
Abstract
One of the key elements responsible for the thyroid response to thyroid-stimulating hormone (TSH) is the TSH receptor (TSHR), which belongs to the G protein-coupled receptor superfamily. Binding of TSH or stimulatory autoantibodies to the TSHR extracellular domain triggers multiple signaling pathways in target cells that are mediated through various types of G proteins and β-arrestins. Inhibitory autoantibodies, in contrast, suppress TSHR activity, inducing hypothyroid states. Activating mutations lead to constitutively active TSHR forms and can trigger cancer. Therefore, the TSHR is one of the key targets for the regulation of thyroid function and thyroid status, as well as correction of diseases caused by changes in TSHR activity (autoimmune hyper- and hypothyroidism, Graves’ ophthalmopathy, thyroid cancer). TSH preparations are extremely rarely used in medicine due to their immunogenicity and severe side effects. Most promising is the development of low-molecular allosteric TSHR regulators with an activity of full and inverse agonists and neutral antagonists, which are able to penetrate into the allosteric site located in the TSHR transmembrane domain and specifically bind to it, thus controlling the ability of the receptor to interact with G proteins and β-arrestins. Allosteric regulators do not affect the binding of TSH and autoantibodies to the receptor, which enables mild and selective regulation of thyroid function, while avoiding critical changes in TSH and thyroid hormone levels. The present review addresses the current state of the problem of regulating TSHR activity, including the possibility of using ligands of its allosteric sites.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
INTRODUCTION
The wide prevalence of thyroid pathology in the human population makes the problem of finding effective approaches to its correction extremely relevant. The worldwide incidence of thyroid dysfunctions varies from 10 to 30%, depending on dietary features at a given area, its remoteness from the sea, and the presence of adverse environmental impacts [1]. Thyroid diseases represent a heterogeneous group of endocrine pathologies, however, the pathogenesis of most of them is associated with an increased or, on the contrary, decreased activity of the thyroid-stimulating hormone receptor (TSHR), which is the main target of TSH in thyroid follicular cells responsible for the synthesis of thyroid hormones. All this makes the TSHR an attractive target for the development of new pharmacological approaches aimed at restoring thyroid function and normalizing thyroid status. Before analyzing the structural and functional organization of the TSHR and the mechanisms of regulation of its activity, it is worth briefly characterizing main thyroid diseases and the currently available ways to correct them.
THE MOST PREVALENT THYROID DISEASES
Hyperthyroidism (Graves’ disease)
Autoimmune hyperthyroidism, or Graves’ disease, is considered as one of the most common thyroid disorders. There is no consensus on the factors that certainly lead to its development, but the most important among them are genetic predisposition and female sex [2]. The pathogenesis of Graves’ disease lies in the generation of stimulatory autoantibodies to the TSHR extracellular domain, which is often accompanied by a decrease in the immune tolerance to other components of the system of thyroid hormone synthesis, such as thyroperoxidase and thyroglobulin. TSHR hyperactivation by stimulatory autoantibodies leads to an uncontrolled increase in the blood level of thyroid hormones, followed by the implementation of their systemic metabolic effects on target tissues, which leads to the clinical manifestations of hyperthyroidism.
Treatment of Graves’ disease is mainly associated with the eradication of excess hormones, either by blocking their synthesis or by reducing the volume of thyroid tissue. All the currently used approaches are associated with several complications. Although thionamide derivatives, which are the most widely used group of antithyroid drugs, have a favorable safety profile, their application entails a number of undesirable side effects, such as agranulocytosis, vasculitis, liver damage, and skin reactions [3]. Moreover, treatment with antithyroid drugs does not avoid a high risk of disease recurrence within two years after treatment discontinuation [4]. Radioiodine therapy, which is the next step in the therapeutic strategy for Graves’ disease, is characterized by a delayed effect, which necessitates simultaneously prescription of antithyroid drugs [5]. Surgical treatment is associated with risks of such complications as bleeding, infection, aesthetic defects, laryngeal nerve palsy, and hypoparathyroidism [6]. In addition, patients who have undergone total thyroidectomy have to take L-thyroxine preparations for life due to a significantly pronounced postoperative hypothyroidism.
Such a variety of side effects and sometimes quite complicated ways of their correction create an urgent need to search for qualitatively new pharmacological approaches to treating hyperthyroid conditions. One of the most interesting of them is targeted therapy, which allows affecting a specific pathogenetic link, such as the TSHR, the target of TSHR-stimulatory autoantibodies. Among such approaches under consideration is the use of autoantibodies able to block the TSHR, as well as its low-molecular allosteric antagonists. Currently, anti-TSHR autoantibodies are in different phases of clinical trials and considered as a very promising group of antithyroid drugs [7]. The allosteric regulators that modify TSHR activity will be discussed below in more detail.
Hypothyroidism
The factors that predispose to the development of hypothyroidism, including its autoimmune form, are burdened family history and female sex, but the greatest contribution to the development of this pathology is made by an alimentary iodine deficiency. A combination of factors leads to the production of autoantibodies against various components of the system of thyroid hormone synthesis, including the TSHR [8]. The classical approach to the treatment of hypothyroidism of any etiology is thyroid hormone replacement therapy, primarily by L-thyroxine. Replacement therapy is relatively safe, and side effects are typically due to overdose and iatrogenic thyroxine excess [9]. However, it should be noted that some patients with hypothyroidism have individual intolerance to thyroxin preparations, which hampers their treatment because of the lack of alternative approaches.
The development of selective agonists of thyroid hormone receptors [10] and allosteric agonists of the TSHR are promising approaches that can become an alternative to the existing therapeutic standard [11]. The mechanism of action of thyroid hormone receptor agonists consists in their specific binding to the β-isoform of these receptors, which results in the potentiation of physiological effects of the thyroid hormones thyroxine and triiodothyronine. However, for some thyromimetics, clearly pronounced toxic effects have already been found at early stages of clinical studies, as manifested in the destruction of cartilaginous and bone tissues [12]. In addition, the use of thyroid hormone receptor agonists is associated with a significant risk of cardiovascular complications. Selective allosteric TSHR agonists refer to a poorly studied, though very interesting group of drugs. The range of their clinical application is not confined to hypothyroidism and can be extended to a variety of metabolic diseases accompanied by a decreased thyroid function, such as obesity and diabetes mellitus of various etiologies. They will be discussed below in an appropriate section.
Thyroid-stimulating hormone receptor as a member of the GPCR superfamily
The TSHR belongs to a large superfamily of heterotrimeric G protein-coupled receptors (GPCRs). Their common feature is the presence of a transmembrane domain consisting of seven hydrophobic helical segments (transmembrane helices, TMHs). Despite the similar topology in the membrane, the amino acid sequences and positional relationships of these TMHs can differ significantly in different GPCR families, leading to different configurations of sites located within the transmembrane domain [13]. The extracellular domain is characterized by a highest variability of the GPCR primary structure and, in the case of the TSHR, directly binds a ligand, being responsible for its primary recognition in most other GPCRs. Intracellular GPCR loops are responsible for the activation of heterotrimeric G proteins, functional interaction with β-arrestins and other regulators of GPCR signaling, and are also targets for GPCR-specific protein kinases. Currently, up to 800 GPCRs have been identified in humans, whose functions range from controlling visual and gustatory functions to regulating reproductive and metabolic processes, as well as neurotransmission. Exactly for this reason, GPCRs are the most popular therapeutic targets when treating numerous pathologies, and more than 30% of all pharmaceuticals are targeted, directly or indirectly, on these receptors [14].
