Article Text

Abstract
Introduction The influence of n-3 long-chain polyunsaturated fatty acids (LCPUFA) supplementation on brain functioning is debated. Some studies have found positive effects on cognition in children with learning difficulties, elderly people with cognitive impairment and depression scores in depressed individuals. Other studies have found null or negative effects. Observational studies in adolescents have found positive associations between fish consumption (containing n-3 LCPUFAs) and academic achievement. However, intervention studies in typically developing adolescents are missing.
Objective The goal of this study is to determine the influence of increasing Omega-3 Index on cognitive functioning, academic achievement and mental well-being of typically developing adolescents.
Methods and data analysis Double-blind, randomised, placebo controlled intervention; 264 adolescents (age 13–15 years) attending lower general secondary education started daily supplementation of 400 mg eicosapentaenoic acid and docosahexaenoic acid (EPA+DHA) in cohort I (n=130) and 800 mg EPA+DHA in cohort II (n=134) or a placebo for 52 weeks. Recruitment took place according to a low Omega-3 Index (<5%). The Omega-3 Index was monitored via a finger prick at baseline and after 3, 6 and 12 months. The supplement dose was adjusted after 3 months (placebo analogously) to reach an Omega-3 Index of 8–11%. At baseline, 6 and 12 months, a neuropsychological test battery, a number of questionnaires and a standardised math test (baseline and 12 months) were administered. School grades were collected. In a subsample, sleep quality and quantity data (n=64) and/or eye-tracking data (n=33) were collected.
Ethics and dissemination Food2Learn is performed according to Good Clinical Practice. All data collected are linked to participant number only. The results will be disseminated on group level to participants and schools. The results will be presented at conferences and published in peer-reviewed journals. The study is approved by the Medical Ethical Committee of Atrium-Orbis-Zuyd Hospital and is registered at the Netherlands Trial Register (NTR4082).
Trial registration numbers NTR4082 and NCT02240264; Pre-results.
- NUTRITION & DIETETICS
- MENTAL HEALTH
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Only known randomised controlled trial investigating the effect of increasing Omega-3 Index with krill oil supplementation on learning, cognition, behaviour and visual processing in typically developing adolescents.
First known study to select participants based on a low Omega-3 Index and includes a personalised dose adjustment based on the Omega-3 Index after 3 months of intervention.
Data on depression, self-esteem and motivation are obtained via self-reported questionnaires, which might increase the risk for systematic bias.
Owing to practical constraints, it was not possible to completely standardise the test procedure (eg, meal before the testing session and the time of testing); this could influence test results.
Introduction
There is a debate whether long-chain polyunsaturated fatty acids (LCPUFA) improve cognitive performance. LCPUFAs from the n-3 family such as docosahexaenoic acid (DHA, 22:6n-3) and eicosapentaenoic acid (EPA, 20:5n-3) are involved in many aspects of brain functioning, for example, neuronal membrane fluidity and neurotransmission.1 ,2 There is evidence that consumption of Omega-3 LCPUFAs plays a protective role in age-related cognitive decline3 and Alzheimer's disease.4 In premature babies, it has been shown that higher Omega-3 LCPUFAs consumption is associated with advanced cognitive development.5 Furthermore, in children, it might lead to improvement of symptoms associated with autism and attention deficit hyperactivity disorder (ADHD).6 Although previous research is not conclusive, it does suggest that in certain sensitive periods Omega-3 LCPUFAs might contribute to optimising cognitive performance and/or cognitive development.
