Article Text

Abstract
The British Society of Gastroenterology in collaboration with British Association for the Study of the Liver has prepared this document. The aim of this guideline is to review and summarise the evidence that guides clinical diagnosis and management of ascites in patients with cirrhosis. Substantial advances have been made in this area since the publication of the last guideline in 2007. These guidelines are based on a comprehensive literature search and comprise systematic reviews in the key areas, including the diagnostic tests, diuretic use, therapeutic paracentesis, use of albumin, transjugular intrahepatic portosystemic stent shunt, spontaneous bacterial peritonitis and beta-blockers in patients with ascites. Where recent systematic reviews and meta-analysis are available, these have been updated with additional studies. In addition, the results of prospective and retrospective studies, evidence obtained from expert committee reports and, in some instances, reports from case series have been included. Where possible, judgement has been made on the quality of information used to generate the guidelines and the specific recommendations have been made according to the ‘Grading of Recommendations Assessment, Development and Evaluation (GRADE)’ system. These guidelines are intended to inform practising clinicians, and it is expected that these guidelines will be revised in 3 years’ time.
- ascites
- cirrhosis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Executive summary of recommendations
Diagnostic paracentesis in new- onset ascites
1.1. A diagnostic paracentesis is recommended in all patients with new-onset ascites. (Quality of evidence: moderate; Recommendation: strong)
1.2. The initial ascitic fluid analysis should include total protein concentration and calculation of the serum ascites albumin gradient (SAAG). (Quality of evidence: moderate; Recommendation: strong)
1.3. Ascites fluid analysis for cytology, amylase, brain natriuretic peptide (BNP) and adenosine deaminase should be considered based on pretest probability of specific diagnosis (Quality of evidence: moderate; Recommendation: weak)
Spontaneous bacterial peritonitis
2.1. Diagnostic paracentesis should be carried out without a delay to rule out spontaneous bacterial peritonitis SBP) in all cirrhotic patients with ascites on hospital admission. (Quality of evidence: moderate; Recommendation: strong)
2.2. A diagnostic paracentesis should be performed in patients with GI bleeding, shock, fever or other signs of systemic inflammation, gastrointestinal symptoms, hepatic encephalopathy, and in patients with worsening liver or renal function. (Quality of evidence: moderate; Recommendation: strong)
2.3. Ascitic neutrophil >250/mm3 count remains the gold standard for the diagnosis of SBP and this can be performed either by manual microscopy or using automated counts, based on flow cytometry for counting and differentiating cells. (Quality of evidence: moderate; Recommendation: strong)
2.4. Ascitic fluid culture with bedside inoculation of blood culture bottles should be performed to guide the choice of antibiotic treatment when SBP is suspected. (Quality of evidence: moderate; Recommendation: strong)
2.5. Immediate empirical antibiotic therapy should be determined with due consideration of context of SBP (community acquired or healthcare associated), severity of infection and local bacterial resistance profile. Cefotaxime has been widely studied, but choice of antibiotic should be guided by local resistance patterns and protocol. (Quality of evidence: moderate; Recommendation: strong)
2.6. A second diagnostic paracentesis at 48 hours from the start of treatment to check the efficacy of antibiotic therapy should be considered in those who have apparently inadequate response or where secondary bacterial peritonitis is suspected. (Quality of evidence: low; Recommendation: weak)
2.7. Patients presenting with gastrointestinal bleeding and underlying ascites due to cirrhosis should receive prophylactic antibiotic treatment (cefotaxime has been widely studied but the antibiotic should be chosen based on local data) to prevent the development of SBP. (Quality of evidence: strong; Recommendation: strong)
2.8. Patients who have recovered from an episode of SBP should be considered for treatment with norfloxacin (400 mg once daily), ciprofloxacin (500 mg once daily, orally) or co-trimoxazole (800 mg sulfamethoxazole and 160 mg trimethoprim daily, orally) to prevent further episode of SBP. (Quality of evidence: low; Recommendation: weak)
2.9. Primary prophylaxis should be offered to patients considered at high risk, as defined by an ascitic protein count <1.5 g/dL. However, it is important that the potential risks and benefits and existing uncertainties are communicated to patients. (Quality of evidence: low; Recommendation: weak)
Dietary salt restriction
3.1. Patients with cirrhosis and ascites should have a moderately salt restricted diet with daily salt intake of no more than 5–6.5 g (87–113 mmol sodium). This translates to a no added salt diet with avoidance of precooked meals. (Quality of evidence: moderate; Recommendation: strong)
3.2. Patients with cirrhosis and ascites should receive nutritional counselling on the sodium content in the diet. (Quality of evidence: weak; Recommendation: strong)
Diuretics
4.1. In patients with the first presentation of moderate ascites, spironolactone monotherapy (starting dose 100 mg, increased to 400 mg) is reasonable. In those with recurrent severe ascites, and if faster diuresis is needed (for example, if the patient is hospitalised), combination therapy with spironolactone (starting dose 100 mg, increased to 400 mg) and furosemide (starting dose 40 mg, increased to 160 mg) is recommended. (Quality of evidence: moderate; Recommendation: strong)
4.2. All patients initiating diuretics should be monitored for adverse events. Almost half of those with adverse events require diuretic discontinuation or dose reduction. (Quality of evidence: low; Recommendation: weak)
4.3. Hypovolaemic hyponatraemia during diuretic therapy should be managed by discontinuation of diuretics and expansion of plasma volume with normal saline. (Quality of evidence: low; Recommendation: weak)
4.4. Fluid restriction to 1–1.5 L/day should be reserved for those who are clinically hypervolaemic with severe hyponatraemia (serum sodium <125 mmol/L). (Quality of evidence: low; Recommendation: weak)
4.5. Hypertonic sodium chloride (3%) administration should be reserved for those who are severely symptomatic with acute hyponatraemia. Serum sodium should be slowly corrected. (Quality of evidence: low; Recommendation: weak)
4.6. It may be appropriate to consider use of midodrine in refractory ascites on a case by case basis. (Quality of evidence: low; Recommendation: weak)
Large volume paracentesis (LVP)
5.1. Patients should give informed consent for a therapeutic or diagnostic paracentesis. (Quality of evidence: low; Recommendation: strong)
5.2. Ultrasound guidance should be considered when available during LVP to reduce the risk of adverse events (Quality of evidence: low; Recommendation: weak)
5.3. Routine measurement of the prothrombin time and platelet count before therapeutic or diagnostic paracentesis and infusion of blood products are not recommended. (Quality of evidence: moderate ; Recommendation: strong)
Use of human albumin solution (HAS)
6.1. Albumin (as 20% or 25% solution) should be infused after paracentesis of >5 L is completed at a dose of 8 g albumin/L of ascites removed. (Quality of evidence: high; Recommendation: strong)
6.2. Albumin (as 20% or 25% solution) can be considered after paracentesis of <5 L at a dose of 8 g albumin/L of ascites removed in patients with ACLF or high risk of post-paracentesis acute kidney injury. (Quality of evidence: low; Recommendation: weak)
6.3. In patients with SBP and an increased serum creatinine or a rising serum creatinine, infusion of 1.5 g albumin/kg within 6 hours of diagnosis, followed by 1 g/kg on day 3, is recommended. (Quality of evidence: low; Recommendation: weak)
Transjugular intrahepatic portosystemic shunt (TIPSS)
7.1. TIPSS should be considered in patients with refractory ascites. (Quality of evidence: high; Recommendation: strong)
7.2. Caution is required if considering TIPSS in patients with age >70 years, serum bilirubin >50 µmol/L, platelet count <75×109/L, model for end-stage liver disease (MELD) score ≥18, current hepatic encephalopathy, active infection or hepatorenal syndrome. (Quality of evidence: moderate; Recommendation: strong)
Umbilical hernia
8.1. Suitability and timing of surgical repair of umbilical hernia should be considered in discussion with the patient and multidisciplinary team involving physicians, surgeons and anaesthetists. (Quality of evidence: low; Recommendation: strong)
Hepatic hydrothorax (HH)
9.1. TIPSS should be considered in patients with HH after discussion with the multidisciplinary team. (Quality of evidence: low; Recommendation: strong)
9.2. In patients with HH who are not undergoing a TIPSS and/or a liver transplant evaluation, alternative palliative interventions should be considered. (Quality of evidence: low; Recommendation: strong)
Non-selective beta-blockers (NSBB) and ascites
10.1. Refractory ascites should not be viewed as a contraindication to NSBB. (Quality of evidence: moderate; Recommendation: strong)
10.2. Patients with refractory ascites who are taking NSBB should be monitored closely, and dose reduction or discontinuation may be appropriate in those who develop hypotension or acute/progressive renal dysfunction. (Quality of evidence: moderate; Recommendation: strong)
Automated low-flow ascites pump
11.1. An automated low-flow ascites pump should be considered only in special circumstances with robust arrangements of clinical governance, audit or research. (Quality of evidence: low; Recommendation: weak)
Palliative care
12.1. Patients with refractory ascites who are not undergoing evaluation for liver transplant should be offered a palliative care referral. Besides repeated LVP, alternative palliative interventions for refractory ascites should also be considered. (Quality of evidence: weak; Recommendation: strong)
Research recommendations
13.1. Randomised controlled trials (RCT) with large sample size should evaluate the role of antibiotics in the secondary prophylaxis for SBP in ascites secondary to cirrhosis.
13.2. Large RCTs should assess the role of midodrine in the management of ascites.
13.3. Cost-effectiveness of long-term administration of albumin to patients with decompensated cirrhosis and ascites should be evaluated.
13.4. Role of nutritional interventions in the management of ascites should be evaluated.
13.5. Large RCT of long-term carvedilol versus no carvedilol in patients with refractory ascites without large oesophageal varices should be carried out.
13.6. Role of TIPSS in the management of hepatic hydrothorax should be compared with other therapeutic interventions.
13.7. The cost-effectiveness and the effect of automated low-flow ascites pumps on the quality of life of patients with refractory ascites should be evaluated.
13.8. Effectiveness and safety of long-term abdominal drains should be assessed in RCTs for the palliative care of patients with cirrhosis and refractory ascites.
Patient summary
These guidelines have been produced on behalf of the British Society of Gastroenterology (BSG) in collaboration with the British Association for the Study of the Liver (BASL). These guidelines are aimed at healthcare professionals who look after patients with cirrhosis and ascites.
Ascites is the build-up of fluid in the belly (abdomen). This occurs when the liver gets irreversibly scarred, a condition known as cirrhosis. Ascites is the most common complication of cirrhosis.
All patients with a new onset of ascites should have the fluid tested. This involves inserting a small needle into the abdomen and removing about two tablespoons of ascitic fluid. The fluid is then analysed for protein and white cell count. Protein count can help differentiate whether the cause of ascites is cirrhosis or whether the ascites is due to other causes like heart disease or cancer. The white cell count indicates whether there is an infection in the ascitic fluid. If infection is present, this is treated with a short course of antibiotics. Infection of ascites should be ruled out at every hospital admission as it carries a high risk of death and should therefore be diagnosed and treated promptly. After this initial treatment, patients are given long-term antibiotics to prevent repeat infections.
No salt should be added at the table to food. The total amount of salt in food per day should not be more than the equivalent of one teaspoon. Patients should read labels on prepared foods to confirm their daily salt intake is within the limit of 5 g of salt. The initial treatment for patients with ascites involves taking medication, commonly known as 'water tablets' (diuretics). These drugs are begun at a small dose, which is gradually increased until the ascites is treated. Diuretics can have side effects such dehydration, confusion, abnormal levels of sodium and potassium and kidney damage. Therefore patients should be monitored while taking these tablets.