The GPCR superfamily can be divided into subfamilies based on phylogenetic analysis of their primary structures, as well as the topology of receptors in the membrane [15]. The glycoprotein hormone receptor subfamily includes the TSHR, follicle-stimulating hormone (FSH) and luteinizing hormone (LH) receptors, and belongs to a larger A (rhodopsin) family. The common feature of TSHR, as well as FSH and LH receptors, is the presence of extremely large extracellular domains (ectodomains) containing up to 340–420 amino acid residues and including leucine-rich repeats. These receptors resulted from a combination of two protein molecules, the “classical” GPCR with a heptahelical transmembrane domain and the hydrophilic β-pleated sheet protein with a regular structure, containing about ten leucine-rich repeats [16]. It has been shown that the amino acid sequence of the TSHR, as well as gonadotropin receptors, is characterized by a relatively high degree of conservatism in various vertebrates. Significant differences among TSH receptors, including those amid higher primates, are due to differences in post-translational modifications of the receptor molecule, primarily at the level of its N-glycosylation. When comparing different classes of vertebrates, e.g., fish and mammals, differences in the TSHR primary structure are expectedly higher. At the same time, the degree of homology of the TSHR primary structure in salmonids and mammals (humans, rodents) is quite high despite 100 million years that have passed since the divergence of these taxa. Meanwhile, the difference between the primary structure of these receptors within the infraclass Teleostei, on the contrary, is very significant, which may be due to a higher rate of accumulation of mutations in TSHRs of the latter [17]. Most of the differences in the primary structure of TSHRs in different vertebrates are concentrated in the N-terminal peptide and intracellular tail, while the extracellular ligand-binding and transmembrane domains are highly conserved.
STRUCTURE AND FUNCTION OF TSH RECEPTORS
Extracellular domain (ectodomain)
The extracellular domain of glycoprotein hormone receptors, including the TSHR, includes two distinct regions: an N-terminal region containing leucine-rich repeats, and a hinge region that links the ectodomain with the transmembrane domain. In the leucine-rich N-terminal region of the TSHR, there are 11 sequentially arranged repeated segments 20–30 amino acid residues long, each of which consists of a β-strand and an α-helix. They form an internal cavity which contains a high-affinity (orthosteric) site responsible for hormone binding [18]. The inner surface of this cavity is formed by the side alkyl groups of hydrophobic amino acids, whereas the side radicals of aromatic amino acids are outside. The repeated segment located in the C-terminus contains two cysteine residues that form disulfide bridges with cysteine residues located in the hinge region, which leads to a stabilization of the inactive TSHR conformation. In this case, the replacement of cysteines by serine residues, unable to form disulfide bridges, evokes permanent activation of the receptor [19].
Currently, the role of the ectodomain hinge region in glycoprotein hormone receptors in hormone binding and signal transduction is being intensively studied. This region contains the sites that can be modified with N-glycans and sulfated, which is indicative of its crucial role in the regulation of the receptor’s functional activity [20]. In 2012, Jiang et al., while studying the FSH receptor, demonstrated the critical importance of the sulfated Tyr335 residue in its hinge region as an additional, second, site for the interaction with FSH [21]. This region performs a similar function in the TSHR, because Tyr385 sulfation is required for receptor activation by a ligand [22], with the TSHR hinge region playing a key role in ligand recognition and providing the specificity of TSH interaction with its receptor [23, 24]. There are grounds to believe that the hinge region in the TSHR and gonadotropin receptors can interact to a greater extent not with the β-subunits of respective hormones, which determine their individuality, but with the α-subunits, common to both TSH and gonadotropins, whose functions consist in the physical impact of the αβ-heterodimeric pituitary hormone on the extracellular loops and transmembrane domain of the receptor. For example, after the binding of a hormone molecule to the receptor, the hinge region is “retracted” into a pocket located between the N-terminal region, which includes leucine-rich repeats, and the external entry into the transmembrane domain. Since the N-terminal part of the ectodomain has an inhibitory effect on the ability to transition into an activated conformation required for signal transduction to heterotrimeric G proteins and intracellular effectors [25, 26], ectodomain–transmembrane domain uncoupling due to such a retraction of the hinge region into the interface between them leads to the removal of the ectodomain’s inhibitory effect and receptor activation. This mechanism is supported by the fact that TSHR ectodomain removal leads to the transition of the receptor to a permanently activated form, insensitive to TSH and stimulatory antibodies [27]. An important role in the implementation of the TSHR activation mechanism can be played by a variable (during TSHR activation) location of the small decapeptide fragment located at the C-terminus of the hinge region, immediately before the first transmembrane region (TMH1), called the “internal inverse agonist” [28]. This fragment wedges in between the external termini of the TMH receptor and prevents signal transduction in the absence of a ligand. When the receptor binds to the hormone, the peptide fragment is pulled out from the entry into the receptor transmembrane channel due to a change in the conformation of the hinge region, thus leading to the activation of signal transduction [29]. Along with its impact on the activated TSHR conformation during receptor binding to the hormone, the hinge region can be a target for stimulatory autoantibodies produced during autoimmune hyperthyroidism [30]. Although autoantibodies to the hinge region, which are detected in some patients with Graves’ disease, do not activate the receptor directly, they can influence post-translational modifications of this region, primarily the sulfation of tyrosine residues, and thereby modulate the TSHR response to its interaction with stimulatory autoantibodies [31].
A modification of TSHR extracellular part by N-glycans at asparagine residues, targets for N-glycosylation, plays an exceptionally important role in TSHR functioning [32]. N-glycans typically have a negative charge and mediate the efficient binding to the TSH molecule, which is also glycosylated at both its α- and β-subunits [33]. The N-terminal domain of the TSHR contains, apart from leucine-rich repeats, five N-glycosylation sites, while there is one more such a site in the hinge region. It has been shown that, in a functionally active state, the receptor must be glycosylated at least at four N-glycosylation sites [34]. The TSHR can be glycosylated at asparagine positions 77, 99, 113, 177, 198, and 302, among which Asp113 is specific for the human TSHR, while Asp177 is specific for other mammalian TSHRs, with the other asparagine residues representing evolutionarily conserved N-glycosylation sites [33, 35]. Of all the sites, glycosylation at Asp77 exerts a greatest effect on the functional activity of the receptor, as the replacement of this residue by glutamine, which shares similar physicochemical properties, leads to a complete loss of biological activity in the mutant receptor, whereas, for example, the replacement of the Asp113 residue by glutamine only reduces the receptor affinity for the hormone [36]. Apparently, glycosylation at other sites does not have an appreciable effect on the receptor affinity for the ligand, as well as its ability to mediate an increase in the intracellular cAMP level in a TSH-bound state.