Adolescence has received limited attention in studies on n-3 LCPUFAs. The brain and prefrontal cortex continue to develop until the late 20s.7–11 It is thus crucial to study the role of Omega-3 LCPUFA in adolescence as they play an important role in brain development and functioning. For example, DHA is an important structural component of the neural cell membrane, influencing membrane fluidity and signal transduction.12 ,13 Moreover, higher DHA intake has been associated with changes in the functional activity of the prefrontal cortex in boys aged 8–10 years.14 Even though EPA is only present in very small amounts in the brain,15 it is also involved in important brain processes such as neurite outgrowth, regulation of gene expression and in anti-inflammatory, antithrombotic and vasodilatory processes which might assist brain functioning.15
Studies on the relationship between measured LCPUFA status or supplementation and cognitive functioning in adolescents are, to the best of our knowledge, not available. Observational studies investigating the association between fish intake and cognitive functioning in adolescents are, however, available. Kim et al16 showed that adolescents aged 15 years who regularly consumed fish had significantly better academic performance than their non-fish consuming or less fish consuming peers. Åberg et al17 demonstrated that high fish consumption in boys at age 15 years was associated with better cognitive performance at age 18 years. Finally, de Groot et al18 studied 700 adolescents aged 12–18 years for whom fish consumption data, end-term grades (for Dutch, English and Math) and score on the Amsterdam Vocabulary Test was collected. Contrast analyses demonstrated a u-shape association between fish consumption and vocabulary (p=0.01) and a nearly significant association with average end-term grades (p=0.07). Thus, higher fish intake was associated with more advanced vocabulary and an almost significant higher average end-term grade. However, eating more fish than the recommended amount (>2 fish portion/week) was not associated with a beneficial outcome.
Studies looking at the measured LCPUFA status and depression in typically developing adolescents are also limited. We are only aware of the study by Mamalakis that showed a negative association between EPA measured in adipose tissue and score on the Beck Depression Inventory (ie, higher EPA, fewer depressive symptoms). Furthermore, a positive association between dihomogamma linolenic acid (DGLA, C20:3n-6) measured in adipose tissue and score on the Centre for Epidemiologic Studies Depression Scale (CES-D) (ie, higher DGLA, more depressive symptoms) was shown.19 This was, however, only true after correction for adiponectin. Although self-esteem has often been associated with depression,20 we found no studies taking self-esteem into account when studying the association between LCPUFA and depression in adolescents.
While observational studies point to a beneficial association between fish intake (the main source of DHA and EPA) and school grades in adolescents and since causality cannot be proven by observational studies, intervention studies are needed. Furthermore, little is known about the effects of Omega-3 fatty acids on depression and self-esteem in typically developing adolescents.
This paper describes the design of Food2Learn, a double-blind, randomised, placebo controlled intervention in which the influence of an increase in the Omega-3 Index with 1-year of krill oil supplementation on cognition, academic achievement and behaviour in typically developing adolescents is investigated. In addition, we try to counteract design issues such as bioavailability, baseline Omega-3 Index and study population which could have caused neutral results in earlier trials.21
Bioavailability
The bioavailability of DHA and EPA depends mostly on the form in which they are bound and the food matrix with which the DHA and EPA are taken. Most previous trials have chosen unemulsified ethyl-ester or triglycerides and have advised participants to consume capsules with breakfast, both of which lead to lower absorption of the LCPUFAs.21–23 In Food2Learn, krill oil is used as supplementation. Krill oil contains 30–65% of the EPA and DHA in the phospholipid form. Phospholipids have amphiphilic properties and therefore emulsifying properties that enhance absorption24–26 and are also better absorbed by the brain than triglycerides.27 Another factor important for DHA and EPA absorption is the presence of fat in the meal. Some studies report a trifold higher LCPUFA absorption when LCPUFA capsules are taken with a high fat meal, compared to a low fat meal.23 This is hypothesised to be caused by the stimulating effect of fat on pancreatic lipase.22 Therefore, participants in Food2Learn are asked to consume the capsules with dinner, the fattiest meal of the day.28
Baseline Omega-3 Index
In earlier studies, participants were often recruited without researchers knowing the baseline Omega-3 fatty acid status of participants. This has led to participants with a wide range in statuses being included, while one can expect that effects of supplementation are more likely in participants with a low Omega-3 fatty acid status. This wide range in statuses can lead to similar end Omega-3 statuses in the placebo and treatment groups and thus similar outcome measures. To increase the chance of observing any effects of supplementation, participants for Food2Learn are recruited on the basis of a low Omega-3 Index (<5%).29 The Omega-3 Index is defined as EPA plus DHA in erythrocytes and is based on a standardised analytical method.21 Additionally, to counteract interpersonal variability in the uptake/metabolism of the LCPUFA supplementation, a dose adjustment based on the individual Omega-3 Index blood levels after 3 months of supplementation was applied. This dose adjustment should ensure that participants in the active treatment group achieve the target range of 8–11%. This target range is an estimate based on the Omega-3 Index associated with the lowest mortality risk in coronary heart disease.29
Study population
Richardson showed that LCPUFA supplementation was especially beneficial in the 20% lowest performing children.30 In the Netherlands, secondary education is divided into three levels: preuniversity, higher general and lower general secondary education (LGSE). Approximately 38% of all adolescents attend LGSE.31 LGSE is further divided into four sublevels. For the current study, students from the highest sublevel, the theoretical learning pathway (TLP), were recruited. Approximately 40% of students attending LGSE are in the TLP.