As the liver disease progresses the ascites may no longer respond to medication. This is known as untreatable or refractory ascites. This requires the patient to come into hospital every few weeks to have a temporary drain inserted into the abdomen and the ascitic fluid drained. If more than 5 L of fluid is removed, patients are also given a protein solution into the vein to prevent dehydration.
In patients with untreatable ascites, alternatives to repeated hospital drainage include placing a small tube (stent) in the liver. This specialised procedure is known as a transjugular intrahepatic portosystemic shunt (TIPSS). The TIPSS procedure is effective in reducing the need for repeated fluid drainage. Because of potential side effects, patients should be selected carefully for this procedure. This is particularly true for patients with more advanced liver disease, where the insertion of a TIPSS can potentially be harmful.
The only curative option for untreatable ascites is liver transplantation. If the patient is not suitable for liver transplantation, medical care then focuses on controlling the ascites symptoms. This is known as palliative care. The most common palliative treatment for untreatable ascites is repeated hospital drainage. Alternative treatments for untreatable ascites, such as long-term abdominal drains, need further research.
Introduction
Contemporary data from an NHS hospital serving a population of 700 000, found 164 adults with a new diagnosis of ascites over a period of 5 years. Of these, 55% had cirrhosis (alcohol-related liver disease 58, non-alcoholic fatty liver disease 21, chronic viral hepatitis 4, autoimmune liver diseases 3 and cryptogenic cirrhosis 4), 29% had malignancies (gynaecological 12, gastrointestinal 25 and others 11), 6% cardiac failure (CF), 3% end-stage renal disease (ESRD) and 7% other aetiologies.
Development of ascites is an important milestone in the natural history of cirrhosis. About 20% of patients with cirrhosis have ascites at their first presentation, and 20% of those presenting with ascites die in the first year of the diagnosis.1 The aim of this guideline is to review and summarise the evidence that guides clinical diagnosis and management of ascites in patients with cirrhosis.
Pathogenesis
A detailed description of the pathogenesis of ascites formation is beyond the scope of this article, but two key factors involved in the pathogenesis of ascites formation are portal hypertension and retention of sodium and water. This is summarised in figure 1.

The pathogenesis of ascites in cirrhosis.
An elevated sinusoidal pressure is essential for the development of ascites, as fluid accumulation does not develop at portal pressure gradient below 8 mm Hg, and rising corrected sinusoidal pressure correlates with decreased 24-hour urinary excretion of sodium.2 3 Architectural changes associated with advanced fibrosis are clearly the primary mechanism underlying increased intrahepatic resistance to the portal flow in cirrhosis. In addition, phenotypic changes in hepatic stellate cells and liver sinusoidal endothelial cells contribute to the pathophysiology. Activated stellate cells become contractile, and their recruitment around newly formed sinusoidal vessels increases the vascular resistance. Reduction in the production/bioavailability of nitric oxide (NO) in the cirrhotic liver adds further to the rise in vascular tone. Overall, vasoconstriction has been estimated to account for about 25% of the increased resistance within the liver.4
Increased portal pressure is sensed by intestinal microvasculature that generates angiogenic factors such as vascular endothelial growth factor,5 and these stimulate the development of portosystemic collaterals through the opening of pre-existing vessels or new vessel formation. When the portal pressure rises further, induction of endothelial nitric oxide synthase and over production of NO leads to splanchnic arterial vasodilatation. This, in turn, increases portal blood flow, thus exacerbating portal hypertension. Portosystemic collaterals also permit vasodilators such as NO, prostacyclin and endocannabinoids6 to enter the systemic circulation leading to a state of ‘effective hypovolaemia’.7 This activates sympathetic nervous system stimulating reabsorption of sodium in proximal, distal tubules, loop of Henle and collecting duct as well as the renin–angiotensin–aldosterone system, leading to sodium absorption from distal tubule and collecting duct.8 Renal sodium retention and eventual free water clearance due to non-osmotic release of arginine–vasopressin and its action on V2 receptor in the collecting duct underlie the fluid retention associated with oedema and ascites in cirrhosis.8
More recently, it has been hypothesised that bacterial translocation associated with portal hypertension in cirrhosis and related pathogen-associated, molecular pattern activated innate immune responses lead to systemic inflammation.9 This is associated with vasodilatation as well as release of proinflammatory cytokines, reactive oxygen and nitrogen species, contributing to organ dysfunction.
Definitions
The terms used in this article have been defined by the International Ascites Club10
Uncomplicated ascites
Ascites that is not infected and which is not associated with the development of the hepatorenal syndrome (HRS). Ascites can be graded as mild when ascites is detectable only by ultrasound examination, moderate when it causes moderate symmetrical distension of the abdomen and large when it causes marked abdominal distension.
Refractory ascites
Ascites that cannot be mobilised or the early recurrence of which (ie, after therapeutic paracentesis) cannot be satisfactorily prevented by medical treatment. This includes two different subgroups.
Diuretic-resistant ascites
Ascites that is refractory to dietary sodium restriction and intensive diuretic treatment.
Diuretic-intractable ascites
Ascites that is refractory to treatment owing to the development of diuretic-induced complications that preclude the use of an effective diuretic dosage.
Evaluation of patients with ascites
Clinical evaluation should include history of exposure to risk factors for cirrhosis and physical examination to look for evidence to support chronic liver disease or an alternative diagnosis. Shifting dullness is detectable when about one and a half litres of free fluid accumulate in the abdomen; the physical sign has 83% sensitivity and 56% specificity in detecting ascites.11 12 However, in the presence of obesity or smaller amount of fluid, imaging such as ultrasound or CT is necessary to confirm the presence of ascites.
Diagnostic paracentesis in new-onset ascites
Aspiration of ascitic fluid and its laboratory analysis is an essential step in the management of patients with newly diagnosed ascites. In cirrhosis, hepatic sinusoids are less permeable owing to fibrous tissue deposition, resulting in ascites with low protein content. It is important to estimate total protein level in ascites fluid; a concentration below 1.5 g/dL (or 15 g/L) is a risk factor for the development of spontaneous bacterial peritonitis. In addition, serum ascites albumin gradient (SAAG) should be estimated routinely. A cut-off point of 1.1 g/dL (or 11 g/L) differentiates between causes of ascites with high sensitivity,13–18 although alternative causes should be considered based on the clinical scenario (table 1).
Grouping of aetiology of ascites based on serum albumin ascites gradient (SAAG)
Hepatic sinusoids are normally permeable in heart failure, which allows for leakage of protein-rich lymph into the abdominal cavity and therefore, total protein concentration in ascitic fluid is high (>2.5 g/dL) in combination with a high SAAG. In such a situation, measurement of brain natriuretic peptide (BNP) in the serum±ascites is useful. Total protein concentrations >2.5 g/dL within the ascites and serum BNP >364 ng/L are suggestive of underlying or additional cardiac disease, whereas serum protein values <182 ng/L rule out cardiac disease.19
In low SAAG states, clinical context and imaging should guide the investigational approach. The yield for positive cytology in the context of malignancy is variable, ranging from 0% to 96.7%, in part determined by the site of the tumour.20 21 Combining cytology with tumour markers in the ascitic fluid may increase the positive predictive value (PPV), specifically the use of carcinoembryonic antigen (CEA), epithelial cell adhesion molecule (EpCAM), CA 15-3 and CA 19-9.20 However, CA 125 in the serum or ascites has no role as a discriminator and will commonly be elevated by the presence of ascites from any cause.22
Where peritoneal TB is considered plausible, ascites can be sent for acid-fast bacilli smear and culture, although culture positivity occurs in <50% and smear-positive ascites is rare.23 Adenosine deaminase is more useful to distinguish between peritoneal TB and carcinomatosis, with an area under the receiver operating characteristic curve of 0.98; adenosine deaminase levels of <40 IU/mL are used to exclude TB.24 25
Pancreatic ascites is a rare complication of pancreatitis, although more common when a pseudocyst is present. In pancreatic ascites, the amylase level in the ascitic fluid is typically >1000 IU/L or greater than six times the serum amylase, with mean values exceeding 4000 IU/L in a recent cohort of 80 patients.26 Raised polymorphonuclear leucocytes (PMN) count may also be found in pancreatic ascites.27
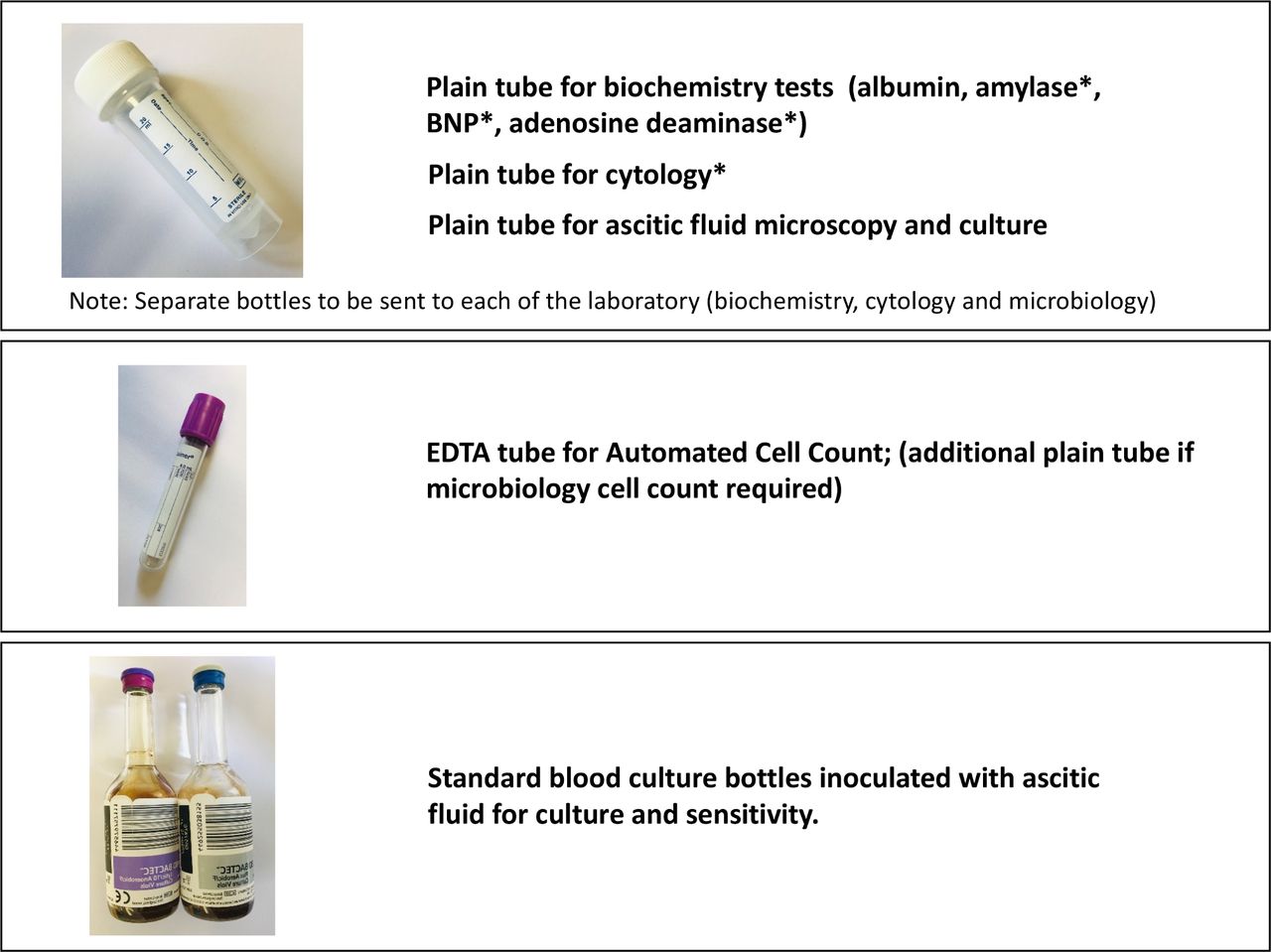
The ascitic fluid samples required from the diagnostic paracentesis is summarised in figure 2.