Transmembrane domain
For want of experimental data of crystallography on the TSHR and other receptors of glycoprotein hormones, still unobtained, information about the spatial structure of their transmembrane domains and conformational changes occurring in there upon binding to hormones is based solely on homologous models. These models are built on GPCRs of the same class A, for which X-ray diffraction data are available, including β-adrenergic and adenosine receptors, as well as the light-sensitive receptor protein rhodopsin [29]. Based on the analysis of the homology of transmembrane domain amino acid sequences, it is believed that the transmembrane domain of the β2-adrenergic receptor is the closest to the TSHR in terms of spatial organization [37]. However, this assumption has a number of significant limitations. Thus, in contrast to most class A GPCRs, the highly conserved proline residue localized in TMH5 (at position 5 × 50) is replaced by an alanine residue in the TSHR [29]. The proline residue is known to refer to helix-breaking residues, and its localization in the middle of TMH5 generates a hard kink in it, which contributes to the formation of a bulky ligand-binding pocket inside the transmembrane channel, as shown, for example, for β-adrenergic receptors. As the TSHR lacks proline, TMH5 forms a regular α-helix in it without any bends breaking its integrity. Another important distinction of the TSHR is the replacement of the large tryptophan residue in TMH6 (at position 6 × 48), characteristic of class A GPCRs, by a relatively small methionine, which also contributes to the formation of a more compact pocket inside the transmembrane channel of the receptor. The functional importance of this replacement is supported by the fact that the reverse replacement of methionine by tryptophan leads to a constitutively active mutant TSHR [29].
The transmembrane domain plays a key role in TSHR activation and hormonal signal transmission to the transducing components of the TSH signaling pathways, with a change in the mutual orientation of TMH, primarily TMH6, playing an important role [29, 38]. For example, hydrophobic interactions between TMH3, TMH5, and TMH6 are most important for the transition to an activated conformation as they provide the outward shift of TMH6 and a more efficient involvement of the interfaces between this helix and the third cytoplasmic loop of the receptor in interaction with G proteins [39]. Hydrophilic contacts between the inner surfaces of TMH2, TMH3, TMH6, and TMH7 also contribute to the stabilization of the activated TSHR conformation. TSH binding to its receptor leads to a change in the efficiency of interactions between the hydrophilic groups of amino acid residues inside the transmembrane channel, which, in turn, alters its configuration and increases the ability to interact functionally with the C-terminal regions of the G protein α-subunits that penetrate into this channel from the cytoplasmic side [40].
TSH receptor signaling pathways
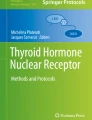
The TSHR can be activated not only by TSH, but also by thyrostimulin [41], anti-TSHR stimulatory autoantibodies, and trypsin cleaving the receptor molecule and removing the ectodomain that inhibits its basal activity [42]. Along with this, permanent TSHR activation results from mutations in its various loci and deletions in the extracellular domain region [43]. TSHR activation promotes its functional interaction with various types of heterotrimeric G proteins belonging to the Gs, Gi/o, and Gq/11 families, as well as with regulatory proteins β-arrestins [44] (Fig. 1).
The “classic” signaling pathway, which is triggered by hormone-mediated TSHR activation, is the cAMP-dependent pathway, which includes the Gs protein and adenylyl cyclase catalyzing the formation of a second messenger, cAMP [43] (Fig. 1). An increase in the intracellular cAMP concentration leads to the activation of protein kinase A and phosphorylation of the targets of this kinase, primarily the transcription factor that specifically binds to cAMP-responsive elements in promoter gene regions (cAMP response element-binding protein, CREB). It is through the activation of the CREB factor that the effects of TSH on the synthesis of thyroid hormones, as well as growth and differentiation of target cells, are implemented [45]. Prolonged elevation of cAMP levels activates signaling cascades that mediate the attenuation of cAMP-dependent signaling pathways, with one of them being mediated by the activation of Gi/o proteins and inhibition of TSH-induced adenylate cyclase activity [29].
TSHR activation via Gq/11 proteins can lead to the activation of phosphoinositide-specific phospholipase C-beta (PLC-β) and, as a result, to the triggering of calcium-dependent and 3-phosphoinositide cascades mediating a broad range of metabolic and growth processes [29, 46] (Fig. 1). PLC-β activation enhances the production of inositol-1,4,5-triphosphate, which mediates the release of calcium ions from intracellular depots and the activation of calcium-dependent proteins and transcription factors, as well as diacylglycerol, an activator of phorbol-sensitive isoforms of protein kinase C (PKC) and the mitogen-activated protein kinase pathway. All these processes promote the implementation of a wide spectrum of regulatory influences on cell growth and differentiation, as well as control over the key stages of thyroid hormone synthesis [47]. PLC-β activation also evokes the activation of phosphatidylinositol-3-kinase (PI3K), an enzyme catalyzing the synthesis of phosphatidylinositol-3,4,5-triphosphate. This, in turn, stimulates the activity of another downstream enzyme, serine/threonine protein kinase B (Akt-kinase), whose targets are a large number of enzymes and transcription factors that regulate the transcription of many genes controlling apoptosis and cell survival [46].
As noted above, the TSHR can be transitioned into a constitutively activated state by replacing a number of amino acids through site-directed mutagenesis, with most of these amino acids being located in the transmembrane domain [49]. Currently, the following activating mutations that affect amino acid residues located in TMH1, TMH2, TMH3, TMH6 and TMH7 have been identified or generated: V421I (TMH1), Y466A (TMH2), T501A (TMH3), L587V (TMH6), M637C (TMH6), M637W (TMH6), S641A (TMH6), Y643F (TMH6), L645V (TMH6) and Y667A (TMH7). Among them, the mutation M637W (TMH6) exerts a strongest activating effect, as it alters a spatial configuration of the transmembrane channel to the greatest extent, thus increasing the efficiency of mutant receptor interaction with G proteins.
All these residues are to some extent involved in the formation of the TSHR allosteric site located inside its transmembrane domain [49]. In this regard, it should be noted that in most GPCRs, the high-affinity orthosteric site is located either within the transmembrane domain or nearby the area of the extracellular entry into the transmembrane channel, while low-affinity allosteric sites reside in the extracellular loops of the receptor. However, in TSHR and gonadotropin receptors, which bind to large pituitary glycoprotein hormones, there is an inverse situation: the position of the orthosteric site in the transmembrane domain is occupied by the allosteric site, while the orthosteric site is moved to the extracellular domain. Thus, there is another very important regulatory site in the TSHR, which resides inside the transmembrane domain and remains vacant in the case of hormone-mediated receptor activation. Speaking more correctly, it contains bound water and simple ions and can become one of the targets for the regulation of the activity of TSH-dependent pathways, both positive (allosteric agonists) and negative (inverse agonists, neutral antagonists) [50].
TSH receptor allosteric regulators with activity of agonists and antagonists
The high functional importance of the TSHR in the hormonal regulation of thyroid function indicates that this receptor may become one of the promising targets for pharmacological agents designed to treat thyroid pathology. The criteria, such a drug must meet, include causing minimal side effects, maintaining normal thyroid function, being safe in pregnancy and lactation, acting at the level of pathogenesis, as well as being economically advisable. TSH preparations are virtually of no use in medicine now, neither do they meet most of the above criteria. At the same time, great prospects are currently associated with TSHR allosteric site regulators. It should be noted at this point that a similar strategy is also used in searching for new regulators and modulators of gonadotropin receptors, although in this case there are gonadotropin preparations that have been clinically used for many years to treat reproductive dysfunctions and in assisted reproductive technologies [51].