Objective and hypotheses
The primary objective of Food2Learn is to study the effect of an increase in the Omega-3 Index due to 1-year of krill oil supplementation in 13–15 year-old typically developing adolescents from LGSE on cognitive performance. The secondary objective is to study the effect of an increase in the Omega-3 Index due to 1 year of krill oil supplementation in 13–15 year-old typically developing adolescents from LGSE on academic achievement and behaviour. Furthermore, the relationship between Omega-3 Index and cognitive performance, academic achievement and behaviour in typically developing adolescents will be further explored. The hypothesis is that 1 year krill oil supplementation and a higher Omega-3 Index will lead to improved cognition, academic achievement scores and behaviour scores in typically developing Dutch adolescents attending the LGSE. The third objective is to study the effect of an increase in the Omega-3 Index due to 1 year of krill oil supplementation in 13–15-year-old typically developing adolescents from LGSE on sleep quality and quantity, and visual processing.
Methods
Study design
Food2Learn is a double-blind, randomised, placebo-controlled trial, with repeated measurements (at baseline, 3 months, 6 months and 12 months) to study the effect of an increase in the Omega-3 Index due to 1-year of krill oil supplementation on cognitive performance, academic achievement and behaviour of second year LGSE students. Informed consent was obtained from all participants and their parent(s) and/or guardian(s). This trial is registered at The Netherlands Trial Register (NTR4082) and at ClinicalTrials.gov (NCT02240264). The Items from the WHO Trial Registration Data Set can be found in the online supplementary files.
Supplemental material
Participants
Inclusion and exclusion criteria
All second year students attending high school at the LGSE TLP level with a baseline Omega-3 Index <5% were eligible to participate in the study. Students were excluded if they had (1) a baseline Omega-3 Index of >5%, (2) an allergy to fish or shellfish or (3) haemophilia.
Determination of participation
Participants could discontinue participation at any time during the study. If a participant indicated that he/she wished to stop supplementation, the reason for discontinuation was asked and the participant was asked to continue with the test sessions according to the intention to treat principle, but both were voluntary.
Recruitment and screening
One hundred and twenty-three schools in the southern provinces of the Netherlands were contacted to participate in Food2Learn. Eventually, 19 school boards gave approval. The target group was then approached in a classroom setting. A video explaining the study was shown, the capsules and the finger prick were shown, and any questions were answered. Students received an information letter and were asked to discuss the study with their parents. If requested, a voluntary additional information evening was held.
If the student wanted to participate, the informed consent form had to be signed by the student and parent(s) and/or guardian(s) and handed in to the researchers at site. All students who handed in an informed consent form received a finger prick to determine the Omega-3 Index; no other prescreening methods were used. If the participant completed the whole study, he/she received a voucher for the cinema. In cohort I of Food2Learn, the needed number of participants was not enrolled; therefore, a second cohort was added to the study. Currently, cohort II is in progress.