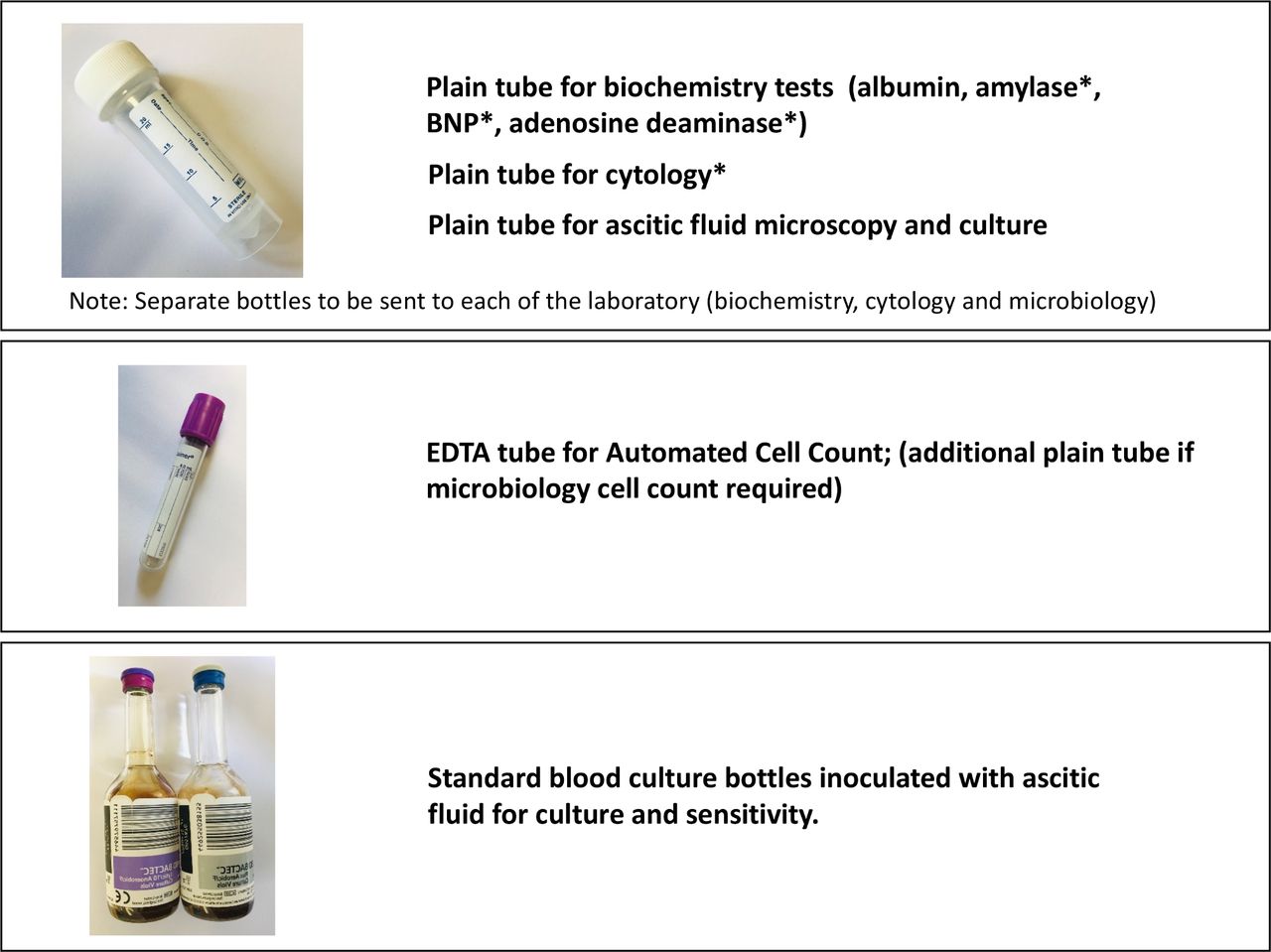
The ascitic fluid samples required from diagnostic paracentesis. *These investigations should be considered based on pretest probability of specific diagnosis. BNP, brain natriuretic peptide.
Recommendations
A diagnostic paracentesis is recommended in all patients with new-onset ascites. (Quality of evidence: moderate; Recommendation: strong)
The initial ascitic fluid analysis should include total protein concentration and calculation of SAAG. (Quality of evidence: moderate; Recommendation: strong)
Ascites fluid analysis for cytology, amylase, BNP and adenosine deaminase should be considered based on pretest probability of specific diagnosis (Quality of evidence: moderate; Recommendation: weak)
Spontaneous bacterial peritonitis (SBP)
Spontaneous bacterial peritonitis is the development of bacterial infection of ascites in the absence of any intra-abdominal surgically treatable source of infection. The prevalence of SBP in outpatients is 1.5–3.5% and approximately 10% in hospitalised patients.28 A recent European study detected a prevalence of 11.3% among inpatients.29 When first described, mortality associated with SBP exceeded 90%, but, in-hospital mortality has been reduced to approximately 20% with early diagnosis and prompt treatment.30 In an observational study, each hour of delay in diagnostic paracentesis after admission was associated with a 3.3% increase of in-hospital mortality after adjusting for model for end-stage liver disease (MELD) score.31 Long-term survival remains poor; 1-year survival after hospitalisation with SBP in a UK study was found to be 34%.32 Patients recovering from an episode of SBP should always be considered as potential candidates for liver transplantation if they have not already been assessed.
Diagnosis of SBP
The diagnosis of SBP is confirmed when ascitic neutrophil count is >250 cells/mm3 in the absence of an intra-abdominal and surgically treatable source of sepsis. A cut-off point of 250 neutrophils/mm3 has the greatest sensitivity, although a cut-off point of 500 neutrophils/mm3 has greater specificity.33 A meta-analysis of primary data from 14 prospective trials has defined the positive and negative likelihood ratios of SBP at different thresholds for total white cell count (WCC) and PMN in ascitic fluid. WCC >1000 cells/µL or PMN ≥500 cells/µL are most accurate and yield positive likelihood ratios of 9.1 (95% CI 5.5 to 15.1) and 10.6 (95% CI 6.1 to 18.3), respectively. Likelihood ratios for WCC >500 cells/µL (5.9; 95% CI 2.3 to 15.5) and PMN >250 cells/µL (6.4; 95% CI 4.6 to 8.8) support routine clinical practice of using lower thresholds, where the greater risk lies with underdiagnosing SBP.18
Historically, ascitic neutrophil counts have been performed by manual microscopy, but, this is time and cost intensive. Automated counts, based on flow cytometry for counting and differentiating cells, are now used in most centres. This technique has been shown to have sensitivity and specificity close to 100%,34 35 allowing a tube containing ethylenediamine tetra-acetate (EDTA; as used for plasma full blood count) to be inoculated with ascitic fluid and processed on a standard blood count analyser. Reagent strips have insufficient sensitivity for reliable use in this context36 and hence cannot be recommended to replace cell count to diagnose SBP.
Ascitic fluid culture
Ascites culture is essential to help guide antibiotic therapy. Patients with ‘culture-negative neutrocytic ascites’ (PMN count >250 cells/mm3) have a similar presentation to those with culture-positive SBP. As both groups of patients have significant morbidity and mortality,37 38 they should be treated in a similar manner. Some patients have ‘bacterascites’ in which cultures are positive, but, ascitic neutrophil count is <250 cells/mm3. In some patients, bacterascites represents a transient and spontaneously reversible colonisation of ascites, in others, particularly those who are symptomatic, it may represent the first step in the development of SBP.33 Discussion with microbiologists about the organism cultured can help differentiate the above two scenarios, and when a positive culture is obtained a repeat tap should be sent to guide management.
Although the identification of pathogen(s) is essential for the management of infectious diseases, ascites fluid cultures often fail to provide positive results, even when using ascites samples from patients who develop clinical manifestations of SBP. Bacterial DNA detection and sequencing have been applied to the diagnosis of several infectious diseases, and molecular techniques can detect small amounts of bacterial DNA within a few hours. These promising techniques have yet to be introduced into routine clinical practice.39
Fungal peritonitis is a rare, less studied complication and observational data suggest a worse prognosis.40 In a large multicentre study of 2743 cirrhotic inpatients, of whom 1052 had infections, 12.7% of infected patients had evidence of fungal infections with a case fatality of 30%. The majority of these were urinary, but the highest mortality was seen with fungaemia and peritonitis (case fatality >50%).41
Secondary bacterial peritonitis
A small proportion of patients with cirrhosis may develop peritonitis secondary to perforation or inflammation of an intra-abdominal organ, known as secondary bacterial peritonitis. In a small retrospective analysis, secondary peritonitis represented 4.5% of all peritonitis in cirrhotic patients.42 This should be suspected in those who have localised abdominal symptoms or signs, very high ascitic neutrophil count, the presence of multiple organisms on ascitic culture or in those with inadequate response to treatment.42 Cross-sectional imaging, such as CT, should be performed with early consideration of surgery in this scenario.
Antibiotic therapy
The most common organisms isolated in patients with SBP include Escherichia coli, Gram-positive cocci (mainly streptococcus species) and enterococci. Empirical antibiotic therapy must be initiated immediately after the diagnosis of SBP.33 In the 1990s, cefotaxime, a third-generation cephalosporin, was extensively investigated in patients with SBP because it was found to cover 95% of organisms and high ascitic fluid concentrations could be achieved.43 44 The take home message from these studies is that matching an effective antibiotic to the cultured organism is key to successful treatment, rather than any apparent superiority of one drug over another. Since these studies, the landscape of bacterial resistance has significantly changed with an increase in antimicrobial resistant organisms,45 and therefore recommending a specific single empirical antibiotic is challenging. Thus, it is crucial to separate community-acquired SBP from healthcare-associated SBP (nosocomial – defined as infection >48 hours after hospital admission)46 and to consider both the severity of infection and the local resistance profile in order to decide the empirical antibiotic treatment of SBP.47 Over recent years there has been a significant increase in the number of infections caused by multidrug-resistant organisms,29 48 defined by an acquired non-susceptibility to at least one agent in three or more antimicrobial categories.49 It is also important to highlight the shift to extensively drug resistant bacteria, defined by non-susceptibility to at least one agent in all but two or fewer antimicrobial categories, or to pan-drug resistance bacteria, defined by non-susceptibility to all agents in all antimicrobial categories.49
A second diagnostic tap should be considered at 48 hours from starting treatment, to check the efficacy of antibiotic therapy in patients who have an apparently inadequate response. If ascitic fluid neutrophil count fails to decrease to less than 25% of the pretreatment value, this should raise suspicion of antibiotic resistance or the presence of ‘secondary peritonitis’.33 50 Specialist microbiology links should be developed within each trust to help guide local policy and patient management and, in addition, de-escalation of anti-microbial agents according to susceptibility of positive cultures is recommended.
The evidence for the use of human albumin solution and recommendations for its use in SBP are discussed in a separate section below.
Prophylactic therapy for SBP
Three groups at high risk of developing SBP have been identified: (i) patients with acute gastrointestinal (GI) haemorrhage; (ii) patients with a low ascitic protein concentration and no prior history of SBP (primary prophylaxis) and (iii) patients with a previous episode of SBP (secondary prophylaxis).51 Although antibiotic prophylaxis to prevent further infection in patients presenting to hospital with upper GI bleeding is established in clinical practice,52–54 there remains uncertainty over prophylaxis in other circumstances. Additional studies related to this area after the Cochrane review53 are summarised in online supplemental table 1.