An undeniable advantage of TSHR allosteric regulators is that they do not interact with the extracellular orthosteric site, thus not preventing the binding of endogenous TSH to the receptor. Along with this, depending on their structure and features of interaction with the TSHR allosteric site, ligands of the allosteric site can be active not only as full agonists (like TSH), but also as inverse agonists and antagonists, which makes them unprecedented among biogenic regulators. As for the treatment of thyroid pathology, TSHR allosteric site ligands with different activities are in demand. Full agonists can be used to correct hypothyroidism and stimulate the pumping of radioactive iodine into thyrocytes when treating thyroid cancer. Currently, TSH is used to boost radioactive iodine uptake, however, this is associated with a number of undesirable effects. In turn, allosteric inverse agonists are instrumental in compensating for autoimmune hyperthyroidism and Graves’ ophthalmopathy, the main cause of which is circulating stimulatory anti-TSHR autoantibodies, while allosteric neutral antagonists are useful in the treatment of TSH-dependent tumors, including those of non-thyroidal localization. Importantly, TSHR allosteric regulators having the activity of inverse agonists and antagonists act gently and only partially suppress the synthesis of thyroid hormones, preventing thereby the development of acute hypothyroid conditions [52–54].
However, there are several challenges in developing TSHR allosteric regulators, among which the most significant is their potential ability to interact with transmembrane allosteric sites of gonadotropin receptors, primarily the LH receptor, which is very alike to the TSHR in terms of the structure of its allosteric site [55]. A high conservatism of the primary structure and spatial organization of the transmembrane allosteric sites of TSHR and gonadotropin receptors is due to the fact that mutational variability characterized almost exclusively the receptor ectodomain, which determines its specific interaction with various isoforms of pituitary hormones, as well as the cytoplasmic regions involved in conjugating with various transducer and regulatory proteins. At the same time, the mechanism of signal transduction to G proteins, which the transmembrane domain is mainly responsible for, remained unchanged, and this led to an evolutionary stability of the allosteric site localized in it [56]. However, despite the structural similarity, there are some differences between the allosteric sites of TSHR and gonadotropin receptors, which can be used to create selective regulators of these sites. For example, the TSHR transmembrane allosteric site, in contrast to the LH receptor allosteric site, is smaller and characterized by a large number of hydrophobic amino acid residues, including those at the external entry to the site [55]. In this regard, more hydrophilic low-molecular allosteric regulators of the LH receptor penetrate into the TSHR allosteric site with low efficiency and have low binding constants to it. For example, a relatively hydrophobic compound S37 with an activity of a TSHR allosteric inverse agonist, developed in 2019 and having a rigid framework structure, suppresses TSHR stimulation both by the hormone and by stimulatory antibodies, but does not affect the functional activity of LH and FSH receptors [57]. The thienopyrimidine derivatives with an activity of TSHR agonists and inverse antagonists, we created in our laboratory, also did not affect the activity of the LH receptor, both in vitro and in vivo [11, 52, 58, 59]. At the same time, in terms of hydrophobicity, they significantly exceeded the corresponding derivatives with an activity of LH receptor agonists and had a smaller volume of side radicals, which completely matched the structural characteristics of the TSHR allosteric site [11, 59].
The docking of low-molecular compounds, endowed with an in vitro and in vivo activity toward the TSHR, to the receptor allosteric site indicates that these compounds interact predominantly with those amino acid residues in the receptor transmembrane allosteric site, whose replacements have a greatest impact on its specific activity. At the same time, the effector specificity of allosteric regulators is of importance, as they activate or, on the contrary, inhibit certain signaling cascades that are implemented through a specific type of G proteins or β-arrestin. This makes it possible to design effector-specific regulators of the TSHR, which, unlike the hormone itself, directionally trigger a certain intracellular signaling cascade and therefore realize quite a certain biological effect.
Currently, full and inverse agonists, as well as neutral antagonists, of the TSHR have been developed (Table 1).
Thienopyrimidine derivatives Org41841 and Org43553, also known as full LH receptor agonists, were the first compounds to be developed and to demonstrate their efficiency as TSHR allosteric agonists [63]. They have also been shown to have a biological effect on the TSHR, although to a much lesser extent. Based on data on the key interactions between these allosteric regulators and the TSHR, the first model of the transmembrane domain of the TSH receptor was created using molecular modeling techniques [55], enabling further designing of new low-molecular ligands of this receptor. For example, the compound NCGC00168126-01 and its more active analog NCGC00161870-01 were developed, with both being characterized by a high selectivity for the TSHR and able to stimulate the receptor activity in the absence of TSH and stimulatory antibodies [50, 60].
Further studies were directed toward searching for compounds with activities of neutral antagonists and inverse agonists. For example, in 2008, the compound NIDDK/CEB-52 was developed, which inhibited hormone- and autoantibody-stimulated TSHR activity, thus allowing compound to be classified as a neutral antagonist [62]. Subsequently, there were synthesized the compounds NCGC00242595 and NCGC00242364 having a pronounced antagonistic activity toward the TSHR [53, 64], as well as the compound s37a which suppressed receptor stimulation not only by TSH, but also by oligoclonal antibodies characteristic of Graves’ disease [57].
Based on the structure of NCGC00165237-01, inverse agonists NCGC00161856 [65] and NCGC00229600 [50] were developed, which suppressed both stimulated and basal TSHR activity. This was important for growth suppression of tumors caused by activating mutations in the TSHR molecule, which lead to a high constitutive activity of the receptor and its inability to be stimulated by endogenous TSH.
Over the past few years, we have developed compounds with an activity of various allosteric regulators of the TSH receptor. The compound 5-amino-N-(tert-butyl)-4-(4-iodophenyl)-2-(methylthio)thieno[2,3-d]-pyrimidine-6-carboxamide (TP48) was characterized by an inverse agonist activity [58]. It reduced the TSH-stimulated production of thyroid hormones in the culture of Fischer rat thyroid follicular cells (FRTL-5), as well as basal levels of thyroid hormones when the compound was administered intraperitoneally (i.p.) to male rats at a dose of 15 mg/kg. When administered half an hour before the treatment with intranasal thyroliberin, a TSH releasing factor, TP48 inhibited a thyroliberin-stimulated increase in thyroxine and triiodothyronine levels and suppressed thyroliberin-stimulated expression of the Tg, TPO, and Dio2 genes encoding the main proteins of thyroid hormone synthesis in thyrocytes: thyroglobulin, the main source of tyrosine for the synthesis of thyroid hormones, thyroperoxidase, which performs tyrosine iodination and the condensation of iodotyrosine molecules into thyroxine, and D2-deiodinase, which converts thyroxine into triiodothyronine, an effector hormone of the thyroid system.
The compound 5-amino-N-(tert-butyl)-4-(4-(3-methoxyprop-1-yn-1-yl)phenyl)-2-(methio) thieno[2,3-d]-pyrimidine-6-carboxamide (TPY1) was similar to TP48 in its ability to suppress TSH-stimulated thyroid hormone synthesis and the expression of thyroidogenic proteins in FRTL-5 cells, as well as to inhibit the stimulating effects of thyroliberin on thyroxine and triiodothyronine production when administered to male rats [59, 66]. However, the TPY1 compound did not affect basal levels of thyroid hormones and the expression of thyroidogenic genes in the rat thyroid gland without thyroliberin treatment. All the aforesaid indicates that TPY1 is endowed with an activity of a neutral antagonist that prevents TSHR stimulation by the hormone, but does not affect the own activity of this receptor.