Randomisation and blinding
On entry, participants received a participant number. An independent researcher was responsible for treatment allocation. The participants were stratified by sex and were randomly allocated to the placebo or krill oil group by an independent researcher. Equal numbers of participants were randomised to the active treatment and the placebo groups. The group allocation sequence was computer generated and executed by an independent researcher. Researchers at site were only told which box number had to be given to which participant number and were not aware how boxes were divided over placebo/krill oil group. To prevent the risk of unblinding, each participant received a personalised box with capsules. The packaging and the capsules themselves were identical for the active treatment and placebo groups. The capsules were coloured black to hide the redness of krill oil. Furthermore, a vanilla odour was added to hide any possible fishy smell/taste. Neither the researchers at the site nor the participants were informed of group allocation prior to the completion of the whole study (cohorts I and II). Preliminary unblinding of the trial was to be executed only by an independent researcher in the case of severe adverse effects.
Procedure—baseline
Before starting supplementation, participants underwent a neuropsychological test battery, filled out questionnaires and performed a standardised math test (see outcome measure, figure 1 and table 1); these tests were executed at school in a classroom setting. Three cognitive tests were administered in a group setting (10 students max): The Letter Digit Substitution Test (LDST), D2 test of Attention (D2) and Digit Span Forward (DSF) and Backward (DSB). These tests were led by one researcher via a standardised protocol, while one or two other researchers (depending on group size) made sure that participants understood the tests and complied with the protocol. All tests were first explained and a practice version was always completed by the participants. After this group test session, all participants filled out the questionnaires individually, during which participants were called one by one to perform the Stroop Test and Concept Shifting Test (CST) individually under supervision of one researcher. After data collection, participants completed a standardised computerised math test, in silence, in a classroom setting.
Questions and questionnaires at different time points

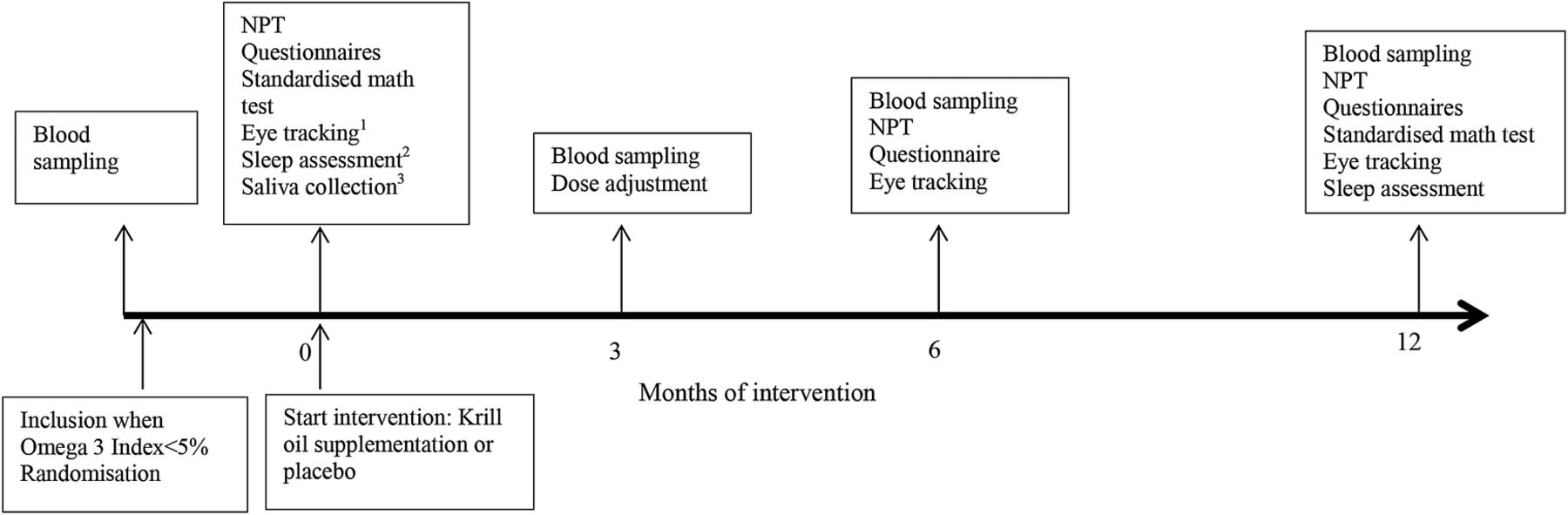{kind=link}
Timeline of study. Neuropsychological tests (NPT) are at all time points equal namely: the letter digit substitution test, D2 test of attention, digit span forward and backward, Concept Shifting Test and Stroop Test. 1Eye tracking was performed in a subsample of participants. 2Sleep was measured in a subsample of participants in the second cohort with a combination of ActivPAL accelerometer data, questionnaires and a self-reported sleep diary. 3To determine Apoe status saliva was collected.