Supplemental material
Primary prophylaxis
Primary prophylaxis is a controversial area and broad recommendations are not straightforward. In 2016 the National Institute for Health and Care Excellence (NICE) recommended offering prophylactic oral ciprofloxacin or norfloxacin for people with cirrhosis and ascites and no history of SBP with an ascitic protein of ≤15 g/L (1.5 g/dL), until the ascites has resolved.55 Six studies were included in their analyses.56–61 The European Association for the Study of Liver (EASL) recommend primary prophylaxis with norfloxacin (400 mg/day) in patients with Child-Pugh score ≥9 and serum bilirubin ≥3 mg/dL, with either impaired renal function or hyponatraemia and ascitic fluid protein lower than 15 g/L.47 The American Association for the Study of Liver Diseases (AASLD) also suggest that antibiotics for primary prophylaxis of SBP should be considered for people at high risk of developing this complication, which was defined as an ascitic fluid protein <1.5 g/dL together with impaired renal function or liver failure.62
In contrast, in a large placebo-controlled randomised clinical trial, the NORFLOCIR trial, norfloxacin did not reduce 6-month mortality in patients with advanced cirrhosis, with >95% of patients included having no history of prior SBP.63 In post-hoc analyses, norfloxacin, appeared to increase survival of patients with low ascites fluid protein concentrations. However, other data have failed to replicate an association of incidence of SBP in patients with pre-existing low total ascitic fluid protein concentration in three large cohorts of hospitalised patients with cirrhosis and ascites.64 65 Furthermore, there are concerns about the potential consequences of long-term oral antibiotic therapy, including resistance, increased risk of Clostridium difficile associated diarrhoea, adverse reactions and drug interactions. In 2019 the Medicines and Healthcare products Regulatory Agency (MHRA) issued updated guidance on new restrictions and precautions for use of fluoroquinolone antibiotics following a detailed EU review of very rare reports of disabling and potentially longlasting or irreversible side effects affecting the musculoskeletal and nervous systems. Although SBP prophylaxis was not specifically considered, renal impairment is considered to increase this risk, and therefore healthcare professionals and patients should be vigilant during treatment with fluoroquinolone antibiotics and discontinue treatment at the first sign of tendon pain or inflammation. Finally, norfloxacin is not widely available in the UK.
In view of the uncertainties outlined above, we advocate primary prophylaxis is offered to patients considered at high risk, as defined by an ascitic protein count <1.5 g/dL. However, it is important that the potential risks and benefits and existing uncertainties are communicated to patients.
It is expected that a large ongoing multicentre UK trial (European Union Drug Regulating Authorities Clinical Trials Database Registration Number: 2019-000581-38) to investigate the efficacy of long-term co-trimoxazole compared with placebo as primary prevention for SBP may deal with these uncertainties.
Secondary prophylaxis
In patients who survive an episode of SBP, the cumulative recurrence rate at 1 year is approximately 70%.33 Probability of survival at 1 year after an episode of SBP is 30–50% and falls to 25–30% at 2 years.66 67 There is only one randomised, double-blind, placebo-controlled trial of norfloxacin (400 mg/day) in patients who had a previous episode of SBP68; treatment reduced the probability of recurrence of SBP from 68% to 20%. A recent systematic review with meta-analysis concluded that rifaximin may be effective for both primary and secondary SBP prophylaxis compared with systemically absorbed antibiotics and compared with no intervention.69 However, additional prospective studies are required before a change in clinical practice can be recommended. It has been suggested that proton pump inhibitor use may increase the risk for the development of SBP and indications for long-term use should be carefully assessed.70 71
We therefore recommend norfloxacin 400 mg once a day as secondary prophylaxis, although in view of limited availability in the UK, many centres use once daily ciprofloxacin 500 mg once a day as an alternative.
Recommendations
Diagnostic paracentesis should be carried out without a delay to rule out SBP in all cirrhotic patients with ascites on hospital admission. (Quality of evidence: moderate; Recommendation: strong)
A diagnostic paracentesis should be performed in patients with GI bleeding, shock, fever or other signs of systemic inflammation, gastrointestinal symptoms, hepatic encephalopathy, and in patients with worsening liver or renal function. (Quality of evidence: moderate; Recommendation: strong)
Ascitic neutrophil >250/mm3 count remains the gold standard for the diagnosis of SBP and this can be performed either by manual microscopy or using automated counts, based on flow cytometry for counting and differentiating cells. (Quality of evidence: moderate; Recommendation: strong)
Ascitic fluid culture with bedside inoculation of blood culture bottles should be performed to guide the choice of antibiotic treatment when SBP is suspected. (Quality of evidence: moderate, Recommendation: strong)
Immediate empirical antibiotic therapy should be determined with due consideration of context of SBP (community acquired or healthcare associated), severity of infection and local bacterial resistance profile. Cefotaxime has been widely studied, but choice of antibiotic should be guided by local resistance patterns and protocol. (Quality of evidence: moderate; Recommendation: strong)
A second diagnostic paracentesis at 48 hours from the start of treatment to check the efficacy of antibiotic therapy should be considered in those who have apparently inadequate response or where secondary bacterial peritonitis is suspected. (Quality of evidence: low; Recommendation: weak)
Patients presenting with gastrointestinal bleeding and underlying ascites due to cirrhosis should receive prophylactic antibiotic treatment (cefotaxime has been widely studied but the antibiotic should be chosen based on local data) to prevent the development of SBP. (Quality of evidence: strong, Recommendation: strong)
Patients who have recovered from an episode of SBP should be considered for treatment with norfloxacin (400 mg once daily), ciprofloxacin (500 mg once daily, orally) or co-trimoxazole (800 mg sulfamethoxazole and 160 mg trimethoprim daily, orally) to prevent further episode of SBP. (Quality of evidence: low; Recommendation: weak)
Primary prophylaxis should be offered to patients considered at high risk, as defined by an ascitic protein count <1.5 g/dL. However, it is important that the potential risks and benefits and existing uncertainties are communicated to patients. (Quality of evidence: low; Recommendation: weak)
Dietary salt restriction
There is little evidence to support salt restriction in patients with cirrhosis in absence of ascites. In patients with cirrhosis and ascites, seven RCTs and one cross-sectional survey have examined the role of salt restriction (online supplemental table 2).72–79 One of the studies has only been published as an abstract.76 Four of the earlier RCTs72–75 found no difference in ascites control in those with and without salt restriction. Two recent RCTs found that a salt unrestricted diet (5–6.5 g/day) in contrast to a salt restricted diet (<5 g/day), resulted in ascites disappearance in a larger proportion (45% vs 16%) over a shorter time period and also significantly reduced the need for large volume paracentesis (LVP).77 78 Additionally, five of the eight above-mentioned studies reported significant adverse events with salt restriction, including hyponatraemia,72 77 reduced caloric intake,76 77 79 higher risk of renal impairment (0% vs 14%),77 hepatic encephalopathy (HE), hepatorenal syndrome (HRS), SBP78 and mortality.77 78 In a study by Sorrentino et al,78 1-year mortality was 45–60% (salt unrestricted diet) versus 82.5% (salt restricted diet).
Thus salt restricted diets (<5 g m of salt, <85 mmol sodium/day) in patients with cirrhosis and ascites do not improve ascites control and, on the contrary, can result in complications. Additionally, such diets are difficult to comply with, especially since the average European ingests about 10 g of salt/day.80–82 A cross-sectional survey79 indicated that only about a third of cirrhotic patients were compliant with salt restriction, with an additional 45% incorrectly stating that they were. Based on these data, patients with cirrhosis and ascites should have a moderately salt restricted diet, with daily salt intake of no more than 5–6.5 g (87 mmol–113 mmol sodium). This translates to a no added salt diet with avoidance of precooked meals. An ongoing systematic review is assessing the role of salt restriction in patients with ascites due to cirrhosis.83
Recommendations
Patients with cirrhosis and ascites should have a moderately salt restricted diet with daily salt intake of no more than 5–6.5 g (87 mmol–113 mmol sodium). This translates to a no added salt diet with avoidance of precooked meals. (Quality of evidence: moderate; Recommendation: strong)
Patients with cirrhosis and ascites should receive nutritional counselling on the sodium content in the diet. (Quality of evidence: weak; Recommendation: strong)
Diuretics
Diuretics remain the main stay in management of ascites, though do not modify its natural history, providing only symptomatic benefit.47 Secondary aldosteronism plays a major role in renal sodium retention in patients with cirrhosis.84 Spironolactone is a specific pharmacological aldosterone antagonist, acting primarily through competitive binding of receptors at the aldosterone-dependent sodium–potassium exchange site in the distal convoluted renal tubule.85 Its hydrophilic derivative is potassium canrenoate. They are usually the first-line diuretics used,84 85 either alone or in combination with a loop diuretic such as furosemide (causing sodium to flood more distal nephron sites).86 Spironolactone appears to be more effective (response rate of 95%) than furosemide (response rate of 52%) in non-azotemic patients with cirrhosis and ascites.87 88 Spironolactone has a long elimination half-life, allowing once a day dosing89–91; dose changes should occur no more frequently than every 3–4 days.86
In those who are intolerant to spironolactone an alternative diuretic is amiloride (acts in the collecting duct). However it is not as effective, an earlier RCT showing response rates of 35% vs 70% in those receiving amiloride versus potassium canrenoate, respectively.92 Other diuretics which have been used in patients with cirrhosis and ascites include bumetanide93 and torasemide.94 95
Sequential versus combined therapy
Three RCTs assessing the role of sequential therapy (spironolactone followed by furosemide) or combination therapy (spironolactone plus furosemide) have given conflicting results (online supplemental table 3). In the first study,88 onset of diuresis was faster in the combination group than in the sequential group. The second RCT mostly included those with first presentation of ascites and found no difference in sequential versus combined therapy for the rapidity of ascites mobilisation and incidence of complications. However, a need for dose reductions was significantly higher in the combination group (68% vs 34%).96 The third RCT included almost two-thirds of patients with prior ascites.97 It reported shorter mean time for ascites resolution, lower risk of adverse events (especially hyperkalaemia), lower treatment failures (24% vs 44%), with ascites resolving in a higher percentage without need for diuretic dose change (76% vs 56%) in the combination versus sequential group, respectively.97
These conflicting results are explained by the heterogeneous patient population as studies by Angeli et al 97 and Fogel et al 88 included those with more advanced disease, explaining the lower response to spironolactone monotherapy. Others have also reported the likelihood of response to spironolactone monotherapy (vs no response) if a first occurrence (56% vs 37%) rather than recurrent (44% vs 63%) or large ascites (16% vs 58%).98 Since in non-azotemic cirrhotic patients with ascites, the distal tubule reabsorbs almost all the sodium delivered, it is unsurprising that the administration of spironolactone alone results in a good natriuretic response in most.96 99 Another advantage of spironolactone monotherapy is its modest diuretic effect,86 as patients with cirrhosis are sensitive to compromises in their intravascular volume.91
Therefore, in patients with first presentation of moderate ascites, starting treatment with spironolactone monotherapy (starting dose 100 mg, increased to 400 mg) is reasonable. In those with persistent or severe ascites, and if faster diuresis is needed (for example, if hospitalised), it may be prudent to use combination therapy with spironolactone and furosemide (starting dose 40 mg, increased to 160 mg). Although maximal daily recommended doses of spironolactone and furosemide are 400 mg and 160 mg respectively,92 97 98 100 these are rarely achieved.88 96 In the largest study until now, which recruited about 2000 patients with ascites, at the time of discharge, mean diuretic units (one unit being 40 mg furosemide and 100 mg spironolactone) varied from 2.5+0.2 to 2.7+0.3.101
Based on evidence from an earlier RCT, it is recommended that diuretic-induced weight loss should not exceed 0.5 kg/day in patients without peripheral oedema, and 1 kg in the presence of peripheral oedema.47 100 Figure 3 summarises the stepped-up98 approach to diuretic treatment.