Compound ethyl-2-(4-(4-(5-amino-6-(tert-butylcarbamoyl)-2-(methylthio)thieno[2,3-d]-pyrimidin-4-yl)phenyl)-1H-1,2,3-triazol-1-yl) acetate (TPY3m) demonstrated the activity of a full TSHR agonist, which increases the expression of genes involved in the synthesis of thyroid hormones [11]. When administered to male rats (15 mg/kg, i.p.), TPY3m gently stimulated basal levels of thyroid hormone and increased Tg, TPO, and Dio2 gene expression. TPY3m pre-administration to rats increased the stimulating effect of thyroliberin on the level of thyroid hormones and expression of the TPO and Dio2 genes, as well as on the expression of the NIS gene encoding the sodium-iodide symporter NIS responsible for iodide uptake by thyroid follicular cells. The TPY3m-induced increase in the expression of the Tshr gene encoding the TSHR in the thyroid gland of control and thyroliberin-treated rats can also contribute significantly to the stimulating effect of TPY3m [11].
Along with allosteric regulators interacting with the transmembrane allosteric site, it seems promising to develop ligands for allosteric sites localized in the TSHR cytoplasmic loops, primarily in its second and third cytoplasmic loops, which contain key molecular determinants responsible for the interaction with G proteins. In this regard, palmitoylated peptide fragments of the TSHR third cytoplasmic loop are promising, as they are able to stimulate the activity of the receptor in the absence of TSH by changing the conformation of its cytoplasmic allosteric sites and thereby to modulate the interaction of the receptor with G proteins [67–69].
Possible mechanisms of action of TSH receptor allosteric regulators
Among the possible mechanisms underlying the inhibitory effect of TSHR allosteric antagonists/inversion agonists, the two hypothetical molecular mechanisms have been proposed (Fig. 2). The first of them consists in allosteric ligand-induced stabilization of the “ionic lock” which represents a polar interaction between a positively charged arginine residue, located at the border of TMH3 and the second cytoplasmic loop, and negatively charged residues of glutamic or aspartic acids residing at the border of TMH6 and the third cytoplasmic loop [64]. The main function of the “ionic lock” is to stabilize the inactive conformation of the receptor. By stabilizing the “ionic lock”, antagonist prevents conformational changes leading to TSHR activation, which blocks the binding of the TSH-TSHR complex to G proteins [70]. At the same time, TSHR allosteric full agonists can destabilize the “ionic lock”, induce conformational changes, primarily due to altering the spatial localization of TMH6 in the transmembrane domain, and thereby stimulate signal transduction to intracellular cascades [71] (Fig. 2).
Another mechanism of action of allosteric antagonists may lie in mechanical impediments to a normal movement of the hinge region in the TSHR extracellular domain [57]. In this case, an antagonist wedges in between the receptor’s extracellular loops and “freezes” the hinge region, preventing it from undergoing conformational rearrangements upon binding of TSH or stimulatory autoantibodies to the extracellular domain. However, given that allosteric regulators penetrate into the TSHR transmembrane domain, it is not entirely clear how they can directly influence hinge motility.
It cannot also be ruled out that allosteric regulators affect the ability of TSHRs to form dimeric and oligomeric complexes, thus influencing their activity and the selectivity of signal transduction to intracellular targets most directly [70]. Such a possibility has been demonstrated for the FSH receptor. The interaction of allosteric regulators with one of the monomers of the FSH receptor oligomeric complex leads to an attenuation of the interaction between the monomers and modifies the ability of receptor molecules to interact with the hormone [72].

TSH signaling pathways in thyrocytes (modified from [48]). Abbreviations: TSH, thyroid-stimulating hormone; PLC, phosphoinositide-specific phospholipase C-β; PI3K, phosphatidylinositol-3-kinase; PKC, calcium-sensitive isoform of protein kinase C; cAMP, cyclic AMP; PKA, cAMP-activated serine/threonine protein kinase A; CREB, transcription factor interacting with the cAMP-response element; PDK1, phosphoinositide-dependent kinase-1; Akt, serine/threonine protein kinase B; mTOR, rapamycin-sensitive kinase encoded by the MTOR (mammalian target of rapamycin) gene belonging to the family of PI3K-like kinases; NFkB, nuclear factor kB; Raf, protooncogenic serine/threonine protein kinase belonging to the family of mitogen-activated protein kinases, a product of the Raf1 gene which phosphorylates MEK1/2 kinase; MEK1/2, mitogen-activated protein kinase, which phosphorylates ERK1/2 kinase; ERK1/2, terminal kinase in the mitogen-activated protein kinase cascade, regulated by extracellular signals; Elk1, ternary complex factor encoded by the Elk1 gene and functioning as a transcription activator.

The mechanism of functioning of the “ion lock” in the TSH receptor (modified from [70]).
CONCLUSION
The obtained experimental and clinical data indicate that the TSH receptor can be considered as one of the most important targets for thyroid function regulation, thyroid status control, and the correction of diseases caused by TSHR hyperactivation (Graves’ disease, cancers caused by activating mutations in the TSHR) or a decrease in its activity (hypothyroid states). Paradoxically, TSH and various constructs based thereupon cannot be widely used to correct the functions of the thyroid system due to their high immunogenicity and grave side effects, while the development of approaches to using stimulating or inhibitory anti-TSHR autoantibodies at its infancy, while their possible applications entails a number of undesirable consequences typical for autoimmune diseases of the thyroid gland. In this regard, TSHR low-molecular allosteric regulators are of considerable interest as they can be endowed with an activity of both full agonists and inverse agonists/antagonists. They interact with the allosteric site located in the transmembrane domain and do not affect its binding to the hormone or autoantibodies, which is realized via the TSHR extracellular regions. The development of allosteric regulators enables finer and milder regulation of TSHR activity without eliciting critical changes in TSH and thyroid hormone levels.
REFERENCES
Vanderpump MPJ (2019) Epidemiology of Thyroid Disorders. In: The Thyroid and Its Diseases. Springer Int Publ, Cham, 75–85.