Procedure—3 months follow-up
After 3 months of supplementation, participants again received a finger prick to determine the Omega-3 Index. Blood analyses and dose adjustments were executed by a researcher who was not actively involved in the study. When the increase in the Omega-3 Index in a participant of the active group was insufficient, the supplementation dose was adjusted in this participant and in one participant in the control group with the same number of capsules. This was carried out to ensure blinding of the researchers. However, the Omega-3 Indexes of the participants of cohort I were found to be significantly lower than the target range at 3 months. Therefore, it was decided that the dose of all participants would be increased to eight capsules per day. Furthermore, it was decided to increase the starting dose of the cohort II to eight capsules per day to ensure that the target range would be achieved.
Procedure—6 months and 12 months follow-up
The procedure completed at baseline was repeated again after 6 months. This process was again repeated after 12 months of intervention. The standardised math test was only completed at baseline and after 12 months (for an overview, see figure 1).
Intervention
After baseline neuropsychological testing, participants started with supplementation. The krill oil contained at least 40 g phospholipids per 100 g krill oil. The fatty acid profile of these phospholipids was at least 14 g EPA and 6 g DHA. The remaining composition of krill oil was mainly triglycerides (32%), free fatty acids (6–7%) and small amounts of cholesterol, cholesterol esters, ash and a trace amount of astaxanthin (80 µg/100 g). One krill oil capsule contained a total of 0.5 g krill oil, which supplied 65 mg EPA and 35 mg DHA. For the placebo capsules, a fatty acid mixture was chosen that reflects the fatty acid composition of the average European diet (26.0% C16:0, 4.6% C18:0, 35.8% C18: 1–9, 16.7% C18:2–6, 2.1% C18:3–3, 0% C20:4–6 and 14.8% other compounds).32 The placebo contained a mix of olive oil, corn oil, palm oil and medium chain triglycerides in the following ratio 4:4:9:3. The placebo contained no marine n-3 fatty acids.
In cohort I, participants were instructed to start with an intake of four capsules per day containing in total 260 mg EPA and 140 mg DHA, almost the daily recommended amount of 450 mg of EPA/DHA per day as set by the Dutch health council.33 In cohort II, the starting dose was increased to eight capsules, as cohort I showed that the initial dose of 400 mg DHA+EPA did not lead to a sufficient increase in the Omega-3 Index. Eight capsules provide 520 mg EPA and 280 mg DHA per day. To increase adherence to the protocol, participants could receive a daily text message reminder. Furthermore, participants who had an insufficient increase in their blood Omega-3 Index after 3 months of supplementation and an equal number of participants from the placebo, as noted by the independent researcher, received a phone call to try to increase compliance. Participants were asked to return all left-over capsules at the end of the study or when they decided to drop out, so compliance could be calculated on the basis of the number of capsules returned.
Outcome measures—cognitive performance measurements
The cognitive tests were selected on the basis of their usability as determined in other studies with adolescents;18 reference scores are thus available. These tests have also previously been shown to increase activation of the frontal cortex, the area of the brain associated with the accumulation of DHA,14 furthermore the prefrontal cortex is the brain area most in development during adolescence.9 Tests used were: the LDST to measure speed of information processing, D2 as a measure for selective attention, DSF and DSB as measures of short-term memory and working memory, CST as a measure for cognitive shifting and Stroop task as a measure for cognitive inhibition. For an explanation of the tests, see online supplementary appendix A.