Approach to the use of diuretics in the management of ascites in patients with cirrhosis.
Adverse reactions to diuretics
All patients initiating diuretics should be monitored for adverse events, the prevalence of which ranges from 19%96 to 33%.88 97 Almost half with adverse events require diuretic discontinuation or dose reduction.88 In hospitalised patients treated with diuretics, hepatic encephalopathy is seen in up to 25%102 and renal impairment in 14–20%,97 102 especially in the absence of peripheral oedema.100 Renal impairment is usually of moderate severity and is reversible on discontinuing diuretics.10 Hyponatraemia occurs in 8–30% and is related to impaired ability of the kidneys to excrete free water.10 97 Hypokalaemia is also a frequent side effect of loop diuretics.10 Similarly hyperkalaemia can occur in up to 11%.97
Gynaecomastia is commonly seen with spironolactone, especially with higher doses.86 It occurs less frequently with potassium canrenoate (53% vs 100%).103 Eplerenone can also relieve the gynaecomastia.104 105
A causal relation is found between cirrhosis and muscle cramps, especially in advanced cirrhosis, with prevalence varying between 26% and 72%,.106–108 The cirrhosis-induced arterial underfilling probably plays a role in the pathogenesis of cramps.107 Diuretics accentuate this reduction in effective plasma volume, thereby increasing the prevalence of cramps.107 An earlier systematic review (including only three RCTs) assessed various interventions for muscle cramps, including zinc, 1-α-hydroxyvitamin D, vitamin E, branched chain amino acids, taurine, intravenous albumin and quinidine. Improvements occurred with most interventions with the exception of vitamin E.109 Recent RCTs have reported beneficial effects with methocarbamol,110 taurine111 and baclofen.112
Monitoring of diuretics
The aim of diuretic therapy is to ensure that urinary sodium excretion exceeds 78 mmol/day (88 mmol intake per day – 10 mmol non-urinary excretion per day).62 113 A random spot urine sodium:potassium ratio between 1.8 and 2.5 has a sensitivity of 87.5%, specificity of 56–87.5% and accuracy of 70–85% in predicting a 24-hour urinary sodium excretion of 78 mmol/day.114 115
Hyponatraemia
Recent guidelines define hyponatraemia as a serum sodium <135 mmol/L, with 130–135 mmol/L, 125–129 mmol/L and <125 mmol/L, constituting mild, moderate and severe hyponatraemia, respectively.47 116 A prospective population survey among patients with cirrhosis found serum sodium <130 mmol/L in 21.6%.117 Hyponatraemia has been associated with higher prevalence of refractory ascites, hepatic encephalopathy, SBP, HRS and mortality.117–119 Acknowledging this, the Model for End Stage Liver Disease (MELD) score now incorporates serum sodium (MELD-Na).120 Those with cirrhosis and chronic hyponatraemia are often asymptomatic and seldom need treatment.62
Both hypovolaemic and hypervolaemic hyponatraemia is observed in cirrhosis.47 Hypovolaemic hyponatraemia results from overzealous diuretic therapy, being characterised by a prolonged negative sodium balance with marked loss of extracellular fluid. Its management requires expansion of plasma volume with normal saline and cessation of diuretics.47 Most hepatologists would discontinue diuretics if serum sodium is <125 mmol/L.
A number of studies (which include four RCTs and a retrospective cohort study) have assessed role of intravenous (IV) human albumin solution (HAS) in patients with hyponatraemia (online supplemental table 4).121–126 These studies did not strictly stratify patients as having hypovolaemic hyponatraemia and mostly included those with Child C cirrhosis and refractory ascites undergoing LVP. There were differences in baseline serum sodium levels, use of diuretics, and degree of salt and fluid restriction. Therefore not unsurprisingly results have been conflicting. An earlier meta-analysis that included three of the above RCTs123–125 reported that use of IV HAS versus no IV HAS reduced occurrence of hyponatraemia (3.9% vs 16.5%) but did not affect mortality.127 A later meta-analysis (IV HAS vs no IV HAS) which included only two RCTs123 124 found no beneficial effects on hyponatraemia or mortality.128 In the retrospective cohort study among hospitalised patients with hyponatraemia (only 42% requiring inpatient LVP), those receiving IV HAS were more likely to have resolution of hyponatraemia than those who did not (85.41% vs 44.78%).126 Hyponatraemia resolution was an independent predictor of 30-day survival, even after adjustment for admission sodium and glomerular filtration rate. At present, however, there is insufficient evidence to routinely recommend IV HAS outside of a LVP setting in patients with cirrhosis and ascites and hypovolaemic hyponatraemia.
Hypervolaemic hyponatraemia is more common in cirrhosis, occurring owing to non-osmotic hypersecretion of vasopressin and enhanced proximal nephron sodium reabsorption with impaired free water clearance, both being caused by effective hypovolaemia.47 129 Impaired free water clearance is observed in about 60% of patients with cirrhosis.130
Hypervolaemic hyponatraemia requires a negative water balance.47 Many hepatologists do recommend fluid restriction of between 1 and 1.5 L/day in presence of severe hyponatraemia (serum sodium <125 mmol/L). However, there are few data to support the level of serum sodium at which to initiate fluid restriction and how much fluid to restrict. It is sodium restriction and not fluid restriction that results in weight loss as fluid passively follows the sodium.62 113 131 Although fluid restriction may be helpful in preventing further decrease in serum sodium, it only rarely improves it. This is because on a practical level, fluid restriction to <1 L /day is not tolerated.129 Water restriction should be reserved for those who are clinically hypervolaemic with severe hyponatraemia (serum sodium <125 mmol/L) with normal serum creatinine and not currently receiving diuretics. These recommendations are based on our consensus and consistent with our earlier guidelines.132 It is also our consensus that fluid restriction is unnecessary in absence of hyponatraemia.
Hypertonic sodium chloride (3%) administration may improve hyponatraemia at the cost of worsening fluid overload. It is best reserved for those with severely symptomatic acute hyponatraemia, especially if a transplant is imminent.47 To prevent rapid increase in serum sodium and the risk of developing central pontine myelinolysis,133 guidelines recommend a serum sodium increase of up to 5 mmol/L in the first hour with a limit of 8–10 mmol/L every 24 hours thereafter until the serum sodium concentration reaches 130 mmol/L.47 116 134 135
Vaptans
Vaptans are vasopressin antagonists that competitively bind and block the V2-receptors of arginine vasopressin in the renal collecting ducts and induce a highly hypotonic diuresis without affecting the excretion of electrolytes.136 In three RCTs involving 1200 patients, satavaptan was no more effective than placebo in controlling ascites and need for LVPs, though it improved serum sodium concentration in those with hyponatraemia.137 Two of the studies were terminated owing to an increase in serum bilirubin, higher mortality (31% vs 22%), mostly due to increased cirrhosis complications and other adverse events.137 Two meta-analyses138 139 on vaptans in cirrhosis reported improved serum sodium levels and ascites mobilisation, but without a beneficial effect on cirrhosis-related complications or mortality (RR=1.06, 95% CI 0.90 to 1.26). Current evidence does not support routine use of vaptans in cirrhosis.
Midodrine
Portal hypertension and splanchnic vasodilatation are major contributors to the development of ascites.7 In fact, mean arterial pressure and plasma norepinephrine are two of the best predictors of prognosis in ascites.140 Therefore, vasopressors such as midodrine, an α-adrenergic agonist, have been used in non-azotemic patients with ascites, resulting in significant increase in mean arterial pressure and urine sodium excretion and significant decreases in plasma renin and aldosterone.141
A small RCT in patients with refractory ascites (midodrine 7.5 mg three times a day vs standard medical therapy) showed that at 3 months 94% versus 50% had a complete/partial ascites control, with a trend for a survival benefit in the midodrine group.142 In another small RCT (midodrine vs placebo), significant reduction in body weight and abdominal girth was observed after 2 weeks of midodrine therapy.143 Though larger RCTs are needed to confirm these findings, it may be appropriate to consider use of midodrine in refractory ascites on a case-by-case basis.
Recommendations
In patients with the first presentation of moderate ascites spironolactone monotherapy (starting dose 100 mg, increased to 400 mg) is reasonable. In those with recurrent severe ascites, and if faster diuresis is needed (for example, if the patient is hospitalised), combination therapy with spironolactone (starting dose 100 mg, increased to 400 mg) and furosemide (starting dose 40 mg, increased to 160 mg) is recommended. (Quality of evidence: moderate; Recommendation: strong)
All patients initiating diuretics should be monitored for adverse events. Almost half of those with adverse events require diuretic discontinuation or dose reduction. (Quality of evidence: low; Recommendation: weak)
Hypovolaemic hyponatraemia during diuretic therapy should be managed by discontinuation of diuretics and expansion of plasma volume with normal saline. (Quality of evidence: low; Recommendation: weak)
Fluid restriction to 1–1.5 L/day should be reserved for those who are clinically hypervolaemic with severe hyponatraemia (serum sodium <125 mmol/day). (Quality of evidence: low; Recommendation: weak)
Hypertonic sodium chloride (3%) administration should be reserved for those who are severely symptomatic with acute hyponatraemia. Serum sodium should be slowly corrected. (Quality of evidence: low; Recommendation: weak)
It may be appropriate to consider use of midodrine in refractory ascites on a case-by-case basis. (Quality of evidence: low; Recommendation: weak)
Large volume (therapeutic) paracentesis
Large volume paracentesis (LVP) is the standard of care for managing large volume ascites both in conjunction with diuresis to relieve symptoms of a tense abdomen, as well as in the management of refractory ascites, when diuretics become ineffective or the side effects preclude their continued use. Development of refractory ascites is of prognostic significance,144 therefore, at its onset, suitability of liver transplantation should be considered and assessed as a priority.
