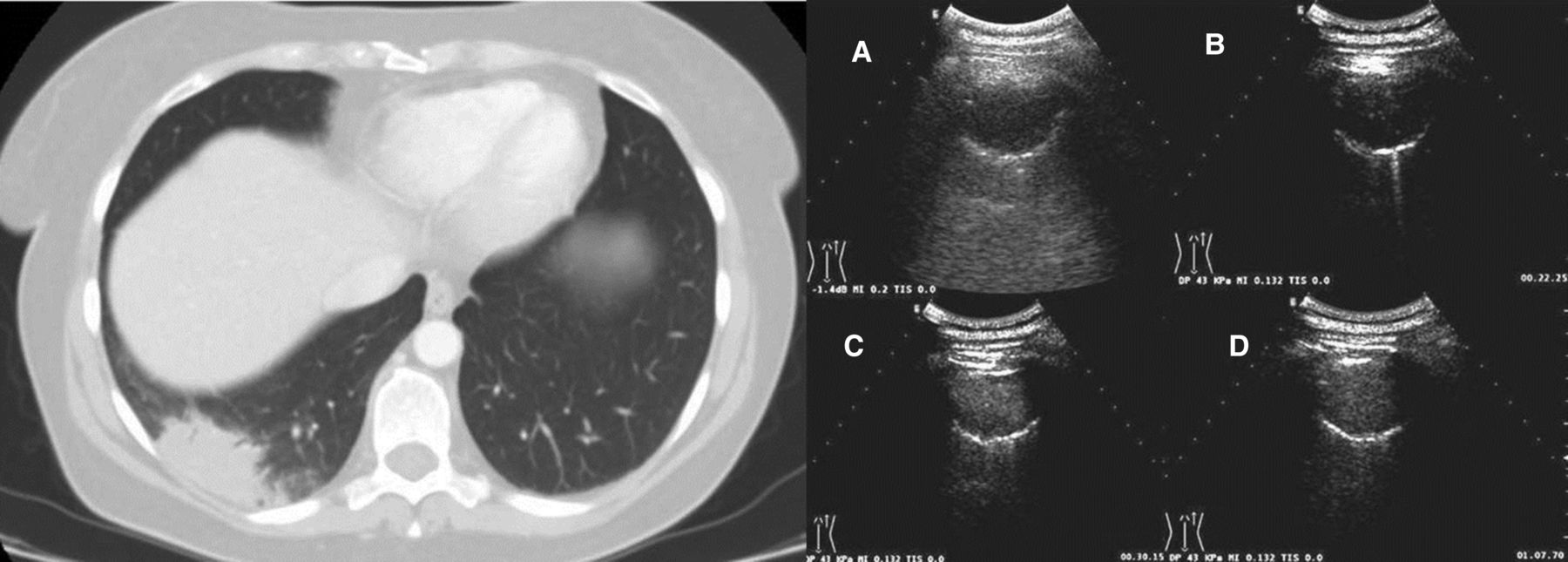
Our results showed that the timing and pattern of CE detected by CEUS of the chest did not significantly distinguish between CAP and LC, therefore CEUS does not discriminate between benign and malignant US-detected lesions. Although our previous work indicated that CEUS may discriminate LC from non-CAP benign lesions, our current findings differ from previous results obtained from smaller samples of patients with lung diseases.3 ,4 In fact, by studying a larger sample of these patients, Görg recognised that the clinical benefit of CEUS is still unclear.7 Moreover, our data do not support previous claims that inflammatory lesions retain contrast for a long time, nor that an early washout could be expected from malignant lesions.7 The reasons for these discrepancies remain hypothetical. Conceivably, the lack of significant differences between CEUS features of CAP and LC could reflect some pathophysiological aspects shared by these conditions. Inflammatory mediators are important components of the tumour microenvironment, stimulate the proliferation and survival of malignant cells, promote angiogenesis, subvert adaptive immune responses and an inflammatory component is invariably present in malignant lesions.8 ,9 This could partly account for the indiscriminate information provided by CEUS in CAP and LC (figure 2). Specific characteristics of Sonovue, whose microbubbles cross the capillary–alveolar barrier10 and are eliminated by expiration, may be confounded by the influence of hydrostatic pressure (ie, patient's position), hypoxic vascular constriction, local circulatory shunt due to comorbidity or atelectasis or many other confounders. We cannot exclude the possibility that the composition of our sample (including a relatively high number of patients with LC compared with CAP, with multiple comorbidities) could also have influenced our results. Indeed, we did not investigate the largest fraction of CAP outpatients, which would possibly form the majority of participants in other series. The strengths of our study include the large number of unselected inpatients studied by a single operator. Our study has some limitations, including generalisability from a single hospital and single operator to other centres, outpatient settings or operators. Although we tried to minimise the latter by estimating interobserver agreement on recorded clips, this does not reflect the routine implementation of CEUS in daily hospital practice, usually performed by several operators. Even considering these limitations, our negative results deserve interest because they hamper overly optimistic beliefs about the performance of CEUS in the discrimination between benign and malignant pulmonary lesions.
{kind=link}
{kind=link}
Left panel: CT imaging of an irregular right-sided area of subpleural consolidation. Right panel: subsequent frames of contrast-enhanced ultrasound (CEUS) showing progression of enhancement followed by vanishing: (A) B-mode ultrasonographic imaging before CEUS; (B) enhancement at 22 s; (C) enhancement at 30 s; (D) late enhancement time at 67 s. Pathological diagnosis: adenocarcinoma.
Footnotes
Contributors MS: designed the study, collected and interpreted data, drafted, revised and approved the manuscript. GR: collected and interpreted data, revised and approved the manuscript. MAG, FT: database setup and revised and approved the manuscript. LMCD: interpreted data and revised and approved the manuscript. VC: analysed data and drafted, revised and approved the manuscript.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ethical approval was obtained from the local ethics committee of Casa Sollievo della Sofferenza San Giovanni Rotondo.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement We accept to share our data for systematic review.