Supplementary appendix A
Academic achievement
Math test
All students complete a standardised math test at baseline and at the end of the study. This math test is based on the end terms as set by the Dutch government. The test is computer-based and participants have to take the test without a calculator.34
School performance
All schools provide school grades (ranging from 1.0=very bad to 10.0=excellent) of participants for the subjects Dutch, English and Mathematics. These subjects are chosen as they are considered core subjects and are therefore compulsory for all students.
Behaviour measurements
Absenteeism
Schools provide the number of hours the participants were absent and the reason for absence.
Motivation
The Motivated Strategies for Learning Questionnaire consists of two parts: a motivation part and a learning strategies part.35 In this study, only the motivation part is used. The motivation section assesses student goals and value beliefs concerning school, their beliefs about their skills to succeed in school and their test anxiety. The internal consistency for the section measuring motivation is very good (α between 0.62 and 0.93).36
Mood
Mood is assessed with the Dutch version of the Centre for Epidemiologic Studies Depression Scale (CES-D),37 a tool sensitive for detecting depressive symptoms and distinguishing between depressed and non-depressed individuals.38 ,39 The CES-D has a high internal reliability in adolescents (α=0.88).40 The 20 questions questionnaire assesses the presence of depressive symptoms in the past week. Total sum scores are calculated (range 0-60), with higher scores indicating more depressive symptoms.
Self-worth/self-esteem
The Rosenberg Self-Esteem Scale (RSE) is a measure of self-esteem.41 The internal reliability in adolescents is high (α=0.88)42 ,43 and construct validity has been shown.43 This test consists of 10 questions requiring participants to indicate their level of agreement with a series of statements about themselves. Higher scores indicate a higher self-esteem.
Other measurements
Fish consumption is measured with a short, validated self-reported questionnaire.44 The pubertal phase is assessed with the Pubertal Development Scale.45 This questionnaire assesses the pubertal status of adolescents by asking to what extent a number of bodily changes related to puberty are present. Furthermore, nationality, country of birth of the participants and parents and/or guardians, language spoken at home, use of medicine, diagnosis related to learning (eg, ADHD or autism), allergies, whether the student wears glasses or contact lenses, whether he/she takes vitamins or fish oil supplements, drinking and smoking behaviour were assessed via a questionnaire. Finally, questions about school career such as whether the participant has ever skipped or repeated a year are asked. At follow-up, additional questions with regard to compliance, side effect and group allocation are asked. For an overview, see table 1.
Biological measurements
Blood analysis
Blood samples are collected with a finger prick. First, the finger of the participants is disinfected with alcohol. Then a prick with an automated one-time use lancet is administered at the fingertip after which blood drops are collected on specially prepared filter paper. Erythrocyte fatty acid compositions are analysed according to the HS-Omega-3 Index methodology as described previously.29 ,46 Fatty acid methyl esters are generated by acid transesterification and analysed by gas chromatography using hydrogen as the carrier gas. Fatty acids are identified by comparison with a standard mixture of fatty acids. Results are given as the Omega-3 Index, which is EPA+DHA expressed as a percentage of total identified fatty acids after response factor correction and a correction for the fact that whole blood was used instead of erythrocytes.46 Furthermore, the concentrations of 26 other fatty acids are determined. The coefficient of variation for EPA plus DHA typically is 5%. Analyses are quality-controlled according to DIN ISO 15189.
ApoE4- analyses
Apolipoprotein E (APOE, protein; Apoe, gene) is a protein which plays an important role in lipid homeostasis. The Apoe gene has four polymorphisms: ε2, ε3 and ε4. Studies have suggested that ε4 carriers have an increased risk of late-onset Alzheimer's disease and accelerated brain atrophy and that healthy carriers of the ε4 allele have poorer performance on neuropsychological tests.47 Furthermore, the effect of an Omega-3 supplement on cognitive performance might be modulated by the presence of ε4 polymorphisms.48 However, not all studies show an interaction between Apoe status and cognitive performance.49–51 To elucidate whether Apoe status interacts with cognitive performance in typically developing adolescents consuming LCPUFA supplementation, all participants donate 2 mL saliva for the determination of Apoe status. The analyses of the Apoe gene will be executed by the departments of Molecular Genetics and Clinical Genetics of the Maastricht University Medical Center+, according to the procedure as described by the Duke University Clinical Molecular Diagnostics Laboratory.52 Shortly, PCR amplification followed by Sanger DNA sequencing is used to determine the genotype of two single nucleotide polymorphisms in the APOE gene Rs7412 and Rs429 358 and the associated APOE genotype. With the participant's and parents’ approval (indicated in the informed consent form), samples will be kept for a maximum of 15 years.