Performance standards
An efficient LVP service can be provided safely in a day case or outpatient setting and non-physician healthcare providers such as GI endoscopy assistants145 and specialist nurses146 can be trained to perform therapeutic paracentesis and lead the service effectively. Exemplar training programmes indicate that 10 supervised procedures would be optimal for training to achieve competence in performing therapeutic paracentesis; mean duration of LVP was 97±24 min, and the mean volume of ascitic fluid removed was 8.7±2.8 L.145
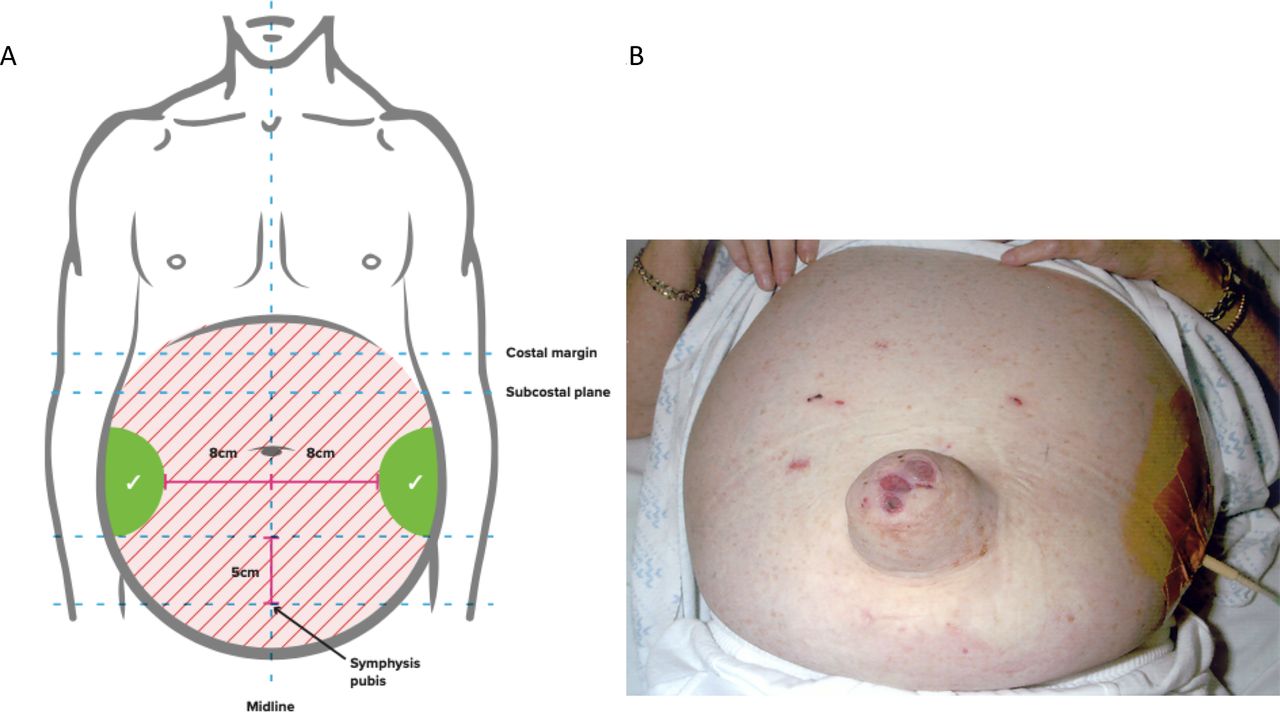
Patients should provide informed consent before the procedure. In 52 patients (15% obese) with ascites due to cirrhosis, ultrasound demonstrated that the left lower quadrant abdominal wall was thinner and depth of ascites greater, therefore, a suitable site for drain insertion.147 To minimise the risk of injury to the inferior epigastric artery (and avoid the liver and spleen) during paracentesis, point of puncture should be at least 8 cm from the midline and 5 cm above the symphysis148–150 (figure 4). All ascitic fluid should be drained to dryness in a single session as rapidly as possible over 1–4 hours assisted by gentle mobilisation of the cannula or turning the patient onto their side, if necessary. After the paracentesis, the patient should lie on the opposite side for 2 hours if there is leakage of any remaining ascitic fluid, and/or a suture (ideally purse-string) inserted around the site of drainage. These steps help to minimise the risk of ascitic fluid leakage.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Anatomical landmarks for the safe performance of paracentesis [A] and performance of ascites drainage in patients with large ascites [B].
Adverse events
A systematic review of adverse events that can result from a paracentesis reported an overall rate of significant bleeding ranging from 0% to 2.7%, ascitic fluid leak in 0% to 2.35%, perforation in 0.83%, residual catheter tip fragment in 0.41% and death in 0% to 17% among studies that were heterogeneous.18 In a retrospective study published in abstract form, of consecutive 3116 ultrasound guided LVPs, the mean international normalised ratio (INR) was 2.1 (range 1.0–7.0) and MELD score 24 (range 6–40) for inpatients, and 1.5 (range 1‐5–5) and 16 (range 5–40) for outpatients, respectively. With no patients receiving fresh frozen plasma (FFP) before the procedure, a total of six patients (0.19%) had post‐LVP bleeding requiring blood transfusion (one inpatient, five outpatients) and one required angiography with embolisation of a bleeding abdominal wall vessel. No patient died.151 In another study where GI endoscopy assistants performed 1100 large volume paracenteses, with a preprocedure mean INR of 1.7 (range 0.9–8.7) and the mean platelet count was 50.4×109/L (range, 19–341×109/L), there were no significant procedure-related complications.145
Risk factors for haemorrhagic complications after paracentesis in three studies (which included patients with acute on chronic liver failure) were high MELD and Child-Pugh scores and renal impairment.152–154 In a study by Hung et al, acute kidney injury at he time of paracentesis was the only independent predictor of post-paracentesis haemoperitoneum, independent of MELD score, large volume paracentesis, sepsis, platelets, INR and haemoglobin levels.153 While some patients with bleeding complications after paracentesis have low platelet counts, elevated INR and low fibrinogen levels, this is invariably accompanied with high MELD scores (>25) and/or renal impairment.152 154
Ultrasound guidance
Use of ultrasound guidance may reduce the adverse events related to LVP.155 In a study involving 1297 procedures, 723 (56%) with ultrasound guidance and 574 (44%) without where the indications for paracentesis were similar between the two groups, the incidence of adverse events was lower in the ultrasound-guided procedures.156 In another retrospective cohort study, 0.8% of 565 patients undergoing paracentesis experienced bleeding complications. After adjustment, ultrasound guidance was associated with lower risk of bleeding complications by 68%.157
Recommendations
Patients should give informed consent for a therapeutic or diagnostic paracentesis. (Quality of evidence: low; Recommendation: strong)
Ultrasound guidance should be considered when available during LVP to reduce the risk of adverse events. (Quality of evidence: low; Recommendation: weak)
Routine measurement of the prothrombin time and platelet count before therapeutic or diagnostic paracentesis and infusion of blood products are not recommended. (Quality of evidence: moderate and Recommendation: strong)
Use of human albumin solution (HAS)
Plasma expansion after paracentesis
One study evaluating haemodynamic and neurohumoral responses in 12 patients after a single, 5 L total paracentesis concluded that it was safe to omit albumin in these patients.158 However, a subsequent study including 80 patients with acute on chronic liver failure (ACLF) found that albumin significantly reduced complications (renal impairment, hyponatraemia and death) following <5 L paracentesis compared with no administration of fluid.159 Thus in <5 L paracentesis we recommend that plasma expansion is not necessary, unless there is evidence of ACLF. This recommendation is based on consensus rather than evidence and is consistent with other international guidance.47
Plasma volume expansion should always be used for LVP with >5 L of ascites removed. Serial paracenteses with and without albumin replacement have been evaluated in patients with tense ascites.123 124 There was a higher rate of renal impairment, fall in serum sodium levels, and a marked activation of the renin–angiotensin–aldosterone system in those not treated with albumin. However, the pooled risk ratio from these studies, which are more than 25 years old, showed only a tendency toward benefit of albumin (pooled RR=0.23, 95% CI 0.03 to 1.64) (online supplemental table 5). The consensus is that volume expansion should be used with LVP. We recommend large volume paracentesis in one session and discourage repeated low volume paracentesis, which offers no additional benefits and carries a higher risk of procedure-related complications.
Some debate remains over the use of albumin or artificial plasma expanders for volume expansion. Pooled analysis of 10 studies160–169 found that cirrhotic patients undergoing paracentesis who received albumin were no less likely to develop renal dysfunction than patients undergoing paracentesis that received an alternative plasma expander (pooled RR=1.11, 95% CI 0.58 to 2.14) (online supplemental table 5). Analysis from two other independently conducted systematic reviews is consistent with these findings.127 128 Pooled analysis from eight studies160 162–164 166 167 169 170 found that cirrhotic patients undergoing paracentesis who received albumin were no less likely to die than those who received an alternate plasma expander (pooled RR=0.83, 95% CI 0.61 to 1.12) (online supplemental table 6), which is supported by two systematic reviews.127 128 However, when all comparators to albumin (including control and vasoconstrictor alone) are pooled (16 RCTs) the RR is 0.77 (95% CI 0.57 to 1.00). This translates to 57 to 100 fewer patients per 1000 dying after LVP when HAS is used (online supplemental table 6).
Less clinically important outcomes have been shown to improve in patients treated with HAS versus other plasma expanders. There is a decreased incidence of post-paracentesis-induced circulatory dysfunction (defined as a decrease in plasma renin) in patients undergoing LVP treated with albumin compared with an alternative plasma expander in a meta-analysis containing eight RCTs127 (OR=0.34, 95% CI 0.23 to 0.51), and a pooled decrease in hyponatraemia in nine RCTs (OR=0.61, 95% CI 0.40 to 0.93).127 Both are supported in a second independently conducted systematic review.128
Most of the plasma expanders used in the described studies are no longer in use and have been restricted by the European Medicines Agency (eg, polygeline carries risk of prion transmission, dextran the risk of allergic reaction and hydroxyethyl starch association with renal impairment and deranged coagulation). Therefore, consensus is that volume expansion should be with HAS due to availability, familiarity of use and suggested benefits in the available studies.
Two small prospective RCTs compared standard dose (6–8 g/L of ascites drained) albumin after LVP with low-dose albumin (2–4 g/L).171 172 Pooled results from 70 patients suggested no difference in post-paracentesis-induced circulatory dysfunction (RR=2.97, 95% CI 0.89, 9.91) and no development of renal dysfunction (no events in either group). A larger retrospective review of 935 patients found no increase in renal dysfunction when adherence to guidance (8 g/L after 5 L drained) was implemented,173 but significant cost savings were made because less HAS was used.
Potential cost savings have been proposed in relation to length of hospital stay in patients with ascites undergoing LVP who are treated with HAS as compared with an alternative plasma expander.166 However, HAS is more expensive than alternatives and is in worldwide shortage, therefore it should be prescribed according to recommended guidance based on the available evidence.174 There have been no cost-effectiveness analyses in the UK.
Until further studies are undertaken to compare efficacy of albumin against clinically available artificial plasma expanders, we would recommend that albumin remains the preferred plasma expander when paracentesis is undertaken. Albumin (as 20% or 25% solution) should be infused after paracentesis of >5 L is completed at a dose of 8 g albumin/L of ascites removed.
Albumin infusion in SBP
Renal impairment develops in up to 30% of patients with SBP and is one of the strongest predictors of mortality,175 176 alongside progressive liver dysfunction. Three studies176–178 have compared albumin with no intervention, and one RCT179 compared albumin with a plasma expander in order to prevent the development of renal impairment in patients with SBP. Cirrhotic patients with SBP treated with albumin were 72% less likely to develop renal dysfunction than patients with SBP who did not receive albumin (288 patients, pooled RR=0.28, 95% CI 0.16 to 0.50) (online supplemental table 7). There was also a decrease in mortality in patients with SBP treated with albumin, with patients 47% less likely to die than those not receiving albumin (334 patients, pooled RR=0.53, 95% CI 0.36 to 0.79) (online supplemental table 8). Therefore, we recommend the use of albumin in patients with SBP to prevent the development of renal dysfunction and decrease mortality.
Although patients with SBP have a higher risk of post-drain renal dysfunction, LVP is not contraindicated. Therefore, if LVP is indicated in a patient with SBP then this should proceed with HAS support. The dose of albumin in original studies was 1.5 g albumin per kg body weight within 6 hours of diagnosis and 1.0 g/kg on day 3, using estimated dry weight, which is often difficult in cirrhotic patients. Some small studies have suggested that lower doses of albumin are as effective in preventing renal dysfunction and mortality in SBP,180 181 and one retrospective review including 88 patients with SBP suggested that doses of HAS in excess of 87.5 g (>4×100 mL 20% HAS) are associated with a worse outcome, possibly secondary to fluid overload.182 Fluid overload has been reported in prospective studies of albumin in patients with cirrhosis and non-SBP infection.183 184 Therefore, if patients have an increased serum creatinine or a rising serum creatinine, we recommend 1.5 g albumin/kg within 6 hours of diagnosis, followed by 1 g/kg on day 3.