Wémeau J, Klein M, Sadoul J-L, Briet C, Vélayoudom-Céphise F-L (2018) Graves’ disease: Introduction, epidemiology, endogenous and environmental pathogenic factors. Ann Endocrinol 79: 599–607. https://doi.org/10.1016/j.ando.2018.09.002
Burch HB, Cooper DS (2018) Antithyroid drug therapy: 70 years later. Eur J Endocrinol 179: R261–R274. https://doi.org/10.1530/EJE-18-0678
Vos XG, Endert E, Zwinderman AH, Tijssen JGP, Wiersinga WM (2016) Predicting the Risk of Recurrence Before the Start of Antithyroid Drug Therapy in Patients With Graves’ Hyperthyroidism. J Clin Endocrinol Metabolism 101: 1381–1389. https://doi.org/10.1210/jc.2015-3644
Walter MA, Briel M, Christ-Crain M, Bonnema SJ, Connell J, Cooper DS, Bucher HC, Müller-Brand J, Müller B (2007) Effects of antithyroid drugs on radioiodine treatment: systematic review and meta-analysis of randomised controlled trials. BMJ 334: 514. https://doi.org/10.1136/bmj.39114.670150.BE
Bartalena L, Piantanida E, Gallo D, Ippolito S, Tanda ML (2022) Management of Graves’ hyperthyroidism: present and future. Exp Rev Endocrinol Metabol 17: 153–166. https://doi.org/10.1080/17446651.2022.2052044
Furmaniak J, Sanders J, Sanders P, Li Y, Rees Smith B (2022) TSH receptor specific monoclonal autoantibody K1-70 TM targeting of the TSH receptor in subjects with Graves’ disease and Graves’ orbitopathy—Results from a phase I clinical trial. Clin Endocrinol 96: 878–887. https://doi.org/10.1111/cen.14681
Garber JR, Cobin RH, Gharib H, Hennessey JV, Klein I, Mechanick JI, Pessah-Pollack R, Singer PA, Woeber KA (2012) Clinical Practice Guidelines for Hypothyroidism in Adults: Cosponsored by the American Association of Clinical Endocrinologists and the American Thyroid Association. Endocr Pract 18: 988–1028. https://doi.org/10.4158/EP12280.GL
Jonklaas J, Bianco AC, Bauer AJ, Burman KD, Cappola AR, Celi FS, Cooper DS, Kim BW, Peeters RP, Rosenthal MS, Sawka AM (2014) Guidelines for the Treatment of Hypothyroidism: Prepared by the American Thyroid Association Task Force on Thyroid Hormone Replacement. Thyroid 24: 1670–1751. https://doi.org/10.1089/thy.2014.0028
Grover G, Mellstrom K, Malm J (2007) Therapeutic Potential for Thyroid Hormone Receptor-β Selective Agonists for Treating Obesity, Hyperlipidemia and Diabetes. Current Vasc Pharmacol 5: 141–154. https://doi.org/10.2174/157016107780368271
Bakhtyukov AA, Derkach KV, Fokina EA, Sorokoumov VN, Zakharova IO, Bayunova L V, Shpakov AO (2022) Development of Low-Molecular-Weight Allosteric Agonist of Thyroid-Stimulating Hormone Receptor with Thyroidogenic Activity. Dokl Biochem Biophys 503: 67–70. https://doi.org/10.1134/S1607672922020016
Meruvu S, Ayers SD, Winnier G, Webb P (2013) Thyroid Hormone Analogues: Where Do We Stand in 2013? Thyroid 23: 1333–1344. https://doi.org/10.1089/thy.2012.0458
Núñez Miguel R, Sanders J, Furmaniak J, Smith BR (2017) Structure and activation of the TSH receptor transmembrane domain. Autoimmun Highlights 8: 2. https://doi.org/10.1007/s13317-016-0090-1
Hauser AS, Attwood MM, Rask-Andersen M, Schiöth HB, Gloriam DE (2017) Trends in GPCR drug discovery: new agents, targets and indications. Nature Rev Drug Discov 16: 829–842. https://doi.org/10.1038/nrd.2017.178
Katritch V, Cherezov V, Stevens RC (2013) Structure-Function of the G Protein–Coupled Receptor Superfamily. Ann Rev Pharmacol Toxicol 53: 531–556. https://doi.org/10.1146/annurev-pharmtox-032112-135923
Hsu SY, Hsueh AJW (2000) Discovering New Hormones, Receptors, and Signaling Mediators in the Genomic Era. Mol Endocrinol 14: 594–604. https://doi.org/10.1210/mend.14.5.0472
Kaczur V, Puskás LG, Takács M, Rácz IA, Szendrői A, Tóth S, Nagy Z, Szalai C, Balázs C, Falus A, Knudsen B, Farid NR (2003) Evolution of the thyrotropin receptor: a G protein coupled receptor with an intrinsic capacity to dimerize. Mol Genet Metabol 78: 275–290. https://doi.org/10.1016/S1096-7192(03)00036-2
Ulloa-Aguirre A, Zariñán T, Jardón-Valadez E, Gutiérrez-Sagal R, Dias JA (2018) Structure-Function Relationships of the Follicle-Stimulating Hormone Receptor. Front Endocrinol 9: 707. https://doi.org/10.3389/fendo.2018.00707
Ho SC, van Sande J, Lefort A, Vassart G, Costagliola S (2001) Effects of Mutations Involving the Highly Conserved S281HCC Motif in the Extracellular Domain of the Thyrotropin (TSH) Receptor on TSH Binding and Constitutive Activity*. Endocrinology 142: 2760–2767. https://doi.org/10.1210/endo.142.7.8246
Mueller S, Jaeschke H, Günther R, Paschke R (2010) The hinge region: an important receptor component for GPHR function. Trends Endocrinol Metabol 21: 111–122. https://doi.org/10.1016/j.tem.2009.09.001
Jiang X, Liu H, Chen X, Chen P-H, Fischer D, Sriraman V, Yu HN, Arkinstall S, He X (2012) Structure of follicle-stimulating hormone in complex with the entire ectodomain of its receptor. Proc Natl Acad Sci USA 109: 12491–12496. https://doi.org/10.1073/pnas.1206643109
Costagliola S (2002) Tyrosine sulfation is required for agonist recognition by glycoprotein hormone receptors. The EMBO J 21: 504–513. https://doi.org/10.1093/emboj/21.4.504
Schaarschmidt J, Huth S, Meier R, Paschke R, Jaeschke H (2014) Influence of the Hinge Region and Its Adjacent Domains on Binding and Signaling Patterns of the Thyrotropin and Follitropin Receptor. PLoS One 9: e111570. https://doi.org/10.1371/journal.pone.0111570
Mueller S, Kleinau G, Jaeschke H, Paschke R, Krause G (2008) Extended Hormone Binding Site of the Human Thyroid Stimulating Hormone Receptor. J Biol Chem 283: 18048–18055. https://doi.org/10.1074/jbc.M800449200
Vlaeminck-Guillem V, Ho S-C, Rodien P, Vassart G, Costagliola S (2002) Activation of the cAMP pathway by the TSH receptor involves switching of the ectodomain from a tethered inverse agonist to an agonist. Mol Endocrinol 16: 736–746. https://doi.org/10.1210/mend.16.4.0816
Zhang M, Tong KP, Fremont V, Chen J, Narayan P, Puett D, Weintraub BD, Szkudlinski MW (2000) The extracellular domain suppresses constitutive activity of the transmembrane domain of the human TSH receptor: implications for hormone-receptor interaction and antagonist design. Endocrinology 141: 3514–3517. https://doi.org/10.1210/endo.141.9.7790
Mizutori Y, Chen C-R, McLachlan SM, Rapoport B (2008) The Thyrotropin Receptor Hinge Region Is Not Simply a Scaffold for the Leucine-Rich Domain but Contributes to Ligand Binding and Signal Transduction. Mol Endocrinol 22: 1171–1182. https://doi.org/10.1210/me.2007-0407
Brüser A, Schulz A, Rothemund S, Ricken A, Calebiro D, Kleinau G, Schöneberg T (2016) The Activation Mechanism of Glycoprotein Hormone Receptors with Implications in the Cause and Therapy of Endocrine Diseases. J Biol Chem 291: 508–520. https://doi.org/10.1074/jbc.M115.701102
Kleinau G, Worth CL, Kreuchwig A, Biebermann H, Marcinkowski P, Scheerer P, Krause G (2017) Structural–Functional Features of the Thyrotropin Receptor: A Class A G-Protein-Coupled Receptor at Work. Front Endocrinol 8: 86. https://doi.org/10.3389/fendo.2017.00086
Chen C-R, McLachlan SM, Rapoport B (2009) A Monoclonal Antibody with Thyrotropin (TSH) Receptor Inverse Agonist and TSH Antagonist Activities Binds to the Receptor Hinge Region as Well as to the Leucine-Rich Domain. Endocrinology 150: 3401–3408. https://doi.org/10.1210/en.2008-1800
Sun S, Summachiwakij S, Schneck O, Morshed SA, Ma R, Latif R, Davies TF (2019) Antigenic “Hot-Spots” on the TSH Receptor Hinge Region. Front Endocrinol 9: 765. https://doi.org/10.3389/fendo.2018.00765
Kursawe R, Paschke R (2007) Modulation of TSHR signaling by posttranslational modifications. Trends Endocrinol Metabol 18: 199–207. https://doi.org/10.1016/j.tem.2007.05.002
Korta P, Pocheć E (2019) Glycosylation of thyroid-stimulating hormone receptor. Endokrynol Pol 70: 86–100. https://doi.org/10.5603/EP.a2018.0077
Nagayama Y, Nishihara E, Namba H, Yamashita S, Niwa M (2000) Identification of the sites of asparagine-linked glycosylation on the human thyrotropin receptor and studies on their role in receptor function and expression. J Pharmacol Exp Ther 295: 404–409.