Substudies
All students entering the main study in cohort II were asked to participate in the sleep study. Pupils of four schools (due to logistic constraints) in both cohorts were asked to participate in the eye tracking study. Participation in both substudies was voluntary and pupils could participate in the main study regardless of participation in the substudies.
Substudy I: eye tracking
A subsample of participants (n=33) participated in an eye tracking study at baseline, 6 months and 12 months. Eye tracking is a method in which eye movements of participants are recorded and can be used to calculate measures such as number of blinks, number of fixations and total duration of fixations. Eye movement measures can help reveal underlying cognitive processes such as amount of visual processing, what participants are processing and the mental effort expended. In Food2Learn, eye tracking is used to measure the effect of krill oil supplementation on cognitive processing in the form of visual processing and mental effort (for more information, see online supplementary appendix B).
Supplementary appendix B
Substudy II: sleep
In cohort II, a subsample (n=64) is included in a study investigating the relation between increasing Omega-3 fatty status and sleep quality and duration. Montgomery et al53 showed that DHA supplementation in children led to increased sleep duration and fewer waking episodes per night. Since sufficient sleep is essential for good health, cognitive performance and school performance,54–56 and insufficient sleep is common in adolescents,57 ,58 this was included as a substudy. Participants wore an ActivPAL3 (Paltechnologies, Glasgow, UK) accelerometer for seven consecutive days at baseline and seven consecutive days after 12 months of intervention. With the help of algorithms, ActivPal data can be used to determine sleep duration and quality. Furthermore, participants filled out a diary in which they noted their bedtime and wake-up time during this week. Finally, they filled out the Adolescent Sleep-Wake Scale and the Adolescent Sleep Hygiene Scale.59
Power calculation
Originally, the sample size calculation was based on a power of 0.8 and a medium effect size of 0.3 and analysis of variance (ANOVA) as the analysis method. However, new insights led to the conclusion that not ANOVA but a mixed methods analysis would be more appropriate. The power analyses were thus redone for this. Also, the new power calculation took into account that there were multiple measurement moments and that dropout is possible. Multiple calculation in RMASS software with standardised input numbers such as an average effect size of d=0.25 at 6 month follow-up and an equal or 10% higher effect size at 12 months follow-up and a dropout of 25% per measurement moment (and thus a total dropout rate of 43%), an error variation varying from 0.4 to 0.5 and a intercept variation of 0.3 to 0.5 with a slope variation of 0.0 (fixed effects), showed that between 183 and 285 participants at baseline should be sufficient to achieve a power of 0.8.
The power calculation for the sleep substudy suggested that 42 students (21 in the placebo group and 21 in the krill oil group) were sufficient. This number of students is based on power calculation with a power of 0.8, α=0.05 and the ability to detect a 20 min difference in sleep duration. For the eye tracking study, no power calculation was executed. As a study looking at the effect of krill oil supplementation on cognitive processing measured with eye tracking had never been executed before, we did not believe that a reliable power calculation would be possible.
Data analysis plan
Data are scored by one of the researchers and both D2 and CST tests are checked a second time by another researcher; 10% of the LDST and digit span are also checked by a second researcher. All data are entered twice and any discrepancies between the two data entries are checked and corrected.