Long term regular outpatient HAS therapy
Improving morbidity and mortality by long-term administration of albumin to patients with decompensated cirrhosis and ascites has been explored in six studies with three recent RCTs, in contrasting patient groups, with contradictory findings (online supplemental table 9).185–190
In the ANSWER185 study, 431 patients with uncomplicated ascites receiving diuretics were randomised to weekly outpatient HAS infusions or no additional intervention (standard medical therapy). The study had a pragmatic approach and was unblinded. Overall 18-month survival was significantly higher in the standard therapy plus HAS than in the standard medical therapy group (Kaplan-Meier estimates 77% vs 66%; p=0.028), resulting in a 38% reduction in the mortality hazard ratio (0.62, 95% CI 0.40 to 0.95). There were additional benefits with lower incidence rate ratio (IRR) for infection (SBP and non-SBP) and renal dysfunction. However, unlike the standard therapy group, the HAS group had weekly medical professional contact when IV albumin was administered which could possibly have caused a confounding effect by improving standard of care in this group.
In the MACHT186 study, a double-blind, placebo-controlled trial, patients with advanced cirrhosis (MELD score 17–18) awaiting liver transplantation received outpatient fortnightly treatment with midodrine and albumin. This slightly suppressed vasoconstrictor activity but did not prevent complications of cirrhosis or improve survival. However, only nine patients were treated for the entire year, the median length of treatment was only 80 days and the mortality rate in both arms was very low due to patients undergoing timely liver transplantation. Perhaps, therefore, a greater dose of albumin or longer duration of treatment is required to benefit patients and should be targeted at those who are not close to receiving a liver transplant.
Di Pascoli et al 190 most recently published outcomes of a study of 45 patients with refractory ascites undergoing regular LVP who accepted 20 g twice weekly albumin plus diuretics and sodium restriction versus 25 patients who did not (non-randomised, single centre, not blinded). Cumulative incidence of mortality was 41.6% in the albumin group versus 65.5% in the standard of care group. Albumin-treated patients had a lower probability of hospitalisation. There were no differences in the number of LVPs performed. Follow-up was 400 days in the albumin group and 318 in the standard of care group. Although the study was non-randomised (patient choice to treatment arm) it does provide some additional evidence that using albumin in a longer-term outpatient setting may be beneficial, as in the ANSWER study, even in patients with very advanced disease. Two older studies support the use of outpatient albumin therapy in decreasing hospital admissions and LVP requirement with conflicting results on mortality.187 189
We expect these studies to stimulate further investigation to determine whether long-term albumin administration is feasible, efficacious and cost-effective in patients with cirrhosis and ascites within the NHS. Further research is required to determine which patients could benefit most from treatment, which seems to be those with less advanced disease who could receive treatment for at least 12 months. At present it is not possible to recommend the use of outpatient albumin administration in patients with ascites due to cirrhosis.
Recommendations
Albumin (as 20% or 25% solution) should be infused after paracentesis of >5 L is completed at a dose of 8 g albumin/L of ascites removed. (Quality of evidence: high; Recommendation: strong)
Albumin (as 20% or 25% solution) can be considered after paracentesis of <5 L at a dose of 8 g albumin/L of ascites removed in patients with ACLF or high risk of post-paracentesis acute kidney injury. (Quality of evidence: low; Recommendation: weak)
In patients with SBP and an increased serum creatinine or a rising serum creatinine, infusion of 1.5 g albumin/kg within 6 hours of diagnosis, followed by 1 g/kg on day 3, is recommended. (Quality of evidence: low; Recommendation: weak)
Transjugular intrahepatic portosystemic stent shunt (TIPSS)
TIPSS decompresses the portal system by creating an artificial communication between the portal and the hepatic vein. TIPSS results in an increase in cardiac output and decrease in systemic vascular resistance in the short term.191–193 Consequently, TIPSS leads to improvement in effective hypovolaemia and renal function, resulting in increased urinary sodium excretion.191–195 The increase in urinary sodium correlates with the reduction in plasma renin activity.195 196
The efficacy of TIPSS in the management of ascites has been compared with LVP in seven RCTs (online supplemental table 10).194 197–202 The first six trials used bare metal stents. Shunt dysfunction due to stent stenosis or thrombosis is a common complication of bare stents and develops in up to 80% of patients.199 201 The use of polytetrafluoroethylene (PTFE)-covered stents has significantly increased the long-term patency of the stent to 92% at 1 year and 89% at 2 years.202–204
TIPSS controls ascites better than LVP. Patients treated with TIPSS are more likely to be free of recurrent ascites than those treated with LVP at 12 months.205 However, the impact of TIPSS on survival is less consistent. The initial trial by Lebrec et al 194 showed a better survival with LVP mainly due to the detrimental effect of TIPSS in Child-Pugh C patients. The subsequent three studies did not show any difference in survival between TIPSS and LVP,197–199 whereas the most recent three studies have shown improved survival with TIPSS.200–202 In the two meta-analyses of the six trials using bare stent grafts, Bai et al 205 reported an improved transplant-free survival with TIPSS but this was limited to patients with recurrent ascites and not refractory ascites in the other study.206 All the six trials with bare metal stents consistently showed that TIPSS resulted in higher incidence of hepatic encephalopathy than with LVP.
PTFE-covered stents are now standard of care, and hence the results of the historical RCTs using bare stents are less relevant. Only the most recent RCTs compared PTFE-covered stent with LVP in patients with recurrent ascites. It demonstrated improved 1-year survival with TIPSS without any increased incidence of hepatic encephalopathy.202
TIPS has also been shown to improve the quality of life and nutritional status in patients with refractory ascites,207–209 but the improvement was dependent on the resolution of ascites.
TIPSS technique
A controlled study comparing TIPSS with 8 mm and 10 mm covered stent was stopped early as the 8 mm stent was not effective in controlling portal hypertensive complications (variceal bleeding and ascites).210 The rate of hepatic encephalopathy was equal between the two groups. However, in another study of variceal bleeding, 8 mm stents were as effective as 10 mm stents in preventing rebleeding, with a 50% reduction in the incidence of encephalopathy with 8 mm stents.211 Nonetheless, the applicability of these data in patients with refractory ascites is unclear, and evidence suggests that stent diameter increases over time.212 In a retrospective study of patients with refractory ascites, 10 mm covered stent led to better control of ascites than an 8 mm stent, without any increase in encephalopathy.213 Data from recent TIPSS registry in Germany reported an improved survival with 8 mm than with 10 mm covered stent.214 The optimal diameter of covered TIPS stent in refractory ascites remains unclear.
The volume of TIPSS being performed in an individual hospital influences outcomes. Inpatient mortality was significantly lower in centres performing more than 20 TIPS procedures per year.215
Patient selection
Careful selection of patients with refractory ascites to be treated with TIPSS is vital to maximise the benefits and reduce the harmful effects of the treatment. The exclusion criteria for the insertion of TIPSS in the seven RCTs are reported in online supplemental table 10.
Patients with advanced stages of cirrhosis have been excluded from the trials as indicated by serum bilirubin,197–202 prolonged prothrombin time,198 199 renal dysfunction194 197 198 200–202 and Child-Pugh score.200–202 Presence of chronic hepatic encephalopathy was an exclusion criterion in all the RCTs; the presence of pre-TIPS encephalopathy has been shown to be a predictor of poor outcome following TIPSS.216–218
In retrospective studies, patients with advanced disease had a worse outcome following TIPS insertion. The MELD score was originally developed to predict survival following TIPSS and included serum creatinine, bilirubin, INR and aetiology of cirrhosis.219 The MELD score has now evolved into a prognostic score in patients with cirrhosis.220 Among patients with refractory ascites treated with TIPSS with covered stent, 1-year survival is 84% in those with MELD score <15 compared with 54% for MELD score >18.221 In refractory ascites, a simple model of serum bilirubin and platelet count has been shown to predict 1-year survival.222 The survival rate of patients with serum bilirubin >50 µmol/L or platelet count of <75×109/L was only 31.2% compared with 73.1% in patients with serum bilirubin <50 µmol/L and platelet count of >75×109/L. The exact survival rate quoted here has to be interpreted cautiously as earlier patients in the cohort were treated with a bare metal stent before the introduction of a PTFE-covered stent. Hyponatraemia has also been shown to be related poor survival following TIPSS,223 but subsequent studies have not reproduced this finding.221 224 Up to 50% of patients with decompensated cirrhosis have sarcopenia, which in turn negatively affects clinical outcome in these patients. However, the direct impact of sarcopenia on outcomes following TIPSS is unclear. Sarcopenia has been shown to be independently associated with development of post-TIPSS encephalopathy, but this study included patients with refractory ascites and uncontrolled variceal bleeding.225 A recent retrospective study published in abstract form on patients undergoing TIPSS for refractory ascites reported no impact of sarcopenia on outcomes after TIPSS.226 Furthermore, they reported an improvement in muscle mass following TIPSS insertion.
Although increasing age has been associated with poorer survival following TIPSS,215 227 228 the mean age in these studies was between 54 and 57 years. Patients above the age of 70 were generally excluded from the previously mentioned RCTs. There is a lack of data in the literature for clinical outcome following TIPS in older patients (>70 years). Interestingly, functional disability as measured by patient-reported activities of daily living predicts post-TIPSS mortality adjusted for MELD score.229
The management of hepatic encephalopathy after TIPSS is beyond the scope of this document and is discussed in the recent BSG/BASL TIPSS guidelines.
Recommendations
TIPSS should be considered in patients with refractory ascites. (Quality of evidence: high; Recommendation: strong)
Caution is required if considering TIPSS in patients with age >70 years, serum bilirubin >50 µmol/L, platelet count <75×109/L, MELD core ≥18, current hepatic encephalopathy, active infection or hepatorenal syndrome. (Quality of evidence: moderate; Recommendation: strong)
Management of umbilical hernia in patients with ascites
In the cirrhotic patient, the incidence of abdominal wall hernia is 16% and reaches 24% in the presence of ascites; more than half of these are umbilical hernias.230 These progressively enlarge and are prone to complications, including ulceration of the overlying skin, incarceration, strangulation, and rupture. Non-operative management of complicated hernias with antibiotics and dressing changes might result in mortality rates in the range of 60–88%.231 On the other hand, hernia repair in cirrhosis has often been avoided due to high postoperative morbidity and mortality. Emergency surgery (OR=10.32, 95% CI 3.66 to 47.82), Child-Pugh-Turcotte class C (OR=5.52, 1.67 to 32.45), American Society of Anaesthesiologists (ASA) score ≥3 (OR=8.65, 3.65 to 87.23) and MELD score ≥20 (OR=2.15, 2.71 to 32.68) are associated with mortality.232
A recent retrospective series of 102 patients, who underwent surgical repair of the umbilical hernia in the presence of ascites, included 45 patients having emergency surgery (24 with incarceration, 12 with rupture of the hernia sac, and nine with skin ulceration or necrosis). Morbidity and mortality rates of 37.2% and 3.9%, respectively, were observed.233 Optimising management of ascites, including LVP and TIPSS perioperatively, could reduce the risk of wound dehiscence and recurrence of hernia.234
Recommendations
Suitability and timing of surgical repair of umbilical hernia should be considered in discussion with the patient and multidisciplinary team involving physicians, surgeons and anaesthetists. (Quality of evidence: low; Recommendation: strong)
Hepatic hydrothorax
Hepatic hydrothorax (HH) is accumulation of transudative fluid in the pleural space in the absence of cardiac, pulmonary or pleural disease, affecting approximately 5–12% of patients with advanced liver disease.235 The first-line management of hydrothorax is based on controlling ascites with diuretics and/or LVP as discussed previously. However, pleural effusion can persist despite successful treatment of ascites, defined as refractory hydrothorax.47
Therapeutic thoracentesis is required to provide symptomatic relief from dyspnoea but the effect is transient. Repeated procedures increase the risks of complications, including pneumothorax, bleeding and pleural infection.236 TIPSS has been suggested either as a definitive treatment or as a bridge to transplantation in patients with refractory hydrothorax. Meta-analysis of six retrospective studies with a total of 198 patients reported a response rate of 56%.237 Mortality within 45 days of TIPSS placement was 18%, mainly related to older age and the severity of liver disease. However, without any data on comparison with standard treatment, it is difficult to interpret the impact of TIPSS on survival. It is also worth noting that only one of these studies reported on patients treated with PTFE-covered stents.238 In patients with contraindications to TIPSS or liver transplant, a permanent indwelling pleural catheter can be considered in conjunction with the patient and the multidisciplinary team taking into account the infection risk.