Ząbczyńska M, Kozłowska K, Pocheć E (2018) Glycosylation in the Thyroid Gland: Vital Aspects of Glycoprotein Function in Thyrocyte Physiology and Thyroid Disorders. Int J Mol Sci 19: 2792. https://doi.org/10.3390/ijms19092792
Russo D, Chazenbalk GD, Nagayama Y, Wadsworth HL, Rapoport B (1991) Site-Directed Mutagenesis of the Human Thyrotropin Receptor: Role of Asparagine-Linked Oligosaccharides in the Expression of a Functional Receptor. Mol Endocrinol 5: 29–33. https://doi.org/10.1210/mend-5-1-29
Costanzi S, Wang K (2014) The GPCR Crystallography Boom: Providing an Invaluable Source of Structural Information and Expanding the Scope of Homology Modeling. Adv Exp Med Biol 796: 3–13.
Rasmussen SGF, DeVree BT, Zou Y, Kruse AC, Chung KY, Kobilka TS, Thian FS, Chae PS, Pardon E, Calinski D, Mathiesen JM, Shah STA, Lyons JA, Caffrey M, Gellman SH, Steyaert J, Skiniotis G, Weis WI, Sunahara RK, Kobilka BK (2011) Crystal structure of the β2 adrenergic receptor–Gs protein complex. Nature 477: 549–555. https://doi.org/10.1038/nature10361
Karges B, Krause G, Homoki J, Debatin K-M, de Roux N, Karges W (2005) TSH receptor mutation V509A causes familial hyperthyroidism by release of interhelical constraints between transmembrane helices TMH3 and TMH5. J Endocrinol 186: 377–385. https://doi.org/10.1677/joe.1.06208
Brüser A, Schulz A, Rothemund S, Ricken A, Calebiro D, Kleinau G, Schöneberg T (2016) The Activation Mechanism of Glycoprotein Hormone Receptors with Implications in the Cause and Therapy of Endocrine Diseases. J Biol Chem 291: 508–520. https://doi.org/10.1074/jbc.M115.701102
Nakabayashi K, Matsumi H, Bhalla A, Bae J, Mosselman S, Hsu SY, Hsueh AJW (2002) Thyrostimulin, a heterodimer of two new human glycoprotein hormone subunits, activates the thyroid-stimulating hormone receptor. J Clin Invest 109: 1445–1452. https://doi.org/10.1172/JCI14340
van Sande J, Massart C, Costagliola S, Allgeier A, Cetani F, Vassart G, Dumont JE (1996) Specific activation of the thyrotropin receptor by trypsin. Mol Cell Endocrinol 119: 161–168. https://doi.org/10.1016/0303-7207(96)03804-X
Kleinau G, Krause G (2009) Thyrotropin and Homologous Glycoprotein Hormone Receptors: Structural and Functional Aspects of Extracellular Signaling Mechanisms. Endocr Rev 30: 133–151. https://doi.org/10.1210/er.2008-0044
Eichel K, von Zastrow M (2018) Subcellular Organization of GPCR Signaling. Trends Pharmacol Sci 39: 200–208. https://doi.org/10.1016/j.tips.2017.11.009
Morshed SA, Latif R, Davies TF (2009) Characterization of Thyrotropin Receptor Antibody-Induced Signaling Cascades. Endocrinology 150: 519–529. https://doi.org/10.1210/en.2008-0878
Hamm HE (1998) The Many Faces of G Protein Signaling. J Biol Chem 273: 669–672. https://doi.org/10.1074/jbc.273.2.669
Jang D, Marcus-Samuels B, Morgan SJ, Klubo-Gwiezdzinska J, Neumann S, Gershengorn MC (2020) Thyrotropin regulation of differentiated gene transcription in adult human thyrocytes in primary culture. Mol Cell Endocrinol 518: 111032. https://doi.org/10.1016/j.mce.2020.111032
Chu Y-D, Yeh C-T (2020) The Molecular Function and Clinical Role of Thyroid Stimulating Hormone Receptor in Cancer Cells. Cells 9: 1730. https://doi.org/10.3390/cells9071730
Hoyer I, Haas A-K, Kreuchwig A, Schülein R, Krause G (2013) Molecular sampling of the allosteric binding pocket of the TSH receptor provides discriminative pharmacophores for antagonist and agonists. Biochem Soc Transact 41: 213–217. https://doi.org/10.1042/BST20120319
Neumann S, Gershengorn MC (2011) Small molecule TSHR agonists and antagonists. Ann d’Endocrinol 72: 74–76. https://doi.org/10.1016/j.ando.2011.03.002
Jungheim E, Meyer M, Broughton D (2015) Best Practices for Controlled Ovarian Stimulation in In Vitro Fertilization. Seminars Reproduct Med 33: 077–082. https://doi.org/10.1055/s-0035-1546424
Shpakov AO (2021) Endogenous and Synthetic Regulators of the Peripheral Components of the Hypothalamo-Hypophyseal-Gonadal and -Thyroid Axes. Neurosci Behav Physiol 51: 332–345. https://doi.org/10.1007/s11055-021-01076-4
Turcu AF, Kumar S, Neumann S, Coenen M, Iyer S, Chiriboga P, Gershengorn MC, Bahn RS (2013) A Small Molecule Antagonist Inhibits Thyrotropin Receptor Antibody-Induced Orbital Fibroblast Functions Involved in the Pathogenesis of Graves Ophthalmopathy. The J Clin Endocrinol Metabol 98: 2153–2159. https://doi.org/10.1210/jc.2013-1149
Krause G, Marcinkowski P (2018) Intervention Strategies into Glycoprotein Hormone Receptors for Modulating (Mal–)function, with Special Emphasis on the TSH Receptor. Hormone and Metabol Res 50: 894–907. https://doi.org/10.1055/a-0749-6528
Jäschke H, Neumann S, Moore S, Thomas CJ, Colson A-O, Costanzi S, Kleinau G, Jiang J-K, Paschke R, Raaka BM, Krause G, Gershengorn MC (2006) A Low Molecular Weight Agonist Signals by Binding to the Transmembrane Domain of Thyroid-stimulating Hormone Receptor (TSHR) and Luteinizing Hormone/Chorionic Gonadotropin Receptor (LHCGR). J Biol Chem 281: 9841–9844. https://doi.org/10.1074/jbc.C600014200
Knudsen B, Farid NR (2004) Evolutionary divergence of thyrotropin receptor structure. Mol Genetics and Metabol 81: 322–334. https://doi.org/10.1016/j.ymgme.2004.01.010