Data analysis will be performed by both the intention-to-treat procedure and related to the blood Omega-3 Index. The main effects of the intervention (krill oil condition in intention-to-treat analyses) and of the Omega-3 Index on the change from baseline with regard to cognitive test scores (primary), scores on questionnaires (secondary) and school grades average (z-score; secondary) will be estimated using mixed models that account for the correlation of repeated measurements within participants. All estimates will be adjusted for drinking behaviour, smoking behaviour, level of parental education, age, sex, body mass index, pubertal status, cohort number and time trends (baseline, 6 months, 12 months) if necessary. Furthermore, moderation analyses for sex and APOE status will be executed and, if necessary, separate group analyses will be executed. Finally, an interaction between treatment condition and time trend will be used to estimate the difference between the groups regarding time trend effects. After these analyses, secondary sensitivity analyses will be executed with treatment adherence instead of intervention condition. These analyses will also be run with the subscores of the neuropsychological tests as outcome variables.
Study monitoring
The study is monitored by the METC, NWO (Dutch Scientific Organisation) and the director clinical trials research and development of AkerBiomarine. The METC and NWO receive a yearly update. NWO had one site visit. The director clinical trials research and development visits the research site twice every year and checks whether all data are complete and the research is executed according to Good Clinical Practice. The risk of participating in the study is judged to be very low as no severe adverse effects of krill oil are known; however, any adverse effects will be registered and the METC will be notified.
Ethics and dissemination
Any major amendments to the protocol will be submitted to the Medical Ethics Committee for approval. A signed and dated informed consent form is required from all participants signed by the participant and parent(s)/guardian(s). All collected data will be linked to the participant number and only the principal investigators will have access to the non-anonymised data. The principal investigators have access to all trial data. The results of the study will be disseminated on group level to participants and schools. The results of this study will also be presented at international conferences and published in peer-reviewed journals.
Included participants
In total, 288 students provided informed consent. No blood sample was obtained for four participants. One participant suffered severe hyperventilation after the blood sampling and was excluded. Two participants withdrew their consent before the study started. Fifteen participants had an Omega-3 Index of >5%. Thus, 266 participants were included in the supplementation study; baseline characteristics can be found in table 2.
Baseline participant characteristics and blood values of selected fatty acids
Discussion
To the best of our knowledge, Food2Learn is the first intervention study in which the influence of an increase in the Omega-3 Index due to 1 year of krill oil supplementation on cognition, academic achievement and behaviour in typically developing adolescents is assessed. Adolescence is a period of brain maturation in general, and especially of the higher order cognitive skills, as well as social and emotional behaviour. Furthermore, adolescence is a critical phase in the school career of students. All in all, adolescence is an important life period to study the association between LCPUFAs and cognition/school performance. Food2Learn is also one of the first studies which has recruited the participants based on a low Omega-3 Index and which makes use of a personalised dose adjustment based on individual response to supplementation. The substudies will shed light on areas that have not received much attention of the LCPUFA research community yet: sleep quantity and quality and visual processing and mental workload. The first students were enrolled in March of 2014; the final data will be collected in August 2016. The first longitudinal results of Food2Learn are expected in the second semester of 2016.
Acknowledgments
The authors would like to thank all participants and schools who participated in Food2Learn. Furthermore, the authors would also like to thank the dedicated research assistants Marije Broens-Paffen, Denise Hofman and Annemarijn Weber. Finally, the authors thank the statistician involved in the project Roeslan Leontjevas.
References
Footnotes
Contributors RHMdG, CvS and KB wrote the study protocol. Funding was acquired by RHMdG. ISMvW conducted the trial together with the research assistants. All authors contributed to the writing of the article. All authors read and approved the final manuscript.
Funding The study is funded by the grant Food, Cognition and Behaviour from the Dutch Scientific Organisation (grant number 057-13-002), Aker Biomarine (Norway) who provides the krill and placebo capsules, and Omegametrix (Germany) who is responsible for the blood analyses.
Competing interests CvS is the owner of Omegametrix, a laboratory for fatty acid analyses. KB was employed by Aker Biomarine, who is partly funding the study. All other authors declare no conflict of interest. The sponsors will have no role in the collection, analyses or interpretation of data.
Patient consent Obtained.
Ethics approval The study was approved Medical Ethical Committee of Atrium-Orbis-Zuyd Hospital (NL45803.096.13).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data will be stored in DANS Easy. Data and personal identifiers will be kept separately at all times. Data can be made available on request. For more information, contact RHMdG.