Recommendation
TIPSS should be considered in patients with HH after discussion with the multidisciplinary team. (Quality of evidence: low; Recommendation: strong)
In patients with HH who are not undergoing a TIPSS and/or a liver transplant evaluation, alternative palliative interventions should be considered. (Quality of evidence: low; Recommendation: strong)
Non-selective beta-blockers and ascites
The portal pressure-lowering effects of non-selective beta-blockers (NSBB) have been known to be beneficial in patients with ascites for three decades. Lebrec’s group demonstrated back in 1991 in a meta-analysis of trial data that NSBB reduce the likelihood of first variceal haemorrhage in the ascites subgroup, while in Child’s Pugh B and C cirrhosis the addition of NSBB to band ligation results in less variceal rebleeding and superior survival.239 240 Proven haemodynamic response to NSBB (drop in hepatic venous pressure gradient (HVPG) of ≥10–20% from baseline, or to <12 mm Hg) has been linked with a lower probability of the development of ascites; and in patients already with ascites, a lower probability of refractory ascites and hepatorenal syndrome.241 242 However, it remains possible that non-response in this context is simply a surrogate marker for disease severity.
In recent years, there has been increasing recognition that the benefits of NSBB in patients with cirrhosis may not be exclusively explained by the reduction in portal pressure. NSBB reduce markers of intestinal permeability, bacterial translocation, systemic inflammation and the incidence of spontaneous bacterial peritonitis independently of haemodynamic response, suggesting a direct effect, potentially via intestinal transit time or on the bowel mucosal integrity.243–245 Given the mounting evidence that bacterial translocation and the systemic inflammatory response contribute to the downward spiral of circulatory dysfunction in cirrhosis, it follows that NSBB may also reduce non-bleeding related mortality.61 246
Despite all this, Lebrec et al 194 introduced controversy to the beta-blocker story in 2010 when his team reported that patients with refractory ascites receiving NSBB had greater all-cause mortality during long-term follow-up.247 The window hypothesis has since been proposed, which postulates that refractory ascites represents the tipping point in portal hypertension when the cardio-inhibitory effects of NSBB compromise organ perfusion.246 Krag and coauthors suggest that the ‘window’ of benefit from NSBB opens when grade 2 oesophageal varices develop and closes with the development of refractory ascites. Yet, concerns have been raised about the methodology of the original observational study; and many subsequent studies, including five meta-analyses and three with propensity risk score matching, have shown either similar or superior survival in patients with refractory ascites receiving NSBB.175 240 247–253 Of relevance is that the Lebrec data observed patients receiving a relatively high dose of NSBB compared with many of the other cohorts studied, and the NSBB type (carvedilol vs propranolol) may be important.247 254
We conclude that, until randomised high-quality data are available, the current evidence supports the use of NSBB when indicated in patients with refractory ascites (online supplemental table 11), unless alternative markers of circulatory failure, such as hypotension or reduced glomerular filtration rate, are present.175
Recommendation
Refractory ascites should not be viewed as a contraindication to NSBB. (Quality of evidence: moderate; Recommendation: strong)
Patients with refractory ascites who are taking NSBB should be monitored closely, and dose reduction or discontinuation may be appropriate in those who develop hypotension or acute/progressive renal dysfunction. (Quality of evidence: moderate; Recommendation: strong)
Automated low-flow ascites pump (ALFApump)
The ALFApump system consists of a subcutaneously implanted battery-powered programmable pump. It is connected to catheters that transfer ascites from the peritoneal cavity to the bladder, from which it is eliminated with urine. Initially, two multicentre safety and efficacy studies255 256 reported substantial reduction of the number and volume of paracenteses in patients with advanced cirrhosis and refractory ascites. However, adverse effects directly related to the device occurred in up to 39% of cases. In a multicentre RCT in patients with refractory ascites, the ALFApump significantly reduced the need for paracentesis and was associated with significantly improved chronic liver disease questionnaire, nutritional parameters such as hand-grip strength and body mass index.257 Meta-analysis of the data from the RCT and several case series showed that 62% of the patients did not require LVP following pump insertion.258 Pooled estimate rates were 30% for acute kidney injury, 27% for bacterial peritonitis and 20% for urinary tract infection. The device had no effect on survival. Currently, NICE recommends that the ALFApump should be used only with special arrangements for clinical governance, consent and audit or research.259
Recommendation
Automated low-flow ascites pump should be considered only in special circumstances with robust arrangements of clinical governance, audit or research. (Quality of evidence: low; Recommendation: weak)
Hepatorenal syndrome
Patients with cirrhosis and ascites can develop a specific form of renal dysfunction, which is termed hepatorenal syndrome (HRS). Traditionally HRS was thought to be due to the altered haemodynamic alterations with hyperdynamic circulation as well as overactive endogenous vasoactive system which results in renal hypoperfusion.260 It is now recognised that systemic inflammation also plays an important role in the pathophysiology of HRS.261 262
The traditional classification of HRS-1 and HRS-2 has recently been revised by the International Club of Ascites.263 HRS-1, which reflects a rapid reduction in renal function, has been proposed to be changed to HRS-acute kidney injury (HRS-AKI). The new definition of HRS-AKI includes an increase in serum creatinine of ≥0.3 mg/dL (27 µmol/L) within 48 hours or ≥50% from baseline, without necessitating a final cut-off value of 1.5 mg/dL (133 µmol/L). This allows treatment to be started earlier. HRS-2, which represents renal dysfunction that does not progress rapidly, has been proposed to be changed to HRS-NAKI (non-AKI).263
The mainstay of treatment of HRS-AKI involves HAS and vasoconstrictors, particularly terlipressin. Combination of terlipressin and HAS has been shown in RCTs to significantly improve renal function in HRS-AKI and improve short-term mortality (online supplemental table 12).264–266 Higher baseline serum creatinine is an independent predictor of failure to respond to vasoconstrictor treatment.262 267 A full review of HRS is beyond the scope of this guideline.
Palliative care
Palliative care is integral to the management of advanced non-cancer conditions, such as cardiac, respiratory and renal disease, often supported by practice guidelines.268–270 Patients with cirrhosis and ascites often report a poor quality of life,271 this being an independent predictor of 12-month mortality.272 However, only a minority of patients with advanced cirrhosis receive timely palliative care and this has been discussed in recent reviews.273 274 A British study indicated that from 2013 to 2015, of the 45 000 cirrhosis-related deaths, about a third required LVP in the last year of their life, overall healthcare costs being over £21 000 per person.275
Substantial literature supports the use of palliative tunnelled long-term abdominal drains (LTAD) in individuals with refractory ascites due to malignancy, including NICE medical technology guidance.276–279 These drains are inserted in hospital and allow drainage of small amounts of ascites 2–3 times a week at home. Potential advantages over LVP include symptom-guided drainage and avoidance of repeated hospitalisations. A recent systematic review on LTAD in cirrhosis showed that the majority of patients could be managed in the community.280
Results from a recent feasibility RCT comparing palliative LTAD with LVP in refractory ascites due to cirrhosis have just been published (REDUCe study).281 In this 3-month study, 36 patients were randomised, 19 to LVP and 17 to LTAD. All patients received prophylactic antibiotics for the study duration. Following randomisation, the median number (IQR) of hospital ascitic drains for LTAD versus LVP groups were 0 (0, 1) versus 4 (3, 7), respectively. Only two patients allocated to LTAD required hospital admissions specifically for ascites drainage. Self-limiting cellulitis/leakage occurred in 41% (7/17) in the LTAD vs 11% (2/19) in the LVP group; peritonitis incidence being 6% (1/17) vs 11% (2/19), respectively. Median (IQR) fortnightly community/hospital/social care ascites-related costs were lower in the LTAD group than in the LVP group, £329 (253, 580) versus £843 (603, 1060), respectively. Qualitative data (currently only published as a summary) indicate that LTAD could transform the care pathway.281
The REDUCe study demonstrates feasibility, with preliminary evidence of LTAD acceptability, effectiveness and safety and reduction in health resource use. Future trials should assess LTAD as a palliative intervention for refractory ascites in cirrhosis.
Recommendations
Patients with refractory ascites who are not undergoing evaluation for liver transplant should be offered a palliative care referral. Besides repeated LVP, alternative palliative interventions for refractory ascites should also be considered. (Quality of evidence: weak; Recommendation: strong)
Conclusions
The development of ascites is a landmark in the natural history of cirrhosis. Therefore, it should be considered an important time point at which an individual patient’s suitability for liver transplantation which is a definitive treatment of ascites and its complications, should be determined. Over the years, there has been a substantial improvement in care of patients with cirrhosis, including those with ascites. A study involving over 780 000 hospitalisations of patients with cirrhosis demonstrated an improvement in inpatient survival over a decade despite higher age and more medically complex disease.282 This was remarkably consistent across several cirrhosis complications, suggesting improved cirrhosis care beyond general improvements in inpatient care. Future research should focus on areas of need and questions where there is no high-quality evidence to guide the management of ascites.
Research recommendations
Randomised controlled trials (RCTs) with large sample size should evaluate the role of antibiotics in the secondary prophylaxis for SBP in ascites secondary to cirrhosis.
Large RCTs should assess the role of midodrine in the management of ascites.
Cost-effectiveness of long-term administration of HAS to patients with decompensated cirrhosis and ascites should be evaluated.
Role of nutritional interventions in the management of ascites should be evaluated.
Large RCT of long-term carvedilol versus no carvedilol in patients with refractory ascites without large oesophageal varices should be carried out.
Role of TIPSS in the management of hepatic hydrothorax should be compared with other therapeutic interventions.
The cost-effectiveness and the effect of automated low-flow ascites pumps on the quality of life of patients with refractory ascites should be evaluated.
Effectiveness and safety of long-term abdominal drains should be assessed in RCTs for the palliative care of patients with cirrhosis and refractory ascites.
Acknowledgments
We are grateful to Shani Steer, voluntary peer mentor, Brighton for her involvement and review of these guidelines. We wish to thank the BSG Liver Section for support and internal review of the guideline. We are grateful to BASL for review and endorsement of this guideline. We also thank Peuish Sugathan and Nottingham University Hospitals NHS Trust for providing data on the underlying aetiology in patients with new onset ascites.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors GA: senior author. NP: co-author (TIPSS, hepatic hydrothorax). LC: co-author (albumin in ascites). SH: co-author (albumin in ascites). LM: co-author (paracentesis). JMR: co-author (spontaneous bacterial peritonitis). EAW: co-author (diagnostic paracentesis). KM: senior author. JAL: co-author (beta-blockers in ascites). PCH: senior author (beta-blockers in ascites). AJO: senior author (albumin in ascites). SV: senior author (diuretics, palliative care). All authors reviewed and approved the final document.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests SV and LM: Received support from Rocket Medical for the NIHR funded REDUce Study.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.