Marcinkowski P, Hoyer I, Specker E, Furkert J, Rutz C, Neuenschwander M, Sobottka S, Sun H, Nazare M, Berchner-Pfannschmidt U, von Kries JP, Eckstein A, Schülein R, Krause G (2019) A New Highly Thyrotropin Receptor-Selective Small-Molecule Antagonist with Potential for the Treatment of Graves’ Orbitopathy. Thyroid 29: 111–123. https://doi.org/10.1089/thy.2018.0349
Derkach KV, Bakhtyukov AA, Sorokoumov VN, Shpakov AO (2020) New Thieno-[2,3-d]pyrimidine-Based Functional Antagonist for the Receptor of Thyroid Stimulating Hormone. Dokl Biochem Biophys 491: 77–80. https://doi.org/10.1134/S1607672920020064
Derkach KV, Fokina EA, Bakhtyukov AA, Sorokoumov VN, Stepochkina AM, Zakharova IO, Shpakov AO (2022) The Study of Biological Activity of a New Thieno[2,3-D]-Pyrimidine-Based Neutral Antagonist of Thyrotropin Receptor. Bull Exp Biol Med 172: 713–717. https://doi.org/10.1007/s10517-022-05462-x
Neumann S, Huang W, Titus S, Krause G, Kleinau G, Alberobello AT, Zheng W, Southall NT, Inglese J, Austin CP, Celi FS, Gavrilova O, Thomas CJ, Raaka BM, Gershengorn MC (2009) Small-molecule agonists for the thyrotropin receptor stimulate thyroid function in human thyrocytes and mice. Proc Natl Acad Sci USA 106: 12471–12476. https://doi.org/10.1073/pnas.0904506106
Boutin A, Allen MD, Geras-Raaka E, Huang W, Neumann S, Gershengorn MC (2011) Thyrotropin Receptor Stimulates Internalization-Independent Persistent Phosphoinositide Signaling. Mol Pharmacol 80: 240–246. https://doi.org/10.1124/mol.111.072157
Neumann S, Kleinau G, Costanzi S, Moore S, Jiang J, Raaka BM, Thomas CJ, Krause G, Gershengorn MC (2008) A Low-Molecular-Weight Antagonist for the Human Thyrotropin Receptor with Therapeutic Potential for Hyperthyroidism. Endocrinology 149: 5945–5950. https://doi.org/10.1210/en.2008-0836
Moore S, Jaeschke H, Kleinau G, Neumann S, Costanzi S, Jiang J, Childress J, Raaka BM, Colson A, Paschke R, Krause G, Thomas CJ, Gershengorn MC (2006) Evaluation of Small-Molecule Modulators of the Luteinizing Hormone/Choriogonadotropin and Thyroid Stimulating Hormone Receptors: Structure–Activity Relationships and Selective Binding Patterns. J Med Chem 49: 3888–3896. https://doi.org/10.1021/jm060247s
Neumann S, Nir EA, Eliseeva E, Huang W, Marugan J, Xiao J, Dulcey AE, Gershengorn MC (2014) A selective TSH receptor antagonist inhibits stimulation of thyroid function in female mice. Endocrinology 155: 310–314. https://doi.org/10.1210/en.2013-1835
Neumann S, Huang W, Eliseeva E, Titus S, Thomas CJ, Gershengorn MC (2010) A Small Molecule Inverse Agonist for the Human Thyroid-Stimulating Hormone Receptor. Endocrinology 151: 3454–3459. https://doi.org/10.1210/en.2010-0199
Bakhtuykov A, Derkach K, Sorokoumov V, Fokina E, Shpakov A (2021) The development of new low-molecular-weight allosteric antagonists of thyroid-stimulating hormone receptor and their effect on the basal and thyroliberin-stimulated production of thyroid hormones. FEBS Open Bio 11: 103–507. https://doi.org/10.1002/2211-5463.13205
Shpakova EA, Shpakov AO, Chistyakova OV, Moyseyuk IV, Derkach KV (2012) Biological activity in vitro and in vivo of peptides corresponding to the third intracellular loop of thyrotropin receptor. Dokl Biochem Biophys 443: 64–67. https://doi.org/10.1134/S1607672912020020
Shpakov AO, Shpakova EA, Tarasenko II, Derkach KV (2014) Peptide 612–627 of thyrotropin receptor and its modified analogs as regulators of adenylyl cyclase in rat thyroid gland. Cell and Tissue Biol 8: 488–498. https://doi.org/10.1134/S1990519X1406008X
Derkach KV, Shpakova EA, Titov AK, Shpakov AO (2015) Intranasal and Intramuscular Administration of Lysine-Palmitoylated Peptide 612–627 of Thyroid-Stimulating Hormone Receptor Increases the Level of Thyroid Hormones in Rats. Int J Peptide Res Therap 21: 249–260. https://doi.org/10.1007/s10989-014-9452-6
Davies TF, Ali MR, Latif R (2014) Allosteric Modulators Hit the TSH Receptor. Endocrinology 155: 1–5. https://doi.org/10.1210/en.2013-2079
Audet M, Bouvier M (2012) Restructuring G-Protein-Coupled Receptor Activation. Cell 151: 14–23. https://doi.org/10.1016/j.cell.2012.09.003
Nataraja S, Sriraman V, Palmer S (2018) Allosteric Regulation of the Follicle-Stimulating Hormone Receptor. Endocrinology 159: 2704–2716. https://doi.org/10.1210/en.2018-00317
Funding
This work was supported by the Russian Science Foundation (no. 19-75-20122).
Author information
Authors and Affiliations
Contributions
Reviewing of literature sources, the writing of the working manuscript (E.A.F.), conceptualization and manuscript editing (A.O.S.).
Corresponding author
Ethics declarations
CONFLICT OF INTEREST
The authors declare that they have no conflict of interest that might be related with the publication of this article.
Additional information
Translated by A. Polyanovsky
Russian Text © The Author(s), 2022, published in Rossiiskii Fiziologicheskii Zhurnal imeni I.M. Sechenova, 2022, Vol. 108, No. 9, pp. 1094–1113https://doi.org/10.31857/S0869813922090060.
Rights and permissions
Open Access. This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Fokina, E.F., Shpakov, A.O. Thyroid-Stimulating Hormone Receptor: the Role in the Development of Thyroid Pathology and Its Correction. J Evol Biochem Phys 58, 1439–1454 (2022). https://doi.org/10.1134/S0022093022050143
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1134/S0022093022050143